
Abstract
Portal vein aneurysm (PVA) is a rare entity that can lead to hemorrhage or thrombosis. Although there is no standard treatment, most cases can be managed conservatively; intervention is reserved for symptomatic or enlarging aneurysms. For patients who are not surgical candidates due to cirrhosis and portal hypertension, endovascular creation of a trans-jugular intrahepatic porto-systemic shunt (TIPS) is an option to reduce portal venous pressure. This report describes a case of an enlarging PVA successfully treated with TIPS in a patient with cryptogenic cirrhosis.
Introduction
Portal vein aneurysms (PVA) are uncommon with fewer than 200 cases reported in the literature.1,2 Although there are currently no guidelines for PVA management, asymptomatic, stable aneurysms may be followed with serial imaging. Enlarging or symptomatic aneurysms require treatment to prevent rupture or portal vein thrombosis.3,4 Surgical aneurysmorrhaphy has been the most commonly reported treatment of PVAs; however, this procedure carries substantial risk in patients with liver cirrhosis and portal hypertension. 5 We present a rare case of trans-jugular intrahepatic porto-systemic shunt (TIPS) creation for the management of an enlarging PVA.
Case Report
A 32-year-old male with history significant for acute lymphocytic leukemia (ALL) in remission presented with an asymptomatic but enlarging PVA. Discovered incidentally years earlier, the PVA had been stable for at least 12 years before interval growth from 4.8 cm to 5.2 cm over a 2 year period was observed on computed tomography (CT) acquired to evaluate an unrelated benign renal lesion. The aneurysm expanded the main portal vein with extension to the upper portion of the SMV (Figure 1). Tran-jugular liver biopsy 3 years earlier had demonstrated marked hepatic steatosis with mild fibrosis.
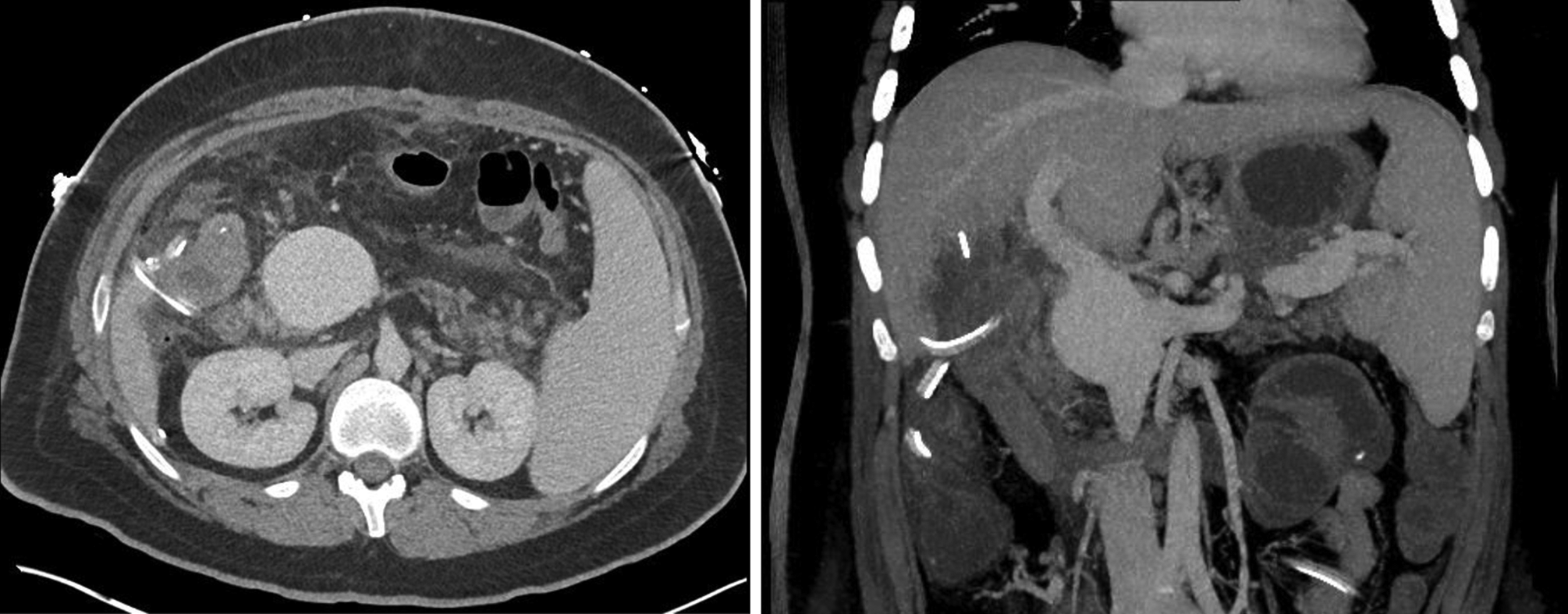
Axial and coronal maximum intensity projection images demonstrating 5.7 cm fusiform aneurysm of the extra-hepatic portal vein extending to the upper superior mesenteric vein.
Given the large size and interval growth of the PVA, operative repair was first attempted but aborted intraoperatively due to the presence of significant cirrhosis upon visual inspection of the liver. Open liver biopsy confirmed cirrhosis with evidence of severe iron overload. The patient had a MELD score of 10 and moderate splenomegaly but no ascites or evidence of varices. An immediate post-operative CT demonstrated further growth of the PVA to 5.7 cm since the prior study obtained 5 months earlier. Following multi-disciplinary discussion, the decision was made to create a TIPS to treat the portal hypertension and reduce the risk of further aneurysm growth while the patient underwent evaluation for liver transplantation.
The procedure was performed with general anesthesia. Right internal jugular vein access was obtained and the right hepatic vein was selected. The initial porto-systemic gradient was 16 mmHg. Trans-hepatic portal vein access was obtained with a Rösch-Uchida set (Cook Medical, Bloomington, IN) and digital subtraction angiography was performed, demonstrating the large PVA (Figure 2). No varices were seen. An 8 + 2 cm × 8-10 mm Viatorr TIPS stent (Gore Medical, Flagstaff, AZ) was deployed and post-dilated to 10 mm in diameter. Final venogram demonstrated brisk flow through the TIPS (Figure 3) and the final porto-systemic gradient was reduced to 8 mmHg.
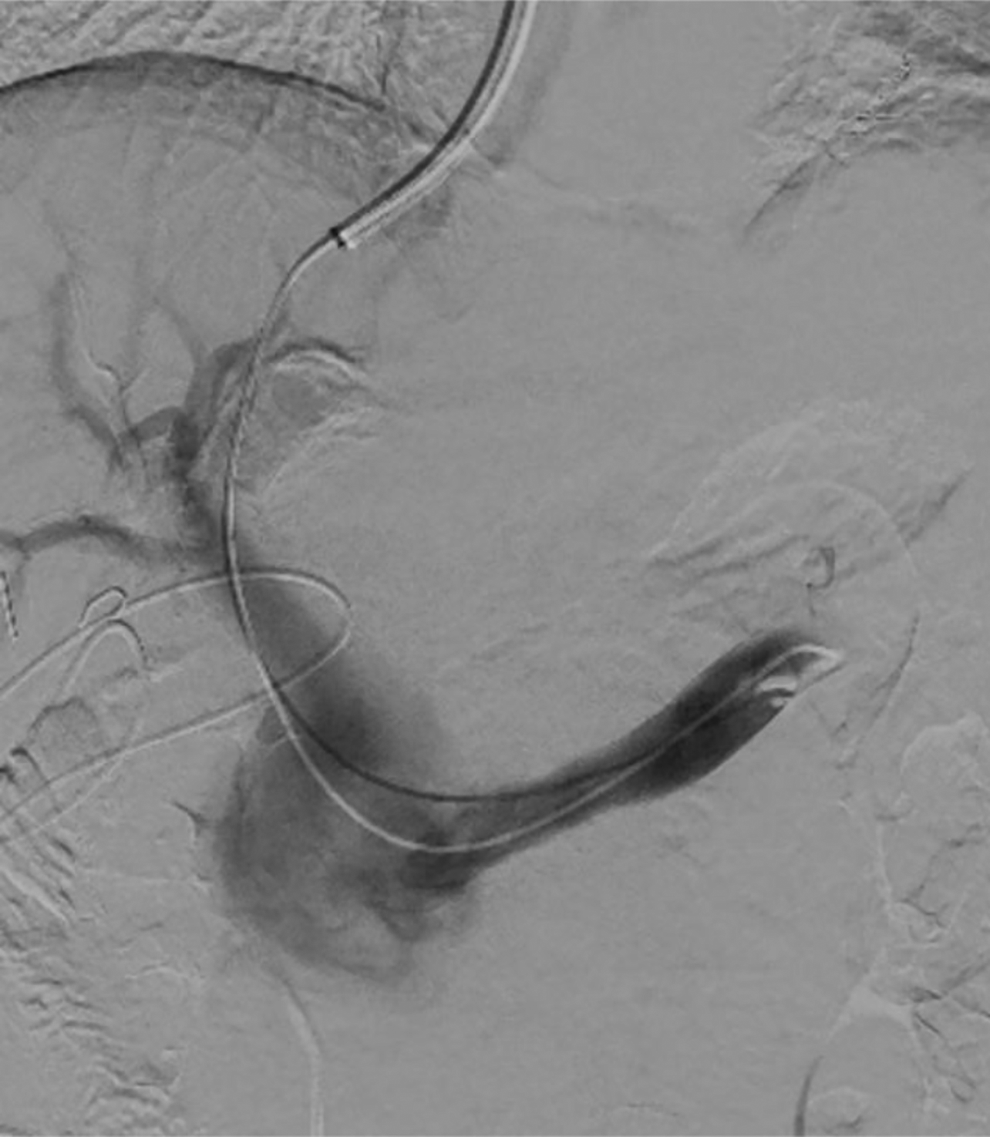
Digital subtraction angiogram following splenic vein injection demonstrating the portal vein aneurysm and hepatopedal flow. No gastroesophageal varices were visualized.
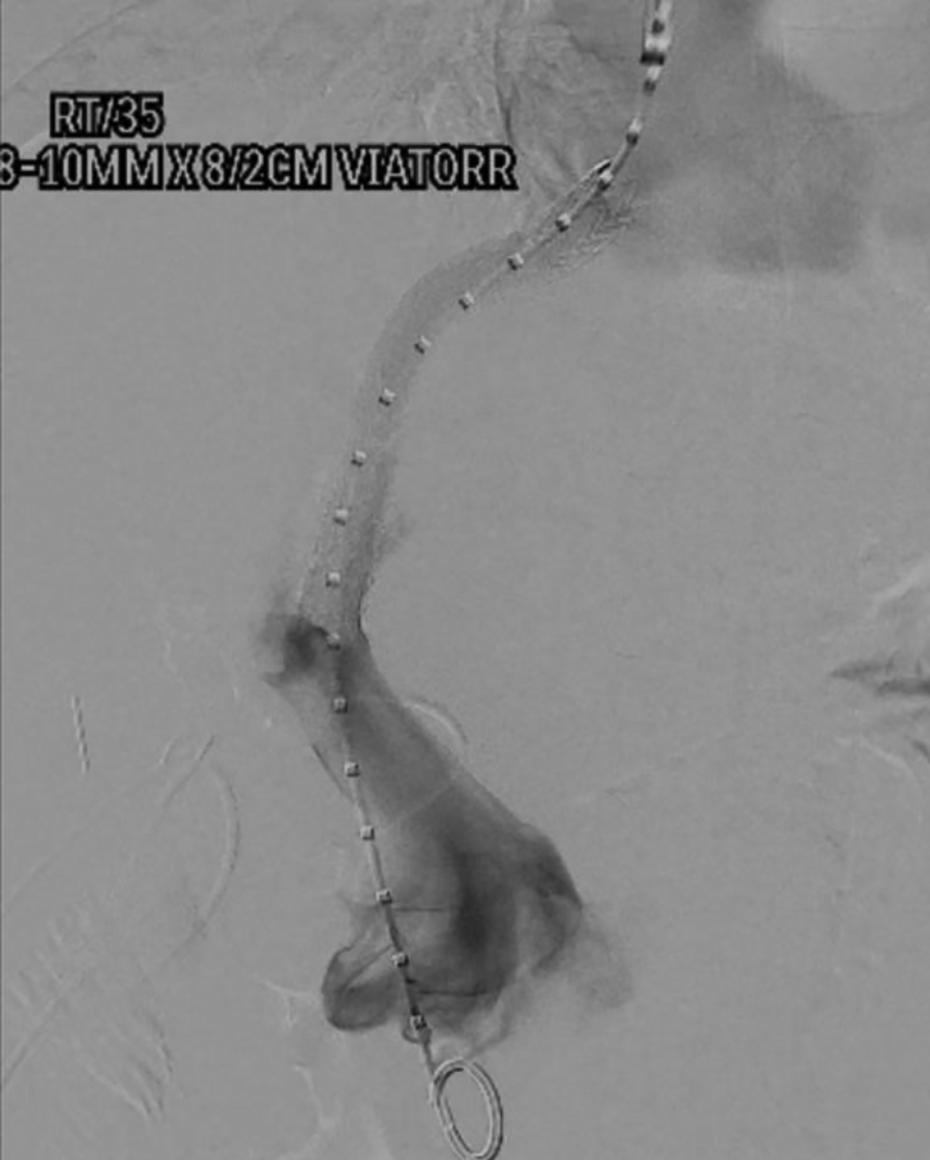
Digital subtraction angiogram following trans-jugular intrahepatic porto-systemic shunt placement, showing brisk flow through the shunt.
The post-operative course was uneventful and there was no evidence of hepatic encephalopathy. Follow-up CT imaging after 3 months demonstrated no further growth of the aneurysm (Figure 4). The patient remained asymptomatic at the 6 month post-procedure clinic visit, the most recent follow-up at the time of writing. His liver disease has been managed with weight loss and therapeutic blood draws. Informed consent was granted by the patient for publication of the case report and accompanying images.
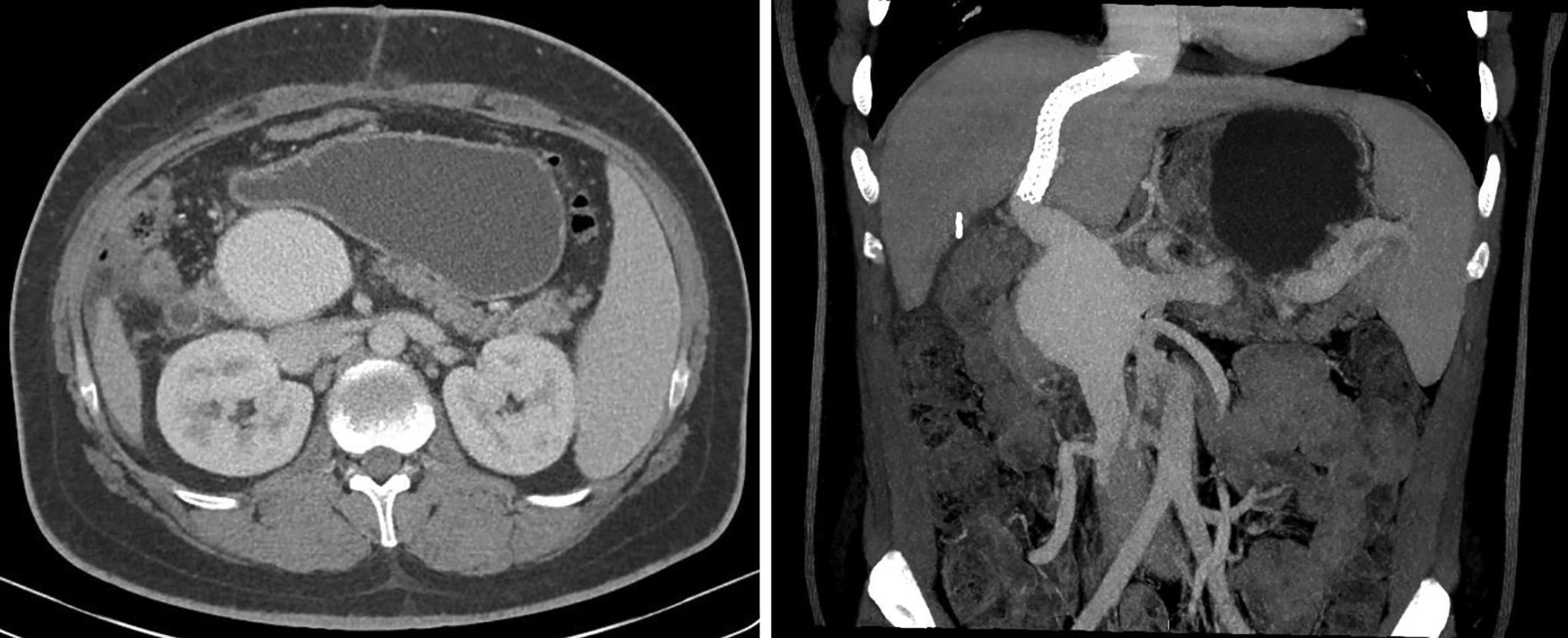
Axial and coronal maximum intensity projection images obtained 3 months status post TIPS demonstrate stable 5.7 cm portal vein aneurysm.
Discussion
Portal vein aneurysms are defined as dilatation of the portal vein greater than 2 cm. 6 While the etiology of PVAs has not been confirmed, PVAs are typically classified as congenital or acquired. 2 It has been postulated that congenital PVAs occur due to incomplete regression of the right distal vitelline vein, leading to a small diverticulum that may progress to a saccular aneurysm.2,7,8 Acquired PVAs are more common and most often attributed to portal hypertension in the setting of cirrhosis. 6 It is thought that elevated portal venous pressures cause weakening of the venous wall through a process of intimal thickening, medial hypertrophy, and eventual fibrous replacement. Additional but less common causes of acquired PVAs include pancreatitis, trauma, iatrogenic injury during surgery, and malignant invasion of the portal vein.9,10
Approximately one third of patients with PVA are asymptomatic. 6 For those with symptoms, non-specific abdominal pain is most common and reported by half of patients. 2 Aneurysmal rupture is rare due to the relatively low portal venous pressures, but risk increases in the setting of portal venous hypertension.3,6,11 Portal vein thrombosis is more common, occurring in up to 20% of patients, and is almost always associated with abdominal pain when acute. 2 Acute portal vein thrombosis, particularly when extending to the superior mesenteric vein, carries risk of bowel ischemia or infarction. Less common manifestations of PVA include jaundice from compression of the common bile duct, gastrointestinal symptoms from compression of the duodenum, and vascular sequela from mass effect on the inferior vena cava.
Evidence-based management guidelines for PVA are lacking; however, most published reports support conservative management of stable, asymptomatic PVAs with serial imaging (typically Doppler ultrasound and/or CT) and clinical follow-up. Procedural intervention is typically reserved for complicated PVAs, including those with associated symptoms, rupture, thrombosis, size greater than 3 cm, or progressive enlargement. Historically, PVAs were treated surgically, but a systemic literature review demonstrated post-operative mortality of 17.5%. 2 Given the increased operative risk associated with cirrhosis, Laurenzi et al proposed a treatment algorithm where non-cirrhotic patients were treated surgically with resection or repair and cirrhotic patients were treated with TIPS creation or liver transplantation. 2
TIPS is a minimally invasive, endovascular procedure that has been proven effective in the management of portal hypertension in cirrhotic patients.12,13 If the etiology of an expanding PVA is related to portal hypertension, TIPS may be an effective treatment option by reducing the portosystemic gradient. Additionally, TIPS has the advantage of treating other sequelae of cirrhosis, such as ascites and variceal hemorrhage, while still preserving future surgical options like aneurysmorrhaphy, aneurysmectomy, and transplantation. Other minimally invasive endovascular therapies for PVAs have been proposed, such as coiling or stent graft exclusion of the aneurysm, as well as transhepatic catheter-directed mechanical thrombectomy in the setting of acute thrombosis of a PVA. 14
This case is 1 of only 3 published PVAs treated with TIPS.10,15 The PVA in our patient was caused by portal hypertension from cirrhosis, which was likely secondary to a combination of drug-induced liver injury from chemotherapy, nonalcoholic steatohepatitis from obesity, and concurrent iron-overload related to the patient’s history of ALL. Childhood cancer has been associated with acute and delayed hepatotoxicity secondary to chemotherapy, transfusion associated iron overload, and cholestatic disease from total parenteral nutrition. 16 Methotrexate, a commonly used agent for ALL that our patient also received, is associated with a high incidence of hepatic fibrosis that leads to a narrow therapeutic index. 17 Interestingly, our patient’s PVA was stable for at least 12 years before subsequent enlargement was observed. While the cause of this delayed enlargement is unclear, it may relate to obesity-related non-alcoholic steatohepatitis or delayed hepatotoxicity from chemotherapy. No new medications or other causative triggers could be identified.
A limitation of this report is the lack of long-term radiologic and clinical follow-up at the time of writing. Tsauo et al and Ding et al noted a decrease in the size of PVAs treated with TIPS at 3 month and 6 month radiologic follow-up, respectively.10,15 While the observed stability in size of our patient’s PVA at 3 month follow-up can still be considered a treatment success, continued imaging surveillance will be necessary and eventual decrease in the size of the PVA is expected.
Due to the rare occurrence of PVAs and limited evidence for various treatments, management of PVAs is not standardized. Conservative management is the best option for most patients; complex cases should be treated at high-volume centers with a multidisciplinary hepatobiliary disease management team.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.