
Abstract
Qualitative health research has examined how people make meaning in the context of Type 1 Diabetes Mellitus (T1DM) diagnoses, often focusing on how patients describe and reflect upon their current health situation. However, meaning is frequently treated as something enclosed within signs, with limited attention to how it emerges dynamically through lived, bodily processes. Addressing these two gaps, this article explores how affect and bodily experience guide the process of meaning
Keywords
Introduction
In its most recent report, the International Diabetes Federation (IDF, 2025) reported that 503,000 new cases of type 1 diabetes mellitus (T1DM) were diagnosed in people of all ages in 2024. The diagnosis represents the beginning of a medical therapy focused on controlling the evolution of the disease and achieving the expected health outcomes. However, international organizations and several studies agree that the treatment of this chronic condition is highly demanding, largely because it is multicomponent and self-administered (Coffen, 2009; Elian et al., 2023; Ortega et al., 2018; World Health Organization [WHO], 2003). Even with the availability of medications, supplies, education, technology and specialized medical care, a significant proportion of patients fail to achieve the expected clinical goals, as shown by recent systematic reviews, meta-analyses and global reports (Boonpattharatthiti et al., 2024; Hafidh & Abdella, 2022; IDF, 2025). Organizations such as the American Diabetes Association have recognized that the diagnosis of T1DM carries psychosocial dimensions that cannot be understood solely from a biomedical approach or through the technical procedures of clinical care (American Diabetes Association [ADA], 2025). The experience of receiving this diagnosis includes feelings of confusion, overwhelm, and worry about the future. It is therefore necessary to approach the subjective experience of those living with a T1DM diagnosis, with the aim of gaining a deeper understanding of what it affectively entails to implement the treatment, expanding upon predominant interpretations that focus mainly on behavioral or rational aspects (Valsiner, 2014).
From a biomedical perspective, the diagnosis of T1DM occurs when the immune system has attacked the beta cells of the pancreas, which are responsible for insulin production (ADA, 2023; IDF, 2025). This chronic condition can lead to long-term complications, such as the deterioration of organs like the kidneys, eyes, heart and feet due to the sustained circulation of elevated blood glucose levels. However, these consequences are often experienced by patients as remote threats, located in the distant future. In this sense, the disease demands greater body awareness and continuous attention to one’s own physiological states and the ways in which they are sensed (Cleves & Ocampo, 2018). Treatment of T1DM, broadly speaking, involves multiple self-administered tasks such as daily insulin delivery (via injections or automated devices), adherence to a healthy diet, regular exercise, constant monitoring of glucose levels, and regular attendance at medical checkups (ADA, 2023; IDF, 2025; Munion et al., 2020; Romero-Castillo et al., 2022; Turton et al., 2023). However, what might appear to be a clearly defined and easily applicable routine from the external point of view of health prescribing, becomes a constant challenge because it demands continuous reorganization of everyday social contexts when associated with feelings of embarrassment or public exposure (Datye et al., 2019; Lv et al., 2021; Raymaekers et al., 2021). In addition, managing blood glucose levels involves avoiding both hypoglycemic episodes and hyperglycemic peaks, which generates persistent feelings of frustration and loss of freedom in many patients (Chatwin et al., 2021; Peter et al., 2023). In this light, it can be argued that the diagnosis of a chronic illness such as T1DM is not merely about identifying an organic dysfunction or initiating a therapeutic intervention. On the contrary, the diagnosis names a condition that profoundly affects how a person can think and decide about themselves, their illness, and the world around them (Bruner, 1990; Janoff-Bulman & McPherson Frantz, 1997; Sontag, 1996). It also allows the diagnosis to be conceived as an embodied reality that reorganizes everyday life (Frank, 2013; Kleinman, 2010, 2020; Kleinman et al., 1978). This makes the experience of diagnosis a privileged space from which to understand, from the internal perspective of those who live with it, how patients experience their condition, as it sheds significant light on the decisions they make regarding their treatment and self-care.
Qualitative research in adult populations has also advanced in describing the lived experience of patients with T1DM (Helgeson, 2021; Overgaard et al., 2021; Walker & Litchman, 2021). For instance, a recent systematic review and meta-analysis aimed to understand how adults experience the diagnosis and the phenomena associated with the early process of adapting to life with diabetes. Its findings identified recurrent themes such as initial disbelief, the process of learning about the disease and self-management, the emotional impact of the diagnosis, the need to integrate the illness into one’s personal identity, the reorganization of everyday life and social roles, the role of family and social support, and the importance of connecting with others living with T1DM (Due-Christensen et al., 2018). A predominant methodological trend in the research has been the use of thematic analysis. These studies describe how the diagnosis is experienced by presenting stable patterns of meaning. One such example is a study aimed at examining the meaning of diabetic identity in adults. It identified seven themes related to illness, individuation, and culture: willingness to identify, stories of the non-sick, legends of the responsible, a tradition of transformation, sense of similarity, mystification of difference, and diabetes as a unifying social category (Walker & Litchman, 2021). Similarly, another study employing thematic analysis explored the underlying mechanisms of the specific challenges faced by individuals with T1DM in the workplace. The findings revealed that these individuals are caught between two competing logics: the logic of the patient and the logic of the worker (Overgaard et al., 2021). In an alternative line of research, the authors of this contribution have been developing a field of inquiry focused on understanding how embodied meanings emerge, persist, and change in guiding patients’ experiences and decisions in the context of T1DM (Cleves et al., 2024, 2025; Cleves & Ocampo, 2018). In doing so, they have shifted the emphasis from the description of experience -as is common in thematic analyses- to its ongoing configuration (Cornish et al., 2014). This shift entails a theoretical and methodological approach aimed at understanding processes of change and relative stabilization of meaning. In line with this, the present study implements a microgenetic analysis in a novel way. The following section presents the theoretical foundation that supports this approach and enables the reporting of findings from the case of Martha to the scientific community.
The Semiotic Construction of Meaning as a Dynamic Process
This study departs from the premise that human beings are continuously engaged in meaning-making processes that are inherently dynamic and never fully complete. In these processes, thought and affect are inseparably intertwined, taking shape through embodied experience and interaction with the world. This perspective assumes that there is no direct experience of reality; rather, everything that is known and felt is mediated by a semiotic order; that is, by signs that acquire meaning in relation to others within a dynamic system (Roncancio et al., 2023; Valsiner, 2007, 2014, 2022; Vygotsky, 2008). This approach argues that people do not merely process pre-existing information from the external world; rather, they actively configure experience through meaning-making operations in which they select, prioritize, and organize certain aspects over others, in an articulatory process that gives rise to emergent and transformable meanings (Bruner, 1990; Salvatore, 2016; Salvatore et al., 2024; Salvatore & De Luca Picione, 2023).
This conception of meaning as dynamic and embodied is particularly enriched by the triadic tradition of Charles S. Peirce, which allows for a more precise understanding of how experience is transformed through signs. Unlike the Saussurean model -where the sign is a relatively stable dyad between signifier and signified, established by a relatively fixed social convention- the peircean perspective holds that a sign does not carry a fixed meaning in itself. Instead, meaning is constructed in a dynamic relationship between a sign, an object, and an interpretant; that is, an instance of interpretation that gives rise to new signs (Peirce, 1932). The process of signification is thus always open, evolving, and requires a subject who interprets. Within this framework, a sign (A) acquires meaning by virtue of the sign that follows it (B), which acts as an interpretation of the former by selecting a relevant aspect of the represented object; that is, what Peirce referred to as the ground. In turn, the semiodynamic model developed by Salvatore and collaborators (Salvatore, 2016; Salvatore et al., 2024) describes this operation as a tension between Signification in Presence (SIP), that is, what the sign actualizes as content of experience, and Signification in Absence (SIA), which refers to the set of meaningful possibilities that remain in the background. For instance, when saying that someone “is tall”, the ground of height is actualized, while other possible dimensions such as age, gender, or profession are relegated. In this dialectic between what is emphasized and what is left out, the subject configures their experiential field in a singular, organized, and affectively relevant way (Reho & Salvatore, 2024; Salvatore & Cordella, 2024).
Importantly, signs do not merely represent; they can also transform the ontological status of objects (Tateo, 2018, 2024). This transformative capacity of signs is particularly powerful for understanding how individuals experience and re-signify illness-related events. In the case of T1DM, this becomes evident when, for example, an insulin syringe -whose materiality is similar to that of any other syringe- becomes, for the person living with T1DM, a sign that reorganizes their relationship with the body (now constantly marked by the need for injections), with time (as insulin administration follows a strict temporal structure, e.g., before each meal or at bedtime), and with the social world (since it must be carried and used in shared spaces, often associated with eating and interpersonal encounters). Thus, understanding the dynamics of the meaning of T1DM diagnosis requires not only analyzing what is verbally expressed through reflective thought processes, but also examining how certain signs acquire relevance, become organized in presence and absence, and stabilize within a network of signs involving the body, affect, thought, and others (Salvatore & De Luca Picione, 2023; Zittoun, 2017). In line with these theoretical premises and the current state of scientific knowledge, the research question guiding this study is: How do meanings related to the experience of a T1DM diagnosis emerge, transform, and stabilize? The aim of this study was defined as analyzing the configuration of meanings attributed to the diagnosis of T1DM across four key experiential moments: (1) the transition into illness, (2) the reception of the diagnosis, (3) the search for a cure, and (4) the embodied experience of a hypoglycemic episode.
Methodology
This study employs an idiographic approach (De Luca Picione et al., 2019; Salvatore & De Luca Picione, 2023; Valsiner, 2024), which emphasizes the singularity of psychological phenomena and proposes an epistemological shift from the traditional paradigm of evidence accumulation toward the development of novel forms of analyses (Branco & Valsiner, 1997; Stavrou et al., 2014; Valsiner, 2022). This perspective holds that deep knowledge can be generated through the intensive study of a single case, situated within a contextual field of relationships and unfolding over time (Yin, 2014; Zittoun, 2016). The epistemological stance asserts that it is possible to identify “general processes within the particular,” as cases reflect the complex interrelation between individual subjectivity and shared cultural meanings (Valsiner, 2014). Accordingly, the case of “Martha” is analyzed based on the assumption that analytic generalizations can be made, which may later contribute to theoretical development through the logical analysis of multiple cases.
Context and Participants
This article presents the case of Martha, a 42-year-old woman who was diagnosed with T1DM at the age of 18. At the time of the study, she lived in a middle-class urban setting in Colombia. She held a university degree, was divorced, and had an 8-year-old son. She shared her household with her mother and her child.
Data Generation
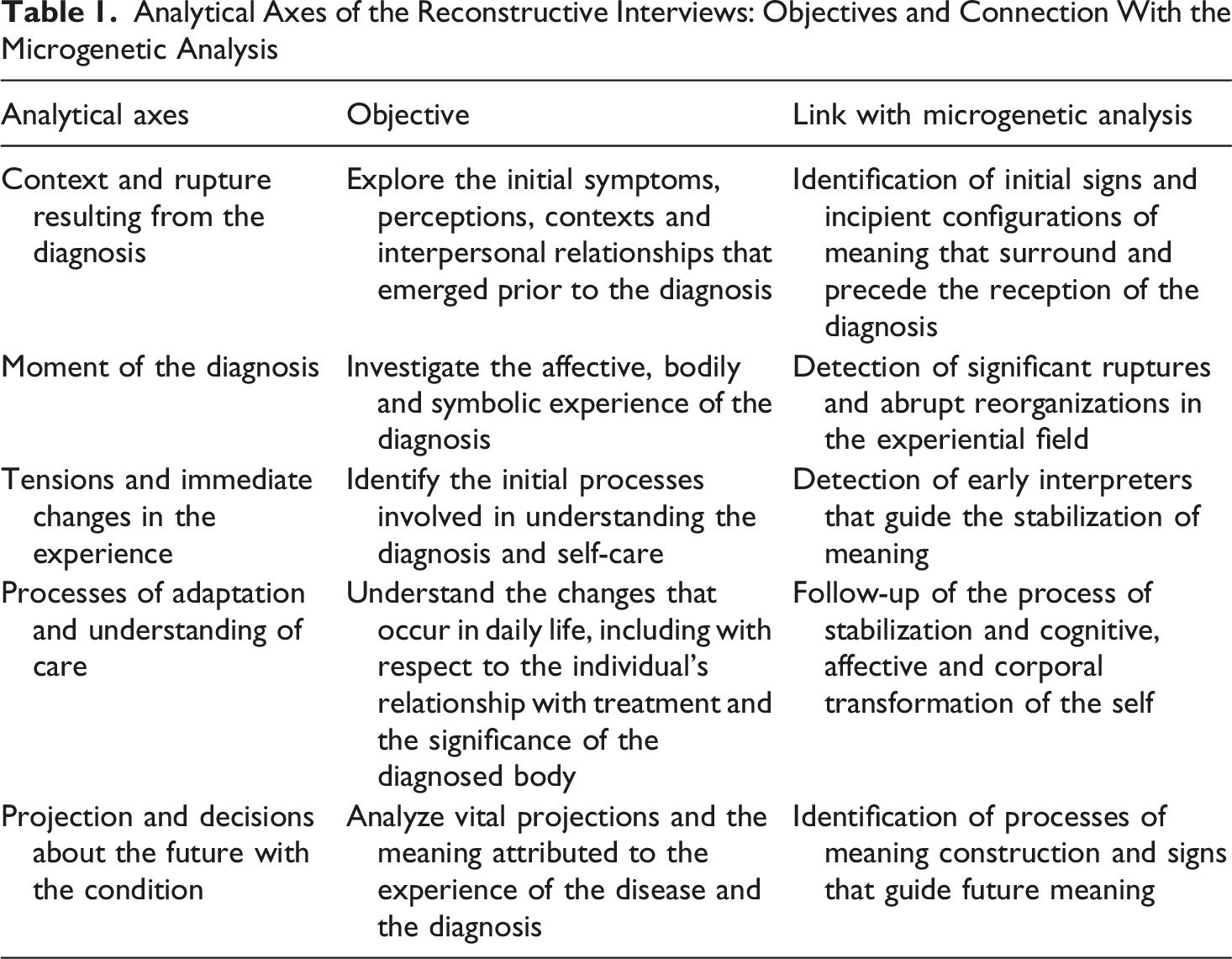
Analytical Axes of the Reconstructive Interviews: Objectives and Connection With the Microgenetic Analysis
Procedure and Data Analysis
After the reconstructive interviews were completed, the material was fully transcribed with particular attention to affective markers in the participants’ speech, such as emphasis, pauses, and silences (De Luca Picione et al., 2019; Lehmann, 2019; Zittoun, 2011). The analysis was carried out within the theoretical framework of the semiodynamic approach using a microgenetic procedure (Salvatore, 2016). This procedure has been conceptualized as a qualitative strategy focused on observing in detail the processes of emergence, transformation, and stabilization of meaning within a specific sequence of time or discourse. It seeks to understand how meanings are configured, reorganized, and stabilized as they emerge, become articulated, and evolve through the subject’s experience (Neves-Pereira, 2019; Reho & Salvatore, 2024; Zittoun, 2009). This procedure was implemented in two complementary phases, characterized by a progressive and dialogical deepening in the interpretation of the data (dos Santos Mammed & Kloetzer, 2023).
Phase 1. Preliminary Reflexive-Dialogical Analysis
The first phase involved an initial interpretive exploration, in which general patterns of meaning were identified. This phase was implemented collaboratively with a researcher with over 15 years of experience in qualitative health research, through a reflexive dialogue that allowed for the comparison of analyses and an enriched understanding of the case. ATLAS. ti software (Version 23) was used as a support tool to organize the material, identify recurring elements, and contrast the content of excerpts, without replacing the interpretive work of the research team. Finally, after individual analyses were conducted in accordance with the degree of investigative experience, joint discussions were held among the researchers. These discussions enabled the team to reach consensus, deepen the affective dimension of the narrated events, and refine the selection of representative excerpts by analyzing their ability to illustrate significant moments in the meaning-making process (Cornish et al., 2014).
Phase 2. In-Depth Semiodynamic Analysis
The second phase focused on a detailed semiotic analysis, guided by the semiodynamic model (Reho & Salvatore, 2024). Key expressions with strong affective content were analyzed to understand how certain meanings shift and become temporarily stabilized. The analytic procedure followed an abductive logic, meaning that it was driven by interpretive inference from particular signs, rather than by pre-established hypotheses. Abduction, as a form of inferential reasoning (Ginzburg, 2013), allowed for a flexible and situated reconstruction of the operations of meaning-making involved. In this context, abductive reasoning proved especially useful for interpreting the affective nuances of experience based on cues such as changes in intonation, silences, and emphases (De Luca Picione et al., 2019; Lehmann, 2019; Packer, 2018).
Ethical Considerations
The study was conducted in accordance with the ethical principles of the Declaration of Helsinki, Colombian regulations (Resolution 8430 of 1993), and the ethical guidelines for the practice of psychology (Laws 1090 of 2006 and 2460 of 2025). The study was reviewed and approved by an expert review board of the University consisting of two evaluators who assessed the ethical conditions and authorized the conduct of the research. This approval was documented in an official approval record. Written informed consent was obtained after explaining the study’s purpose, procedures, and confidentiality safeguards. A pseudonym (“Martha”) was used to protect the participant’s identity, and the data were securely stored. Upon completion of the study, the participant received feedback on the findings.
Results
The case of Martha is presented and analyzed through four key moments in the configuration of meanings around her diagnosis: (1) the transition toward illness, (2) receiving the diagnosis, (3) the search for healing, and (4) the embodied experience of a hypoglycemic episode. (1) The road to diagnosis: Martha “earns the diabetes”
The reception of the T1DM diagnosis is preceded by a context marked by significant social relationships and life transitions. The first relates to the shift from private to public education. During high school, Martha attended a private, all-girls school, characterized by structured routines. This environment, which was characterized by stability and order, stood in contrast to the public educational system that she subsequently entered: a space for men and women with diverse socioacademic backgrounds that features an infrastructure that Martha perceived as disorderly (Quote 1). In this context, Martha indicates that she spends time “obsessing over” her academic performance. This reference to obsessing suggests that she experiences this situation with guilt, thus anticipating the development of diabetes (Quote 2). However, notably, this situation is not limited to the fact that she has developed an obsession. That is, the use of a term should not be confused with the full meaning that the situation offers in this context. Rather, Martha faces a significant change in her position within a new relational system (mainly with respect to her peers). Similarly, she occupies the position of a “facha” among her peers (Quote 3). Being “facha” is a local term associated with upper-class status, refinement, or being ‘too posh’. That is, she becomes positioned as different, occupying a socially advantageous place from which it may be difficult to establish relationships with her classmates.
As Martha undergoes this transition, her personal notion of ‘order’ is brought into question. The contrast between the ‘order’ she associated with her former school and the ‘disorder’ she perceives in the university setting not only reflects her discomfort with the new environment, but also reveals an ongoing process of self-understanding (of where she comes from and who she has been) through which she seeks to reaffirm her identity in relation to others (Quotes 1, 3, and 4).
Within this relational and affective context, Martha situates the emergence of her diagnosis. The way she narrates the shift in routines between school and university is marked by emotional intensity, evident in how she elongates certain words and emphasizes others (Quote 5). At the same time, her account shows how changes in certain practices are configured in relation to other people (such as her engagement with coffee, cigarettes, and staying up late). Affective expressions emerge in various forms. In terms of guilt, for instance, this is reflected in the way she refers to these practices as ‘vice’ rather than simply habits (Quote 6). Feelings also manifest as a sense of losing control—both over herself and the demands of university life—as she puts it: ‘I became incredibly disordered.’ At the same time, they appear as part of a struggle, in which the body becomes the medium for an intense practice, namely, reading
Now, when Martha says, “maybe this is how they manage to endure the reading”, a meaning-in-absence is implied: the “they”: those who can endure it. It is important to consider that in her field of study, reading is not only a demanding academic task but also a key practice for participating in the academic community. As such, it becomes a desirable activity that enables a sense of group belonging and identity formation. Therefore, coffee, staying up late, and smoking are not merely inadequate or unhealthy strategies for coping with academic demands. They are also signs expressing a need to belong to the group and, at the same time, a form of resistance to external pressures (Quote 7). In this process, the body operates as both a limit and a medium through which these tensions become inscribed and shape experience. Nevertheless, even though the situation involves all these elements, Martha seems to locate the cause of her diagnosis within herself (Quote 8). There is a process in which she assumes, with a sense of guilt, that she earned diabetes as a consequence of an ongoing inner struggle, as well as changes in her habits and routines (Quotes 2, 3, 8, and 9):
This case illustrates a situation in which, despite the presence of a meaningful narrative that connects various events, reflects upon them, and communicates them in an articulated way, the process of signification remains open and unfinished (Quote 8). This becomes more apparent when comparing the meaning-in-presence—“I think”, which conveys probability—with the meaning-in-absence: certainty. (2) “Already too diabetic to turn back”: The three hundred and eighty of the diagnosis
Martha’s case shows that receiving the diagnosis does not operate merely as the transmission of medical information to be rationally processed or understood. Rather, it emerges as a meaningful event that entails a reorganization of experience. This moment can be understood as a point of collision, convergence, and tension among meanings that will later, as we will see, be reconfigured and stabilized—allowing Martha to make decisions regarding her treatment, even privileging the expert knowledge of health science (Quote 20).
The expression “way too far gone” (Quote 10), uttered with a tone of astonishment and strain, gives rise to a strong meaning-in-presence—namely, the number “three hundred and eighty” that follows. Taken outside of an interpretive relationship, as if the sign carried meaning in itself, the signification would point merely to an abnormally high blood glucose level. However, for Martha, the number becomes a sign that reorganizes the meanings associated with the body—now marked by a difference that no longer allows a return to a state of health. Here, the number functions as a sign that delineates a before and an after. Moreover, it reconfigures what it means for her to inhabit her body—not merely as someone who had been experiencing symptoms and feeling unwell, but now as “a diabetic person”. The situation becomes more complex when considering the temporal coincidence with her birthday (Quote 11), which introduces a tension among three simultaneous meanings: the celebration of life, the beginning of an altered life, and the beginning of an altered life at a moment symbolically charged with future projection and autonomy (at 18, the age that marks legal adulthood in Colombia). The affective tone —marked by crying and the emotionally emphasized phrase “everything was the last”—suggests an affective operation that mobilized her experiential field. Provisionally, Martha found herself in a position of imminent loss and closure of possibilities: sugar, champagne—that is, everyday pleasures—as well as restrictions on movement, agency, and decision-making in the world, all of which are typically associated with reaching adulthood.
Martha’s case illustrates the emergence and gradual stabilization of meanings that unfold over time. Although there is an attempt to assimilate what she has experienced, the body has not yet been fully integrated as a diagnosed body (Quotes 11 and 12). Later, meaning-making gives rise to implications regarding the lifelong need for injections, which entail a redefinition of both the body and everyday life (Quote 12). Eventually, a certain stabilization of the experience becomes visible, as a process of meaning construction takes place in which Martha connects past events and develops an explanation—framed in terms of adaptation—to convey her experience of living with Type 1 Diabetes (Quote 13). A notable aspect here is that Martha turns to a general category: not that of herself as a person, but of herself as a human being. That is, she appeals to a broader symbolic framework, possibly to reduce the sense of exceptionalism tied to her individual condition and to elaborate a viable way of coexisting with the illness. (3) The hope in pancreatic recovery
Following the diagnosis, a reorganization of Martha’s field of meanings emerges, orienting her actions toward the search for a cure with the aim of returning to a pre-diagnostic state.
This search appears as an active meaning-making process in which Martha reinterprets what it means to inhabit an altered body. The expression “make my pancreas work the way it used to” suggests that the pancreas functions as a condensed sign of non-normality: not only in its physiological role of secreting insulin to regulate blood glucose levels, but also as a representation of a way of life that Martha wishes to restore (Quote 14). This attempt at restoration is enacted through actions guided by an affective and symbolic logic of dietary detoxification, seeking to reintegrate the body within a network of meanings that allow her to feel like someone who can once again be “healthy” by being “non-intoxicated” (Quote 15). The strength of this emerging meaning is such that it transforms her eating practices to the extent that Martha relinquishes pleasurable sensory and bodily dimensions (Quote 16).
The process of seeking a cure begins to reveal to Martha how the illness functions, particularly after undergoing a personal crisis that involved hospitalization. This moment represents a turning point, partly due to the reprimand she receives from the healthcare staff, but more importantly for two key reasons. First, it constitutes a novel experience for her, for which she has few prior meaning structures to stabilize or anticipate what is happening. Second, it initiates a cognitive process of meaning-making, involving the association between insulin and food intake (Quote 17).
Later on, Martha’s case illustrates the coexistence and tension between biomedical knowledge and other forms of understanding the illness, which she refers to as “esoteric” (Quotes 18, 19, and 20). The oscillation between “holding on with faith” and “letting go” (Quote 18) enacts a dual affective semiosis, in which meanings alternate between hope and hopelessness and are reformulated over time, ultimately enabling Martha to reach a more stable decision regarding treatment (Quote 20). Her use of the expression “most definitely” (Quote 19) conveys not only empirical certainty but also an affective mark of disillusionment, in which the idea of a cure—conceived as an absent sign—loses plausibility. Due to space limitations, we cannot fully analyze the entire process of Martha’s search for alternative treatments. However, we can show that this search leads to greater proximity to biomedical knowledge and contributes to a more stable experience of illness. Rather than a complete rejection of the meanings associated with what she calls “the esoteric things”, this dimension becomes complementary to formal medical knowledge—not as a path to healing, but as a way of connecting with broader dimensions of existence (Quote 20). (4) The experience of the “downer” and the opening of the pores
The crisis triggered by a hypoglycemic episode illustrates how Martha gradually constructs the semiosis of insulin and the diagnosed body. This crisis revolves around a sweet food she particularly craved—specifically, a turrón (nougat).
Martha constructs a creative negotiation in which she transforms the meaning of insulin administration prior to the crisis. It ceases to function solely as a medical regulation tool and becomes a sign that articulates her agency in response to normative care demands. Rather than adopting a dichotomous logic of obedience or disobedience, increasing the insulin dose before eating the nougat allows her to experience a sense of freedom in her decisions without fully breaking away from the constraints of her condition (Quote 21). This reconfiguration introduces novelty into the process of semiosis, as it momentarily alters the interpretive framework through which Martha organizes her experience. It opens a space of possibility in which her desire for freedom is not experienced as an absolute rupture. In this way, she actively appropriates the demands of her illness. During the crisis, by contrast, Martha’s experience reveals a disruption in her sense of agency as it emerges from the body. The phrase “it wasn´t responding” suggests a perceived distance between her identity and her body (Quote 22). Insulin mediates this relationship and acquires a meaning that places tension on her identity—positioning her simultaneously as a patient who seeks control and freedom within her own body, and as a person who must respect the administration of the hormone (Quotes 22 and 23). Following the crisis, Martha’s case reveals a dual meaning of respect and fear toward insulin. The expression “My God, what a horrible thing I felt!” illustrates how insulin temporarily becomes an object of fear (Quote 23).
Martha’s experience illustrates the embodied unity of cognition and affect. As can be seen, she uses technical and procedural language to describe the calculation of insulin doses and their bodily effects. She organizes this experience around temporal and causal elements, which enables her to construct meaning from the crisis event (Quote 24). At the same time, this calculation is infused with affective experience. She not only reconstructs the episode but also resignifies it as a form of learning about her body and the illness. In this way, her understanding of “peaks” and “downers” becomes a foundation she can eventually draw on to manage diabetes in the future. Moreover, the case also reveals the intensity of affect as expressed through bodily terms: the profuse sweating and the sensation of her pores opening up become signs of exposure and vulnerability (Quote 25). It is as if the body were speaking and being interpreted by Martha, forming a bridge between what is lived and what can be represented through communication and thought. If the body functions as a point of mediation between the self and the world, the opening of the pores might signify a moment in which the boundaries between the internal and the external are perceived as more porous, intensifying the connection with both dimensions. The intensity of affect, evident in the words she chooses (“buckets,” “every single pore”), operates as a sign that expresses, articulates, and organizes her perception of the crisis (Quote 25). In this sense, affect is not merely a reaction to the biological effects, but a force that mediates Martha’s relationship with her body, her treatment, and her sense of self in relation to the world.
Discussion and Conclusions
This study contributes to an emerging strand of qualitative health research concerned with how the body operates as an active source of meaning in the specific context of adults diagnosed with T1DM. This perspective remains largely underexplored in relation to this chronic condition and opens new pathways for analyzing the diagnostic experience beyond thematic descriptions or representational frameworks of meaning-making. The discussion has been structured in three main dimensions. First, the moment of diagnosis is presented as a life-altering event that involves a symbolic reconfiguration of personal experience. Second, the lived body and affective dynamics are shown to operate as active forces in the organization of meaning, particularly through hypoglycemic episodes. Third, attention is given to the processes through which meaning becomes relatively stabilized over time and how this affects the ways in which individuals manage and care for their illness. This analytical strategy makes it possible to return to the research question, which sought to understand how meanings about the diagnosis of T1DM emerge, transform, and stabilize.
The moment of diagnosis is often regarded in clinical practice as the formal entry point into therapeutic intervention. However, in Martha’s case, it does not merely label a biological alteration; rather, it involves a reorganization of what the diagnosis comes to mean for her, based on what she feels and notices in her own body. This case illustrates that, initially, there is only a partial integration of the diagnosis as something meaningful, which nonetheless triggers an intense emotional response (crying) and a sense of loss regarding pleasurable elements (such as sweet foods and alcoholic beverages). Subsequently, driven by an active search for a return to her previous state of health (the desire to reverse the illness by restoring pancreatic function), she experiences a hypoglycemic crisis that contributes to stabilizing the experience of the diagnosis. This occurs by enabling her to grasp how the treatment works and what it personally entails to endure a severe hypoglycemic episode. Following this, the process of meaning-making leads her to opt for a form of treatment more aligned with biomedical knowledge. This finding resonates with the notion of rupture, according to which destabilizing events such as disease diagnoses interrupt ongoing processes of meaning-making and demand the construction of new symbolic mediations, learning processes, and resources (Zittoun, 2006, 2023). Similarly, it echoes the understanding of illness as a moment in which individuals lose both the “map” and the “compass” that once oriented their lives, facing problematic situations related to desire and control (Frank, 2013; Kleinman, 2020). However, what this study adds to previous work is a more detailed account of the temporal unfolding of meaning, allowing us to observe that receiving a diagnosis does not operate as an immediate or univocal symbolic act, but rather as a semiotic chain whose effects develop over time.
Hypoglycemic episodes, in turn, trigger more lasting reorganizations of meaning. The intensity of these episodes leads the patient to re-signify her treatment, not only through external instructions on how to manage her illness, but through a felt, embodied experience that imposed itself as meaningful, thus turning the body into an active semiotic field. This finding aligns with a previous study in which the authors reported to the academic and scientific community that the initial sensation of physical distress -that is, the critical drop in blood glucose levels- serves as a starting point for a meaning-making process that extends to core aspects of the individual’s life. Moreover, the hypoglycemic symptom, understood as a set of experiences capable of destabilizing the subject, should be considered in evaluating how one’s sense of self is affected (Cleves et al., 2025). The analysis of hypoglycemic crises in this case also resonates with semiotic approaches that emphasize how signs are integrated within sign networks and acquire transformative functions with respect to the ontological status of objects (Tateo, 2018, 2024). However, the present case adds a bodily dimension that is often absent from such accounts, allowing for a better understanding of the transformative power of bodily signs. In this sense, the case illustrates that hypoglycemic bodily signs are not neutral alarms; rather, they reorganize the connection to and sense of agency one feels with respect to the body, while also transforming the meaning of insulin-based treatment; imbued with both respect and fear. From the perspective of the semiodynamic model, this moment exemplifies the tension between Signification in Presence (the immediate and pressing need to interpret the hypoglycemic crisis) and Signification in Absence (what the bodily crisis means to the subject and how it gradually shapes their perception of the future). Understanding signification in this way makes it possible to see how it becomes a vector that guides treatment decisions beyond the mere avoidance of physiological alarm states (Salvatore et al., 2024).
The progressive stabilization of meaning around the diagnosis is particularly illuminating when contrasted with many qualitative studies that tend to organize patients’ experiences through relatively fixed themes or narrative typologies, such as those of restitution, chaos, or quest (Due-Christensen et al., 2018; Frank, 2013; Helgeson, 2021; Overgaard et al., 2021; Walker & Litchman, 2021). While these approaches have been valuable in making patients’ subjectivity visible, they may also produce a static image of meaning by failing to adequately address how meaning is dynamically configured through the body and affect in concrete situations. Similarly, some works have proposed that the social metaphors circulating around illness -though embodied and affectively experienced- tend to shape the experience from the outside, often simplifying or stigmatizing it (Sontag, 1996). In contrast, the microgenetic analysis of Martha’s case demonstrates that meanings are not passively imposed, but are actively reorganized through embodied experience. In this process, hypoglycemia is configured as a loss of personal agency and a dissolution of the boundaries between body and environment, producing a sense of vulnerability that grounds new understandings of the body. Once this meaning becomes consolidated, it begins to guide practical decisions related to treatment. That is, such stabilization allows for greater structuring of the experiential field -yet remains dynamic- making it possible to evaluate specific treatment options (such as insulin patches or sublingual insulin) as viable responses to perceived fragility. In this way, the stabilization of meaning organizes experience and configures the horizon of possibilities from which a person decides, acts, and relates to their illness.
It is important to highlight that the proposed analysis opens new pathways for qualitative research in health, especially when the aim is not merely to document suffering or adaptation to illness. The findings suggest that a person’s actions in relation to their diagnosis and treatment -what they do, avoid, or prioritize- are semiotically mediated by a dynamic and embodied network of meanings. In this sense, the microgenetic approach enables a processual understanding that may enhance the sensitivity of clinical practice, allowing professionals to better recognize moments in which interventions resonate affectively, or in which symbolic reorganizations are taking place beneath the surface of observable behavior (Munion et al., 2020; Romero-Castillo et al., 2022; Turton et al., 2023). The analytical tools used here may be adapted to other chronic conditions that require constant bodily attention, affect regulation, and ongoing social negotiation. From a clinical perspective, rather than attributing non-adherence or lack of engagement with treatment to informational deficits, these findings invite greater attunement to the ways in which patients are immersed in dynamic fields of meaning that shape what feels possible, desirable, or threatening in relation to the diagnosis and its treatment (Lv et al., 2021; Raymaekers et al., 2021). Finally, these results must be considered in light of their scope. By focusing on a single case, the study does not aim to represent the full range of possible experiences in T1DM, but rather to offer a precise and in-depth analysis of a singular process. Nonetheless, the analytical density afforded by the microgenetic approach offers a pathway for the progressive construction of theory, by generating interpretive hypotheses that may be explored in future research, whether through additional case studies or through comparative analyses of other systematically documented cases. Furthermore, longitudinal studies -including the precise moment of diagnosis- are needed to observe in greater detail how the meaning of the diagnosis is initiated and transformed over time. In this regard, a fertile field of inquiry remains open for qualitative health research to provide a richer understanding of how the meaning of diagnosis evolves in patients’ lived experience.
Footnotes
Acknowledgments
The authors would like to thank the participant, Martha, for generously sharing their experiences.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.