
Abstract

Report of a Case
A woman in her 50s presented in our connective tissue diseases clinic with a 6-month history of a recalcitrant eruption of the upper chest and back that failed treatment with clobetasol ointment and ketoconazole cream. Her medical history was significant for a stage IIb breast cancer diagnosed 10 years prior, with recent local-regional recurrence and bone metastasis. The patient deferred chemotherapy treatment, and unfortunately, attempts at hormonal therapy were unsuccessful due to the severity of side effects and disease progression. Therefore, 2 months prior to the development of the eruption, palbociclib and fulvestrant were introduced. Notably, the patient was taking no other medications or herbal remedies.
On examination, the upper chest and back had annular, erythematous scaly plaques (Figure 1A,B). A review of systems was negative other than fatigue and nausea related to her cancer treatment regimen.

Clinical images of the patient 2 months after introduction of palbociclib and fulvestrant. Annular, erythematous scaly plaques on the patient’s upper chest (A) and back (B).
Given clinical suspicion for subacute cutaneous lupus erythematosus (SCLE), a biopsy was performed, which demonstrated vacuolar interface dermatitis with perivascular chronic inflammation and extensive dermal mucin deposition (Figure 2A-C). Laboratory findings revealed trace antinuclear antibody (ANA) positivity; anti-dsDNA, anti-Ro/SSa, and anti-La/SSb antibodies were negative.
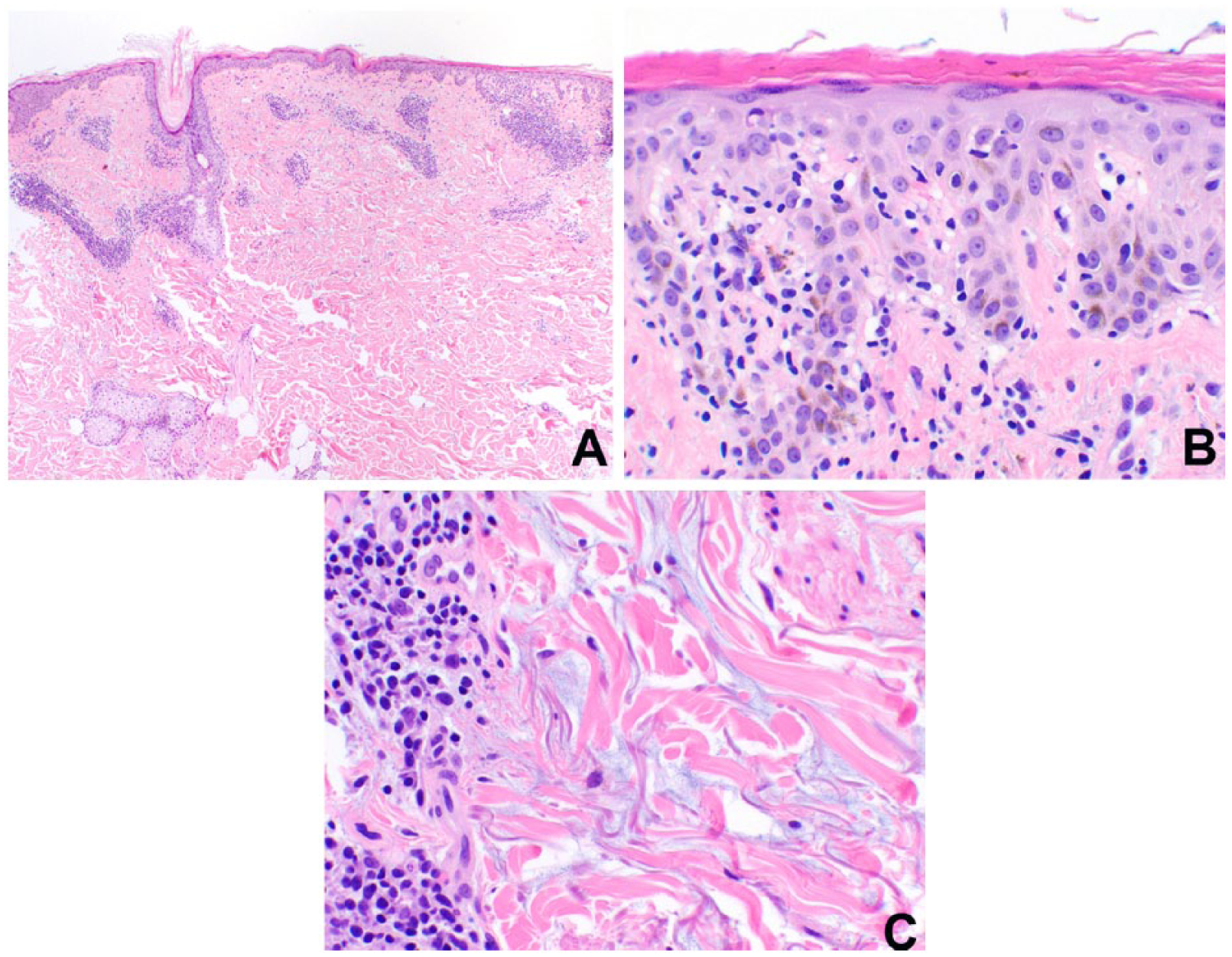
Punch biopsy specimen. (A) At scanning magnification, a “cuffed” perivascular lymphocytic infiltrate is seen (hematoxylin-eosin, ×40). (B) At higher magnification, lymphocytes are seen along the dermal-epidermal junction associated with vacuolar interface changes (hematoxylin-eosin, ×400). (C) In addition to a perivascular lymphocytic infiltrate, extensive dermal mucin, seen as pools of light blue material between eosinophilic collagen fibers, was present (hematoxylin-eosin, ×400).
Given the clinicopathologic diagnosis of SCLE, the patient was prescribed hydroxychloroquine but never initiated treatment. One month later, the patient discontinued palbociclib due to side effects but remained on fulvestrant. Within a month of discontinuing palbociclib, her cutaneous eruption resolved. Therefore, a diagnosis of drug-induced SCLE (DI-SCLE) by palbociclib was favored.
Discussion
Since DI-SCLE was first described in 1985, an increasing number of drugs have been associated with its development. Some conventional chemotherapeutic agents, including taxanes, pyrimidine analogues, and anthracyclines, have been established as culprits for years. 1 More recently, the emergence of targeted cancer therapies has led to new patterns of skin toxicities. To date, only 3 cases of SCLE induced by targeted therapies have been described, one from the multikinase inhibitor pazopanib and 2 from the antivascular endothelial growth factor monoclonal antibody bevacizumab. 2
Palbociclib is a novel targeted therapy with activity against cyclin-dependent kinases (CDKs) 4 and 6. Cyclin D1 and CDK 4/6 are downstream of multiple signaling pathways, which lead to cellular proliferation. Through inhibition of cyclin D–CDK4/6 complex activity, palbociclib inhibits the phosphorylation of retinoblastoma (Rb) protein, blocking cell cycle progression from G1 to S phases. This new drug, in combination with letrozole, has been demonstrated to prolong progression-free survival in postmenopausal women with estrogen receptor (ER)–positive, human epidermal growth factor receptor (HER2)–negative metastatic breast cancer. 3 The increased cell apoptosis induced by palbociclib may lead to a release of nucleosomes, as hypothesized with other chemotherapeutic agents that induce SCLE, thus triggering autoimmunity. 4
Notably, this patient was also on fulvestrant, an estrogen-selective receptor downregulator. A double-blind placebo-controlled trial using fulvestrant as therapy for systemic lupus erythematosus (SLE) demonstrated significant improvement in the SLE disease activity index (SLEDAI) score. 5 We hypothesize that this could explain the limited skin involvement in our patient.
No diagnostic criteria exist for DI-SCLE, but a case definition has been proposed. This includes the initial appearance of an eruption indistinguishable clinically, histopathologically, and immunologically from idiopathic SCLE following systemic administration of a drug, along with spontaneous resolution of the eruption upon discontinuation of the triggering medication. 1 A recent systematic review of DI-SCLE showed that the condition predominantly affected white women who were, on average, older than those with idiopathic SCLE. Eighty percent had positive anti-Ro/SSa antibodies. The median time interval between introduction of a new drug and development of DI-SCLE was 6 weeks, but this varied widely and was often shortest for chemotherapy-induced cases. Most cases of DI-SCLE resolved within weeks of drug withdrawal. 1
In our case, reintroduction of palbociclib to confirm a drug culprit was not feasible and ethical given that this cancer treatment regimen was discontinued due to severe fatigue and nausea and not because of the skin findings. Despite this, the clinical findings, classic histopathology, and timing support a diagnosis of DI-SCLE as the patient developed an eruption compatible with SCLE after 2 months of palbociclib therapy, which resolved 1 month following treatment discontinuation and never recurred after 1-year follow-up. Furthermore, 20% of DI-SCLE cases are negative for Ro antibodies.
To our knowledge, this is the first reported case of SCLE induced by palbociclib in the literature. Given that palbociclib is increasingly being used for the treatment of advanced breast cancer, it is important for clinicians to be aware of this possible cutaneous complication.
Footnotes
Acknowledgements
We are indebted to the patient for granting us permission to publish this case, including clinical photos.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Drs Patel, Granter, and Vleugels have no relevant financial interests to report. Dr Joanie Pinard serves as consultant for Celgene. Dr Joseph Merola serves as consultant/advisor for Biogen IDEC, AbbVie, Amgen, Eli Lilly, Novartis, Pfizer, Janssen, UCB, Kiniksa, Momenta, and Mallinckrodt.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.