
Abstract
The importance of management strategies for subclavian artery aneurysms (SAAs) is underscored by the risks of aneurysm rupture and distal ischemia. However, there is no consensus on the optimal timing or strategies for treatment due to their low incidence. The existing literature primarily comprises case reports and small retrospective studies, providing limited high-quality evidence. The preservation of the vertebral artery (VA) is critical to the prognosis of SAA repair, particularly when a dominant ipsilateral VA exists and the circle of Willis is incomplete. In this review, we integrate published literature together with our center’s experience to classify SAAs into four types based on the anatomical relationship between the VA and the aneurysm, and we outline the treatment strategies for each type. Furthermore, given the substantial influence of diverse etiologies on disease progression, we address the clinical features and management approaches for SAAs based on distinct etiologies.
Introduction
Subclavian artery aneurysm (SAA), defined as a subclavian artery diameter exceeding 1.5 times its normal diameter, is an uncommon vascular pathology, accounting for only 0.2% of all aneurysms and 1% of peripheral aneurysms. 1 These aneurysms are frequently detected incidentally and may present with clinical manifestations including a pulsatile mass, shoulder pain, local compression leading to dysphagia, or rupture. Treatment options encompass open surgery, hybrid procedures, and endovascular techniques. However, the natural history of SAAs remains largely unknown, as there are few cases documenting changes in aneurysm diameter. Halldorsson et al. reported a case with no aneurysm growth after 12 months of follow-up, 2 whereas Nishimori et al. reported bilateral SAAs secondary to aortitis syndrome, with the right aneurysm enlarging to 4 cm and requiring surgical intervention after 10 years, whereas the left remained stable at 20 mm. 3 Given these uncertainties, the management of incidentally discovered SAAs remains unclear, and their natural history may vary depending on the underlying etiology. Additionally, the anatomical relationship and involvement of the vertebral artery (VA) play a crucial role in determining treatment strategies. In the absence of randomized clinical trials (RCTs), management strategies and optimal repair timing remain controversial. To address these uncertainties, we reviewed the published reports on SAAs to provide a concise overview of the clinical presentations and treatment strategies, categorized by etiology and anatomical characteristics. A comprehensive literature search of English language publications up to November 2025 was conducted in MEDLINE, Embase, Web of Science, and Cochrane Library electronic databases using a combination of the following terms: ‘subclavian aneurysm,’ ‘subclavian artery aneurysm,’ ‘SAA,’ ‘therapy,’ and ‘treatment.’
Diagnosis and prevalence
The diagnosis, timing, and management of SAAs are closely determined by the patient’s clinical presentation. Among 619 reported cases, 39.3% of patients presented with local signs, 27.1% with distal ischemia, 25.2% with compression, and 8.4% with rupture (Table 1). Prompt intervention is warranted in cases of distal ischemia or rupture, whereas patients with small asymptomatic aneurysms may be managed conservatively through blood pressure control, avoidance of neck massage, and regular surveillance. Sixteen studies, each including more than 10 patients, have detailed patient characteristics and management strategies for SAAs and are summarized in Supplementary Table S1.1-16
Symptoms and signs of subclavian artery aneurysm from 619 reported cases.

The number of reported SAA cases has increased substantially over time, from fewer than 10 cases per decade before 1963 to 437 cases between 2013 and 2022 (Figure 1). This apparent rise, however, is likely influenced by publication bias. Historically, open surgical repair was the standard of care and became less frequently reported as outcomes stabilized. In contrast, the increasing adoption of endovascular techniques in recent years has stimulated renewed reporting to evaluate these evolving techniques. Additionally, cases managed conservatively or deemed not to require treatment may be underrepresented in the literature, further contributing to bias in the observed trends.
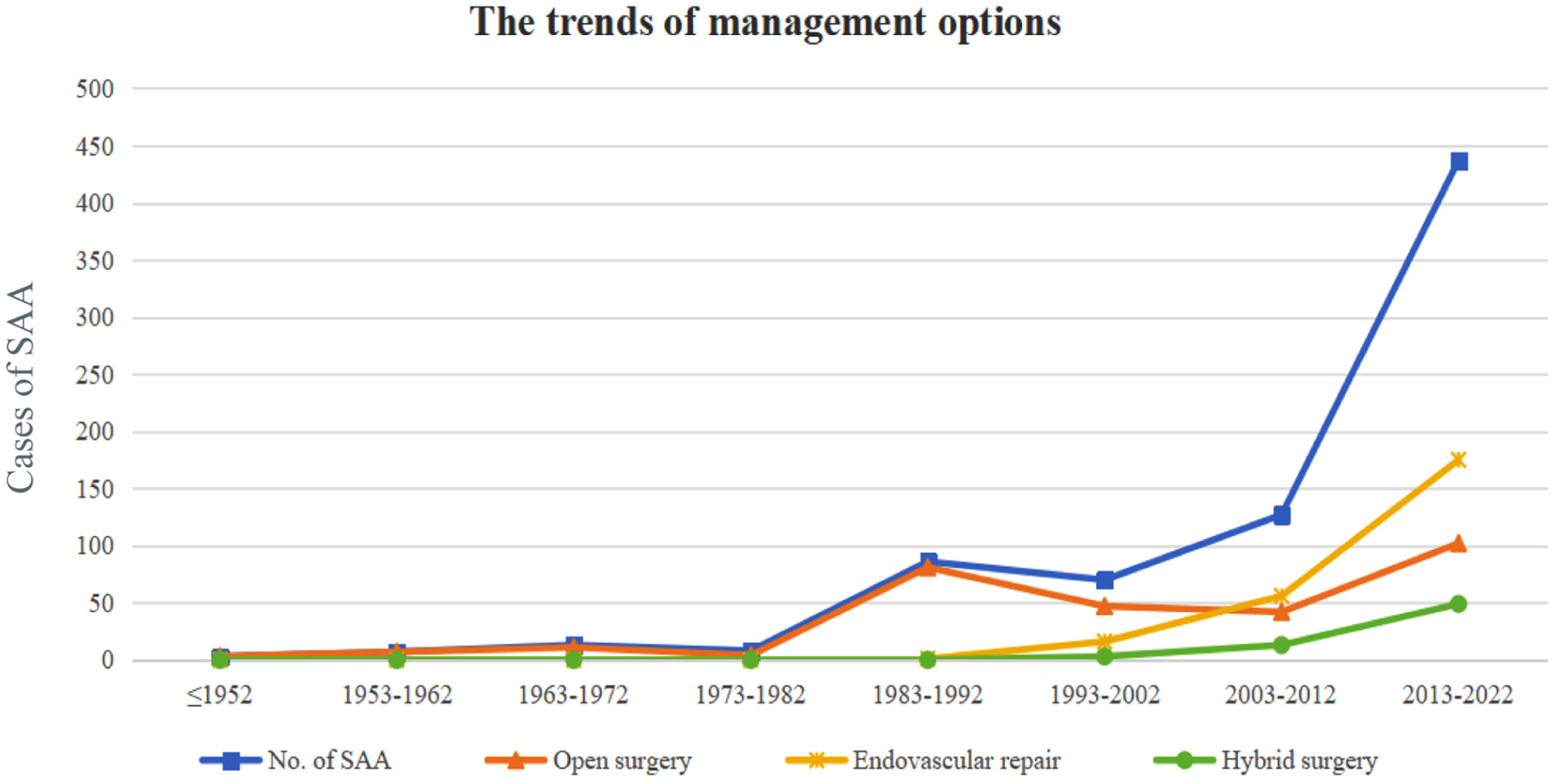
Depiction of changing trends in the treatment of subclavian artery aneurysm (SAA).
Anatomical classification
To provide a concise overview of treatment options for SAAs, we summarized published reports and, based on our clinical experience, propose a pragmatic anatomic classification that characterizes SAAs into four types. Notably, this classification is derived from our own observations and has not yet been formally validated.
Type I subclavian artery aneurysm (SAA)
Type I SAAs involve aneurysms of the aortic arch at the origin of the subclavian artery (Figure 2). The traditional open repair entails resection of the diseased segment of the aorta and subclavian artery, followed by replacement with a synthetic vascular prosthesis. Right-sided Type I SAAs can only be repaired via open surgery.
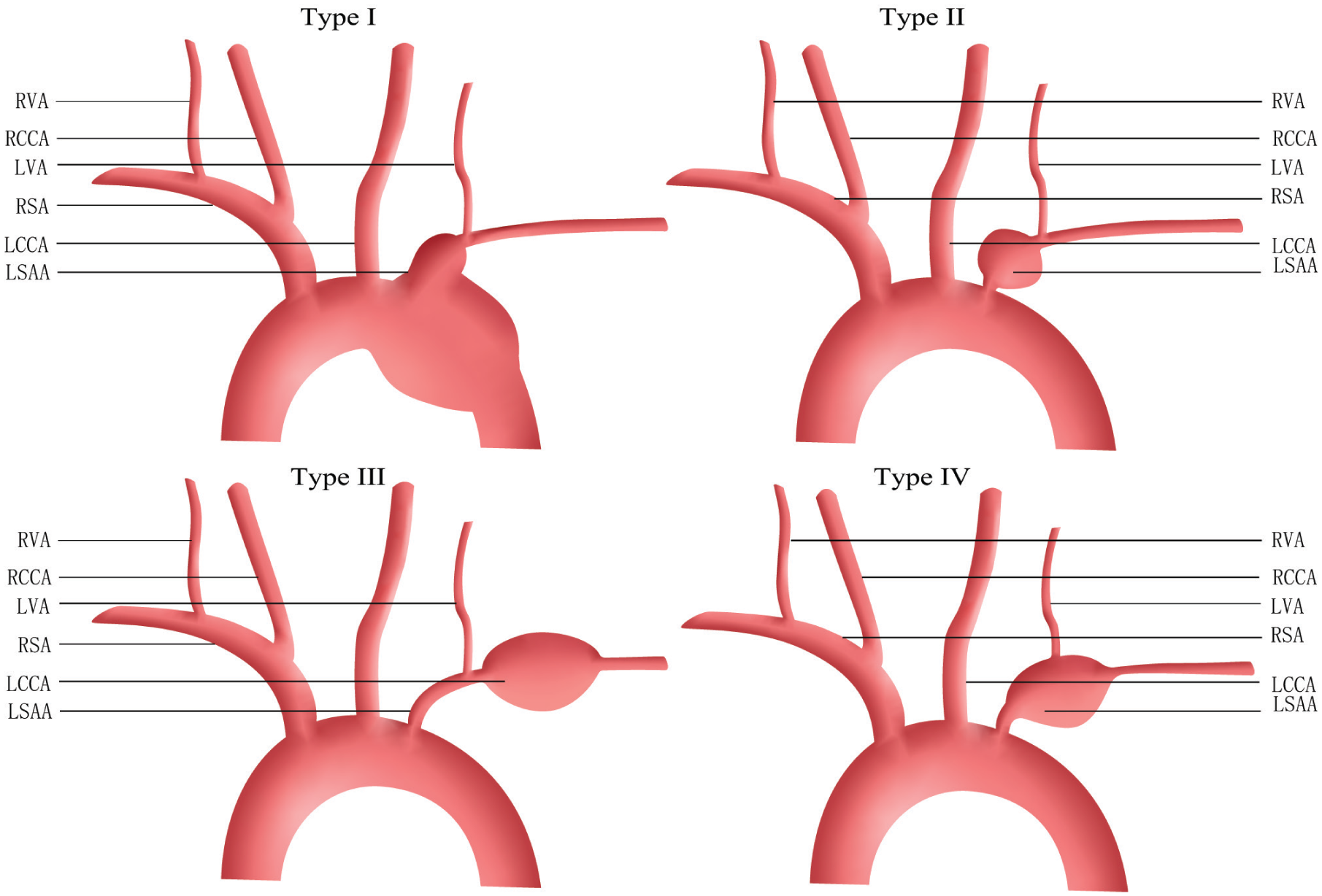
Subclavian artery aneurysm types.
For left-sided type I SAAs, hybrid surgery represents a viable alternative. This approach typically involves placement of a stent graft to exclude the aortic arch aneurysm, occlusion of the subclavian aneurysm sac with a plug or occluder placed proximal to the VA, and subclavian artery bypass for reconstruction. Notably, patients undergoing zone 2 thoracic endovascular aneurysm repair (TEVAR) with concurrent left subclavian artery bypass on the same day have demonstrated higher in-hospital mortality compared to patients undergoing staged bypass within 30 days of TEVAR (21.3% vs 3.7%). 4 These findings suggest that a staged strategy may offer improved safety, though its applicability to SAAs remains uncertain.
Two cases of total endovascular repair with custom-made thoracic endografts have been reported, demonstrating that there is sometimes adequate room for stent anchoring before VA takeoff. One case employed a custom mono-branch thoracic graft to repair intrathoracic SAAs, 5 whereas another used a fenestrated graft for aberrant right subclavian artery (ARSA) repair. 6
Type II SAA
Type II SAAs are located proximal to the VA. When the VA orifice lies ⩾ 10 mm distal to the aneurysm, endovascular stenting that preserves VA flow is typically preferred. 7 Furthermore, two case reports have demonstrated exclusion of the aneurysm using occluders or vascular plugs placed at the SAA origin proximal to the VA, thus maintaining retrograde subclavian flow and potentially enhancing upper-extremity perfusion.8,9 Outcomes vary: one patient remained asymptomatic 9 months postoperatively, 9 and another eventually required axillo-axillary bypass surgery due to persistent hand pain. 8 Although subclavian steal syndrome may occur, it was not observed in these reports. Overall, this technique allows postoperative assessment of upper-extremity and cerebral perfusion and may obviate the need for bypass surgery.
Standard open surgery involves resection or ligation with end-to-end anastomosis or interposition grafting. Type II SAAs are mostly proximal; consequently, thoracotomy may be necessary in some cases. Thus, hybrid repair combining endovascular exclusion with subclavian reconstruction offers another feasible alternative.
Type III SAA
Type III SAAs arise distal to the VA origin. Both open and endovascular repair are viable options, with endovascular treatment increasingly favored in recent years.
Endovascular therapy is preferred when the VA originates ⩾ 10 mm proximal to SAAs, providing adequate space for stent fixation. 7 Preservation of the left internal mammary artery (IMA) is essential, particularly for potential coronary artery bypass grafting (CABG). Long-term surveillance is necessary as endoleaks may arise from the thyrocervical trunk or IMA after endovascular repair.
Type IV SAA
Type IV SAAs occur when the VA originates from the subclavian aneurysm itself, necessitating VA preservation whenever possible. In this context, hybrid or open surgery is preferred, as total endovascular repair carries a high risk of stent stenosis or occlusion due to the VA’s small caliber and its susceptibility to compression from head and neck movements. Open surgery typically involves aneurysm resection, subclavian artery bypass, and VA transposition or reimplantation. Hybrid surgery is an alternative when adequate proximal and distal landing zones are available, combining stent graft exclusion with VA transposition or bypass.10–12 For right-sided SAAs with limited proximal landing zones, a stent can be extended from the innominate artery to the common carotid artery (CCA) to exclude the subclavian origin, with carotid–axillary and carotid–vertebral bypasses performed for revascularization. 13 Alternatively, a stent from the innominate artery can be combined with carotid–carotid and vertebral–carotid bypasses. 12
The decision to preserve the VA depends on the completeness of the circle of Willis and bilateral VA flow, which can be confirmed preoperatively via cerebral and neck angiography. Temporary balloon occlusion of the affected VA in awake patients may further clarify the necessity of preservation. 14 If the circle of Willis is complete and the ipsilateral VA is nondominant, or if the patient has no symptoms of cerebral ischemia after preblock, VA sacrifice is acceptable.
Etiological classification
The etiology of SAAs is summarized in Table 2. Different etiologies result in distinct clinical presentations and management strategies.
Etiology of subclavian artery aneurysm from 682 reported cases.
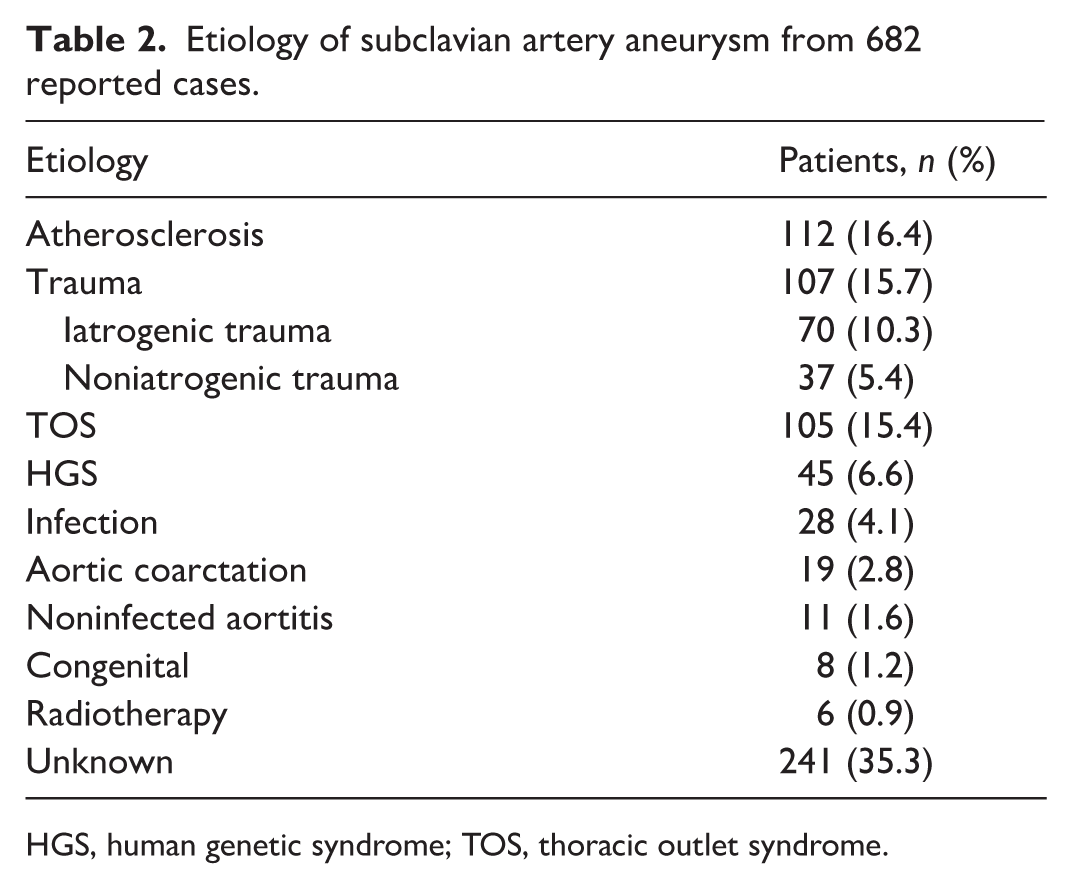
HGS, human genetic syndrome; TOS, thoracic outlet syndrome.
Thoracic outlet syndrome-related SAA
In thoracic outlet syndrome (TOS)-related SAAs, aneurysmal dilation results from turbulent blood flow secondary to arterial compression at the thoracic outlet. Archie et al. reported mean aneurysm diameters of 21 mm (range, 20–22 mm) in seven patients with TOS-related SAAs, whereas another study reported that all patients with TOS-related SAAs experienced upper-extremity pain and most developed limb-threatening ischemia. 15 Repair is recommended even for small aneurysms, as intraluminal thrombosis (ILT) formation increases the risk of cerebral infarction and limb loss. This aligns with the findings of Vierhout et al., who observed thrombosis in true aneurysms with relatively small diameters of 12–25 mm. 16
Standard treatment involves SAA repair, correction of distal ischemia, and TOS decompression, with limb salvage achieved in all patients following such procedures.15,17,18 In some smaller aneurysms, exclusive decompression without aneurysm repair increases the risk of recurrent embolization from ILT detachment. 19 Thus, aneurysm exclusion is warranted when ILT is present, regardless of size, to prevent recurrent distal embolism. Additionally, TOS decompression is essential after stenting to prevent stent occlusion or fracture from first-rib compression.20,21
Sympathectomy, previously used for ischemia relief and tissue loss prevention, is now largely abandoned due to high recurrence and complications such as Horner’s syndrome.19–22 Current strategies favor thrombectomy or bypass for upper-limb ischemia, with bypass demonstrating superior patency (75% vs 58%). Current strategies favor thrombectomy and bypass procedures for upper-limb ischemia, with bypass surgery demonstrating superior patency (75% vs 58%). 17 This is because, in cases of chronic and recurrent occlusion, intraluminal synechiae and fibrosis complicate complete thrombectomy and increase the risk of recurrent thrombosis. 17
Human genetic syndrome-related SAAs
Human genetic syndromes (HGS), such as Marfan syndrome, Loeys–Dietz syndrome (LDS), and Ehlers–Danlos syndrome (EDS), are associated with increased tissue fragility. As these conditions often involve aortic complications, SAA repair is typically performed early in conjunction with aortic disease management. The characteristics of SAAs vary depending on the type of HGS. For instance, patients with vascular EDS have higher rates of complicated dissections, symptomatic aneurysms, and emergent ruptures than those with Marfan syndrome and LDS, leading to poorer prognosis. 23
Open repair involving aneurysm resection with graft replacement or end-to-end anastomosis has shown promising outcomes. However, these outcomes may be influenced by publication bias and limited follow-up, as studies often report favorable results and many have follow-up periods shorter than 2 years, potentially missing late complications.24,25 Consistent with aortic aneurysm guidelines, open surgery is recommended as first-line treatment in young patients with suspected connective tissue disorders and abdominal aortic aneurysms (Class I, Level C). 26 Its long-term durability surpasses endovascular repair, which has been reported to have higher secondary intervention rates (20.0% vs 12.0%, p < 0.05).23,27 Currently, endovascular procedures serve mainly as a bridge to open surgery in emergencies or for technically complex anatomies, with 79.5% of patients undergoing endovascular treatment having previously undergone open aortic surgery. 23 Moreover, patients with HGS are prone to vascular injuries during endovascular procedures, such as brachial artery injury during sheath removal, and should therefore be treated with caution. 28 In a reported case, multiple previous surgeries related to Marfan syndrome resulted in severe adhesions, making both open surgery and further endovascular intervention challenging; therefore, direct sac puncture embolization was adopted as an alternative, successfully achieving complete exclusion of the aneurysm. 29
Infected SAA
Infections can originate from primary arterial infections or secondary spread from adjacent structures, infective endocarditis, or bacteremia and fungemia. Common pathogens include Staphylococcus aureus, Treponema pallidum, and Mycobacterium tuberculosis. Infected aneurysms are typically aggressive, often presenting with hemoptysis due to erosion into the lung parenchyma and early rupture. Fatal rupture without timely diagnosis and intervention has been reported.30,31 Therefore, early diagnosis, prompt systemic antibiotic therapy, and timely surgical treatment are essential for improving prognosis.
Open surgery, involving complete aneurysm excision, autologous vein graft revascularization, and thorough debridement, remains the gold standard for treating infected SAAs. When aneurysms are densely adherent to surrounding structures, in situ reconstruction may not be feasible, and extra-anatomic bypass or even endovascular repair is recommended.32–34 However, the use of long conduits in this approach increases the risk of early thrombosis. Endovascular aneurysm repair can serve as a permanent or palliative treatment for those unfit for open surgery.35–37
After SAA repair undertaken for infection, postoperative antibiotics are essential, although optimal duration remains controversial—ranging from several months32,38 to lifelong treatment.39,40 Residual infected tissue after endovascular treatment carries the risk of persistent or recurrent infection, highlighting the need for individualized management and prolonged antibiotic therapy. 38
Aortic coarctation-related SAA
Aortic coarctation (CoA), typically distal to the left subclavian origin, predisposes to proximal left-sided SAAs, often presenting with compressive symptoms.
CoA repair is indicated when hypertension is present, whereas small SAAs may be preserved due to their low risk of rupture and distal ischemia. However, current evidence suggests that CoA is associated with congenital defects promoting inflammation, apoptosis, and oxidative stress, particularly in patients with concurrent bicuspid aortic valve (BAV), a known risk factor for postrepair aortic enlargement.41–43 Therefore, periodic follow-up is essential, as the natural history of CoA-related SAAs may involve rapid expansion compared to atherosclerosis-related SAAs. Pogorzelski et al. documented a 30% increase in the size of CoA-related SAAs over 4 years, underscoring the importance of regular monitoring. 44
Surgical repair is preferred for long and tubular coarctation or diffuse arch hypoplasia. 45 Repair methods for CoA include graft interposition, Dacron patch, or ascending-to-descending aorta bypass. Concurrent SAA repair generally involves aneurysm resection and graft interposition. Published outcomes support the safety and efficacy of simultaneous repair of CoA and SAAs, with only one reported mortality due to acute renal tubular necrosis and ventricular fibrillation. 46
For discrete CoA, stent implantation is preferred and often covers the left subclavian origin. Hybrid approaches, such as subclavian–carotid artery bypass combined with stent placement, have been shown to be safe and effective while simultaneously preserving left upper-limb function.47,48 Total endovascular repair using ‘Sandwich’ or ‘Chimney’ techniques can also minimize surgical trauma and preserve the subclavian artery but they require advanced expertise. 49 Owing to extensive collateral circulation that develops from long-term blood insufficiency below the coarctation, sacrificing the subclavian artery is acceptable. One case reported no neurological events or left upper-extremity ischemia despite not reconstructing the subclavian artery. 44
Noninfected aortitis-related SAA
Takayasu arteritis and Behçet’s disease are leading causes of aortitis-related SAAs. Inflammatory cell infiltration in the aortic wall promotes the destruction of elastic lamina and aneurysm formation. Aortitis can result in aortic aneurysms, rupture of the vessel wall, acute dissection, and/or thrombotic occlusion, increasing the risk of morbidity and mortality. 50
Guidelines recommend assessing inflammation activity for effective management. Immediate corticosteroids should be administered upon diagnosis, and elective SAA repair should be delayed until the acute inflammatory state is controlled, as active disease increases graft failure and stent restenosis rates. Suppressing inflammation may also help prevent further aneurysm development.50–52 However, high-dose corticosteroid therapy may weaken the arterial wall and increase rupture risk. 53 Consequently, in emergent situations, open surgery remains reasonable despite ongoing inflammation. For instance, one patient with Behçet’s disease underwent urgent aneurysm repair during active inflammation with an erythrocyte sedimentation rate of 40 mm/h. The patient experienced perioperative thrombosis but showed no recurrence of the aneurysm or complications at the anastomosis site during a 13-month follow-up. 54
Case reports on noninfected aortitis-related SAA repair generally show favorable outcomes, supporting individualized revascularization strategies using either open surgery or endovascular repair. In Takayasu arteritis, a meta-analysis revealed a higher risk of stroke and a lower risk of restenosis after open surgery compared with endovascular intervention. 55 Restenosis occurred in 31.7% of patients with Takayasu arteritis after endovascular repair, but stable disease and postinterventional immunotherapy treatment can reduce the risk. 52
The destruction of medial elastic fibers causes anastomotic fragility and the risk of anastomotic aneurysm after surgery. Miyata and colleagues reported a 12% cumulative incidence of anastomotic aneurysms 20 years after repair in patients with Takayasu arteritis. Their findings suggested that aneurysmal disease itself, rather than systemic inflammation control or steroid use, may be a key risk factor for postoperative anastomotic aneurysms, as repairs for aneurysms had a higher risk of anastomotic complications than those for stenosis. 56 Nevertheless, some experts advocate for bypass surgery as an alternative strategy to avoid anastomosis at inflamed sites, potentially reducing the incidence of anastomotic aneurysm complications. 57
Aneurysmal aberrant right subclavian artery (ARSA)
An ARSA typically arises from the descending thoracic aorta as the last branch, with ARSA and a left-sided aortic arch being the most common subclavian artery anomaly. 58 Most ARSAs develop aneurysms at their origin, known as Kommerell’s diverticulum. ARSAs are usually located behind the esophagus (80%), between the esophagus and trachea (15%), or in front of the trachea (5%). 59 Owing to its location, an ARSA often causes local compression symptoms such as dysphagia and dysphonia. 60 Aneurysmal ARSA is more unstable than native SAAs and carries a high risk of rupture or dissection, with rupture rates up to 6% and dissection or rupture rates up to 53%. 58 Cinà et al. reported an average aneurysm rupture size of 58 ± 20 mm (range, 20–100 mm), suggesting that size alone does not predict rupture risk, and that different threshold sizes for repair (20 mm or 30 mm) are determined by expert opinions.58,60
Surgical repair options include oversewing the subclavian artery origin or aneurysm resection with carotid–subclavian bypass. Hybrid approaches are the primary choice for elective SAA repair, with TEVAR combined with subclavian artery reconstruction being the most frequently used. Additionally, coils or Amplatzer plugs deployed at the VA can prevent VA reflux.61,62 TEVAR with distal ligation yields lower mortality and greater aneurysm shrinkage than distal occlusion devices, without significant differences in endoleak or complication risks. 63 In emergencies, TEVAR or percutaneous transluminal angioplasty is used to occlude the aneurysmal ARSA origin and control bleeding, allowing time for subsequent operations.64,65
Two main strategies for total endovascular repair are used: (1) covering the ARSA ostium with a stent or occluder, sacrificing the subclavian artery with distal upper-extremity blood supplied by retrograde VA flow, and (2) deploying a stent within the SAA to exclude it. Notably, care must be taken to avoid ILT detachment during stent and guidewire placement, as reported cases of impaired vision and subsequent posterior circulation ischemia highlight this risk. 66 Advanced techniques such as periscope or fenestrated TEVAR can also enable subclavian preservation.6,67
Conclusions
Open surgery, endovascular repair, and hybrid surgery all provide effective treatment and low complication incidence for SAAs, with strategy selection tailored to patient-specific anatomy and clinical status. Our proposed four-type anatomical classification based on the relationship to the VA offers practical guidance for individualized management. Furthermore, the natural progression of aneurysms varies depending on the underlying etiology; thus, etiology-specific considerations are essential. TOS-related SAAs warrant early repair due to the high risk of limb ischemia. HGS-related SAAs favor open surgery for durability, but long-term complications may reduce patient survival, necessitating long-term follow-up. Infected SAAs require antibiotic therapy and complete debridement of infected tissue. CoA-related SAAs benefit from simultaneous coarctation correction and aneurysm resection. Noninfected arteritis-related SAAs demand inflammation control before intervention. Aneurysmal ARSA carries a particularly high rupture risk, necessitating early intervention.
Supplemental Material
sj-docx-1-vmj-10.1177_1358863X261425578 – Supplemental material for Subclavian artery aneurysms: Management strategies by etiology and anatomical classification
Supplemental material, sj-docx-1-vmj-10.1177_1358863X261425578 for Subclavian artery aneurysms: Management strategies by etiology and anatomical classification by Ke Zhang, Yuanrui Gu, Haorui Zhang and Chenxi Ouyang in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was financially supported by the Fundamental Research Funds for the Central Universities (grant no. 3332024132).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.