
Abstract
Introduction
Chronic wounds which do not heal as expected, are common in residential aged care homes (RACHs). While specialised wound care is essential for improving outcomes, access is challenging in RACHs. Emerging virtual interventions are known to improve access to wound care, but little is known about use in this setting. This scoping review identifies and maps virtual wound care use in RACHs.
Methods
An electronic search of Medline, CINAHL, Embase, AgeLine, IEEE Xplore, ACM digital library and clinical trial registries was conducted from database inception to March 2026. Studies were screened and data extracted by two independent reviewers using a reviewer-developed tool.
Results
Of the 17 included studies, a combined model of telehealth and store and forward was most frequently used (n = 9). Virtual wound care was used for both diagnosis and management (n = 15) and commonly delivered by teams of clinicians (n = 8). Included studies demonstrated wound care could be delivered safely and facilitated clinical decision-making. Acceptability of virtual wound care by residents, families, staff and other care providers was high. Reliable internet, stable workforce and adjunct in-person care were enablers to virtual interventions. Lack of training participation, workforce shortages and technology limitations were perceived barriers to virtual wound care.
Conclusions
Current evidence indicates that virtual wound care is being used in RACHs though it remains under investigated. Addressing workforce, training, and technology barriers can support broader implementation of virtual wound care and improve chronic wound outcomes for aged care residents.
Review registration
Open Science Framework https://osf.io/j97bt
Introduction
Chronic wounds that fail to progress through the normal stages of healing are increasingly common 1 and associated with substantial health and socio-economic burden. 2 Older people in residential aged care homes (RACHs) are particularly vulnerable to developing chronic wounds.3,4 Access to wound specialists can improve wound outcomes 5 but is a persistent challenge in RACHs. 6 Virtual wound care, including telehealth and store and forward technologies, can overcome access barriers and have been shown to be safe and effective. 7 Despite their potential benefit and significant increase in use in recent years, 8 little is known about how these technologies are used in RACHs or the factors influencing implementation.
Chronic wounds are common, affecting between 1.9% and 2.5% of adults.9,10 Common wound types include diabetic, arterial and venous ulcers and pressure injuries. 11 Chronic wounds are characterised by an absence of systematic and predictable healing 12 and can cause infection, sepsis and limb amputation. 13 In the United States, it is estimated over 10.5 million people experience chronic wounds 14 costing approximately US$25 billion annually. 13 Global estimates from 2022 propose even higher wound care expenditure at $148.65 billion in the United States, followed by China ($42.78 billion) and Japan ($22.91 billion Purchasing Power Parity) 15 with costs expected to grow. 16
Older people are disproportionately affected by chronic wounds due to comorbidities such as diabetes and peripheral vascular disease, increasing frailty and skin vulnerability.17,18 In RACHs, a home-like environment where older people receive personal and clinical care, 19 chronic wounds present a significant burden of disease. 4 Specialised wound care can reduce delays and improve healing outcomes 20 but is often limited in this setting due to workforce and resource shortages, variable wound care expertise among staff and fragmented access to expert care.21,22 Lack of access to specialist wound care affects the timeliness and quality of wound care and poor wound outcomes remain one of the most common complaints in aged care. 23
One solution to increasing access to specialist wound management is virtual care. Virtual care refers to healthcare delivered remotely using information and communication technology services 24 and includes telehealth (phone or video), store and forward (image capture and electronic transmission), remote patient monitoring and apps. 25 Virtual care may be delivered synchronously as real-time interactions between clinicians and patients, or asynchronously where clinicians review and interpret patient data at a later time. 26 Virtual wound care has demonstrated safety and effectiveness in wound healing9,10 and enables access to specialist wound care while reducing travel burden and costs in community and hospital settings.27,28
Significant growth in virtual care has been associated with major technological advances such as high-definition videoconferencing, remotely accessible medical devices and artificial intelligence (AI) and accelerated significantly with the COVID-19 pandemic.29,30 Despite this, few studies have been undertaken in RACHs where residents are particularly vulnerable to chronic wounds and face major access barriers. 31 This scoping review maps global evidence on virtual wound care in RACHs, detailing care types, usage patterns, and key enablers and barriers to use.
Methods
Protocol and registration
The review was conducted in accordance with JBI (formerly known as Joanna Briggs Institute) methodology for scoping reviews32,33 and an a priori protocol. 34 It was registered in Open Science Framework [https://osf.io/j97bt] and reported using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines. 35
Eligibility criteria
Population
Eligible studies involved adult patients (aged 18 years and over) with chronic wound living in RACHs. The review encompassed all chronic wounds which had failed to heal in a timely manner, often greater than 4 weeks and regardless of underlying aetiology.
Concept
The review considered all virtual wound care with particular focus on intervention type and frequency and associated enablers and barriers to use. Virtual care modalities included one or more of: telephone or video telehealth, remote monitoring, store and forward clinical information exchange, digital platforms, and website and mobile apps. 25 Frequency of care referred to how often the virtual care was delivered to recipients.
Context
This scoping review considered studies in RACHs, also known as nursing homes, long-term care, skilled nursing facilities and residential aged care facilities, across diverse geographical locations.
Types of sources
Quantitative, qualitative and mixed methods study designs were eligible for inclusion. To identify completed but unpublished, ongoing and planned virtual wound care trials, the World Health Organization International Clinical Trials Registry Platform (WHO ICTRP), US National Institutes of Health Ongoing Trials Register (ClinicalTrials.gov) and the Australian and New Zealand Clinical Trials Registry (ANZCTR), were searched as grey literature sources. Conference abstracts, unpublished works, and text and opinion papers were not considered for inclusion as they were unlikely to contain adequate information about the intervention for complete data extraction.
Search strategy
The search strategy was developed by one author (HR) with the assistance of an academic librarian. An initial limited search of MEDLINE (OVID) and Scopus was undertaken to identify articles on the topic. Text words contained in titles and abstracts and index terms used in relevant articles were used to develop a full search strategy for MEDLINE (OVID), CINAHL (EBSCO), Embase (OVID), AgeLine, IEEE Xplore and ACM digital library. The search strategy combined keywords and subject headings for the population e.g., “chronic wounds”, concept e.g., “virtual care” and context e.g., “residential aged care” and was adapted for each included database. The reference lists of all included sources, grey literature and systematic and scoping reviews on the same or similar topics, were screened for additional studies. The literature search was conducted up to 14 March 2026.
Studies published in French, German, Spanish, Portuguese, Chinese, Japanese or Thai were translated using translation engine DeepL Translate (Cologne, Germany). Translations were not checked due to financial constraints. No limitations were placed on date of publication. The search strategies for each data source can be found in Supplemental material A (Tables A1 and A2).
Study selection
All identified citations were collated in EndNote 21 (Clarivate Analytics, Pennsylvania, USA) and exported to Covidence (Veritas Health Innovation, Melbourne, Australia) for screening. The eligibility criteria were piloted by screening a small number of articles. Following the pilot test, titles and abstracts were screened against the review inclusion criteria by at least two independent reviewers (HR, MBJ and GL). Potentially relevant sources were retrieved in full and assessed against the inclusion criteria by at least two independent reviewers (HR, MBJ, AB, MM and GL). Reasons for exclusion of sources of evidence at the full text stage were recorded and reported. Disagreements between reviewers were resolved through consensus discussion, or with additional reviewer or reviewers from the research team.
Data extraction
Data was extracted from included papers by at least two independent reviewers (HR, MBJ, AB, MM and GL) using a data extraction tool developed by the reviewer based on the JBI template. 32 The draft data extraction tool was piloted, modified and revised as necessary during the process of extracting data from each included evidence source. Characteristics of included studies were reported including author, year, country of publication, care types, usage patterns, and key enablers and barriers to use. Where required, authors of papers were contacted by email up to three times over 3 months to request missing or additional data.
Summary of included publications.
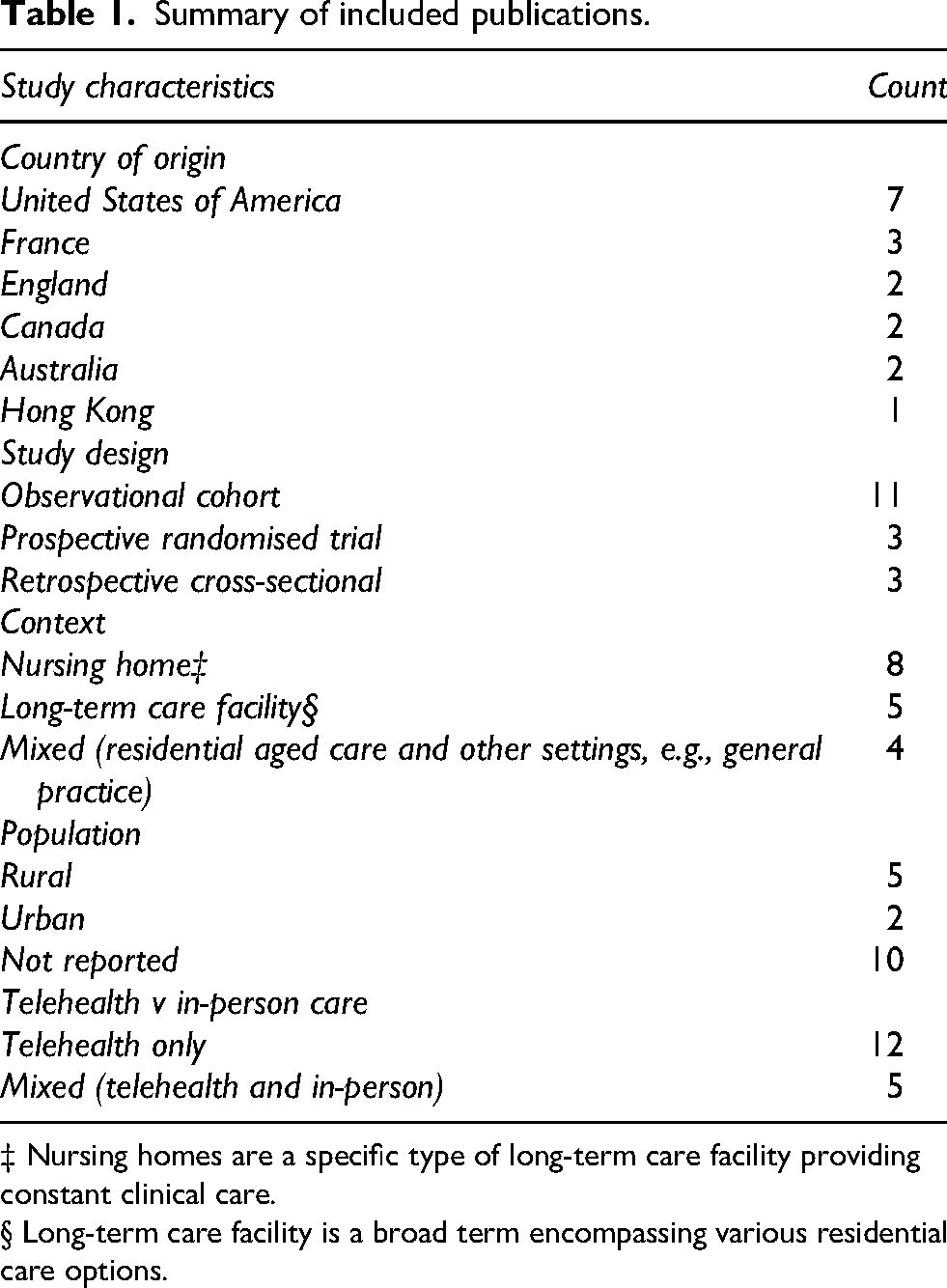
‡ Nursing homes are a specific type of long-term care facility providing constant clinical care.
§ Long-term care facility is a broad term encompassing various residential care options.
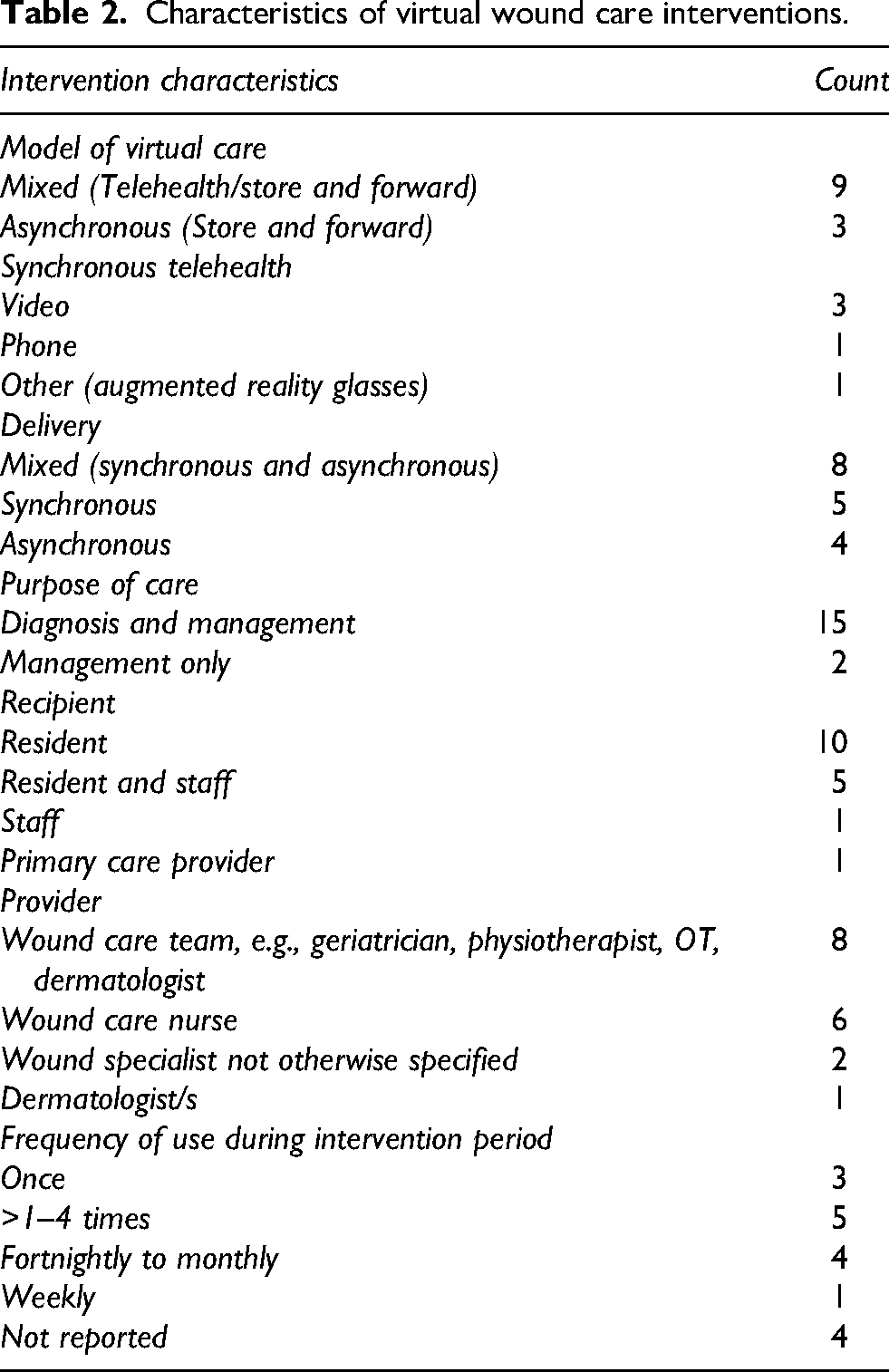
Characteristics of virtual wound care interventions.
Results
The database and grey literature search identified 477 data sources. The database search identified 313 studies with 265 studies remaining after duplicates were removed. Following title and abstract screening, 24 full-text papers were retrieved and nine studies were excluded based on the eligibility criteria (Supplemental material B, Table B1). An additional 164 studies were identified through grey literature searches including two from citation screening, 143 from Clinicaltrials.gov, 15 from ANZCTR and four from WHO ICTRP. Four studies were retrieved for full-text review with two remaining based on eligibility criteria (Supplemental material B; Table B2). A total of 17 studies were included in the review (Figure 1). 36
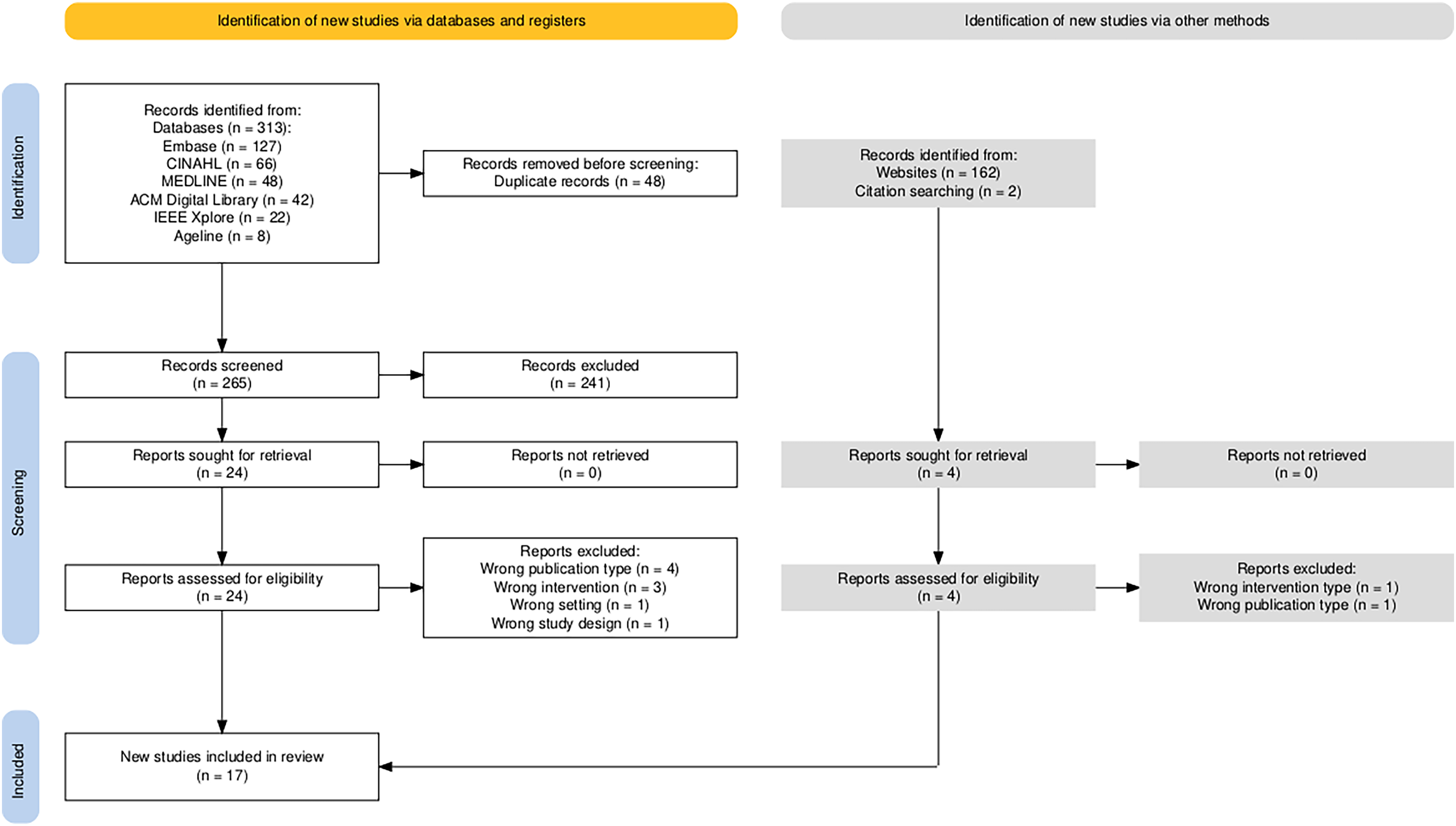
PRISMA flow diagram.
Study characteristics
Of the 17 included studies, publication date ranged from 2001 to 2025 (Supplemental material C, Table C1). Figure 2 illustrates the frequency of publications by year.
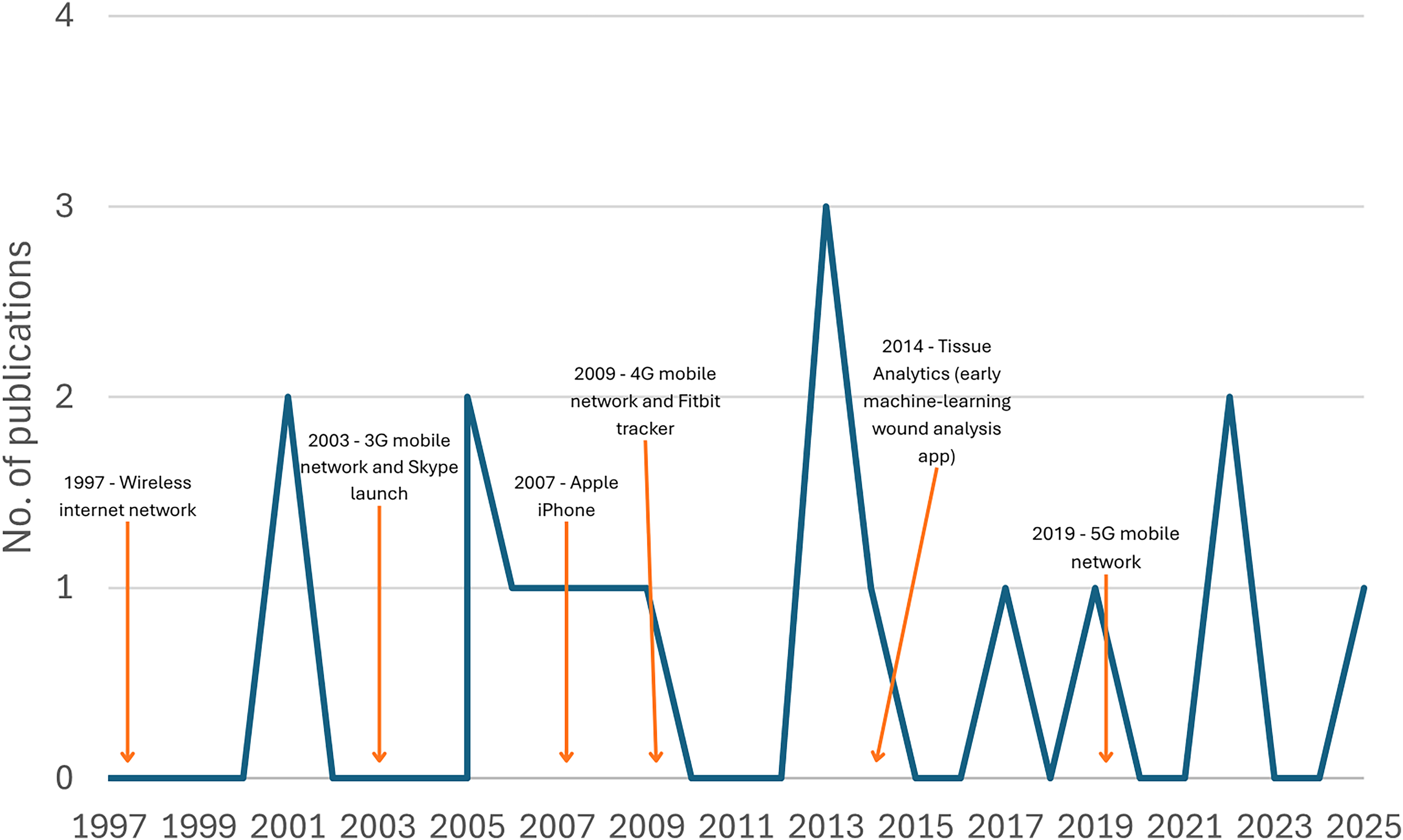
Included papers by years of publication and major technological advances†.
Most included studies were observational cohort designs (n = 11)37–47 followed by prospective randomised trials (n = 3)48–50 and retrospective cross-sectional analysis (n = 3).28,51,52 The United States was the most common country of origin (n = 7)39–44,48 followed by France (n = 3),45,46,52 England (n = 2),49,51 Canada (n = 2),47,50 Australia (n = 2)28,37 and Hong Kong (n = 1). 38 Two studies were translated from French to English using DeepL Translate (Cologne, Germany). Five studies were conducted in rural settings,28,37,41,42,46 two in urban40,47 and setting was not reported in 10 studies.38,39,43–45,48–52 Table 1 summarises the characteristics of included studies.
Synthesis of results
Types of virtual wound care
A combination of telehealth and store and forward was the most used type of virtual care (n = 9; Table 2).28,38–40,45,46,48,50,52 In three studies, asynchronous store and forward alone was used37,49,51 and synchronous telehealth was used in five studies (phone n = 1, video n = 3, other n = 1).41–44,47 Most virtual care (n = 15)28,37–43,46–52 was used for both diagnosis and management of chronic wounds and two for wound management only.44,45 In most included studies, the recipients of the intervention were aged care residents (n = 10)39,41–43,45,46,48,49,51,52 or residents and staff (n = 5)28,37,38,40,44 and care was mostly provided by wound care teams (n = 8)38,39,42,45,47,48,50,52 which included geriatricians, physiotherapists, occupational therapists, dermatologists and wound care nurses. Several included studies used a combination of virtual and in-person care.39,42,43,48,50
Frequency of use
Frequency of use of virtual wound interventions ranged from once (n = 3)39,43,48 in the study period to weekly (n = 1). 49 Four interventions were used one to four times28,40,46,51,52 and four were used fortnightly to monthly.37,44,45,50 Frequency of use was not reported in four studies.38,41,42,47 Two studies reported the length of time required for the intervention which ranged from 30 minutes 44 to 1 hour. 45
Outcomes
Included studies demonstrated that wound care could be delivered safely,51,52 was associated with favourable clinical outcomes42,49 and facilitated clinical decision-making.40,42 Overall, there was high acceptability of virtual wound care by residents and families 41 along with staff 38 and other care providers. 47 Studies assessed a broad range of outcomes including clinical outcomes, patient and staff satisfaction and costs.
Clinical outcomes
In virtual wound care studies where clinical outcomes were assessed, decreased wound surface area was reported, 51 as well as accelerated healing outcomes and earlier recognition of wound deterioration. 49 Pressure injuries, a common wound type in RACHs healed in 60% of residents in a study of 579 participants, 51 but showed no significant difference when compared with standard care in a smaller study. 50 Dobke et al. 39 reported that wound management plans developed virtually compared with in-person had a sensitivity of 94%, specificity of 99%, and positive predictive value of 94%. In only two cases of the 120 assessed, the plan developed during the in-person consultation differed significantly from initial management, but appropriate care was not delayed. 39
Patient satisfaction
Virtual care was viewed favourably by patients and families, who appreciated timely remote access to wound care expertise and reduced travel times.38,41,43–45,52 Specialist wait times were reduced from several months to 3 to 14 days with the virtual intervention in two studies.28,38 Residents in one study were more satisfied with virtual care than in-person care (55% vs. 40%). 43 In another study where in-person and virtual care were used, duration of subsequent in-person consultations was reduced and patient acceptance of recommended management was reported to improve. 48 Chan et al. 38 showed most residents (96%) developed rapport quickly, could ask questions, found the image and sound quality acceptable and would participate in telehealth again. 38 Virtual wound care was shown to be well accepted by patients with dementia, 41 but resident participation in telehealth consults was limited in one study due to hearing and vision issues. 43
Staff satisfaction
RACH staff reported virtual wound care interventions increased local confidence and perceived expertise in wound care37,40,41,44,45 and decreased professional isolation by fostering partnerships between tertiary and aged care settings.38,52 Staff were reassured by access to wound care experts who could coach and teach during the virtual care intervention.41,49 Nurses and wound care experts reported feeling comfortable making decisions and following orders based on computer-based exchanges of information 40 and virtual care was perceived to support the ability of local staff to provide improved care.43,44 Primary care physicians who accessed virtual services for wound care advice also reported strong satisfaction and their concerns were adequately addressed, avoiding acute care transfer in 46% of cases. 47
Costs
Seven included studies evaluated costs associated with virtual wound care in residential aged care settings.28,38,44,45,49,50,52 A Canadian study reported reduced direct costs by an average of CA$650 per resident through discontinuation of expensive non-evidence-based treatments. 50 Reductions in dressing change frequency were also associated with cost-savings.45,49 Additional cost savings included fewer specialist referrals,45,49,52 hospitalisations,44,45,47,52 emergency department presentations 52 and ambulance use. 44 Indirect costs such as transportation, escorts and staff time were also reported to be reduced through use of virtual wound care28,38,45 with one study demonstrating a US$650 and 3-hour saving per clinic visit. 44 In one Australian study, virtual wound care was associated with reported savings of an average of AU$507.49 and 444 minutes per round trip for those living more than 201 km from specialist centres. 28 Virtual wound care also allowed staff additional ‘time to care’ which was perceived as a potential cost benefit. 37
Enablers
High-quality, streamlined training supported by appropriate resources was reported to be helpful to staff, ensured adequate quality wound images and enabled virtual care. 40 Kaylor et al. 41 demonstrated that augmented reality glasses (ARG) training required less than 1 hour to ensure competent use. Only basic orientation was needed to ensure high-quality wound images 40 and image quality obtained in the included studies was generally sufficient to enable use of virtual wound care. 44 Staff reported that ‘on the job’ training helped them use and integrate the intervention once familiar with the equipment. 49 Prior to implementation, rapid testing and refinement at pilot sites and identification and implementation of local solutions were also reported to aid integration of virtual care interventions. 47
User interfaces (UI), the point of interaction between staff and technology, 53 which were intuitive, visually appealing and easy to navigate, were reported as enablers of virtual wound care. 40 Staff reported that live video enabled the wound to be seen from multiple angles, ensuring immediate feedback was provided by wound experts and active participation of the patient and family in the consultation. 44 Some staff found the virtual wound care intervention to be more efficient and less time-consuming than expected and staff enjoyed working with each other virtually. 40 While virtual care was reported to be an acceptable stand-alone approach for wound care, having the option for a combination of in-person and virtual care was reassuring to staff. 44
Barriers
Several included studies reported that virtual wound care interventions required additional time for training and use37,40,45 and extra personnel 44 which limited implementation. Additionally, insufficient managerial support 50 and lack of wound care supplies37,50 hampered uptake of virtual care interventions. Staff resistance was reported in several studies and was attributed to uncertainty regarding new wound care approaches38,40,52 and wariness of time required to use the intervention. 40 Intervention integration into routine care was also impacted by high staff turnover and workforce shortages leading to a loss of trained staff.37,50 In one study, only 47% of the healthcare providers trained to use the software at the beginning of the trial were still employed when the trial ended 8 months later. 37 Prolonged periods of understaffing at several participating sites also limited capacity to implement and sustain use of the intervention. 37 Workforce challenges were addressed in some studies through orientation of new staff to the virtual intervention. 40 Implementation and integration were reported to be facilitated when management and external wound clinicians were familiar with the intervention. 40
Lack of familiarity with the technology,40,42 insufficient digital literacy 40 and inadequate training were cited as barriers to delivery of virtual wound care.40,44,52 Inadequate wound image quality was noted in several studies44,49 along with the inability of remote staff to palpate, probe and detect wound odour. 43 Limitations in wound margin and drainage assessment 41 and conveying wound depth, size and fine details were also reported in two studies though these studies were more than 20 years old and substantial technological advances have since been achieved in photographic quality.39,42 The availability of an on-site team member provided valuable input to the assessment and management of the wound. 43 Poor sound quality and inadequate ambient lighting 42 along with resident vision and hearing limitations 43 affected participation in the consultation. These challenges were addressed with larger and better positioned screens and using a private space where the call volume could be maximised. 43 Issues with third generation (3G) wireless technology 49 and difficulty moving telehealth equipment 38 were also cited as limitations to virtual wound care.
Discussion
Summary of evidence
This scoping review demonstrated that a combination of telehealth and store and forward technologies was most often used for virtual wound management in RACHs. Virtual wound care was used for diagnosis and management and commonly delivered by wound care teams which included nursing, medical and administrative staff. Key reported benefits of virtual wound care interventions included reduction in specialist wait times and prompt access to wound care.28,38 Staff and patients reported mostly positive experiences.38,39,41,42,44–46 Similar to previous work in other settings,54,55 virtual wound care in residential aged care performed well when compared to in-person care38,39 and offered time and cost savings.28,39,44,45,50,51
Included studies reported virtual wound care implementation was hindered by the perceived requirement for additional time, personnel and resources.37,40,44,45,50 Insufficient managerial support and high staff turnover also affected implementation in some sites37,50 but was addressed through streamlined, on the job training and orienting new staff to the intervention.40,49 Local piloting and problem-solving prior to implementation 47 along with managerial and remote wound clinician support 40 also enhanced intervention implementation. Limitations of the technology to comprehensively assess the wound were reported to be managed by working with on-site staff 43 and the use of in-person consults when necessary. 44
Implementation considerations
The current review highlights a significant gap in implementation and evaluation of virtual wound care models in RACHs with only 17 included studies. Despite reported evidence of improved wound outcomes, enhanced access to specialists and potential cost savings associated with virtual wound care, there remains limited research in this setting. With telehealth use accelerating since the COVID-19 pandemic and an expanded understanding of barriers and enablers to implementation, 56 these learnings may be applied to virtual wound care interventions in RACHs to overcome key challenges and support sustained use.
User-related factors including lack of knowledge or awareness and insufficient digital literacy are frequently cited barriers to implementation of virtual care. 57 This is exacerbated in rural and aged care settings by staff shortages and high workforce turnover contributing to loss of telehealth knowledge, skills and confidence.58,59 Evidence indicates that tailored, ongoing training and support reduces resistance to implementation of virtual care interventions and can improve uptake. 60 Specifically, continuous learning environments that focus on telehealth knowledge, skills and competencies as well as associated policies and workflows, are needed to ensure robust uptake and implementation.60,61 Additionally, engagement with external stakeholders, such as general practitioners and wound care experts, can enhance integration of virtual care models within the broader health system. 62
Technology-related factors such as useability, reliability and compatibility with workflows present further challenges to virtual care implementation. As noted in the current study, intuitive and easy to navigate UIs enabled virtual wound care 40 but poor infrastructure and connectivity was a barrier to use. 63 Included studies reported use of video enhanced wound care 44 but video telehealth is frequently underused in RACHs,61,62 particularly rural RACHs where telephone remains the main mode of telehealth consultation with primary care providers. 64 RACH staff and external health care providers require ongoing support to transition from phone to video telehealth 62 to optimise wound care provision and ensure the digital divide between rural and urban aged care residents does not widen.64,65
Lack of managerial support and resources was a reported barrier to implementation of virtual care in the current study. This aligns with contemporary literature indicating that strong leadership enhances resource allocation and readiness for change. 60 Workplaces with innovative, collaborative cultures are also more receptive to digital solutions and iterative, feedback-driven implementation strategies with high levels of staff engagement improves adoption and sustains use. 60 Such strategies are likely to help to address staff resistance to implementation of virtual wound care which was reported in several included studies and may offer the additional benefit of improved staff retention and satisfaction.
Strengths and limitations
This review has several strengths. It identified and included all available studies on virtual wound care in residential aged care settings, providing a comprehensive review of the current evidence base. This allowed for mapping of the evolution of the field and highlighted a clear gap in the literature despite the high prevalence of chronic wounds in this setting.1,2 The review also synthesised evidence across a range of outcomes, including clinical outcomes, patient and staff experiences, and costs, providing a broad understanding of implementation and impact.
However, several limitations should also be considered. The generalisability of findings may be limited as several included studies were more than 10 years old, and the technologies used are likely to be outdated due to rapid advancements in digital health. 66 In addition, intervention descriptions were often inconsistently reported, limiting reproducibility and detailed comparison across studies. While reporting frameworks such as TIDieR-telehealth have since been developed to improve intervention reporting and reproducibility, 67 many included studies predated these standards, contributing to variability in reporting quality.
Deviations from protocol
The data extraction template used in this scoping review was updated after publication of the a priori protocol 34 to include clinical outcomes, satisfaction and costs. These outcomes measures were added to provide a more robust overview of the included studies and to better understand the possible advantages and disadvantages of virtual wound care in RACHs.
Future implications
The growing burden of chronic disease 68 along with an ageing population 69 will contribute to rising rates of wounds requiring high-quality and seamless access to specialist wound care services. Increased demand for services will necessitate more sophisticated models of virtual wound care to ensure equitable access. Specialised wound care clinics are frequently confined to major centres limiting in-person attendance by rural and immobile aged care residents. 20 Centralisation of wound care services presents a major barrier to timely diagnosis and management, contributing to delayed wound healing and avoidable complications. 70 Even in locations with existing specialist wound services, virtual wound care has been shown to optimise use of resources, 71 reduce travel burden and costs 28 and avoid burdensome in-person wound consultations for frail aged residents. Virtual wound care models have the potential to significantly enhance specialist access and improve wound outcomes, particularly for residents in rural and aged care settings, but will require careful observation to ensure equitable access.
Since the COVID-19 pandemic, the use of virtual care for chronic wounds has grown significantly improving access to specialist wound care8,47 though its uptake and evaluation have lagged in residential aged care. A lack of information technology (IT) infrastructure, varying levels of staff technological skills, and limitations in assessing residents with cognitive, visual or hearing impairment are commonly cited barriers to virtual care delivery in RACHs. 64 Recent investment in telehealth equipment in Australian RACHs 72 is a positive step towards increasing delivery of virtual care but additional support to develop a digitally capable aged care workforce and build sustainable virtual wound care models in RACHs is still needed. 73
Successful implementation of virtual wound care in RACHs requires simultaneous consideration of user, technological and organisational factors. 60 While virtual care training may increase user knowledge and competence, workforce challenges and staff retention issues remain. Broader implementation of strategies to boost video telehealth in RACH settings is also needed to ensure sustainable virtual care implementation. Increased reimbursement for video telehealth to encourage its use over phone telehealth may be an important policy setting to consider. Comprehensive evaluation of virtual wound care interventions and strategies to address implementation are urgently needed to improve wound outcomes and enhance sustainable models of care in RACHs.
Conclusion
Virtual wound care is being used in residential aged care settings though its uptake and evaluation is limited, highlighting the need for further investment to improve wound outcomes and quality of life for residents. Future virtual wound care trials in residential aged care should utilise validated templates for consistent description and reproducibility and ensure prompt evaluation and dissemination of research findings in the rapidly changing field. While virtual wound care is well accepted by staff, residents and families, workforce, training and technology barriers must be addressed to improve uptake in residential aged care.
Supplemental Material
sj-docx-1-jtt-10.1177_1357633X261462025 - Supplemental material for Virtual care for chronic wounds in residential aged care settings: A scoping review
Supplemental material, sj-docx-1-jtt-10.1177_1357633X261462025 for Virtual care for chronic wounds in residential aged care settings: A scoping review by Heather Russell, Georgina Luscombe, Annie Banbury, Meredith Makeham and Michelle Barakat-Johnson in Journal of Telemedicine and Telecare
Supplemental Material
sj-docx-2-jtt-10.1177_1357633X261462025 - Supplemental material for Virtual care for chronic wounds in residential aged care settings: A scoping review
Supplemental material, sj-docx-2-jtt-10.1177_1357633X261462025 for Virtual care for chronic wounds in residential aged care settings: A scoping review by Heather Russell, Georgina Luscombe, Annie Banbury, Meredith Makeham and Michelle Barakat-Johnson in Journal of Telemedicine and Telecare
Supplemental Material
sj-docx-3-jtt-10.1177_1357633X261462025 - Supplemental material for Virtual care for chronic wounds in residential aged care settings: A scoping review
Supplemental material, sj-docx-3-jtt-10.1177_1357633X261462025 for Virtual care for chronic wounds in residential aged care settings: A scoping review by Heather Russell, Georgina Luscombe, Annie Banbury, Meredith Makeham and Michelle Barakat-Johnson in Journal of Telemedicine and Telecare
Footnotes
Acknowledgements
The authors would like to thank Ms. Bernadette Carr, academic librarian at the University of Sydney, for assistance with the scoping review search strategy.
Author's note
Annie Banbury is also affiliated at Centre for Online Health, School of Medicine, The University of Queensland, Brisbane, Australia. Michelle Barakat-Johnson is also affiliated at Nursing and Midwifery, Sydney Local Health District, Sydney Australia.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is funded by a Medical Research Future Fund (MRFF) Rapid Applied Research Translation grant (RARUR000158), Department of Health 2022: Transforming Wound Care through Telehealth in Aged Care. The funder of the study had no role in the design, conduct, writing of the paper, or decision to submit for publication.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The broader study, Transforming Wound Care through Telehealth in Aged Care, has been undertaken in partnership with Coviu Global Pty Ltd who, with research partners, are developing WoundView, a novel wound analysis tool embedded in the Coviu telehealth platform.
Data availability statement
All data analysed during this study are included in this published article and its supplementary information files. The database search undertaken for this scoping review can be replicated by following the steps in the supplementary information file.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.