
Abstract
Chronic superior vena cava (SVC) occlusion is a challenging complication in hemodialysis patients, particularly when conventional endovascular approaches fail. We describe the successful use of a manually straightened transseptal needle for sharp recanalization in a symptomatic dialysis patient with extensive collateralization and exhausted access options. Prior attempts using re-entry devices and back-ends of stiff guidewires had been unsuccessful. Under biplanar fluoroscopy, the transseptal needle was advanced transfemorally to cross the occlusion, allowing passage of a 0.018″ guidewire and subsequent snaring through a left axillary loop graft. A VBX 11 × 39 mm balloon-expandable stent-graft was deployed and post-dilated to 14 mm. Clinical symptoms, including facial and upper limb edema with prominent thoracic collateral veins, resolved by the following morning. No complications occurred, and patency remains stable at 9 months. This case highlights the utility of transseptal needles as a readily available sharp recanalization tool in expert centers, especially when other strategies have failed.
Keywords
Introduction
Chronic occlusion of the superior vena cava (SVC) in dialysis patients is a significant clinical problem, often resulting from prolonged use of central venous catheters. 1 Endovascular recanalization is the first-line approach, but standard wire and catheter techniques may fail in long-standing, fibrotic occlusions. In such cases, sharp recanalization techniques, including the use of transseptal needles, may be considered.2,3
A variety of tools have been described to perform sharp recanalization, including re-entry catheters, radiofrequency (RF) wires, and the back-end of stiff guidewires.3,4 However, many of these devices are either expensive or not widely available in all countries. In contrast, transseptal needles are accessible in most interventional suites, originally designed for left atrial access.
This technical note describes a successful endovascular recanalization of a chronic SVC occlusion using a transseptal needle in a patient with no alternative access for hemodialysis. The procedure was performed by vascular surgeons with extensive experience in thoracic and complex venous interventions, including prior use of sharp techniques in iliocaval occlusions.
Technical report
A 66-year-old woman with hypertension, dyslipidemia, and end-stage renal disease of indeterminate etiology was on chronic hemodialysis via a left axillary loop graft, in use for the past 3 months. Since the initiation of dialysis through this access, she developed typical symptoms of superior vena cava (SVC) syndrome, including facial swelling, upper limb congestion, and exuberant thoracic collateral circulation. She had a history of multiple prior central venous catheters. Imaging revealed a chronic total occlusion of the SVC with extensive collateralization (Figure 1). Surgical ligation of the graft and placement of a permanent femoral tunneled catheter were being considered due to symptom severity.
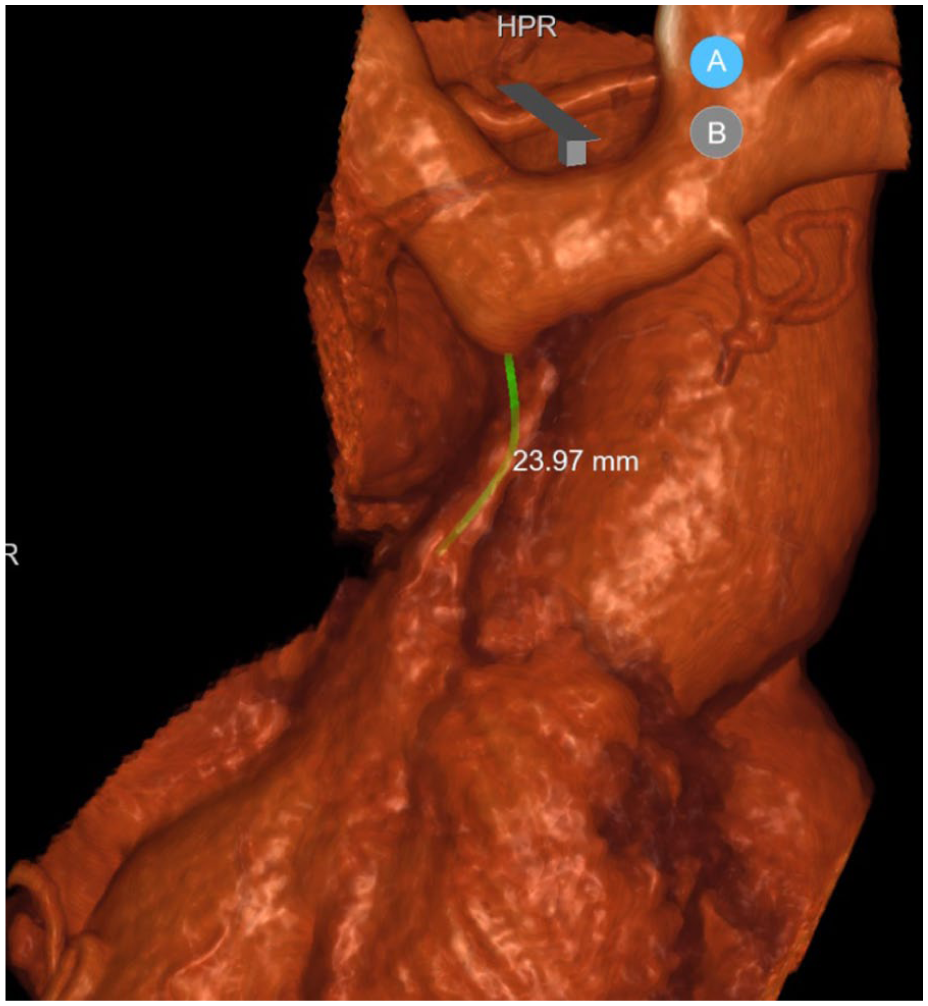
3D reconstruction of the CT-angiogram depicting the short, occluded segment of the superior vena cava.
A previous recanalization attempt via a combined antegrade approach (through the dialysis graft) and retrograde transfemoral access had failed, with access to various re-entry techniques, including the needle-based re-entry device and the back-end of multiple guidewires (0.035″, 0.018″, and 0.014″). However, none crossed the occlusion. She was electively readmitted for a second attempt using advanced sharp recanalization.
Under general anesthesia, a 6-Fr introducer was placed in the left axillary loop graft and an 8-Fr long sheath in the right common femoral vein. Biplanar fluoroscopy was used to map the occluded segment. A Brockenbrough BRK transseptal needle, which has a natural curvature, was manually straightened on the table prior to use, as no straight transseptal variants are commercially available. Chiba needles were not suitable due to insufficient working length (<20 cm), whereas sharp recanalization of SVC chronic occlusions from transfemoral access typically requires a working length of approximately 50–65 cm. As illustrated in Figure 2(b), the needle was fully straightened to eliminate all curvature memory. It was introduced through an 8-Fr long sheath to maintain directional control and procedural safety. A controlled puncture was performed under roadmap guidance. Positioning within the central venous system was confirmed via contrast injection through the needle (Figure 3).

Transseptal needle: (a) regular curved configuration and (b) after manual straightening before advancement.

Lateral view: (a) roadmap showing advancement of the straightened transseptal needle from the transfemoral 8-Fr sheath and (b) angiogram through the needle confirming intravenous positioning.
A 0.018″ Halberd guidewire was advanced through the needle and captured from the axillary access using a 30-mm snare, establishing a through-and-through access (Figure 4a). A 5.5 × 80-mm semi-compliant balloon was advanced to the occluded segment and dilated, facilitating advancement of the 8-Fr sheath (Figure 4b).
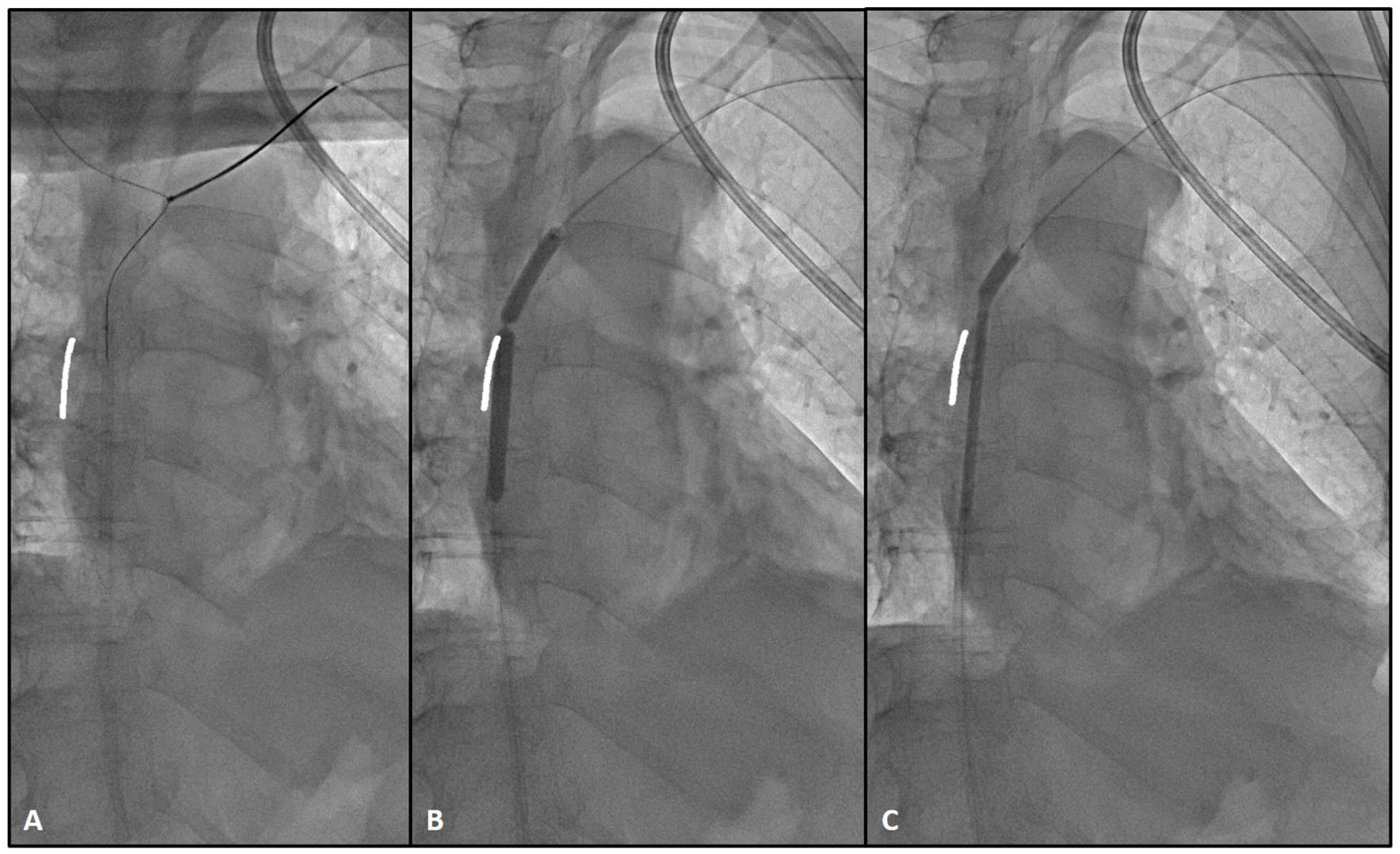
Posteroanterior view: (a) snaring of the 0.018″ guidewire into the left axillary loop graft, (b) balloon imprint at the site of occlusion, and (c) balloon-assisted tracking of the 8-Fr transfemoral sheath using the semi-compliant balloon.
A balloon-expandable stent-graft (VBX 11 × 39 mm) was deployed and post-dilated with a 14-mm balloon. The final angiogram confirmed restoration of patency with no extravasation (Figure 5). Hemostasis was achieved by manual compression at the femoral site and a single stitch of the axillary loop access. By the following morning, the patient showed complete resolution of facial and upper limb edema, along with marked improvement in the prominent superficial thoracic venous circulation.

Final control angiogram after deployment and post-dilation of the balloon-expandable stent-graft.
No new antithrombotic regimen was initiated post-procedure, in line with our institutional protocol for stent-graft use in dialysis access interventions, and the patient remained off antiplatelet therapy throughout follow-up.
At 9-month follow-up, the patient maintained primary patency of the SVC segment. Control angiography confirming this was performed during two subsequent interventions for venous anastomotic stenosis of the axillary loop graft. Dialysis adequacy remained optimal throughout the follow-up period.
Discussion
Superior vena cava (SVC) occlusion is a recognized complication in hemodialysis patients with long-standing central venous catheters. While endovascular therapy remains the preferred modality, chronic total occlusions (CTOs) may pose technical challenges, particularly when conventional wire and catheter techniques fail to traverse the fibrotic segment.1,2
In such cases, sharp recanalization tools—including radiofrequency wires, re-entry catheters, and needles—have been described.3,4 The transseptal needle, originally designed for left atrial access, offers a sharp, directional alternative that is widely available in most interventional suites. Its stiffness and maneuverability, especially when manually straightened, allow focused force to be applied at the occlusion site under fluoroscopic control.
This case was performed by vascular surgeons with experience in non-cardiac thoracic procedures and multiorgan procurement. Although this was our first case of SVC sharp recanalization using a transseptal needle, we had prior experience in ilio-caval occlusions using needle-based techniques (typically Colapinto). Since this index case, we have successfully performed two additional SVC recanalizations using the same approach.
This case highlights the feasibility of using a transseptal needle for SVC recanalization in dialysis patients. The combination of biplanar fluoroscopy and through-and-through wire technique enabled safe traversal, control, and stent delivery. The use of a balloon-expandable stent-graft provided immediate sealing and restoration of central venous flow, confirmed angiographically. Anatomically, when puncturing the SVC from a transfemoral direction, the risk of atrial or pericardial injury is substantially lower compared with trans-jugular approaches, and pneumothorax is unlikely because the trajectory does not involve pleural traversal. The primary risk is inadvertent puncture of the adjacent brachiocephalic artery, which must be carefully avoided through biplanar roadmap guidance.
Prior studies report high technical success rates for endovascular treatment of SVC syndrome, with rates approaching 98% and low complication rates. 2 However, in patients with benign, fibrotic occlusions, success depends heavily on the availability of advanced tools and operator expertise. In one of the most extensive case series of sharp recanalization, Chen et al. reported a 97% technical success rate using various sharp techniques, including Chiba needles, with major complications occurring in 4% of cases. 3
We believe the transseptal needle may be a safe and effective addition to the recanalization armamentarium when other options fail. Nonetheless, we caution that this technique should be reserved for experienced centers with adequate imaging, bailout tools, and surgical backup. It is not a first-line strategy and requires familiarity with complex venous interventions. In our institution, a full range of bailout tools is readily available, including covered stents (balloon-expandable and self-expanding) from 5 to 16 mm in diameter, as well as thoracic and abdominal endografts. Transesophageal echocardiography (TEE) was not used, as it is not typically required in this anatomical context.
Footnotes
Author contributions
Luís Loureiro: conceptualization, procedure, writing—original draft and revisions. Paulo Almeida: procedure, supervision, critical review. Davide Freitas: image acquisition, processing, interpretation. Rui Machado: supervision, methodology, manuscript review.
Data availability
All data supporting the findings of this study are included in the article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not required for this type of publication at our institution.
Informed consent
The patient provided written informed consent for the procedure and for publication of anonymized data and images.