
Abstract
Background:
This study aims to assess the efficacy and safety of a staged endovascular management for non-maturing arteriovenous fistulas (AVFs) and identify prognostic factors associated with patency.
Methods:
Between September 2016 and June 2025, 67 patients (age: 62.8 ± 10.8 years; male: 67.2%) underwent staged endovascular management according to a standardized institutional protocol. This strategy prioritizes correction of underlying stenotic lesions, even when the severity of stenosis is mild. Embolization of collateral veins was performed in cases of persistent maturation failure.
Results:
Technical and clinical success rates were 97.4% (76/78) and 83.6% (56/67), respectively, with a complication rate of 5.1% (4/78). Initial PTA achieved clinical success in 54 of 67 patients (80.6%). Among 11 patients with persistent maturation failure, four underwent collateral embolization, resulting in clinical success in 2. Postintervention primary and assisted primary patency rates at 3, 6, and 12 months were 85.7%, 81.7%, and 73.1%, and 98.2%, 96.3%, and 94.2%, respectively. Diabetes mellitus (HR, 5.43; 95% CI, 1.23–23.96; p = 0.026) and thrombotic occlusion (HR, 7.05; 95% CI, 2.62–18.93; p < 0.001) were significant predictors of reduced primary patency. The reintervention rate was 0.45 events/access-year. Outcomes did not differ significantly according to lesion characteristics.
Conclusions:
A staged endovascular approach offers a safe and effective strategy for managing non-maturing AVFs, enabling tailored clinical decision-making with favorable patency outcomes. The identification of diabetes mellitus and thrombotic occlusion as predictors of primary patency enables more precise risk stratification.
Keywords
Introduction
Non-maturing arteriovenous fistulas (AVFs) remain a major challenge in hemodialysis access.1,2 Percutaneous transluminal angioplasty (PTA) is widely accepted as the cornerstone of endovascular treatment for non-maturing AVFs. 3 However, considerable variability persists in treatment strategies, particularly regarding the management of coexisting collateral veins and low-grade stenotic lesions. 4 In many clinical settings, the presence of collateral veins is interpreted as an indication for embolization, whereas angiographically mild stenoses are often disregarded because they do not meet conventional thresholds for significant narrowing. In standard clinical practice, this threshold is typically defined as a luminal reduction of ⩾50%.5–7
In non-maturing AVFs, overall flow reserve is limited, and adaptive vascular remodeling has failed to occur, rendering the circuit highly sensitive to even modest increases in resistance. Under these conditions, angiographically mild stenoses may exert a disproportionate functional impact, while collateral veins may represent a compensatory response to upstream resistance rather than an isolated cause of non-maturing AVF. 8 Consequently, strategies that focus primarily on collateral embolization without first addressing potentially flow-limiting stenotic lesions may fail to correct the fundamental hemodynamic disturbance.4,6,9
To overcome these issues, our institution has implemented a standardized protocol for staged endovascular management since September 2016. This protocol prioritizes angioplasty as the initial intervention—even when angiographically mild—and interval reassessment for persistent maturation failure, defined as failure to achieve maturation despite initial endovascular intervention. Embolization is reserved for cases with persistent maturation failure after correction of stenosis. This enables clinicians to more accurately identify cases where collateral vein embolization is truly warranted.
The purpose of this study was to evaluate the efficacy and safety of this staged endovascular management for non-maturing AVFs and to identify prognostic factors associated with patency.
Materials and methods
The Institutional Review Board of a tertiary care hospital approved this retrospective study and waived written informed consent for using clinical and imaging data (IRB no. 2025-09-036). Written informed consent for interventional procedures was obtained from all patients.
Staged endovascular management protocol
At our institution, routine Doppler ultrasound was recommended 6 weeks after surgical AVF creation to assess fistula maturation.3,10,11 This evaluation was part of a standardized postoperative surveillance and staged endovascular management protocol (Figure 1). Maturation status was determined using the University of Alabama at Birmingham (UAB) criteria (vessel diameter ⩾4 mm and blood flow ⩾500 mL/min).12–14 AVFs that failed to meet these criteria were considered non-maturing and were referred for endovascular salvage.
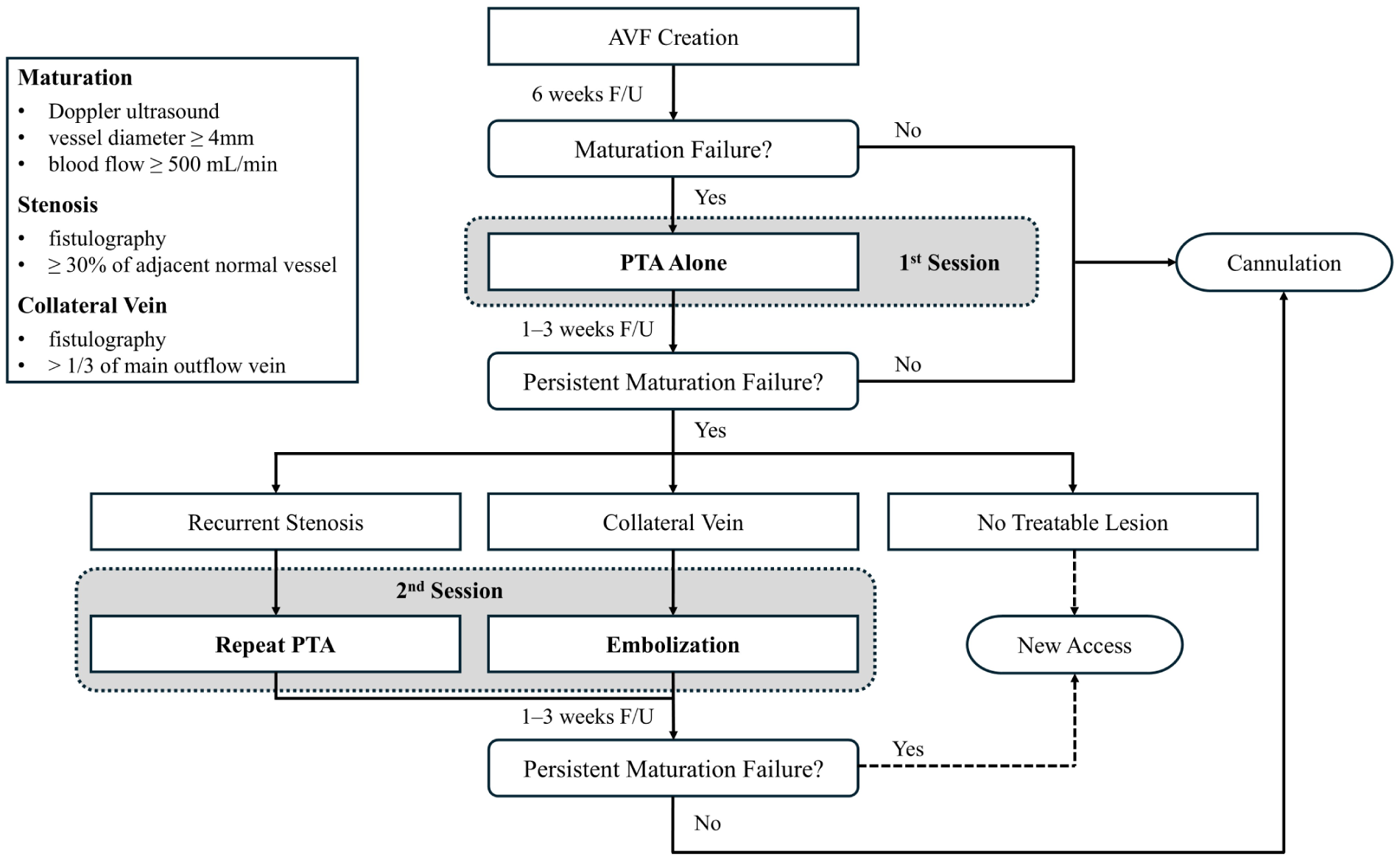
Flowchart illustrating the staged endovascular approach.
During the initial session, fistulography was performed to assess the presence of underlying stenotic lesions, followed by PTA as the primary intervention. While a stenosis of ⩾50% is conventionally regarded as significant, our predefined protocol targeted lesions with ⩾30% narrowing in the setting of non-maturing AVFs, reflecting a stenosis-first strategy aimed at avoiding under-treatment of potentially contributory lesions.3,15 A follow-up Doppler ultrasound was obtained 1–3 weeks after the initial PTA to evaluate for persistent maturation failure.
For patients with persistent maturation failure, repeat fistulography was performed to assess for recurrent stenosis or the presence of collateral veins. Recurrent stenoses were treated with repeat PTA. Collateral veins, defined as veins with a diameter exceeding one-third of the primary outflow vein, were embolized selectively when present (Figure 2). If neither recurrent stenosis nor collateral veins were identified, creation of a new dialysis access was considered. After the second intervention, maturation status was reassessed within an additional 1–3 weeks.
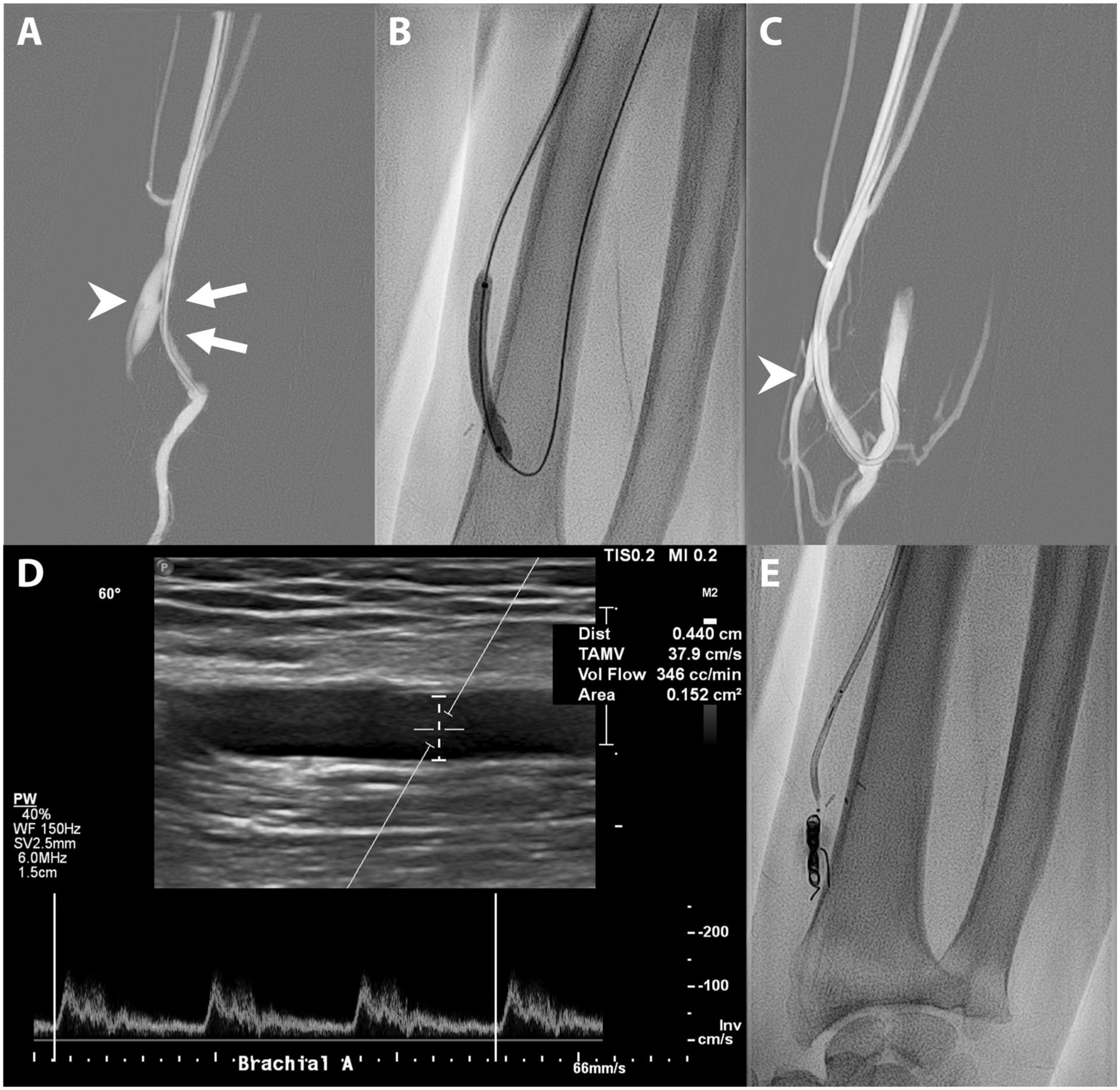
Staged endovascular management in a 61-year-old man presenting with a non-maturing radiocephalic arteriovenous fistula: (a) the initial fistulogram reveals moderate stenosis at the inflow segment (arrows) along with a collateral vein (arrowhead), (b) a fluoroscopic spot image during the first intervention session demonstrates an angioplasty balloon positioned at the juxta-anastomotic site, (c, d) follow-up fistulogram and Doppler ultrasound show residual collateral vein flow (arrowhead) and an access flow volume of 346 mL/min, indicating persistent maturation failure despite resolution of the stenosis, and (e) during the second session, a fluoroscopic spot image shows dense coil packing within the collateral vein.
Study design
Based on a retrospective review of electronic medical records (EMR), 712 AVFs were surgically created at our institution between September 2016 and June 2025. Of these, 665 completed scheduled postoperative Doppler ultrasound evaluation. Among them, 67 AVFs met the UAB criteria for non-maturation and were referred for staged endovascular salvage. Each of these AVFs belonged to a different patient; thus, 67 consecutive patients (mean age, 62.8 ± 10.8 years; 67.2% male) were included in this study.
Clinical data were collected from EMR, including demographic characteristics, comorbidities, preoperative dialysis status, fistula type, and fistula side. Three specific time intervals were documented: (1) from AVF creation to ultrasound evaluation, (2) from AVF creation to the first intervention, and (3) from the first intervention to cannulation. Follow-up data included dates of intervention, access abandonment, and last clinical follow-up.
Procedure details
All procedures were performed by one of two board-certified interventional radiologists with 12 and 16 years of experience, respectively. The puncture site was chosen for either an antegrade or retrograde approach through the venous limb of the fistula. If a suitable access site could not be identified, alternative routes were used—radial artery access for forearm AVFs and transjugular venous access for upper arm AVFs. In cases involving thrombotic occlusion, mechanical thrombectomy was performed using a Desilets–Hoffman sheath (Cook Medical, Bloomington, IN, USA) before proceeding with angioplasty. Following thrombus removal, the underlying stenotic lesion was identified and treated accordingly.
Stenotic lesions were traversed using a 0.035-inch guidewire (Terumo, Tokyo, Japan), followed by angioplasty using a balloon catheter (Mustang; Boston Scientific). If residual stenosis persisted after standard balloon angioplasty, high-pressure balloons (Conquest; Bard Peripheral Vascular, Tempe, AZ, USA) were applied. When a small vessel caliber or marked angulation prevented passage of a 0.035-inch high-pressure balloon, a 0.018-inch cutting balloon (Peripheral Cutting Balloon; Boston Scientific) was utilized after exchanging the guidewire with a 0.018-inch system (V18; Boston Scientific, Marlborough, MA, USA).
For embolization, the vein with the largest diameter among collateral veins was selected as the treatment target. The target vein was selectively catheterized using a 1.9-Fr microcatheter (Carnelian SI; Tokai Medical Products, Kasugai, Japan) and a 0.016-inch guidewire (ASAHI Meister; Asahi Intecc, Nagoya, Japan). Embolization was then conducted using either microcoils (Concerto; Medtronic, Sunnyvale, CA, USA) or a mixture of N-butyl cyanoacrylate and Lipiodol, depending on the vein’s size, flow characteristics, and anatomical features.
Image analysis
All available angiographic images were retrospectively reviewed by an independent board-certified interventional radiologist, who was blinded to the clinical outcomes. Measurements were obtained manually using dedicated PACS software.
The percentage of stenosis was calculated by comparing the minimal luminal diameter at the stenotic segment with that of the adjacent normal or upstream reference vessel. The severity of stenosis was then categorized as mild (30%–50%), moderate (50%–70%), or severe (>70%). The location of stenosis was categorized as inflow or outflow. The inflow segment referred to the arterial side of the access circuit, including the juxta-anastomotic region within 5 cm of the anastomosis. The outflow segment was defined as the venous limb distal to the juxta-anastomotic region and extending centrally to the right atrium. Lesions longer than 3 cm were classified as long-segment involvement. In cases with multiple lesions, the location and severity of the lesions were determined based on the highest-grade stenosis.
The presence of collateral veins in the juxta-anastomotic region and future cannulation zone was evaluated using the initial fistulogram. To maintain consistency with the study protocol, only collateral veins with a diameter exceeding one-third of the primary outflow vein were included in the analysis. Thrombotic occlusion was assessed based on a combination of findings from initial ultrasound and fistulography, defined as a segmental obstruction of the access circuit without contrast opacification. Lesions with partial obstruction, such as the presence of mural thrombus with preserved luminal flow, were not classified as thrombotic occlusion.
Endpoints
The primary endpoint was clinical success, defined as successful maturation enabling two-needle cannulation for at least three consecutive hemodialysis sessions. Secondary endpoints consisted of technical success, complications, postintervention primary and assisted primary patency, and reintervention burden. Technical success after angioplasty was defined as residual stenosis of <30% on the completion fistulogram. For cases undergoing embolization, complete occlusion of the targeted collateral vein was additionally required. Complications were classified as major or minor according to guidelines from the Society of Interventional Radiology Standards of Practice Committee.15,16
Postintervention primary patency was defined as the interval from the first successful cannulation to the first reintervention or access thrombosis. Assisted primary patency was defined as the interval from the first successful cannulation to access thrombosis or access abandonment, with interventions allowed to maintain patency during this interval.17,18 Reintervention burden was assessed as the proportion of patients requiring reintervention, the number of reintervention events, and the rate of reintervention per access-year of follow-up after successful cannulation.
Statistical analysis
For descriptive statistics, continuous variables were expressed as mean ± standard deviation, while categorical variables were presented as counts and percentages. Categorical variables were compared using Fisher’s exact test. Patency rates were estimated using the Kaplan–Meier method, with comparisons performed using the log-rank test. Patients who died with a functioning access, underwent renal transplantation with a functioning access, or retained a functioning access at the time of last follow-up were censored.
Cox proportional hazards regression analysis was performed to identify predictors of patency. Variables included in the multivariable model were selected based on clinical relevance and univariable analysis. Clinical outcomes were evaluated based on the severity of stenosis. A p < 0.05 was considered statistically significant. All statistical analyses were performed using R version 3.6.3 software (Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline characteristics
Baseline patient characteristics are summarized in Table 1. Hypertension (91.0%) and diabetes mellitus (DM, 74.6%) were the most frequent comorbidities. The majority of patients (71.6%) were already on hemodialysis, whereas 25.4% were pre-dialysis and 3.0% were on peritoneal dialysis. Most fistulas were radial–cephalic (59.7%), followed by brachial–cephalic (37.3%) and brachial–basilic (3.0%), and were predominantly located on the left side (85.1%). The mean interval from AVF creation to ultrasound evaluation was 47.9 ± 14.0 days, and the mean interval from AVF creation to the first intervention was 55.6 ± 16.8 days. Following the first intervention, the mean time to successful cannulation was 27.0 ± 26.0 days.
Patient characteristics.
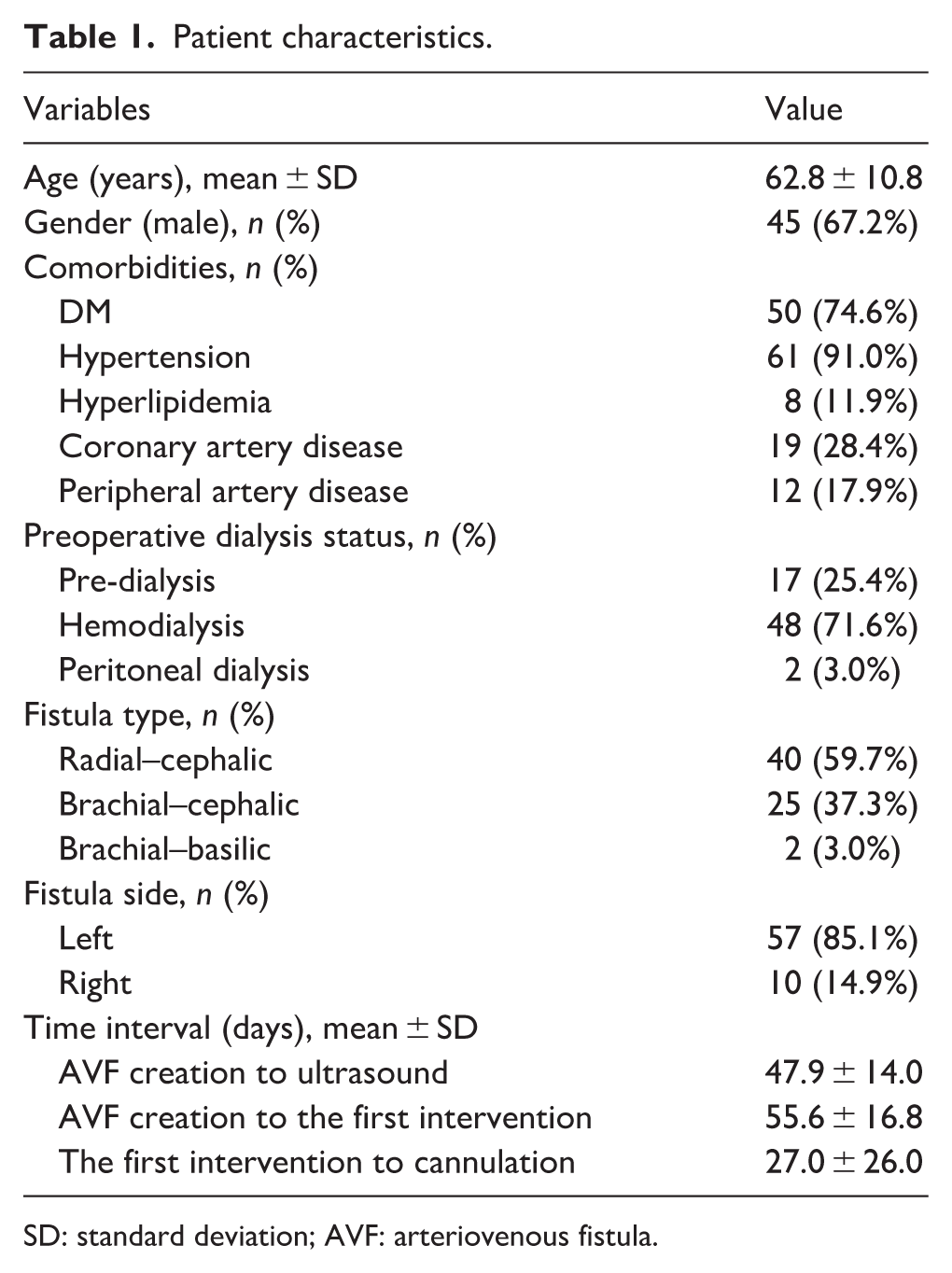
SD: standard deviation; AVF: arteriovenous fistula.
Lesion characteristics
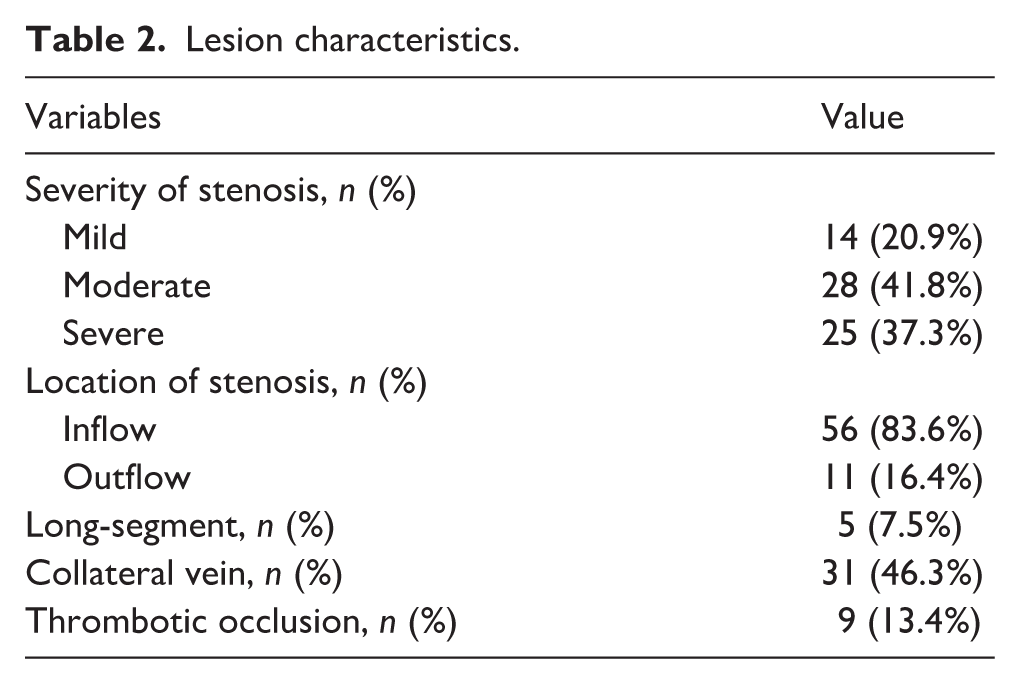
Lesion characteristics are summarized in Table 2. Initial fistulograms demonstrated at least one stenotic lesion in all patients. Specifically, the severity of stenosis was mild in 20.9%, moderate in 41.8%, and severe in 37.3% of cases. The majority of lesions were located in the inflow segment (83.6%), followed by the outflow segment (16.4%). Long-segment involvement was observed in 7.5% of patients. Additionally, collateral veins were identified in 46.3% of patients, and thrombotic occlusion was observed in 13.4% of patients.
Lesion characteristics.
Procedural and clinical outcomes
The overall technical success rate was 97.4% (76/78 procedures), and the overall clinical success rate was 83.6% (56/67 patients). The complication rate was 5.1% (4/78 procedures). The single major complication resulted from an uncontrolled vessel rupture after cutting-balloon angioplasty, requiring surgical repair. Three minor complications, all vessel ruptures, were successfully managed with balloon tamponade. At the initial PTA, technical and clinical success rates were 97.0% (65/67 procedures) and 80.6% (54/67 patients), respectively. Two technical failures were due to residual stenosis. Thirty-one patients (46.3%) had collateral veins identified on the fistulogram; however, embolization was not performed during the initial session.
Among 11 patients with persistent maturation failure, six patients underwent a second intervention. At the second session, technical success was achieved in all six procedures, without complications, and clinical success in two of six patients. Four patients with collateral veins underwent embolization, and two patients who had recurrent stenosis but no collateral veins underwent repeat PTA. Embolization resulted in clinical success in two of four patients, whereas repeat PTA failed to achieve maturation in either case. The remaining five patients had no identifiable treatable lesion (i.e. neither recurrent stenosis nor collateral veins) on repeat fistulography and were therefore referred for new access creation according to our predefined protocol.
Patency and reintervention burden
Postintervention primary patency rates at 3, 6, and 12 months were 85.7%, 81.7%, and 73.1%, respectively, while assisted primary patency rates were 98.2%, 96.3%, and 94.2%. Figure 3 shows the survival curves for the postintervention primary and assisted primary patency of the accesses. In multivariable Cox regression analysis, DM (HR, 5.43; 95% CI, 1.23–23.96; p = 0.026) and thrombotic occlusion (HR, 7.05; 95% CI, 2.62–18.93; p < 0.001) were independently associated with reduced primary patency (Table 3). No other demographic, anatomical, or procedural variables showed a significant association with primary patency.
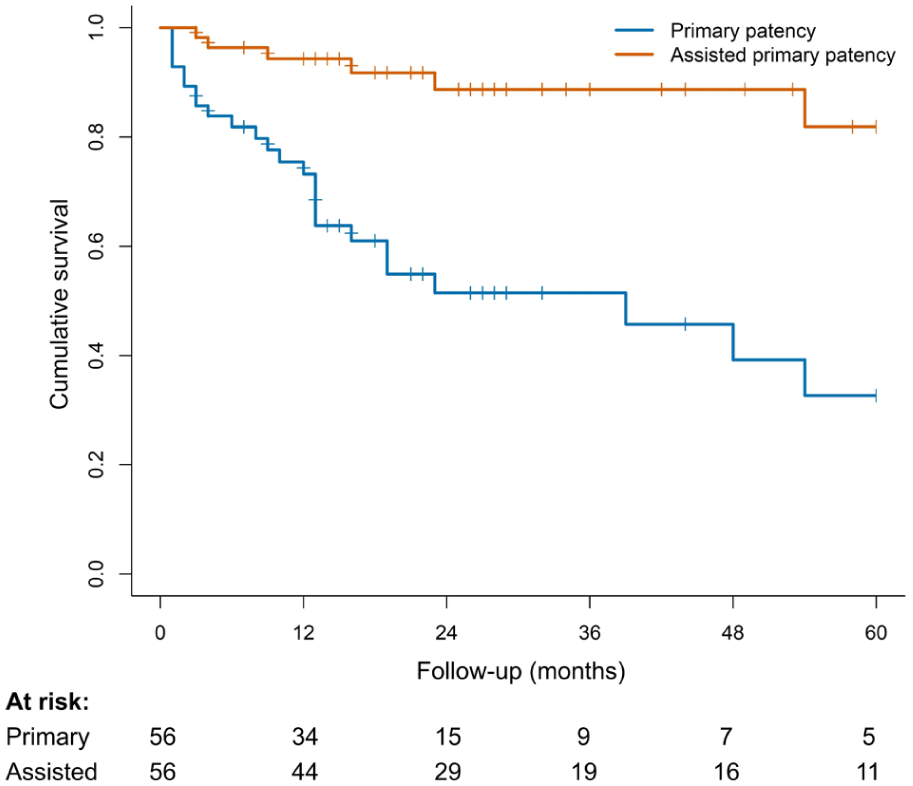
Kaplan–Meier curves of postintervention primary and assisted primary patency.
Prognostic factors for postintervention primary patency.
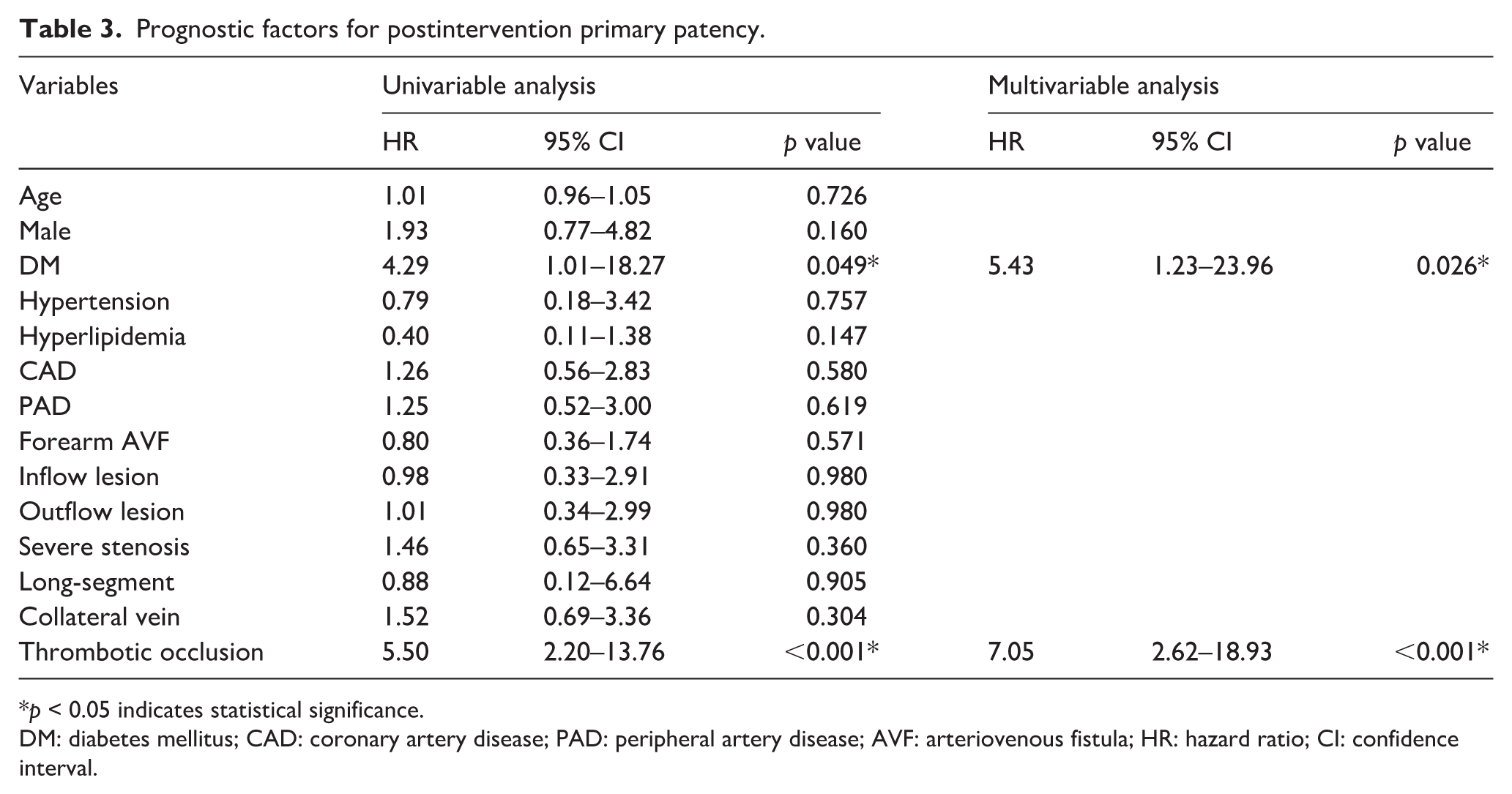
*p < 0.05 indicates statistical significance.
DM: diabetes mellitus; CAD: coronary artery disease; PAD: peripheral artery disease; AVF: arteriovenous fistula; HR: hazard ratio; CI: confidence interval.
Among the 56 patients who achieved clinical success, the median post-cannulation follow-up duration was 23.3 months. During this period, 61 reintervention events were recorded in the maturation cohort. Reintervention was required in 26 of 56 patients (46.4%), corresponding to a mean of 1.09 reintervention events/patient. Based on 135.2 cumulative access-years of follow-up after cannulation, the rate of reintervention was 0.45/access-year. The median time from successful cannulation to the first reintervention was 6.4 months.
Comparison of outcomes according to lesion characteristics
Clinical outcomes were compared according to stenosis severity by stratifying patients into two categories: mild and moderate-to-severe. Collateral veins were identified in eight of 14 patients (57.1%) with mild stenosis and in 23 of 53 patients (43.4%) with moderate-to-severe stenosis. Initial PTA achieved clinical success in 10/14 (71.4%) patients with mild stenosis and 44/53 (83.0%) patients with moderate-to-severe stenosis, with two additional successes after a second session in the latter group. Overall clinical success rates were 71.4% (10/14) and 86.8% (46/53), respectively (p = 0.223). All complications occurred in the moderate-to-severe stenosis group (p > 0.99).
No statistically significant differences were observed in postintervention primary patency (p = 0.848) or assisted primary patency (p = 0.794), based on Kaplan–Meier analysis over the entire follow-up period. The reintervention rate was 0.30 and 0.50/access-year in the mild and moderate-to-severe groups, respectively. No significant differences in clinical success or patency outcomes were observed according to AVF location (forearm vs upper arm; all p > 0.05). The reintervention rate was 0.33 and 0.70/access-year in forearm and upper arm AVFs, respectively.
Discussion
This study demonstrates that a staged endovascular approach is a safe and effective strategy for managing non-maturing AVFs. Most patients achieved successful maturation following PTA alone, with additional interventions required in a limited subset of cases. Although postintervention primary patency declined over time, assisted primary patency remained well preserved, suggesting that access function could be durably maintained with reintervention after successful maturation. Notably, DM and thrombotic occlusion emerged as significant predictors of reduced primary patency.
Previous studies with endovascular salvage of non-maturing AVFs have reported technical success rates of 88%–98% and maturation rates of 43%–97%.19,20 Despite the limitations of direct comparisons between studies, the outcomes achieved with our staged endovascular approach remain favorable. This is particularly noteworthy given that nearly 60% of fistulas in our cohort were radiocephalic, which are considered more challenging to salvage due to smaller vessel caliber and less robust flow.3,21 In addition, the definition of clinical success used in this study was more stringent than in some prior series, where a single successful cannulation was sufficient to classify an AVF as mature.9,19
A key concept underlying our staged strategy is the prioritization of stenotic lesion correction before considering collateral vein embolization. Although collateral veins are commonly encountered, establishing uniform thresholds for intervention is particularly challenging when only mild stenosis is present. 8 The staged protocol applied in this study offers a potential solution to this problem by separating angioplasty and embolization into distinct sessions, thereby allowing the need for embolization to be reassessed based on subsequent maturation. Notably, this strategy differs from that of Nauta et al., who performed embolization of residual collateral veins during the same session following angioplasty. 1
In many clinical practices, collateral vein embolization is frequently performed, with reported rates of ~20%–60% in non-maturing AVFs.1,2,9 In our cohort, collateral veins were identified in 31 patients at baseline; however, only four patients ultimately required embolization after interval reassessment. This observation suggests that the angiographic presence of collateral veins alone may not invariably warrant immediate embolization. In this context, routine embolization of collateral veins should be applied cautiously, given its potential impact on resource utilization, cost, and exposure to risks associated with the procedure (e.g. coil migration and occlusion of venous pathways that may compromise future access options).1,4 Nevertheless, given the limited number of embolizations performed, these findings should be interpreted cautiously and considered hypothesis-generating.
The use of a ⩾30% angiographic threshold may raise concern regarding angiographic measurement variability and potential overtreatment. Visual estimation of stenosis severity represents a continuous spectrum rather than a discrete categorical entity. This limitation is particularly relevant when lower treatment thresholds are applied. However, the treatment strategy in this study was applied in the specific context of clinically evident non-maturing AVFs. Therefore, the 30% threshold was not intended to serve as a rigid anatomic cutoff, but rather to identify potentially flow-limiting lesions.
Importantly, stratified analysis demonstrated no significant differences in clinical success or postintervention patency between mild and moderate-to-severe stenosis groups. The single major vessel rupture occurred in a patient with moderate-to-severe stenosis during cutting balloon angioplasty, and no excess complication signal was observed in the mild stenosis subgroup. These findings do not indicate a safety concern specifically attributable to the lower treatment threshold in this cohort. In this context, mild stenosis alone may not preclude consideration of endovascular salvage in non-maturing AVFs.
Beyond procedural strategy, the findings of this study have significant practical implications for managing non-maturing AVFs. Our protocol emphasized early identification of non-maturing AVFs through routine postoperative ultrasound, enabling timely intervention before irreversible access failure occurred.9,22 Once successful maturation was achieved, long-term patency in our cohort approximated that reported for mature AVFs, suggesting that the principal vulnerability of immature fistulas lies in the early post-creation period.10,23 These findings support the concept of timely endovascular salvage as a key opportunity to convert non-maturing fistulas into durable dialysis access.
Our study also provides insight into the durability of access maintenance following successful maturation. In our cohort, fewer than half of the matured AVF required at least one reintervention, with an overall rate of 0.45 reintervention events/access-year. Prior studies of endovascular salvage for non-maturing AVFs have reported that maintaining long-term access function often requires repeated procedures, with reported rates ranging from 0.37 to 1.7 reinterventions/access-year.24,25 While direct numeric comparisons should be interpreted cautiously given differences in study design and patient populations, the observed reintervention burden indicates that favorable assisted primary patency was maintained without an excessive need for repeat procedures.
Thrombotic occlusion and DM emerged as independent predictors of reduced primary patency. These results align with previous studies, which have shown that access thrombosis is associated with decreased patency.26–28 Thrombus formation and subsequent removal may aggravate endothelial injury and inflammatory responses, thereby promoting neointimal hyperplasia and recurrent stenosis. 29 DM has been widely recognized as a critical systemic risk factor for access failure, influencing both maturation and long-term patency. Proposed mechanisms include endothelial dysfunction, enhanced neointimal hyperplasia, impaired vascular remodeling, and altered inflammatory responses.30–32
The current study has several limitations. It was a retrospective, single-center analysis with a relatively small sample size, potentially limiting generalizability. The absence of randomization and a control group restricts causal inference, and the limited number of events constrained the multivariable analysis, precluding inclusion of several potentially relevant clinical variables (e.g. body weight, antiplatelet, and central venous catheter). Selection bias may also have influenced the favorable outcomes, as a rigorous preoperative evaluation protocol was applied. In addition, catheter-related outcomes were not systematically assessed, although these may better reflect patient-centered benefit beyond patency alone.
Conclusion
A staged endovascular approach offers a safe and effective strategy for managing non-maturing AVFs. By prioritizing PTA as the first-line intervention and reserving embolization for persistent maturation failure, this protocol facilitates tailored clinical decision-making while maintaining favorable patency outcomes. The identification of DM and thrombotic occlusion as predictors of primary patency enables more precise risk stratification.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Soonchunhyang University Research Fund. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Ethical approval
The Institutional Review Board of a tertiary care hospital approved this retrospective study and waived written informed consent for using clinical and imaging data (Soonchunhyang University Cheonan Hospital, IRB #2025-09-036).
Informed consent
Written informed consent for interventional procedures was obtained from all patients.