
Abstract
Background:
The “Fistula First” paradigm has long guided vascular access selection in hemodialysis, but its applicability in the growing elderly population is increasingly questioned. Aging, frailty, and comorbidity burden significantly influence vascular access outcomes, challenging a uniform approach.
Methods:
We performed a narrative, pathophysiology- and evidence-based analysis of vascular access strategies in elderly patients on hemodialysis. We propose a patient-centered, proportionate decision-making framework integrating prognostic stratification, frailty assessment, cardiovascular risk, vascular anatomy, and patient goals of care. A novel multidimensional tool, the Proportional Access Score (PAS), was developed to operationalize this approach.
Results:
In elderly and frail patients, the clinical benefit of AVF is attenuated by higher primary failure rates, delayed maturation, and increased procedural burden, often without clear survival advantage. Conversely, CVC use, although associated with infectious and thrombotic risks, may represent a proportionate strategy in selected patients with limited life expectancy or high clinical vulnerability. Evidence suggests that vascular access type reflects patient selection rather than acting as an independent determinant of outcomes. Frailty emerges as a key modifier of risk–benefit balance, influencing access performance, complications, and quality of life. The proposed PAS enables stratification along a continuum of clinical vulnerability, supporting AVF-first strategies in robust patients, hybrid approaches in intermediate profiles, and catheter-centered strategies in highly frail individuals.
Conclusions:
Vascular access selection in elderly patients should move beyond a “one size fits all” model toward a proportionate, patient-centered strategy. Integration of frailty, prognosis, and patient preferences allows alignment of access choice with realistic clinical benefit. The Proportional Vascular Access Framework and PAS provide pragmatic tools to support individualized decision-making and may contribute to redefining standards of care in the elderly hemodialysis population.
Introduction
The “Fistula First” approach has long represented the reference paradigm in vascular access planning for hemodialysis, supported by evidence demonstrating a reduction in infectious and thrombotic complications, as well as lower morbidity and mortality rates in patients with arteriovenous fistula (AVF) compared with those using central venous catheters (CVC).1,2 Such evidence is primarily derived from observational studies conducted in relatively young and selected populations, with limited representation of elderly and frail patients, who now constitute an increasingly large proportion of the contemporary dialysis population.2,3 The concept of vascular access selection in elderly patients is not new, it remains highly clinically relevant. The increasing proportion of elderly individuals initiating hemodialysis, combined with marked heterogeneity in frailty, comorbidity burden, and life expectancy, continues to pose complex, evidence-based challenges in optimizing access strategies. The role of frailty in vascular access decision-making has been increasingly recognized in recent years. Several studies have demonstrated that frailty is associated with delayed access maturation, higher rates of primary failure, and increased procedural burden, supporting its use as a relevant factor in clinical decision-making. 4 However, despite this growing body of evidence, frailty is still inconsistently integrated into routine vascular access planning, and its application often remains descriptive rather than operational. The present work does not aim to readdress the concept of frailty per se, but to translate it into a structured and clinically applicable decision-making framework. We propose a proportional, patient-centered approach that integrates frailty with prognosis, cardiovascular vulnerability, vascular capital, and patient goals of care, operationalized through the Proportional Access Score (PAS). The progressive aging of the hemodialysis population has highlighted the clinical limitations of an indiscriminate application of the “Fistula First” strategy. In elderly AVF creation and maturation are frequently compromised by vascular aging, resulting in higher primary failure rates and prolonged maturation times, often exceeding the patient’s residual life expectancy and limiting the expected time-to-benefit.3,5,6 The traditional approach has prioritized vascular access survival as the primary outcome, overlooking aspects that are particularly relevant for elderly, such as quality of life, functional autonomy, procedural burden, and continuity of care.7,8 Reassessing the “Fistula First” concept does not devalue AVF, which remains preferred when appropriate, but supports a more flexible, proportionate approach tailored to the patient’s clinical and prognostic profile. 6 In older and frail patients, initiation of hemodialysis with CVC remains common despite adequate predialysis planning, often reflecting a mismatch between access strategy and individual prognostic horizon. Progression of frailty, functional decline, and limited life expectancy may render AVF a disproportionate option, highlighting that the issue is primarily clinical rather than technical. 9 Data from the Dialysis Outcomes and Practice Patterns Study (DOPPS) have played a pivotal role in this critical reassessment, demonstrating that the association between vascular access type and survival is strongly influenced by patient selection factors (age, comorbidity burden, and functional status) rather than by the access itself.10,11 DOPPS analyses have also highlighted marked international heterogeneity in vascular access practices, suggesting that access choice reflects differing clinical and cultural approaches to risk–benefit assessment. 12 The survival advantage attributed to AVF does not appear to be universally transferable across all dialysis populations, but rather is mediated by the clinical and functional characteristics of the treated population. 13 Significant evidence gaps remain, particularly with regard to elderly, who are still underrepresented in the studies that have informed historical recommendations.2,3,13 Clinical heterogeneity, variability in life expectancy, and the frequent coexistence of geriatric syndromes—frailty, disability, cognitive impairment, and sarcopenia—make the decision-making process particularly complex and rarely integrated into traditional access selection models.3,13 Vascular access selection in elderly should not rely solely on chronological or technical criteria. Frailty integrates biological age, functional reserve, and vulnerability to procedural stress, guiding proportionate and patient-centered access decisions.11,13 Thus, the unmet need is not the identification of risk factors, but their integration into a coherent and actionable clinical strategy.
Why “Fistula First” fails in the elderly
In elderly, vascular aging represents the main biological determinant of failure of the “Fistula First” strategy and impairs the vascular remodeling required for AVF maturation (arterial calcifications, vascular stiffness, endothelial dysfunction, and reduced venous compliance). These alterations result in reduced technical feasibility, higher rates of primary failure, and longer maturation times compared with younger patients.14,15 So many AVF are not adequately mature at the initiation of hemodialysis, necessitating corrective surgical or endovascular procedures, with a consequent increase in the risk of hospitalizations, clinical instability, and CVC use.15,16 Time-to-benefit becomes a central criterion in access selection. Survival advantage of AVF in the elderly is strongly influenced by selection bias, as patients able to receive and use AVF are generally more robust and less comorbid. 17 The presumed survival advantage of AVF in the elderly is influenced by significant selection bias: patients who are able to use an AVF are generally more robust and less comorbid, whereas more frail patients are more often initiated with CVC. 18 Thus, access type is more reflective of the patient’s overall clinical status than an independent determinant of outcomes. 19 The applicability of the “Fistula First” initiative in older adults has been examined in several studies with heterogeneous findings. A recent nationwide cohort study of Korean patients aged ⩾80 years reported better patency and lower mortality with AVF compared with grafts; however, these findings should be interpreted cautiously due to the observational design and potential selection bias, reinforcing that patient characteristics—rather than access type alone—drive outcomes. 20 Increasing evidence supports shifting from age-based to comorbidity- and frailty-driven decision-making. Age should be considered a covariate rather than an independent determinant. This supports a proportionate, patient-centered approach in which vascular access selection is guided by clinical vulnerability, vascular capital, and expected time-to-benefit. 21
Frailty as a key determinant of vascular access outcomes in hemodialysis
Frailty, defined as a state of reduced physiological reserve and increased vulnerability to procedural and hemodynamic stressors, is highly prevalent in the elderly dialysis population and represents a major determinant of mortality, hospitalizations, functional decline, and deterioration in quality of life. 22 Frailty is associated with impaired vascular adaptive responses, limiting access maturation and tolerance to interventions. 23 Intensification of salvage procedures may not only be ineffective in terms of access survival, but may further contribute to functional decline and loss of autonomy. In individuals with low frailty and preserved physiological reserve, AVF creation may offer medium- to long-term benefits. Conversely, in patients with moderate to severe frailty, the high incidence of primary failure, delayed maturation, and the need for repeated corrective interventions are associated with increased procedural burden and prolonged exposure to CVC, often in the absence of a clear prognostic benefit.24,25 Frailty is not merely an additional risk factor, but a key variable capable of redefining the risk–benefit balance of different vascular access options. In selected patients, the use of tunneled CVC may therefore represent a more clinically appropriate choice, consistent with patient-centered care goals. 26 The systematic integration of frailty assessment into decision-making processes allows for moving beyond standardized models and guiding access selection based on overall clinical consequences for the elderly patient on hemodialysis, rather than solely on access survival. 27
AVF versus CVC in the elderly: Mortality, hospitalization, quality of life
In elderly, the comparison between AVF and CVC cannot be limited to a technical assessment of patency or mechanical complications, but must be framed within a prognostic and patient-centered perspective. 28 The potential prognostic benefit of AVF tends to diminish, while the procedural burden associated with repeated surgical interventions, salvage endovascular procedures, and access-related hospitalizations increases. 2 CVC is not a neutral intervention and carries clinically relevant infectious, thrombotic, and procedural risks. The rationale for tunneled CVC use in selected elderly and frail patients is not risk minimization, but proportionality between procedural burden, prognostic horizon, and patient-centered benefit. 29 Hard outcomes must be interpreted in light of their impact on health-related quality of life (HRQoL), which is recognized as an independent predictor of mortality. Patient satisfaction with their vascular access is closely associated with overall HRQoL and its physical and mental components, influencing clinical stability, social functioning, and the perceived treatment burden. 30 Vascular access selection should systematically integrate prognosis, frailty, patient preferences, and goals of care, moving beyond a prescriptive “one size fits all” approach. 31 A substantial proportion of the evidence supporting AVF derives from non-randomized studies in which patients with AVF are systematically younger, less comorbid, with better functional status, greater vascular reserve, and longer life expectancy compared with those treated with CVC. 32 By contrast CVC is more frequently used in patients with late referral, advanced comorbidities, frailty, clinical instability, or limited prognosis, resulting in substantial confounding by indication. In this context, vascular access type often reflects the patient’s overall clinical condition rather than representing a direct causal determinant of the observed outcomes. 33 Long-term observational studies have shown that mortality in incident hemodialysis patients is more closely associated with comorbidity burden—particularly cardiovascular and systemic vascular disease—than with vascular access type. 34 In multivariable analyses, tunneled CVC is not associated with an increased risk of death compared with AVF, particularly in elderly subgroups, suggesting that vascular access serves more as a marker of overall clinical status than as an independent prognostic factor.35,36 Importantly, catheter-based strategies should not be interpreted as a general alternative to arteriovenous access, but rather as a proportionate option limited to carefully selected patients with advanced frailty, high comorbidity burden, or limited life expectancy.
Prognostic stratification and the role of KFRE in vascular access planning
In elderly with advanced chronic kidney disease, vascular access planning requires careful prognostic assessment to estimate the risk of progression to end-stage kidney disease in the short and medium term. Estimated glomerular filtration rate, while a fundamental indicator of renal function, often fails to capture the marked heterogeneity of disease trajectories typical of the geriatric and frail population. The Kidney Failure Risk Equation (KFRE) is a validated prognostic tool that provides a quantitative estimate of the risk of ESKD at 2 and 5 years. Its use has been shown to improve predialysis planning, helping to reduce unplanned dialysis initiation and the use of temporary CVC. When integrated with the assessment of frailty, comorbidities, and individual goals of care, KFRE allows alignment of the vascular access strategy with the patient’s realistic therapeutic horizon. This approach supports proportionate decision-making, avoiding unnecessary invasive procedures and promoting truly patient-centered vascular access management. 37
Longevity and complications access
In elderly on hemodialysis, vascular access longevity cannot be considered merely an index of long-term reliability, but must be interpreted in the context of the patient’s overall clinical stability. The higher primary and secondary patency of AVF compared with CVC tends to be significantly attenuated, for the reasons previously outlined, and may be achieved at the cost of a substantial clinical and procedural burden.38,39 Vascular access management for hemodialysis requires careful evaluation of the hemodynamic implications associated with AVF. A particularly relevant complication in the elderly is high-flow access syndrome. Although its incidence does not appear significantly higher than in other age groups, the systemic effects of AVF hyper flow may carry greater clinical impact in elderly patients due to the reduced cardiovascular reserve typical of advanced age. The frequent coexistence of diastolic dysfunction, structural heart disease, vascular stiffness, and reduced contractile reserve results in a diminished ability to compensate for the increased venous return and cardiac output induced by high access flows. In this setting, high-flow AVF syndrome represents a paradigmatic condition of the interaction between dialysis access and cardiovascular vulnerability, substantially contributing to the risk of high-output heart failure. A hyperfunctioning access may lead to dyspnea, reduced exercise tolerance, intradialytic instability, and increased hospitalizations for heart failure.35,40 Management of these AVF often requires repeated corrective interventions aimed at flow reduction, with a further increase in procedural and care burden. 41 CVC, although associated with well-known infectious, thrombotic, and procedure-related risks, may still provide immediate treatment continuity and represent a clinically proportionate strategy in patients with limited life expectancy, advanced comorbidities, or severe vascular capital impairment in these subgroups, the clinical priority is not the maximization of access duration, but the reduction of hospitalizations, stability of the dialysis course, and preservation of quality of life. Vascular access longevity does not necessarily translate into clinical benefit, as it may come at the cost of increased procedural burden, making clinical stability and quality of life more relevant than technical durability. 42
Patient-centered algorithm for vascular access selection in elderly hemodialysis patients
Vascular access selection in elderly patients on hemodialysis represents a complex clinical decision with well-documented prognostic, functional, and quality-of-life implications. Guidelines emphasize the need for individualized assessment, clinical practice still reflects a predominantly access-centered approach, largely anchored to the “Fistula First” paradigm. As previously highlighted, this model does not adequately reflect the heterogeneity of the elderly population, characterized by wide variability in life expectancy, frailty, cardiovascular reserve, and vascular capital. When a CVC-based strategy is clinically appropriate, the focus should shift from access type alone to functional performance. Technical aspects such as optimal tip positioning of the tunneled CVC, stability of blood flow, and minimization of recirculation become key determinants of dialysis adequacy and treatment stability. The concept of a “functional tip” highlights the need for a dynamic assessment of catheter performance: suboptimal positioning may compromise delivered dialysis dose and increase the risk of mechanical complications, even when CVC use represents a proportionate and patient-centered choice. 43 We propose a patient-centered decision-making algorithm, grounded in the principle of treatment proportionality, which introduces a practice-changing paradigm in vascular access management in elderly patients (Table 1). Although the Clinical Frailty Scale inherently integrates comorbidity, functional, and cognitive domains, we retained separate domains for cardiovascular burden and systemic vascular disease to capture their independent impact on vascular access feasibility and hemodynamic tolerance. Each domain included in the Proportional Access Score (PAS) was selected based on its direct impact on vascular access feasibility, expected time-to-benefit, and overall clinical burden. Frailty reflects physiological reserve, prognosis defines the likelihood of benefit within life expectancy, cardiovascular and vascular disease capture hemodynamic and structural constraints, vascular capital determines anatomical feasibility, clinical status reflects tolerance to procedures, and patient goals ensure alignment with individual preferences.
Proportional access score (PAS).
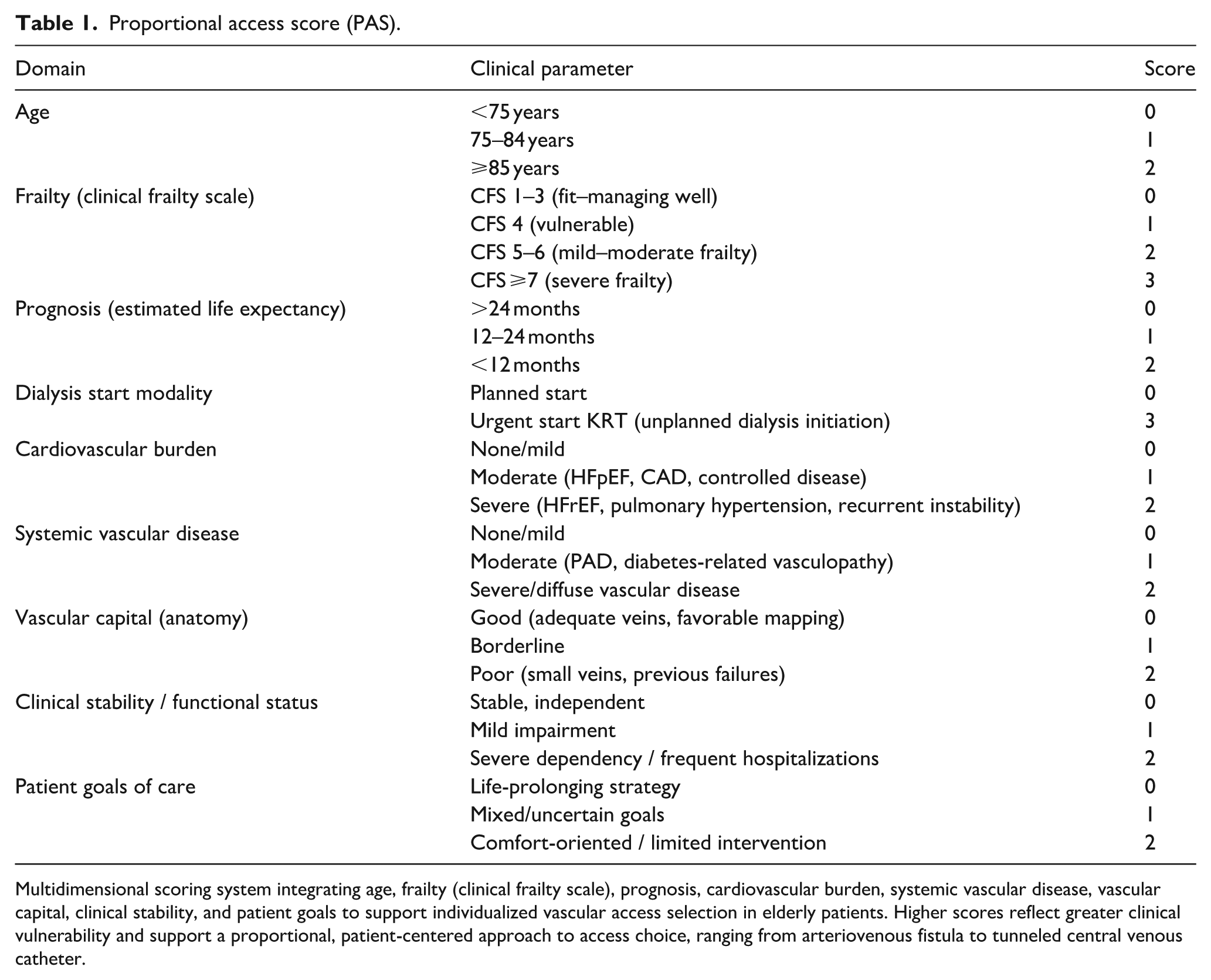
Multidimensional scoring system integrating age, frailty (clinical frailty scale), prognosis, cardiovascular burden, systemic vascular disease, vascular capital, clinical stability, and patient goals to support individualized vascular access selection in elderly patients. Higher scores reflect greater clinical vulnerability and support a proportional, patient-centered approach to access choice, ranging from arteriovenous fistula to tunneled central venous catheter.
In patients with preserved life expectancy, mild-to-moderate frailty, favorable vascular anatomy, and adequate surgical suitability, AVF remains the preferred option, provided it is incorporated into a realistic strategy for access maturation and salvage. Thus, in patients with high frailty, limited prognosis, advanced comorbidities, cardiovascular vulnerability, or severely compromised vascular capital, a proportionate CVC-based strategy may represent a clinically appropriate choice, consistent with a quality-of-life–oriented approach and stability of the dialysis course. This algorithm allows moving beyond the “one size fits all” paradigm, shifting the focus from maximizing access longevity to maximizing overall clinical benefit. By systematically integrating prognostic stratification, frailty assessment, cardiovascular risk, and patient preferences, the algorithm provides an operational framework for truly multidisciplinary management and genuinely shared decision-making. We developed the Proportional Access Score (PAS) as a pragmatic, multidimensional decision-support tool to guide vascular access selection in elderly patients. The PAS integrates key clinical domains to stratify patients according to overall clinical vulnerability and expected benefit, supporting a proportionate, patient-centered approach. Detailed score structure and interpretation are provided in Tables 1 and 2. The PAS should be considered a conceptual, expert-informed and hypothesis-generating framework, requiring prospective validation before routine clinical use.
Score interpretation for vascular access strategy based on the proportional access score (PAS).
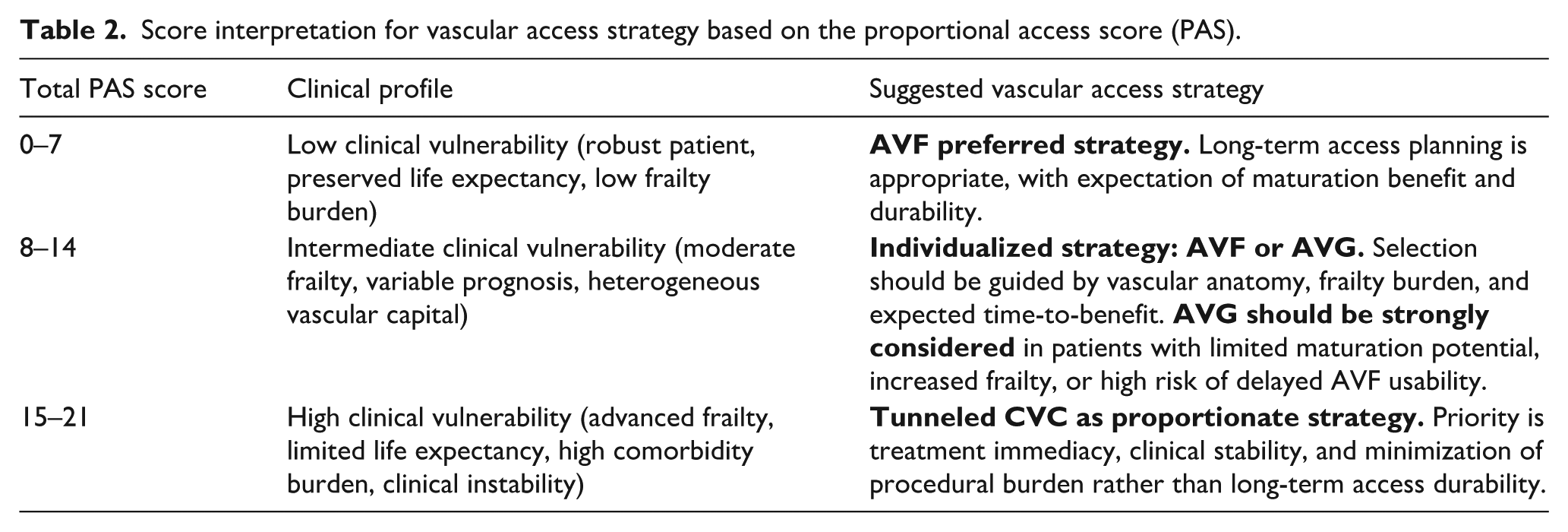
Total PAS values stratify patients into three clinical profiles to guide vascular access selection: scores 0–7 identify patients suitable for a long-term strategy with arteriovenous fistula (AVF) as the preferred option; scores 8–14 support an individualized approach with AVF or arteriovenous graft (AVG) based on vascular capital and prognosis; within intermediate PAS categories,8–14 the choice between AVF and AVG should be guided by vascular capital, frailty burden, and expected time-to-benefit, with AVG representing a clinically appropriate alternative in patients with limited maturation potential or increased vulnerability. scores 15–21 indicate high clinical vulnerability, where a proportional strategy with tunneled central venous catheter represents an appropriate option (Table 3).
Clinical application of the proportional access score (PAS) across representative patient profiles.
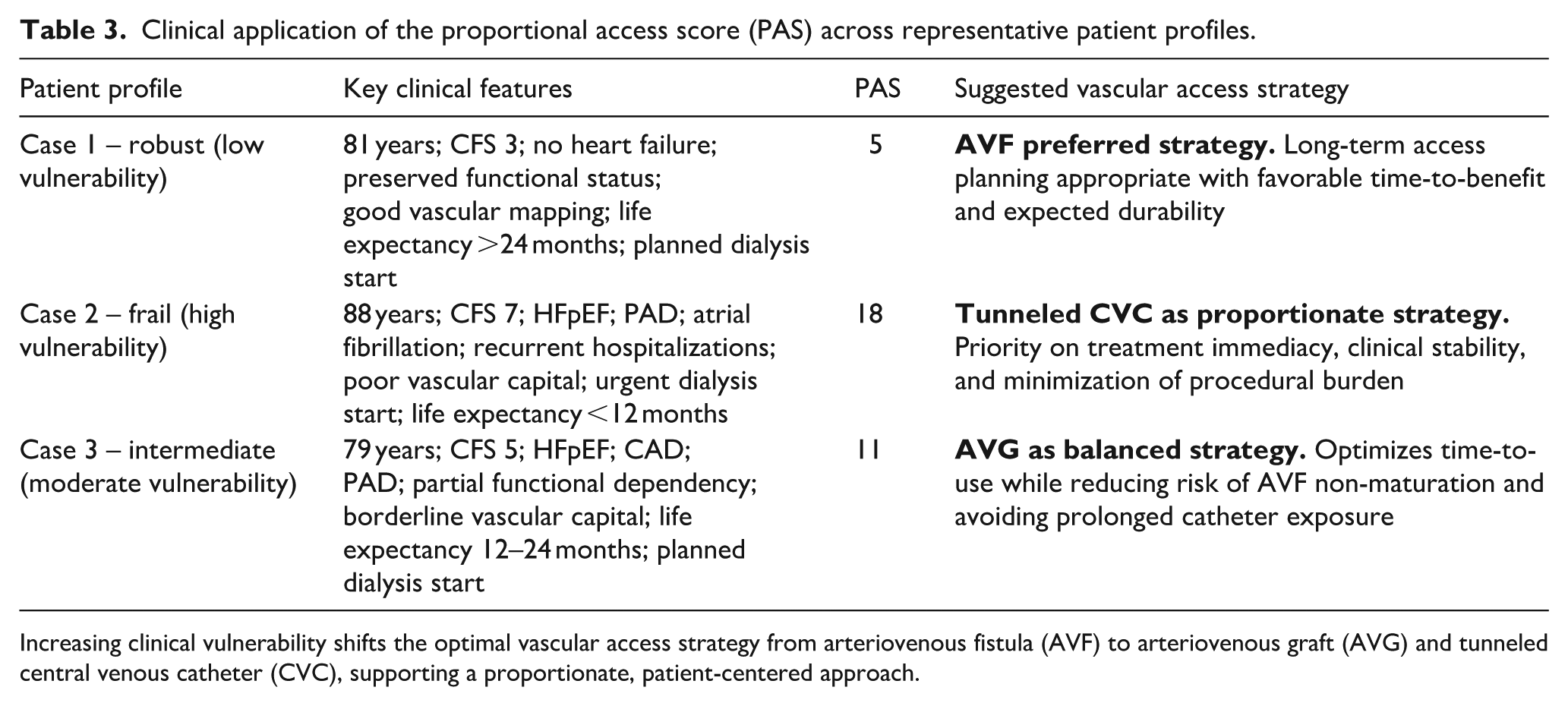
Increasing clinical vulnerability shifts the optimal vascular access strategy from arteriovenous fistula (AVF) to arteriovenous graft (AVG) and tunneled central venous catheter (CVC), supporting a proportionate, patient-centered approach.
Clinical application of the proportional access score: Illustrative cases
Case 1: An 81-year-old male with advanced chronic kidney disease (eGFR 11 ml/min/1.73 m2) was referred for planned dialysis initiation. His medical history included well-controlled hypertension and type 2 diabetes without end-organ damage. He was functionally independent (Clinical Frailty Scale (CFS) 3), with no history of heart failure or significant cardiovascular disease. Echocardiography showed preserved left ventricular function, and vascular mapping demonstrated adequate cephalic vein diameter and favorable arterial inflow. Estimated life expectancy was >24 months. The calculated Proportional Access Score (PAS) was 5 (age 1, frailty 0, prognosis 0, cardiovascular burden 0, vascular disease 1, vascular capital 0, clinical stability 0, patient goals 0, planned start 0), indicating low clinical vulnerability. An autologous AVF was selected as the preferred access, in line with a long-term strategy and an expected favorable maturation and usability profile. Case 2: An 88-year-old female with advanced chronic kidney disease (eGFR 9 ml/min/1.73 m2) presented with unplanned dialysis initiation due to uremic symptoms and fluid overload. Her medical history included heart failure with preserved ejection fraction (HFpEF), atrial fibrillation on anticoagulation, peripheral arterial disease (PAD), and insulin-dependent diabetes complicated by neuropathy. She had severe frailty (CFS 7), recurrent hospitalizations, and partial dependency in activities of daily living. Vascular assessment revealed poor vascular capital, with small-caliber veins and diffuse arterial calcifications. Estimated life expectancy was <12 months. The calculated PAS was 18 (age 2, frailty 3, prognosis 2, urgent start 3, cardiovascular burden 2, vascular disease 2, vascular capital 2, clinical instability 1, patient goals 1), indicating high clinical vulnerability. In this setting, a tunneled CVC was considered a proportionate strategy, prioritizing treatment immediacy, clinical stability, and minimization of procedural burden over long-term access durability. Case 3: A 79-year-old male with advanced chronic kidney disease (eGFR 12 ml/min/1.73 m2) was referred for vascular access planning. His medical history included ischemic heart disease with prior percutaneous coronary intervention, heart failure with preserved ejection fraction (HFpEF), and type 2 diabetes with peripheral arterial disease (PAD). He was partially dependent in instrumental activities of daily living and classified as moderately frail (Clinical Frailty Scale (CFS) 5). Vascular mapping revealed borderline vascular capital, with small-caliber superficial veins and suboptimal venous distensibility, while arterial inflow was preserved. Dialysis initiation was expected within 3–6 months, and estimated life expectancy was approximately 12–24 months. The calculated Proportional Access Score (PAS) was 11 (age 1, frailty 2, prognosis 1, cardiovascular burden 1, vascular disease 1, vascular capital 1, clinical stability 2, patient goals 1, planned start 0), indicating intermediate clinical vulnerability. In this setting, an arteriovenous graft (AVG) was considered the most appropriate strategy, balancing the need for timely usability with a reduced risk of primary failure and delayed maturation compared with AVF, while avoiding the long-term complications associated with catheter-based access.
Notably, the intermediate-risk profile represents the most clinically challenging scenario, in which the PAS may provide the greatest added value, guiding individualized decisions.
Conclusion
The benefit of vascular access is not universal, but depends substantially on the individual patient’s biological, functional, and prognostic profile. The proportionate, patient-centered decision algorithm proposed here provides an operational framework to translate guideline recommendations into real-world clinical practice, systematically integrating prognosis, frailty, cardiovascular vulnerability, vascular capital, and goals of care. In line with the evolution of KDOQI guidelines and the concept of the ESKD Life-Plan, this approach reframes vascular access decision-making from a strategy focused on maximizing access longevity to one centered on overall clinical benefit for the patient at a specific point in their disease trajectory. The structured integration of geriatric assessment into the decision-making process supports truly shared decision-making, reduces disproportionate procedural escalation, and promotes access strategies aligned with clinical stability and quality of life in more frail patients. Within this perspective, the Proportional Vascular Access Framework and the Proportional Access Score (PAS) represent pragmatic tools to move beyond binary models and support access selection guided by treatment proportionality. The integration of vascular access nephrology and clinical geriatrics thus emerges as a necessary evolutionary direction for the development of a new standard of care—outcome-oriented and genuinely patient-centered—in the growing population of elderly patients undergoing hemodialysis. Accordingly, the present framework should not be interpreted as a shift from “fistula first” to “catheter first,” but rather as a move toward proportionate access selection based on individualized clinical benefit. The PAS should therefore be considered a conceptual and hypothesis-generating framework, intended to support clinical reasoning rather than replace it, pending prospective validation. Future directions include the development of a digital decision-support tool, such as a mobile application, to facilitate bedside implementation of the PAS. This may enhance clinical usability and promote standardized, patient-centered vascular access decision-making, pending prospective validation.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.