
Abstract
Māori (Indigenous peoples of Aotearoa New Zealand) continue to experience inequitable health and social outcomes shaped by colonisation and ongoing racism. Well Child Tamariki Ora (WCTO) services provide universal nursing and parenting support for whānau (extended family group) with tamariki (children) under 5 years, however, service design and delivery are not consistently aligned with Māori worldviews and whānau realities, limiting uptake and ongoing engagement. This study used a Kaupapa Māori methodology with constructivist grounded theory methods to explore Māori whānau experiences of WCTO services. Data were generated through interviews and focus groups with 35 Māori participants and analysed using constant comparative methods, with additional theoretical sampling to refine emerging categories. Three theoretical categories were identified: moving from ‘doing to whānau’ to working with whānau; upholding whānau mana; and supporting whānau to access what they need. These findings informed the Mahi Ngātahi framework, which outlines culturally responsive processes for relationships, communication and service delivery aligned with whānau realities. The study demonstrates that when services fail to uphold whānau mana and reflect Māori worldviews, engagement is reduced. In contrast, whakawhanaungatanga (relationship building), manaakitanga (care and hospitality) and flexible, whānau-led approaches support meaningful engagement. Strengthening culturally responsive practice within WCTO services requires attention to policy, workforce development and accountability to ensure culturally safe care and improved outcomes for whānau Māori.
Keywords
Introduction
Maternal, child and family nursing services play a crucial role in supporting pēpi and tamariki health and whānau wellbeing through prevention, early identification, and guidance on parenting and child development. In Aotearoa New Zealand (Aotearoa), Well Child Tamariki Ora (WCTO) services offer universal health and social support for whānau with tamariki under 5 years of age. The current specifications of WCTO services are grounded in the principle of proportionate universalism, which involves allocating increased resources to whānau assessed as having higher levels of need. However, inequities persist, particularly for Māori, the Indigenous peoples of Aotearoa. Māori communities are disproportionately affected by adverse health and social outcomes and therefore may have a greater need for supportive services (Curtis et al., 2019). Māori were also subjected to assimilationist policies that marginalised Māori cultural values and worldviews, and many whānau continue to encounter systemic racism when accessing health services (Graham & Masters-Awatere, 2020; Wepa & Wilson, 2019).
Despite being identified as having a high level of need, many whānau Māori (Māori extended family networks) struggle to engage with WCTO services. For instance, in 2016, while 72% of all babies born in Aotearoa received their allocated assessments at critical developmental milestones, only 57% of Māori babies and their whānau received their WCTO service entitlement (Ministry of Health, 2016). National monitoring data further show that although early WCTO contacts are achieved for most pēpi (babies), completion of later contacts declines over time and remains consistently lower for Māori than for the total population, suggesting that inequities relate not only to access but to sustained engagement with services (Ministry of Health, 2016). This pattern highlights that disparities in WCTO are not only about initial uptake but about the ability of services to maintain meaningful relationships with whānau over time. Despite the pressing need for research and interventions to address these disparities, there has been limited exploration into Māori experiences of WCTO services.
Background
Māori in Aotearoa have continued to experience traumatic and intergenerational losses due to colonisation. Assimilationist policies and practices targeted Māori peoples, contributing to the marginalisation – and in some cases loss – of Māori cultural values and worldviews, disrupting traditional roles and functions within Māori society and weakening whānau connections with whenua (land) (Pool, 2015). The history of Māori and WCTO services in Aotearoa is reflective of these ongoing impacts. A high infant mortality rate in the early 1900s led to Aotearoa joining the Western world ‘infant welfare movement’ and the establishment of the Royal New Zealand Plunket Society (‘Plunket’), a voluntary organisation that provided information and guidance about child-rearing practices for mothers (Bryder, 2020). Plunket nurses did not initially provide services to Māori mothers as Public Health services were responsible for Māori health service provision. This arrangement remained in place until the 1960s, when Plunket attempted to address the stigma and racism embedded in organisational policy (Bryder, 2020).
Today, WCTO services are offered universally to all whānau in Aotearoa with tamariki under 5 years. However, many whānau Māori do not experience WCTO services as accessible, culturally safe, or responsive to their realities, which can reduce uptake and ongoing engagement (Ministry of Health, 2016). These challenges reflect broader calls to decolonise health services so that Māori knowledge, leadership, and decision-making authority are embedded within models of care. In 2020, Plunket officially rebranded as ‘Whānau Āwhina, Plunket’ and redeveloped the philosophy of the service with an explicit focus on equity for Māori. Tamariki Ora (well child health) services within Iwi (tribal nations) and Māori service providers also deliver WCTO services. The Well Child Tamariki Ora Review Report (Ministry of Health, 2020a) highlighted a lack of flexibility within current WCTO provision as contributing to inequitable outcomes for Māori, and it called for a reorientation of WCTO so Māori are meaningfully involved in service design and delivery. The cultural shift required to achieve these aspirations is challenging established structures that have formed the backbone of WCTO services in Aotearoa. While inequities are well documented, Māori whānau continue to demonstrate strong relational knowledge, adaptive strategies, and commitment to collective wellbeing. This study therefore seeks not only to examine barriers but also to foreground whānau strengths and aspirations.
The Study
Aims
This study aimed to understand Māori whānau experiences of WCTO services and generate insights that support cultural alignment of services with whānau needs. We asked, What are the processes involved in working together in a culturally responsive way with Māori accessing Well Child Tamariki Ora services?
Design
We used a Kaupapa Māori methodological approach with constructivist grounded theory methods. Situated within Māori cultural values and practices, Kaupapa Māori research contributes to decolonisation by critiquing contemporary and historical influences on equity for Māori. Kaupapa Māori research also recognises Māori worldviews as fundamental to the handling and interpretation of Māori data (Smith, 2015). Kaupapa Māori methodologies encompass a spectrum of Māori worldviews and understandings (Mahuika, 2015). The Kaupapa Māori methodology for this research was based on Cram’s (2019) Kaupapa Māori Inquiry paradigm components. The components included the recognition of pūrākau (traditional creation narratives), whakapapa (genealogy and interconnectedness), and whānau as central to Māori realities, with mātauranga (Māori ways of knowing) facilitating the exploration and understanding of the data.
We also used constructivist grounded theory methods (Charmaz, 2014) to analyse and manage data, underpinned by four Māori principles: whakawhanaungatanga, manaakitanga, wairuatanga (spirituality) and kaitiakitanga (guardianship). These four principles arose through consultation with kaumātua (elders) and the research advisory rōpū (group), comprising five members, including kaumātua, Māori health practitioners and researchers who provided guidance on research design, analysis and interpretation. Durie’s (2004) ‘research at the interface’ framework supported using Kaupapa Māori methodology with constructivist grounded theory methods. Durie argued that blending mātauranga Māori with Western science optimises Indigenous research within Western research frameworks. The constructivist grounded theory process in this research allowed for an iterative process of adapting and building upon ideas that honoured Māori voices in the development of the theory. The analytic process aimed not only to generate explanatory categories but to develop a practice-oriented framework grounded in whānau accounts, which became the Mahi Ngātahi framework.
Participants
The inclusion criteria were whānau who identified as Māori, located within the greater Auckland and Waikato regions, and who had one or more tamariki under 5 years of age. We used purposive sampling to ensure participation from whānau with direct experience of WCTO services and to capture a range of whānau circumstances relevant to the study aim (Patton, 2015). Recruitment occurred via word of mouth, whakawhanaungatanga through existing networks, and advertising using flyers and social media platforms. We also used snowball recruitment, whereby participating whānau shared study information with others who met inclusion criteria, which supported access to whānau networks that may be less reachable through service channels (Noy, 2008).
Following initial purposive sampling, we undertook additional theoretical sampling – three interviews and three focus groups – to test, refine, and strengthen emerging categories, consistent with constructivist grounded theory and Kaupapa Māori commitments to iterative sense-making with whānau (Charmaz, 2014; Pene et al., 2024). In total, the dataset comprised 18 interviews with Māori whānau and three focus groups, including those undertaken during theoretical sampling to refine emerging categories.
Across the interview component, most interviews involved mothers and tamariki or mothers with extended whānau present, two interviews were with fathers only and two with both mothers and fathers. In reporting, interview quotes are attributed as ‘Whānau [letter]’ and focus group quotes as ‘Focus Group [number]’.
Data Collection
Data collection and analysis occurred concurrently to facilitate the construction of the theory from the data. Data were collected and analysed from March 2018 until February 2020. We used a constructivist interviewing technique whereby the relationship between the interviewer and participants was central to understanding what was said for both interviews and focus groups. This approach also upheld the mana of whānau and encouraged them to lead the kōrero in meaningful ways. Interviews and focus groups were held in settings preferred by whānau, such as whānau homes or community venues, and followed a hui-style (meeting style) process that prioritised whakawhanaungatanga, whakawhiti kōrero (shared discussion), and kai where appropriate. Consistent with a hui-informed approach, interviews commonly began with karakia (prayer)– as guided by whānau – and concluded with karakia; kai was shared during interviews and focus groups, and koha (gift cards) was provided at the beginning to acknowledge participants’ time. An extended process of whakawhanaungatanga often occurred prior to formal questioning, including making connections through whānau, places, and shared experiences. Information sheets were read and explained, questions were invited, and consent forms were discussed prior to signing. Most interviews involved mothers (sometimes with tamariki and/or extended whānau present), with some interviews undertaken with fathers only and some with both parents; focus groups were conducted with mothers only. The interviews and focus groups were semi-structured using the following four questions:
What have been your experiences with (Well Child Tamariki Ora) services?
What matters to you in a (Well Child Tamariki Ora) service?
How would relationships look if they were working well between yourself, your whānau and your Well Child Tamariki Ora provider?
What does partnership look like when working with a Well Child Tamariki Ora service provider?
We digitally recorded the interviews and focus groups and took notes that provided a source for reflection throughout the data analysis. As categories and properties were identified, they were contextualised within the existing constructions of the theory. Constructivist grounded theory methods and input from the research advisory rōpū supported the co-construction of the data analysis. Data collection began with purposive sampling before moving into targeted theoretical sampling to strengthen identified leads.
Indigenous Governance and Relational Accountability
Māori governance and relational accountability were supported through engagement with the research advisory rōpū and consultation with kaumātua throughout the research process. The rōpū contributed to decisions about recruitment approaches, interpretation of findings, and refinement of the developing Mahi Ngātahi framework. This collective approach reflects Kaupapa Māori commitments to shared decision-making, protection of Māori knowledge, and ensuring the research remained accountable to whānau and Māori communities.
Data Analysis
We used constant comparative analysis throughout data collection and analysis (Charmaz, 2014). Transcripts and field notes were uploaded to NVivo Version 12 to support data management. Initial open coding was undertaken close to the data to identify actions, meanings, and processes. Codes were then compared within and across interviews and focus groups to develop focused codes and provisional categories. Memos were used to document analytic decisions and to track category properties and relationships over time. Co-construction of analysis occurred through regular wānanga with the research advisory rōpū, where emerging interpretations were discussed, challenged, and refined, and where implications for the developing Mahi Ngātahi framework were tested against Māori values and whānau realities.
Analytic saturation was considered reached when additional data did not add new properties to the core categories and when the developing framework adequately accounted for variation in whānau experiences across data sources. Where feasible, we shared emerging interpretations back with participating whānau and/or the advisory rōpū for comment and clarification as a form of validation. Participant validation was supported through several processes. During interviews and focus groups, the interviewer used clarifying questions and paraphrasing to check understanding in the moment, supporting co-construction of meaning. Participants were invited to review their transcripts and to follow the research progress via the study website. The research advisory rōpū acted as kaitiaki of the research and provided ongoing cultural guidance and critique of the developing analysis through kanohi ki te kanohi (face to face) meetings and regular engagement with individual members as the research progressed.
Author Positionality and Reflexivity
In keeping with Kaupapa Māori research, we describe our positionality and reflect on how our roles, relationships, and responsibilities shaped the research process and interpretations. The research team included Māori and non-Māori researchers with experience in child health and family nursing, Māori health, and qualitative methods. Several team members had professional or community connections to WCTO services and/or Māori health providers. The lead author (Z.T.) is Māori (Kai Tahu and Kahungunu) and a registered nurse. Her practice worldview has been strongly influenced by the cultural safety movement and its emphasis on power, relationships, and the recipient determining whether care is appropriate. She also brings substantial sector and organisational experience, including 11 years at Plunket in various roles, which provided deep familiarity with WCTO systems and constraints. Throughout the study, she aimed to remain reflexive about how these experiences and commitments to culturally safe, relational care might shape data generation, analysis, and the conclusions drawn. This reflexive positioning, alongside the involvement of Māori advisors and participants, aligns with CONSIDER expectations that Indigenous leadership, relational accountability, and transparency of researcher positioning are visible within Indigenous health research (Huria et al., 2019).
We approached this work with a commitment to Te Tiriti o Waitangi, kawa whakaruruhau (cultural safety underpinned by Māori worldviews), and cultural safety, and we used ongoing reflexive discussion and memoing to consider how our assumptions and positions influenced data generation, analysis, and the development of the Mahi Ngātahi framework. In preparing this manuscript, we used the CONSIDER statement for Indigenous health research and the SRQR guidelines to check completeness and transparency of reporting (Huria et al., 2019; O’Brien et al., 2014).
Ethics
The Auckland University of Technology’s Ethics Committee (AUTEC 17/155) approved this research. The cultural mores of Māori society have Māori ethical principles deeply embedded and provide a vehicle to reclaim and retain lost Māori knowledge. ‘Te Ara Tika: Guidelines for Māori Research Ethics’ (Hudson et al., 2010) underpinned the ethical approach to the study. These ethical guidelines ensured that Māori decision-making and consultation were at the forefront of decisions made and that whānau involvement enhanced their mana (identity, spiritual power). The support and advice provided by the research advisory rōpū ensured a forum to address concerns as they arose, and those key decisions were made collectively.
Findings
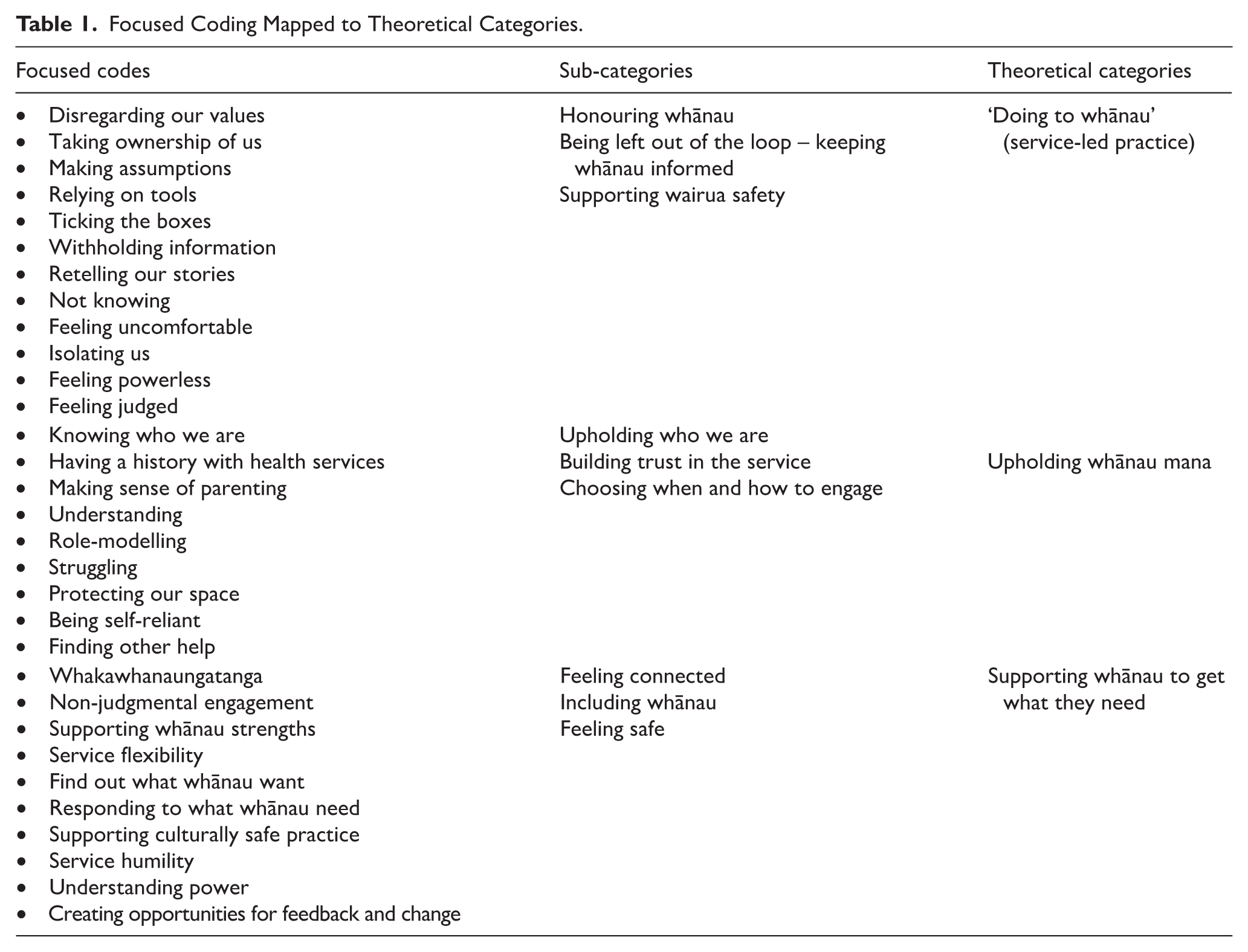
Thirty-five people participated in whānau interviews and focus groups. Analytic saturation – as defined in Methods – was reached when further data did not add new properties to the core categories and when the developing explanation resonated with whānau accounts and advisory rōpū interpretations. Although some category titles describe service-led patterns, they are presented to illuminate the shifts whānau identified as necessary for culturally responsive practice. Thirty-one focused codes were identified, which generated nine sub-categories – see listed in Table 1. The sub-categories led to three theoretical categories that explained Māori whānau experiences of WCTO services. The presentation of the findings relates to the three theoretical categories, illustrated with participants’ examples.
Focused Coding Mapped to Theoretical Categories.
Working With Whānau (Moving From ‘Doing to Whānau’)
‘Doing to whānau’ is a pattern of service-led practice that whānau described as the opposite of mahi ngātahi (working together). The cycle began when providers entered whānau spaces in ways that did not honour tikanga or whānau preferences – honouring whānau space. It continued when information and decisions were not shared transparently, leaving whānau uncertain about what was happening and why – keeping whānau informed. Over time, these interactions contributed to whānau withdrawing or ‘shutting down’, including limiting contact with services to protect themselves and their tamariki.
Whānau experienced a lack of whakawhanaungatanga and manaakitanga when accessing WCTO services. Relational networks are foundational to Māori worldviews, and making connections with broader whānau was often missing from their experience of WCTO service delivery. This situation extended to using tools – graphs, developmental assessments, computers - that WCTO services used to direct the discussion instead of finding out what whānau wanted to know. WCTO services disregarded existing information sharing processes used by whānau, demonstrating a lack of recognition of knowledge across generations:
That bedsharing thing. So this Pākehā [non-Māori] nurse, she came out and said, ‘You can’t sleep with your baby, do not put the baby in your bed, ra-ra-ra’. . . . I’m like, shut up, not that I was going to anyway. But traditionally, you know, I’m surprised I’m here! And my grandmother, she had us in bed with her. . . (Whānau M).
Direct questioning about the child’s welfare without establishing authentic relationships led whānau to feel that WCTO made assumptions about their realities. This approach led to whānau feeling uncomfortable having the service in their homes:
I don’t think I knew anything about my nurses. Like they would tell me their names, but you know, nothing else. Whereas especially with Māori, we like to get to know the person and where they’re from and have that conversation. But no, it’s just ‘Hi, I’m da-da-da, and I’m here to do this’, and they pull out their computer. I’m like, you’re in my house - I wanna know who you are (Focus Group 2).
Whānau felt they were ‘left out of the loop’ as recipients of a WCTO service. Whānau experienced WCTO service providers as focusing on completing a checklist of tasks rather than building relationships beyond a superficial level. Participants became uncertain about the purpose of WCTO services and suspicious of the information collected or withheld during these interactions:
I kind of like, not relied on [them], but I thought that they would come and either reassure me or teach me or say I was doing a good job. And then I feel like when they came, it was kind of the surface information. They [WCTO] weigh them [baby] and see how long they are, and then get a general overview for their own records. . . (Whānau T).
Whānau described the process of retelling their stories to multiple health professionals as indicative of a lack of connection within and between service providers. The experience of being treated like a data source rather than people with unique stories and needs led to whānau identifying other people to discuss their situations with outside of WCTO service providers.
This ongoing lack of connection with WCTO services led to whānau feeling uncomfortable in their interactions with WCTO service providers. Whānau described how they shut down when they thought the WCTO service providers had values and expectations that did not align with their realities. An example of this was the lack of acknowledgement of wairuatanga as fundamental to Māori worldviews in providing structures to guide parenting practice:
What the nurses don’t see is that our tupuna [ancestors] have left us templates, and we’ve just got to find them. Even in our waiata [songs], our whaikōrero [formal speeches], everything, the templates are already there for us to follow (Whānau T).
At times whānau felt powerless that WCTO service providers would over-ride their decision-making authority by people who did not trust their ability to make decisions. When whānau experienced powerlessness within interactions with a health or social service, they anticipated a similar experience when accessing other services. Feelings of powerlessness are linked closely to feeling judged. Whānau described how some service providers made assumptions about their lives before getting to know them. These assumptions made some whānau think they were ‘not Māori enough’ while others felt ‘too Māori’ to fit in with the service:
Just how they speak to you. The way you’re looked at. ‘Do you have a community services card?’ I bet they don’t ask others that. I just smile and nod and think to myself, I am not going to spend my time with you again (Focus group 1).
Upholding Whānau Mana
The second category, Upholding whānau mana, describes how service-led practices can undermine mana and how whānau respond by protecting who they are. When providers overlooked the whakapapa of parenting knowledge and did not recognise whānau strengths, whānau often felt judged or misunderstood. In response, whānau defended their parenting practices, were cautious about trust, and in some cases avoided further contact with WCTO providers:
The values. I mean, what my parents taught us, they’re just normal. That’s just how we were brought up. I mean, it’s not like we went to school and learnt it. It was what it was. It is who we are. I don’t know if those nurses understand that (Whānau J).
Accessing health or social services can create anxiety for whānau due to negative historical and intergenerational encounters with providers. WCTO services lacked an exploration of the history of whānau engagement with health and social services. Whānau protected themselves from being let down by WCTO service providers based on personal and extended whānau experiences.
When whānau felt uneasy about how the WCTO service providers interacted, they attempted to reclaim their power by avoiding contact. Whānau protected their physical space by not being at home for appointments. They missed clinic appointments and screened phone calls from WCTO services. When whānau felt uncomfortable in their wairua (spirit) during the assessments, they were more likely to shut down the questions by giving the answers they thought the health care providers would want to hear. Whānau would look for ways to access support and information from others if they lacked trust WCTO services would maintain the mana of their whānau:
I just said to her I would take baby to the GP for a weigh. I didn’t want them coming in here with their judgments, making me feel like a bad mother. I’ll just weigh her when I get her jabs (Focus group 1).
Supporting Whānau to Access What They Need
The third category, Supporting whānau to access what they need, describes the relational and service processes that can interrupt the cycles above and enable whānau-led engagement. The Mahi Ngātahi framework – see Figure 1 – illustrates how WCTO services can provide culturally responsive care when working within a whānau context. Building whānau confidence required time and relationship investment by the provider, flexibility in how support was offered, and a commitment to respond to what whānau identified as most pressing, rather than requiring whānau to fit service expectations.
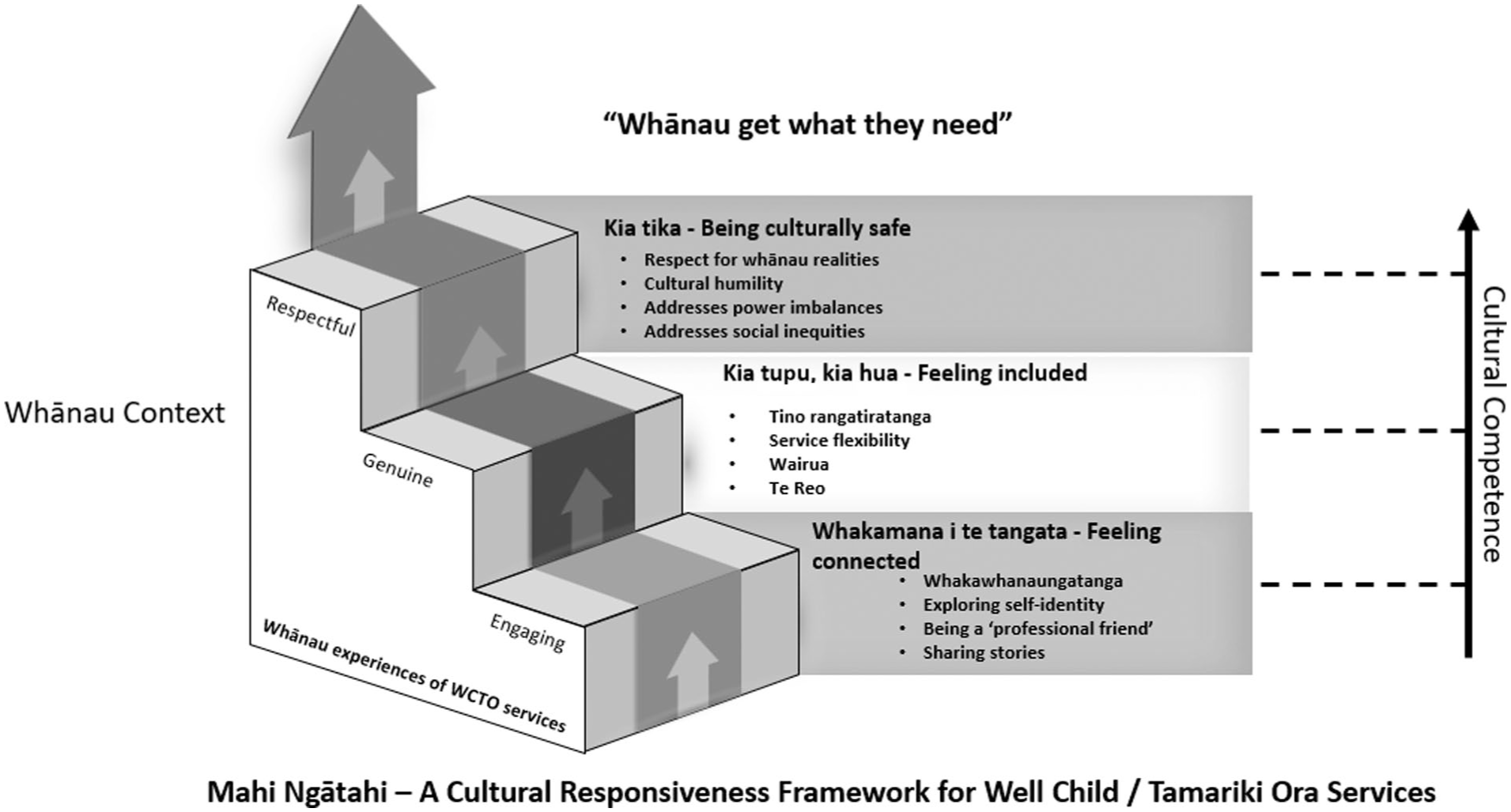
Mahi Ngātahi framework.
The Mahi Ngātahi Framework in Figure 1 outlines three steps to achieving culturally responsive WCTO service delivery to whānau. Whakamana i te tangata - Being connected reflects the connection between the WCTO service provider and whānau. Engaging whānau with WCTO services promotes the likelihood of growing a positive relationship. Whakawhanaungatanga refers to building relationships by identifying areas of commonality. Whānau are more likely to engage positively with WCTO providers who share something of themselves to find points of connection. Making connections involves initially putting the business to one side and allowing time for whānau to get a sense of who was working with them:
. . . speak to me from your heart before you tell me what you know (Whānau G).
Whānau needed WCTO providers to be friendly and supportive, and interested in them as people. Many whānau described the positive impact WCTO service providers have when they focus on whānau strengths rather than weaknesses:
She [WCTO provider] was really friendly. She always told me I was doing well and was really encouraging. I felt like I could be honest with her about what was going on for us (Whānau R).
Kia tupu, kia hua (to grow, to flourish) - Including whānau in the Mahi Ngātahi framework outlines the need for the genuine inclusion of whānau in WCTO service delivery. Whānau should be included in the design and delivery of WCTO services, particularly if services are to achieve their equity aspirations for Māori. Ensuring whānau are involved in how WCTO services are delivered is critical to upholding tino rangatiratanga (self-determination), so whānau have the choice and power to determine what happens to them.
Service flexibility was another key influence over how WCTO providers included whānau within WCTO services. Whānau described how some nurses worked with them to meet the most pressing needs, such as providing transport to get groceries or for health or social appointments. Furthermore, creating space for spiritual and holistic practices as part of WCTO assessments ensured there was a platform to establish authentic relationships with whānau:
People go into people’s houses all the time and say a prayer, make sure there’s no bad energy, clear the energy out. I believe in this, and it’s good to make sure we are in a good space. For me, being Christian is really powerful to us (Whānau J).
The final step in the Mahi Ngātahi Framework is whānau experiencing a WCTO service that is Culturally safe - Kia tika. Whānau described feeling safe within their cultural environments, supported by service providers that demonstrate cultural humility. Cultural humility refers to service providers not expecting that whānau will conform to the cultural norms of the service. Understanding the service culture and its impact on whānau and the power attached to interactions, is fundamental to respectful engagement. When health promotion education contradicts whānau beliefs, WCTO providers position themselves in opposition to whānau. In these circumstances, many whānau feel pressured to lie about their parenting practices to avoid judgement:
I think if you want to glean as much information in terms of baby’s progress and development and what whānau are doing, then you need to have a really good relationship with the wahine (woman) that you’re working with, so they can speak freely. They’re not restricted, not hiding stuff (Whānau B).
When whānau are uncertain about what the service is for, they may be unable to identify whether it meets their needs. WCTO service providers need to ensure they share information so whānau can understand and make informed decisions about their care.
Discussion
This study aimed to understand Māori whānau experiences of WCTO services and to generate insights that support cultural alignment of services with whānau needs. The findings show that when WCTO practice is service-led (‘doing to whānau’) and does not uphold whānau mana, whānau may limit contact or seek support elsewhere. In contrast, whānau described positive experiences when providers were friendly and supportive, took time for whakawhanaungatanga, and focused on whānau strengths. The Mahi Ngātahi framework brings these insights together as a practical blueprint for reorienting WCTO relationships, communication, and service delivery so whānau feel connected, included, and safe.
The study design and analytic approach were shaped by Kaupapa Māori methodology and aligned with the CONSIDER framework, which emphasises Indigenous governance, community relevance, and accountability throughout research processes (Huria et al., 2019). This positioning strengthens the interpretation of findings as grounded not only in participant experience, but in Indigenous research principles guiding the work.
The framework aligns with established Māori models of health that emphasise relational and holistic wellbeing, including Te Whare Tapa Whā, Te Wheke, and Te Pae Māhutonga, where connection, cultural identity, and supportive environments are central to pae ora (healthy futures) (Durie, 1985, 1999; Ministry of Health, 2020b; Pere, 1991). Locating WCTO practice within these Māori health frameworks reinforces that culturally responsive care is not an ‘add on’, but a core mechanism for enabling whānau and tamariki wellbeing.
The Mahi Ngātahi framework provides a blueprint for culturally responsive practice when working with whānau accessing WCTO services. Cultural responsiveness refers to culturally informed service provision within a broader socio-political context (Werkmeister-Rozas & Klein, 2009). Culturally responsive care depends on both the qualities and skills of the health professional and the infrastructure that supports services. Whānau in this study wanted a WCTO service that engaged with them for who they are and what matters to them. Cultural responsiveness requires WCTO providers to prioritise whānau voice, practise cultural humility, and critique surrounding policies and processes to enable flexible, whānau-led approaches. It also requires system-level reorientation of WCTO services to sustain the cultural realities of whānau, including te reo Māori and wairuatanga.
Cultural safety is critical to WCTO service cultural responsiveness because it requires recognition of the social and political power dynamics that influence the provision and receipt of care (Ramsden, 2015). Whānau described the need for WCTO providers to understand how professional and organisational power shapes interactions, and to work in ways that strengthen whānau outcomes. The extent to which a service is culturally safe is determined by the recipient(s) of care. This reinforces the need for WCTO services to create non-racist, respectful, and affirming environments and to embed accountability for culturally safe practice within supervision, professional development, and organisational policy.
Recent shifts in Aotearoa health policy and professional regulation further emphasise Te Tiriti o Waitangi obligations and culturally safe practice. The Waitangi Tribunal’s Wai 2575 stage one Hauora report identified systemic failures to address Māori health inequities and made recommendations to better give effect to tino rangatiratanga and equity (Waitangi Tribunal, 2019). The Ministry of Health’s Whakamaua: Māori Health Action Plan 2020–2025 provides direction for achieving pae ora through system-wide action (Ministry of Health, 2020b). In nursing, the Nursing Council of New Zealand’s 2024 registered nurse standards of competence consultation positions Te Tiriti, kawa whakaruruhau, cultural safety, and equity as fundamental to safe practice (Nursing Council of New Zealand, 2024). These developments support the paper’s argument that reorienting WCTO requires both relational practice change and sustained Māori health leadership and workforce development within services. Achieving these shifts also depends on strengthening Māori health leadership and workforce pathways within WCTO services. Māori practitioners play a critical role in embedding relational, culturally safe practice and shaping service design from within.
Racism remains a determinant of health because it creates additional stress for whānau and barriers to accessing and receiving respectful care (Harris et al., 2019). The findings from this study reinforce how racism can be experienced through everyday interactions and organisational practices that undermine whānau mana, leading some whānau to avoid future engagement with health services. These results align with prior qualitative evidence that cultural alienation contributes to Māori patients and whānau disengaging from health care interactions (Graham & Masters-Awatere, 2020).
To achieve cultural competence, health professionals must work effectively within diverse cultural contexts and respond to the unique needs of individuals (Hart & Moreno, 2016). The Mahi Ngātahi framework illustrates the cultural competency of the WCTO practitioner on a continuum in which their position changes based upon the skills they bring into relationships with different whānau. All health professionals in Aotearoa must demonstrate cultural competence in their practice as stipulated by the Health Practitioner’s Competence Assurance Act 2003 and the later amendment (Health Practitioners Competence Assurance Amendment Act 2019). In the broader nursing literature, cultural competence focuses on the nurse’s awareness, attitudes, and behaviours to recognise that the process is ongoing and ever-evolving (Hart & Moreno, 2016). Therefore, binary definitions of cultural competence do not reflect the complex realities of whānau and nurses’ needing to respond and adapt to cultural differences.
Limitations
The sample size of 18 whānau comprising 35 participants was relatively small, and participants were all located within the Auckland and Waikato regions, which limits transferability to other geographic locations. Analytic saturation – as defined in the Methods – was reached for the core categories within this dataset, however, additional research with whānau in other regions and with different service providers may extend or refine the framework. The provision of WCTO services by Plunket and other WCTO providers was not analysed comparatively within this study. Further research into service-specific experiences would assist in identifying how individual services could strengthen responsiveness to whānau.
Conclusion
Māori in Aotearoa have long experienced health services that disregard their values and priorities through the imposition of dominant cultural norms. This study shows how WCTO service-led practices can undermine whānau mana and reduce engagement, while culturally responsive practice grounded in whakawhanaungatanga, inclusion of whānau, and cultural safety can strengthen relationships and support whānau to access what they need. The Mahi Ngātahi framework provides a structure to guide WCTO providers and services when working with whānau Māori. Future work should focus on implementing the framework in partnership with whānau and evaluating its impact on service experience and equity outcomes. Addressing racism and embedding cultural responsiveness and safety within WCTO services remain essential for reducing inequities and supporting pae ora for whānau Māori in Aotearoa New Zealand. More broadly, this study illustrates how Kaupapa Māori research approaches can strengthen health service research by ensuring that Indigenous knowledge, relational accountability, and community relevance remain central to both evidence generation and service improvement.
Footnotes
Acknowledgements
We are deeply grateful to the whānau who shared their stories, experiences and aspirations, and who trusted us with their kōrero. We acknowledge the research advisory rōpū and kaumātua for their ongoing guidance, wisdom and critical input throughout the research process. Their collective contribution ensured the study remained true to Kaupapa Māori values and responsive to whānau realities.
Authors’ Note
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is based on research undertaken as part of a doctoral programme supported by a Health Research Council of New Zealand Māori Health PhD Scholarship. No specific funding was received for the preparation of this manuscript or its publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Glossary
hui-style meeting-style
Iwi tribe or nation
kaitiakitanga guardianship
kanohi ki te kanohi face to face
karakia prayer
kaumātua elders
Kaupapa Māori Māori approach or methodology; grounded in Māori worldviews
kawa whakaruruhau cultural safety underpinned by Māori worldviews
mana spiritual power, authority, prestige
manaakitanga hospitality, kindness, respect
mātauranga Māori knowledge, ways of knowing
Pākehā New Zealander of European descent
pēpi babies
pūrākau traditional creation narrative
rōpū group, collective
tāngata whenua people of the land, Indigenous people of Aotearoa
tamariki children
Tamariki Ora Healthy children
Te Tiriti o Waitangi The Treaty of Waitangi (Māori version)
tino rangatiratanga self-determination, sovereignty
tupuna ancestors
waiata song
wairua spirit
wairuatanga spirituality
whakapapa genealogy, lineage, interconnectedness
whaikōrero formal speech
whānau extended family group
Whānau Āwhina Plunket Organisation providing child and family health services in Aotearoa
whanaungatanga relationship building