
Abstract
Purpose
In patients with end-stage renal disease, arteriovenous fistulas (AVFs) are the access of choice for hemodialysis but are often complicated by stenosis. We present single-center experience of 78 ultrasound-guided angioplasty procedures for treating peripheral stenoses of AVFs.
Methods
Between January 2013 and November 2015, 78 angioplasties were performed under ultrasound guidance in 53 patients with end-stage renal disease who were referred from dialysis centers with low flow rate, difficult cannulation, increased cannulation site bleeding, immature or thrombosed AVF. Angioplasties were carried out in the presence of a structural lesion in the AVF resulting in at least 50% reduction in vein diameter with a blood flow of <250 mL/min or a peak systolic velocity >300 cm/s. Clinical success, anatomical success and post-intervention primary and secondary patency rates at 6, 12, 18 and 24 months were studied.
Results
In 49/53 patients (92.4%), 74 angioplasty procedures were successfully performed, whereas 4/53 patients (7.6%) had primary failure. A total of 35/49 patients (71.4%) underwent single angioplasty procedure whereas 14/49 patients (28.6%) underwent multiple angioplasty procedures. Post-intervention primary patency rates at 6, 12, 18 and 24 months were 78.6%, 60.2%, 53.8% and 48.9%, respectively. Post-intervention secondary patency rates at 6, 12, 18 and 24 months were 100%, 100%, 95.4% and 89%, respectively. Clinical success and anatomical success was 94.8% and 89.7%, respectively.
Conclusions
Ultrasound-guided angioplasty is an effective method with good long-term outcomes in selected dialysis patients with peripheral stenosis of AVF.
Introduction
In patients with end-stage renal disease, native arteriovenous fistulas (AVFs) are the access of choice for hemodialysis (1). However, AVFs are often complicated by stenosis that might delay maturation, limit the efficacy of dialysis or result in thrombosis (1, 2). The functioning of these stenosed and failing AVFs can be improved with the use of endovascular procedures like percutaneous balloon angioplasty or balloon-assisted maturation (1, 2). Although the majority of balloon angioplasties are carried out under fluoroscopic guidance, use of fluoroscopy is limited by cost of equipment and limited availability. It is also associated with radiation hazard to both patients and physicians as the patients often need multiple interventions. There might be need to avoid use of intravenous contrast in some patients having dysfunctional AVF with residual renal function while awaiting dialysis. All these problems can be overcome by use of ultrasound guidance for angioplasty as fistula veins are superficial and can easily be visualized by use of ultrasound. There is limited data in literature regarding long-term results after ultrasound-guided angioplasty of AVFs. We present our single-center experience of seventy-eight ultrasound-guided angioplasty procedures for treating peripheral stenosis of native AVFs.
Methods
Patient selection and pre-treatment evaluation
Between January 2013 and November 2015, 78 angioplasties were carried out under ultrasound guidance in 53 patients with end-stage renal disease on regular maintenance hemodialysis. Patients were referred from dialysis centers with access dysfunction in the form of low flow rate during dialysis (<200 mL/min), difficult cannulation, increased cannulation site bleeding, immature or thrombosed AVF. All patients signed informed consent forms before their procedures were performed. The procedures were performed in a day-care setting by two experienced operators under local anesthesia. Ultrasound (Sonosite Inc., Bothell, Washington, United States) was used for the diagnosis of stenosis and measurement of blood flow and velocities in AVF. The pre-procedure, peri-procedure and post-procedure ultrasounds were performed with the same machine. A high frequency (6-13 MHz). linear probe was used intraoperatively for angioplasty guidance. Angioplasties were carried out in the presence of a structural lesion in the AVF resulting in at least 50% reduction in diameter of the vein. Other criteria used for defining stenosis in AVF were either a blood flow of <250 mL/min or a peak systolic velocity (PSV) of >300 cm/s or ratio of adjacent PSVs >3 (3, 4). In patients with stenotic lesions <2 mm, a two stage procedure was carried out to avoid rupture where a full dilatation was done during second angioplasty procedure within two weeks. However, for statistical analysis those procedures were considered as a single procedure. The mean interval between AVF creation and in angioplasty procedure was 7.2 ± 4.7 months.
Angioplasty procedure
The fistula was examined and the areas to be treated were identified by pre-procedure ultrasound. Access of AVF was obtained using a percutaneous entry thin wall needle of 18G size, 7 cm (Cook Medical, William Cook Europe ApS, Bjaeverskov, Denmark). The access was either antegrade or retrograde depending upon the location of the stenosis. The arterial antegrade access was used when diameter of the artery was >3 mm and distance from the anastomosis was >2 cm. Antegrade venous access was used if radial artery was not suitable. An appropriately sized sheath, 5Fr or 6Fr (Input; Medtronic Inc., Minneapolis, MN, USA) was placed over a short J wire and another 0.035-inch angled guidewire (Radifocus; Terumo Corporation, Tokyo, Japan) was directed through the AVF under ultrasound guidance. Injection Heparin (2500 units) was given intravenously and heparinized saline was flushed through the access sheath intermittently. An angioplasty balloon catheter (Conquest; Bard Peripheral Vascular Inc, Tempe, AZ, USA) was then directed over the guidewire and positioned appropriately across the stenotic segment of vein. Balloon catheters were sized at 1 to 2 mm larger than the normal vein size and ranged from 4 to 7 mm in diameter, with lengths of 2 to 4 cm. Balloon inflation device (Everest, Medtronic or Caliber, Bard Peripheral Vascular) was then attached with the balloon catheter and was inflated at the site of stenosis up to a maximum pressure of 30 atm. After ensuring complete dilatation of the balloon with disappearance of stenotic waist, the balloon catheter, guidewire and the sheath were taken out. Local pressure over the puncture site was given for around 5 minutes. After the procedure, all patients were given clopidogrel 300 mg orally as a single-dose tablet. After keeping the patient under observation for two hours, all patients were sent home on the same day.
Definitions and outcome measures
Patients were followed up until 24 months and blood flow and velocities in AVF were measured at regular intervals. Post-intervention primary and secondary patency rates at 6, 12, 18 and 24 months were calculated. Mean number of interventions per dialysis year was also calculated. Clinical success was defined as the ability to provide adequate dialysis for at least one session for thrombosed AVF and resolution of pre-procedure indicators of access dysfunction (5, 6). Anatomic success was defined as restoration of flow in the fistula with residual stenosis of less than 30% for any underlying significant stenosis (5, 6). Post-intervention primary and secondary patencies of the AVFs were defined in accordance with Society of Interventional Radiology reporting standards and quality improvement guidelines (5–6–7). Primary patency was defined as patency during the interval between primary intervention and fistula thrombosis or repeated radiologic intervention. Secondary patency was defined as patency during the interval between the intervention and the time when the access was surgically declotted, revised or abandoned because of inability to treat the original lesion as per the choice of surgeon, transplant, death of the patient or loss to follow-up. Percutaneous thrombectomy and multiple repetitive angioplasty procedures were included in the secondary patency. Any additional surgical procedure required to maintain patency of fistula was excluded from the secondary patency.
Statistical analysis
NCSS software (version 9.0.21). was used for the statistical analysis. Primary and secondary patency rates for AVFs after angioplasty procedure were calculated by using the Kaplan-Meier curves and tested by log-rank test. The Student's t-test or the Wilcoxon rank sum test was used for univariate analysis of continuous variables, and categorical variables were evaluated by using the Chi-square test or Fisher's exact test. A two-sided p value of less than 0.05 was considered to indicate a statistically significant difference.
Results
Table I shows the demographics of the patients (n = 53), the type of AVFs, clinical indications and the site of stenosis in 78 angioplasty procedures performed. The mean age of the patients, predominantly males, was 51.4 ± 14.5 years and mean interval between the angioplasty procedure and the primary AVF creation was 7.2 ± 4.7 months. Radiocephalic (55.1%) and brachiocephalic (21.8%) were the most common AVFs in which angioplasty was done. The predominant areas of stenosis in the AVFs were juxta-anastomotic (37.2%), draining vein (30.7%) and cannulation site (21.8%). The mean number of stenoses in the AVFs were 1.32 ± 0.59 (range 1-3). Table II shows the access used, primary outcome, mean PSVs and blood flows in the pre-procedure and post-procedure period, post-intervention primary and secondary patency rates. In 49/53 patients (92.4%), 74 angioplasty procedures were successfully performed whereas 4/53 patients (7.54%) had primary failure. A total of 35/49 patients (71.4%) underwent single angioplasty procedure, whereas 14/49 patients (28.5%) underwent multiple angioplasty procedures, range 2-5. Four of 49 patients (8.2%) presented with a thrombosed AVF and had a stenotic lesion detected on ultrasound. These patients underwent percutaneous thrombectomy along with ultrasound-guided balloon angioplasty of the stenotic lesions. One of 49 patients (2.0%) had recurrent stenotic lesions after three sessions of angioplasty procedures and finally underwent a venous patch angioplasty. Four of 53 patients (7.5%) had primary failure either because of intraoperative complication or because of failure to dilate the stenotic lesion with angioplasty alone. One patient had rupture of the vein and developed perilesional hematoma which was not appreciated at the time of procedure and gradually increased leading to thrombosis of access. In 3/4 patients, there were tight stenotic lesions which could not be optimally dilated and as in our early experience there was apprehension to use higher inflation pressures. In 62 cases (79.5%), retrograde venous access was used for angioplasty and in 12 cases (15.4%) antegrade venous access was used. In four cases (5.1%) distal radial artery was of good caliber (>3 mm diameter) and used for antegrade arterial access. The PSVs and blood flow measurements were available for 45 cases only and showed a significant decrease in mean PSVs from pre-operative value of 385.03 ± 30.11 cm/s to 149.48 ± 67.16 cm/s (p<0.0001) in the post-operative period. Mean blood flow across the AVFs increased from 290.26 ± 86.34 mL/min to 822.77 ± 211.29 mL/min (p<0.0001) after the angioplasty procedure. The post-intervention primary patency rates at 6, 12, 18 and 24 months were 78.6%, 60.2%, 53.8% and 48.9%, respectively (Fig. 1). Post-intervention secondary patency rates at 6, 12, 18 and 24 months were 100%, 100%, 95.4% and 89%, respectively (Fig. 2). The mean number of interventions per dialysis year was 0.87. Clinical success and anatomical success was 94.8% and 89.7%, respectively.
Demographics of the patients (n = 53), the type of AVFs and the site of stenosis in 78 angioplasty procedures performed
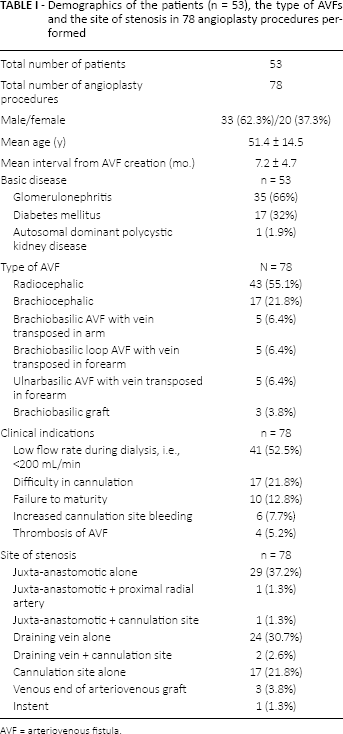
AVF = arteriovenous fistula.
The access used, mean peak systolic velocity and blood flows in the pre-procedure and post-procedure period, primary outcome, post-intervention primary and secondary patency rates in the 78 angioplasties performed
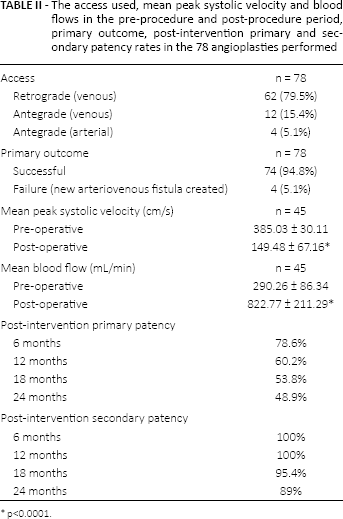
p<0.0001.
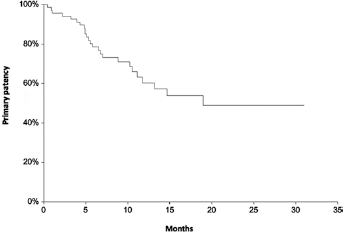
Kaplan-Meier curve of estimated primary patency after ultrasound-guided angioplasty.
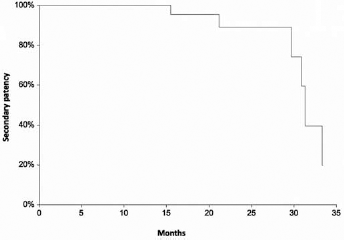
Kaplan-Meier curve of estimated secondary patency after ultrasound-guided angioplasty.
Discussion
In patients with end-stage renal disease, survival and quality of life depends upon a patent and well-functioning hemodialysis access. Native AVFs have been considered as the dialysis access of choice; however, they often become dysfunctional and eventually fail due to development of stenosis (1, 2). Early diagnosis of stenoses in AVFs and subsequent treatment by endovascular interventions has led to substantial reduction in the number of thromboses per patient-year and hence reductions in the cost of access-related hospital care (8, 9). However, repeated endovascular treatment sessions are often necessary, because of high restenosis rates in AVFs. Over the years, endovascular procedures have been traditionally performed under the fluoroscopic guidance and have been the mainstay of non-surgical treatment of stenosed AVFs. However, the need for frequent retreatments has led to an ever-increasing list of patients waiting for an endovascular procedure. In this context, successful development of ultrasound guidance for selected group of patients with peripheral stenosis can ease the burden on fluoroscopic labs. Ultrasound guidance for salvaging vascular access was started in 2013 in a similar situation at our center. The present study demonstrated early experience of ultrasound guidance for angioplasty of dysfunctional vascular access with a procedural success rate of 92.4% which compares favorably with the reported short-term success rate of 85%-98% of fluoroscopy-guided procedures (10, 11). This suggests that ultrasound guidance for angioplasty is a suitable modality for treating selected patients with dysfunctional vascular access, especially in resource-constrained setting. Although there are studies describing the excellent early outcomes of ultrasound-guided angioplasty in stenosed AVFs, there is paucity of data regarding long-term patencies of such treated AVFs (12–13–14–15). Post-intervention primary patency rates in the present study at 6, 12, 18 and 24 months were 78.6%, 60.2%, 53.8% and 48.9%, respectively. Post-intervention secondary patency rates at 6, 12, 18 and 24 months were 100%, 100%, 95.4% and 89%, respectively. This is the first study describing long-term patency of stenosed AVFs treated with ultrasound-guided angioplasty. These rates again are similar to the long-term success of such procedures under fluoroscopy guidance where primary patency at 6 and 12 months have been reported to be 47%-67% and 16%-62%, respectively, and secondary patency rates at 6 and 12 months to be 80%-89% and 76%-86%, respectively (5, 10, 11, 16, 17). Most vascular surgeons use Doppler ultrasound in planning surgical procedures to create dialysis access fistulas as well as for diagnosis and follow-up of AVF malfunctions. Adapting to ultrasound guidance for angioplasty was easy in our experience and could be incorporated in our training program as well. The use of dynamic parameters like PSV and flow measurements provides a real time assessment of success of treatment of stenotic lesions. The earliest experience regarding use of ultrasound for angioplasty was reported in 2007 in 10 patients where the mean preoperative PSVs at the most significant stenosis was shown to decrease from 558 ± 111 cm/s to 236 ± 87 cm/s (p<0.01) and mean volume flow increased from 658 ± 324 mL/min to 1154 ± 402 mL/min (p<0.01) (18). The same group later published a similar experience in larger series of 32 interventions on 25 patients with no peri-procedural thrombosis or any serious complications (19). In the present study, significant improvements in the blood flow measurements with simultaneous reduction in the PSVs after the angioplasty were used to define success of the procedure.
The associated complications described with endovascular procedures are formation of wall hematoma, extravasation or rupture, spasm, thrombosis, and formation of puncture-site hematoma with the reported incidence of less than 4% (13). These complications can be diagnosed and managed with ultrasound guidance but can result in failure of procedure. In our early experience, 4/78 (5.1%) procedures were unsuccessful. One patient had a rupture at the site of the lesion with perilesional hematoma and thrombosis, which could have been salvaged by use of endovascular covered stent. There was reluctance to use higher pressure for tight stenotic lesions after this complication and patients were staged where very tight lesions were initially dilated to less than target diameter and proceeding to optimal dilatation at a second procedure done at an interval of 1-2 weeks. The staged procedure was required only for extremely tight lesions requiring high pressure but could be managed without using endovascular stents which would have resulted in loss of usable length of fistula.
Ultrasound-guided angioplasty can also be used to treat peripheral arterial lesions as well. In our series, only one patient had stenosis of proximal radial artery along with juxta-anastomotic venous stenosis and was successfully treated. Recently, ultrasound guidance has been used to dilate stenotic and unsuitable arteries for AVF creation with promising results (12). In the present study, all the angioplasty procedures were performed under ultrasound guidance and fluoroscopic assistance was not required in any case. The procedure was well tolerated and all patients were sent home on the same day. This shows that with careful selection of patients, the need for fluoroscopic assistance or surgical salvage is minimized as has also been shown in other studies (13–14–15).
Doppler ultrasound guidance has multiple advantages over fluoroscopy for vascular access interventions. Apart from being cost effective and easily available, it is associated with no radiation hazard and avoids nephrotoxic contrasts. As AVFs are superficial, visualization of the endovascular instruments like balloon catheters, wires, and sheaths is better as compared to other sites (18, 19). Ultrasound guidance allows local infiltration of anesthetic agents along the areas of the stenotic lesions. However, there are certain limitations associated with this modality. Any additional central lesions are likely to be missed, as visualization beyond axillary vein may not be adequate, especially in obese patients. Ultrasound technology remains highly operator dependent and requires adequate training. The results of this study are limited by the fact that it was an initial experience and subsequent results are bound to be better. Further, this was not a controlled trial and the number of subjects was not large enough to lay down a conclusive recommendation. A randomized controlled trial comparing fluoroscopy and ultrasound guidance in endovascular management of AVFs with peripheral stenosis is required to compare the results with the two techniques.
Conclusion
Ultrasound guidance for angioplasty is an effective method with good long-term outcomes in selected dialysis patients with peripheral stenosis of AVF and offers advantages over fluoroscopic procedures. It also provides a complete dialysis access management tool, both in planning surgical procedures to create dialysis access fistulas as well as for diagnosis, management and follow-up of AVF malfunctions in selected patients.
Footnotes
Financial support: No grants or funding have been received for this study.
Conflict of interest: None of the authors has financial interest related to this study to disclose.