
Abstract
This article describes the development and application of a wrap-around, multidisciplinary, brain-based, developmental and attachment-focussed intervention for children who have experienced significant trauma in the context of their early life. It outlines the presentation of the children and families who are referred to the service and the model of treatment that they receive. In doing so, it identifies the core components underpinning Neuro-Physiological Psychotherapy (NPP) and links the application of the integrative model to research and practice in the field of neuroscience and attachment and to the use of therapeutic approaches that are beneficial to maltreated children and their adoptive parents. It highlights the need for a neuro-sequential approach that impacts all aspects of the child’s life in the effort to redress the impact of developmental trauma with the aim of improving their overall functioning and their ability to develop healthy relationships into the future.
Keywords
Context of model development
Family Futures CIC is a Voluntary Adoption Agency and Community Interest Company that specialises in Adoption Support. It has been offering specialised therapeutic support to looked-after children and children adopted from care and their parents since its inception in 1998. Its therapeutic treatment approach to recovery for children who have experienced sustained trauma in the context of their birth family environment has been influenced by the pioneering and leading research and practice in the field. It has been informed by research and practice in developmental trauma (Van der Kolk, 2005), neuroscience (Perry, 2006; Porges, 1998; Siegel, 1999), somatic experience (Levine, 2010; Levine & Kline, 2006), sensorimotor psychotherapy (Ogden, Minton, & Pain, 2006), sensory integration (SI) (Ayres, 1979), play (Booth & Jernberg, 2009) and family-focussed attachment-based approaches to psychotherapy (Hughes, 2006). The model has been in development over the past 18 years. It is a brain-based, sequential and developmental approach to therapeutic treatment of children which integrates leading attachment and neuroscience research with sensory, somatic, play-based, attachment and trauma-focussed therapy and narrative, therapeutic life story work.
Referral and assessment
Children and families who are referred to the organisation are often at crisis point and many have been declined services by local mental health teams when they do not fit their referral criteria (often not falling into criteria defined by discrete psychiatric disorders) or whose complex needs cannot be met by available services. 1 Often, though not always, they have not received anything by the way of a psychological assessment or a comprehensive formulation of their needs. The starting point at the organisation is to offer a comprehensive, specialised assessment of their difficulties which leads to a formulation of their complex presentation and needs. This assessment includes standard psychological and sensory processing screening tools, measures of attachment and child/parent interactions, family and child observations and projective assessments of children. The assessment is also multi-informant, using parent, child and teacher responses. A detailed file search is conducted when possible to provide information regarding the nature of the trauma and possible psychological and neurological developmental impact.
If a family is considered suitable for the intervention provided by the service (a consensus reached by the professional system), they may receive additional assessments that allow an elaboration of the formulation and ensures support is directed to critical areas. This includes cognitive, paediatric and psychiatric assessments by consultants who are experts in their field. Further SI assessment is also carried out by the Occupational Therapist within the organisation. The organisation is not a diagnostic service but, rather, provides formulations of the child and family’s difficulties which are considerate of the complexity of their lives. These formulations consider the in utero and early life experiences, developmental timeframe, genetic factors, cognitive difficulties, trauma responses, attachment difficulties, parent factors and wider systemic factors. If a child’s presentation is considered as meeting criteria for a discrete diagnosis, a referral is made to appropriate services. Links are encouraged with the family’s local health services and a significant minority of children are in receipt of medication aimed at reducing attention deficit/hyperactivity disorder or extreme hyperarousal symptoms.
Neuro-Physiological Psychotherapy – an integrative neuro-sequential approach
Burnell and Vaughan (2012) state the following as the organising principle of the model:
Children import with them into their substitute family, the developmental delay and damage that their previous life experiences have impacted upon them. It is vital therefore that this neuro-physiological and psychological damage is addressed in order for secure attachment to be developed in permanent placements. (p. 202; authors’ translation)
The approach has been informed by current neuro-developmental research and documented in publications as it developed (Archer & Burnell, 2003; Burnell & Vaughan, 2006, 2008, 2012). In particular, the approach has largely been informed by work regarding the hierarchical structure of brain formation (e.g. Schore, 2001). Burnell and Vaughan (2006) published a version of the chart above (Figure 1) that links therapeutic intervention to brain structure. The term ‘neuro-sequential’ was first introduced by the work of Bruce Perry (2006) who developed the Neuro-sequential Model of Therapeutics (NMT) approach. While the organisation’s model is informed by NMT, it does not profess to offer this, and there are differences between the two. However, the model can be considered neuro-sequential as (a) it follows the hierarchical sequence of brain and central nervous system development in neonates and infants and (b) in doing so directs its therapeutic attention to three main areas of brain function – the primitive brain system, the mid-brain (limbic) and the higher order functioning of the cortical brain.
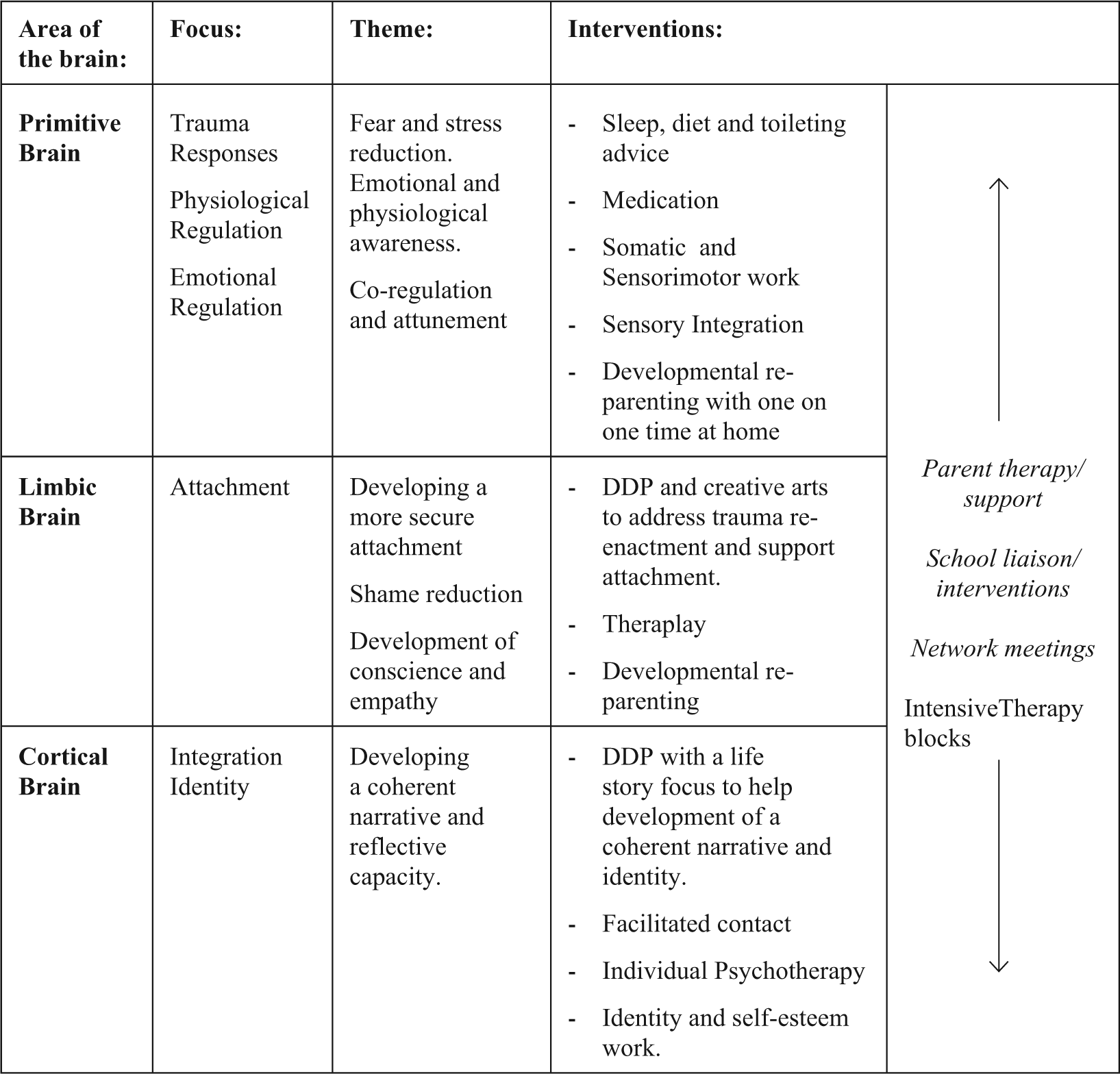
The Neuro-Physiological Psychotherapy model.
Therapeutic aims of the Neuro-Physiological Psychotherapy model
Children who have been exposed to persistent trauma in the context of their early development often have entrenched fight/flight or freeze responses which, while adaptive in the context of maltreatment, are maladaptive in a safe, loving adoptive or foster care placement. These responses are thought to be hardwired as ways of coping and may appear as highly dysregulated, aggressive or dissociative behaviours within the context of an adoptive placement. The aim of the treatment programme is to enable the child to develop alternate ways of managing in the face of triggering and highly dysregulating events by being helped to physiologically and emotionally regulate by their parent. Consequently in a calmer, less reactive state, the child is supported to experience their parent as available to them and as able to help them make sense of their world. The child is supported to move from a reliance on primitive, reactive brain responses towards the use of cortical brain responses – more rational thought. The executive functioning system should ideally be more readily accessed, children become less emotionally labile and engage more ‘secure’ attachment-based strategies, for example, accessing their parents for help. In terms of education, children are supported to engage self-regulatory strategies and to develop alternate neural pathways to those developed in the context of maltreatment, with the aim of improving their concentration and learning, in theory having better access to higher order thinking.
Figure 1 shows the process of the treatment programme and the types of intervention that aim to target each brain region. While the overall approach is sequential, it is not a strictly linear one and there is movement between the levels. It is underpinned by Dyadic Developmental Psychotherapy (DDP; Hughes, 2006), and certain aspects such as parent therapy and support, school consultation and support and network liaison remain perpetual with emphasis placed on each of these as each case demands. Michael Tarren-Sweeney, a leading epidemiologist in the mental health of children in alternate care, argues that for services to meet the needs of children with complex trauma histories, they should provide such wrap-around services alongside whole inter-governmental accountability (Tarren-Sweeney, 2014).
Core modalities in the Neuro-Physiological Psychotherapy model
The following core modalities have been integrated into the Neuro-Physiological Psychotherapy (NPP) model and are woven into the assessment and treatment programme. This synergy of therapeutic approaches is what gives this model its richness and potency. Synergising these core modalities enables the clinicians to respond in a neuro-sequential way to the child’s neurophysiological responses to stress and interpersonal relationships.
Sensory Integration (SI)
SI theory, developed by occupational therapist Ayres (1979), is based on the assumption that the brain is hierarchically organised, and normal development occurs sequentially. Ayres defined SI as ‘the neurological process that organises sensation from one’s own body and from the environment making it possible to use the body effectively within the environment’ (in Bundy, 2002, p. 4). Ayres believed that infants synthesise their environmental experiences to provide them with the foundations for SI development (Cermak, 2001). SI theory outlines the impact of early life experiences on regulation and motor development.
For children who have had adverse and traumatic life experiences in the womb and in early infancy, SI does not develop as it should and leads to sensory processing disorder (SPD). These sensory difficulties explain how, for some children, their nervous system struggles to take in sensory information and integrate it to support their ability to manage in the world. These sensory processing difficulties can have adverse effects upon self-regulation, movement, motor skill development, learning and interaction with others as well as the child’s capacity to engage and attend. This theoretical position provides a strong case for the use of SI techniques for children who have had significant early life trauma and who present with complex symptomatology that impacts their capacity to learn and develop positive relationships.
Koomar described how Developmental Trauma Disorder (Van der Kolk, 2005) ‘captures the multiple or chronic exposure to traumatic events over critical developmental periods; complex disruption of affect regulation and disturbed attachment,’and identified common features of SI disorder and trauma disorders (Koomar, 2009, p. 1).
SI difficulties can be seen in isolation or, more frequently, in combination with other diagnoses of childhood disorders. SI assessment and therapy as part of the NPP model is led by a Paediatric Occupational Therapist specialising in SI, but is practised collaboratively with other clinicians in the team, with the child’s parents and, at times, with school staff. The SI element of the NPP model focuses on improving the child’s ability to regulate and provides strategies for physiological regulation.
While little empirical research on the efficacy of SI in working with traumatised populations has been completed to date, a small study conducted by Kaiser, Gillette, and Spinazzola (2010) with adults with complex trauma found that an SI programme using auditory, visual and vestibular components resulted in positive changes on a number of outcomes including total scores for self-perception and affect/ impulse regulation.
Somatic experiencing and sensorimotor psychotherapy
Somatic experiencing (SE) was developed by Peter Levine (Levine & Kline 2006, Levine 2010) and sensorimotor psychotherapy by Pat Ogden (Ogden, Minton & Pain, 2006). Both of these therapeutic approaches provide clinical tools for working with trauma in the nervous system. Peter Levine’s work draws heavily upon studies of how animals process stress and how humans share similar stress responses but that these get inhibited, causing physiological and psychological distress. Ogden’s work has a particular emphasis on the need to complete the physiological cycle of stress resolution, which has become stuck or is incomplete. It is now widely recognised that instinctual fight/flight and freeze responses in traumatised children become their dominant response to stress, even once the original trauma has passed. Working with a child’s trauma in the nervous system requires attention to be given to the body and the child’s stress responses. The NPP model pays particular attention to the autonomic nervous system stress responses and body-based ways of supporting children to regulate and resolve these, now maladaptive, ways of managing stress in the here and now. A key part of the healing process is to help children transform feelings of hopelessness and numbness into empowerment and mastery. A combination of age-appropriate psycho-education and body-based work can help children as part of the NPP model make sense of their bodily responses and explore other ways of managing.
This body-based way of working is also relevant to the parent support element of the NPP approach as many parents either bring trauma issues of their own or are suffering from vicarious trauma due to the impact of parenting a traumatised child.
There is little empirical research into the effectiveness of somatic experience and sensory motor psychotherapy. However, a study of 31 participants conducted across two residential therapeutic units working with traumatised children aged 12–22 years found that compared to the treatment-as-usual group, the intervention group that received the Sensory Motor Arousal Regulation Treatment (SMART) model (Warner, Cook, Westcott, & Koomar, 2011) showed a significant reduction in internalising symptoms (p < .011) as measured by the Child Behaviour Checklist (CBCL) (Achenbach, 1991) following the SMART treatment programme (Warner, Spinazzola, Westcott, Gunn, & Hodgdon, 2014).
Theraplay
The Theraplay Institute was established in 1971 by Ann Jernberg and Phyllis Booth having grown out of their work in Chicago with the Head Start programme. Phyllis Booth had spent time in the United Kingdom as a student of John Bowlby, and Attachment Theory heavily influenced her work.
Theraplay is a child and family therapy aimed at building and enhancing attachment, self-esteem, trust in others and joyful engagement. It is based on the natural patterns of playful, healthy interaction between parent and child and is personal, physical and fun. Theraplay interactions focus on four essential qualities required for secure attachment relationships between the parent and child: structure, engagement, nurture and challenge. Theraplay sessions work towards creating an active, emotional connection between the child and parent or caregiver, supporting the child in developing a changed view of themselves as loveable and understood by the adoptive parent, in this context. This is achieved by the therapist guiding the parent in a series of very structured playful interactions with the child. These interactions are developmentally appropriate and attachment enhancing.
Theraplay has been used with a range of children with attachment difficulties including traumatised children who are adopted or fostered. Theraplay’s assessment tool, the Marschak Interaction Method (MIM), is also a key assessment tool used during the Family Futures assessment process to look at parent–child interactions. The NPP model integrates Theraplay in a pure form, with parent and child Theraplay sessions, and also as part of other family therapy sessions. Alongside this, Theraplay concepts are woven into the therapists’ thinking about parents’ strategies and thinking developmentally about the child and their needs.
As yet, no empirical research has been conducted on the use of Theraplay for children with developmental trauma or for children in alternate care provision. Wettig, Coleman, and Geider (2011) conducted a study of 167 children aged 2–7 years, including a clinical group with a dual diagnosis of social anxiety and language disorder and a non-clinical control group. The clinical group received a course of Theraplay (average 18 sessions). Before treatment, the clinical group had significantly higher symptom levels across all variables compared to the non-clinical control group. After the Theraplay intervention, measures of shyness, attention deficit, poor cooperation, mistrust and over-conformity in the clinical group decreased such that there were no significant differences between the intervention and control groups. For the treatment group, all variables showed significant decrease (p < .001) in post-treatment mean compared with pre-treatment mean scores. However, the findings are limited by a lack of a clinical control group.
A smaller study (n = 46) of primary school–aged children in Hong Kong which included a clinical control group was conducted by Siu (2009). Children who exhibited clinical levels of internalising behaviours (measured by the CBCL; Achenbach, 1991) were allocated to a treatment (8 Theraplay sessions) or wait-list group. The mean internalising scores decreased from pre- to post-treatment significantly more (p < .01) in the treatment group than in the control group with a large effect size (partial eta squared = .26).
Dramatherapy and the creative arts
The use of the expressive arts in therapy with traumatised children is a core feature of the NPP model. For children who have been traumatised, whatever their age, talking about their experiences and their feelings can be too overwhelming. Dramatherapy and the use of creative arts approaches (which covers the constellation of art, dance, drama, movement, music, play and puppetry) are the tools that Family Futures therapists use to facilitate the child’s expression of life experiences. Drama techniques come to the fore particular during life story work enabling children to bring their life story to life and interact with figures from their past as well as feel empowered to re-work elements of it (Vaughan, 2007, 2010).
These ways of working enable children to explore difficult and painful life experiences through an indirect approach. Dramatherapy, as with all of the creative arts, provides an ‘aesthetic distance’ through the modality of the art form, which facilitates safe exploration that feels manageable for the child. Dramatherapy provides a way for the feelings that the child embodies to be worked with and links with the emphasis in the NPP model on body-based and non-verbal intervention. This expressive arts approach is used not only with children one-to-one but also in the parent–child dyad and sibling and family sessions. The expressive arts provides a very powerful palate for enabling the child to find mediums through which they can feel safe, empowered and gain mastery of their feelings and an understanding of how these feeling impact all aspects of their being.
Academic research on dramatherapy is almost exclusively of a qualitative nature – taking approaches such as case study analysis (Folostina et al., 2015; Novy, 2003) or an exploration of the theory behind the practice (Pendzik, 2008). There are a small number of quantitative experimental studies on the effectiveness of dramatherapy (Anari, Ddadsetan, & Sedghpour, 2009; Mackey, Gold & Gold, 1987). These studies showed a decrease in problematic symptoms post-treatment, albeit with varying levels of statistical significance. Although dramatherapy is centred on non-observable phenomena such as creative processes and insight (Landy, 1984), there is a need for more rigorous research, with verifiable methods and treatment outcomes in order to evaluate dramatherapy and the efficacy of dramatherapy in working with developmental trauma and attachment.
Dyadic Developmental Psychotherapy (DDP)
The NPP approach is underpinned by DDP (Hughes, 2006) at all levels and aims to help the parent/carer and child to first develop a manner of open engagement that is characteristic of the parent–child attachment and intersubjective experiences at all ages, and then make the connection between their current emotional, cognitive and behavioural responses within their adoptive families and their past experiences within the birth family. This is done with the organising principles of Playfulness, Acceptance, Curiosity and Empathy (PACE) and affective–reflective (A-R) dialogue and further develops the intersubjective experience between parent and child. Given the high level of dysregulation of many of the children who present at the organisation, DDP may initially be in the background of the NPP treatment where the attuned, intersubjective relational engagement is interwoven with the body-focused activities so that the child may be more fully engaged with and better able to respond to such activities. DDP will also focus on the parents’ willingness and ability to safely facilitate their child’s attachment with them. The principles of PACE and A-R dialogue are fully present in direct sessions with parents alone so that they are more able to provide the home environment needed for their children to heal, resolve past traumas and learn to become engaged with them with attachment security. The approach aims to be non-intrusive and in a manner which facilitates the child’s development of integrative experiences through the co-regulation of affective states associated with stressful or traumatic events, along with the co-creation of new meanings of such events.
Initial research into the effectiveness of DDP in working with children in alternate care provision has been positive (Becker-Weidman, 2006) but can only be considered as pilot studies due to methodological shortcomings. Hughes acknowledges the need for further research to be conducted before DDP can be considered an evidence-based intervention (Hughes, Golding, & Hudson, 2015).
Life story work
Life story books are still the tool most used in facilitating the development of the child’s narrative and one that has been institutionalised by the social work profession and now enshrined in regulation. Life story books vary in form, content and quality. Their origins lie in research on baby adoptions where adult adopted people wanted more information about their past in order to address their ‘genealogical bewilderment’ (Humphrey & Humphrey, 1986).
Family Futures’ therapy model was informed by attachment theory. Two of Bowlby’s concepts – ‘internal working models’ and ‘coherent narratives’ (Bretherton, 1992; Pulkkinen & Caspi, 2002) – became central to the therapeutic work of the agency in its early days. In order for a child to bring into their conscious mind their internal working model of adults and for those models to be de-constructed and re-constructed, it is necessary that they are able to make sense of, and give meaning to, their early life experience. In order to do this, it is necessary that they should possess a coherent narrative. This coherent narrative gives a chronological account of people and places as per the life story book, but should also include feelings and conscious awareness of interpersonal relationships with significant others.
Life story work now has become one of the central therapeutic exercises undertaken during NPP, which incorporates the use of all the above-mentioned therapeutic modalities. The life story work will usually take the form of a large painting of the child’s lifeline on to which many aspects of their early life experience (much of which is obtained through extensive file searches) are given representation. During the process of the exploration of their lifeline, the child is helped to become aware of experiences and feelings and integrate them using various different treatment modalities supported by the adoptive parents as their primary attachment figures and affect and sensory regulators. This process is reworked and deepened at different stages of the child’s development (Archer & Burnell, 2003; Burnell & Vaughan, 2006, 2008). While a wealth of clinical experience testifies to the importance of therapeutic life story work for children, there is no research evidence for its effectiveness. The provision of words and a coherent narrative that goes some way to making sense of the child’s experience is considered to be an essential part of the NPP model.
Neuro-Physiological Psychotherapy framework
Working with the primitive brain
With its neuro-sequential theoretical basis and acknowledgement of the neuroplasticity of the brain in childhood (Schore, 2010; Siegel, 1999), the model’s therapeutic approach aims to enable the child to develop self- and co-regulatory strategies for emotional and physiological modulation. This is achieved through the use of sensorimotor (Ogden et al., 2006), somatic experience (Levine & Kline, 2006; Levine, 2010), SI (Ayres, 2005; Koomar, 2009) and play (Booth & Jernberg, 2009) techniques. The aim here is to help children develop alternate experiences and therefore, it is posited, neural pathways to the hardwired fight/flight or freeze responses developed in the context of persistent actual or felt threat in early life. Parents are integral to this regulatory work whether it is play- or body-based as this aims to further the child’s experience of being understood and having their needs met by them. As Burnell and Vaughan (2012) outline in their more detailed description of the model, because of the developmental insults the child has experienced, parents have to go back in order to go forward with their child developmentally. Parents are encouraged to engage in developmental re-parenting whereby they aim to meet the developmental needs of the child in the here and now (Siegel & Hartzell, 2004). Developmental re-parenting is a way of parenting that involves a parent thinking about the child’s needs developmentally rather than in relation to their chronological age. This is a parenting concept that developed in the field of fostering and adoption from the late 1990s onwards (Archer, 1999a, 1999b; Archer & Burnell, 2003; Burnell & Vaughan, 2012) and is based on attachment theory. Developmental re-parenting provides a way for parents to understand the needs of children from the care system who have a history of trauma and are considered to be developmentally traumatised with the trauma impacting all aspects of their development. Developmental re-parenting is based on the premise that the child’s history needs to be understood and then their behaviour made sense of in relation to this history and their development.
The impact of parenting a traumatised child on the parent’s own nervous system (Rothschild, 2006) is also addressed in treatment and parents are supported to become familiar with and able to regulate their own and their child’s nervous systems.
Working with the mid-brain
Once the child has, through his or her experience of developmental re-parenting, developed a greater capacity to both self-regulate and co-regulate with the support of their parents and therapists, the focus of the work can turn towards the attachment relationship. As the child is not always able to articulate their thoughts and feelings, at this stage there is a greater emphasis on the use of the creative arts as a form of expression of the child’s inner world. The child’s therapist and parents’ therapist then facilitate the exploration of the child’s inner world. The child is also supported to make connections between their past experiences and how the feelings connected to those manifest now. Both the child and parent are involved in this process. The parent is supported by the therapist to actively validate and sensitively respond to the child in an attuned manner using the principles outlined in the DDP approach. It is often the case that regulatory techniques that are directed towards more primitive brain responses of flight/fight or freeze will also be engaged. For example, parents may engage in SI techniques involving movement while these connections are made. Theraplay methods (Booth & Jernberg, 2009), in particular, are conducive to integration with DDP techniques at this stage. It too is attachment-focussed and aims to redress the absence of play in early years that typically promotes the formation of attuned parenting and secure attachment strategies in the child. This therapy is mid-brain-focussed which is where it is thought that attachment formation occurs (Perry, 2006), and it is through repeated experience and learning that the child experiences the parent as psychologically available and responsive to them.
Working with the cortical brain
An essential part of helping a child to come to terms with their early life experiences and their own template for relating is therapeutic life story work (Burnell & Vaughan, 2006, 2008, 2013; Rees, 2009; Rose, 2012; Ryan & Walker, 1999). This is a narrative form of therapy that is aimed at helping the child develop a coherent narrative of their whole life and helping them develop a sense of self and identity. It also aims to promote a more integrated view of their earlier experiences, which acknowledges positive experiences and perceptions they may hold of their birth family alongside the reality and experience of their neglect. It also aims to provide validation of what has been difficult and positive within their adoptive family. Life story work can be carried out in many formats and levels, depending on the child’s developmental needs. It can begin with puppetry, move to a three-dimensional (3D) format, such as model making, and then a more narrative format where the timeline is shown on a large roll of paper. Art and movement are used throughout to facilitate modulation of arousal levels and to allow processing. Again the child’s experience and feelings in response to the work are processed using the DDP approach. The therapist’s role is to remain sensitive to the needs of the child and parents, ensuring that both remain emotionally and physiologically regulated and that negative feelings are expressed and processed, while also noting and celebrating the positive. This process of encouraging the child to think about themselves in the context of what they now experience as a safe family with the use of objects, art, regulatory techniques and attuned therapy and care hopefully promotes left to right brain thinking whereby, it is thought, unconscious implicit feelings and experiences are consciously considered. The aim is that this facilitates higher order thinking and reflection and helps the child develop a more coherent narrative of their story and reflect on their identity. During this process, the core elements of DDP – attunement; mindful intersubjectivity and affective–reflective dialogue – come to the fore. What the model has done is replace an attachment theory of mind with a brain-based neuro-sequential approach in which attachment is a key element.
This process is carried out over a period of time that is dictated by the child and family’s needs and internal resources. This phase of work can overlap with that which is carried out in the second ‘mid-brain’ phase but less likely to occur in the earlier stages of therapy when the child is unable to regulate and might experience it as a further psychological assault and cause re-traumatisation. An exception to this would be if a clinical decision was made that it would be of benefit to the child and reduce their hyperarousal, but again, this would be at an appropriate level and pace.
Parent/couple therapy and support
The organisation believes that parents are central to any change the child can make. Parents must be aligned, consistent and authentic in their approach to their child. Therefore, parent therapy, psycho-education and support are key aspects of therapeutic success. There is a significant focus on this ‘parent work’ throughout the therapy programme. Parents are invited to explore the impact of parenting a traumatised child, their own attachment relationships and their coping mechanisms. They are supported to reflect on their own parenting history in order to understand their own unresolved attachment needs which may be triggered by their child’s attachment-seeking behaviour (Siegel, 2004). They are also provided with training and support to re-frame their understanding of their child’s behaviour and understand it as coming from a place of distress and fear (Forbes & Post, 2006; Post, 2009). The therapist aims to reduce the impact of secondary trauma for parents caring for traumatised children. They are supported to have compassion for themselves and understand that less attuned parenting responses or ‘blocked care’ behaviour towards the child has manifested as a result of the neurological impact of chronic stress on a parent (Hughes & Baylin, 2012) rather than due to any intrinsic ‘fault’ on their part. The provision of a safe and non-judgemental therapeutic space in which the therapists take the DDP stance of PACE promotes the parent’s experience of being held in mind, understood and contained. As well as modulating the emotional arousal of the parent, this also models the emotional environment the child demands from the parent.
Wrap-around service provision
Extended network support
Parenting traumatised children can often have a socially isolating effect. The model offers training and network liaison to the parent’s family and friend network to encourage understanding and support within their immediate system.
Professional network liaison
If parents are to offer containment to children, then it is essential that the network supporting them is both cohesive and containing. Across the model, the team works to maintain good collaboration and communication throughout the professional network to ensure consistency and continuity in treatment. This will also involve liaising at a higher organisational, sometimes governmental level and across health, social care and education bodies.
School consultation and support
The impact of developmental trauma on a child’s learning and peer relationships is an important factor in the model. In the organisation’s experience, responses and strategies developed in the context of maltreatment can cause problems in the classroom. Compliance and dissociative strategies can lead to children’s needs not being picked up until the transition to secondary school where their strategies collapse. Defensive, aggressive behaviours often lead to exclusion. These behaviours are considered as fear- and stress-based and consequently prohibitive of the cognitive functioning required to engage successfully in learning, including poorer executive functioning (Liston, McEwen, & Casey, 2009; Taylor, Eisenberger, Saxbe, Lehman, & Lieberman, 2006), working memory (Qin, 2009) and attention (Beers & De Bellis, 2002). The model’s approach is to work with schools to reduce child’s fear-based responses and promote good cognitive and executive functioning in the classroom. The treatment programme also aims to improve relational difficulties which interfere with the formation of positive peer relationships.
Multidisciplinary working, consultation and supervision
Central to the process is the multidisciplinary make-up of the team which ensures that therapeutic practice is integrative and fluid. The team models its own practice and regular formal supervision and processing, and reflective opportunities are provided to limit the impact of secondary trauma, which can otherwise have adverse effects on professional teams (Conway, 2009). Therapy team members also undertake their own therapy as and when appropriate.
Moving towards practice-based evidence
There is a paucity of research into the effectiveness of therapeutic interventions for children in alternate care provision, particularly interventions which aim to improve the quality of attachment between children and their caregivers. Recent National Institute for Health and Care Excellence (NICE, 2015) guidelines on attachment outcomes in the United Kingdom also point to the scarcity of both interventions and research on interventions which address attachment difficulties in children in alternate care provision. It is essential that the NPP model, like any other, is able to evidence its efficacy. This process has begun and an evaluation of NPP exploring treatment outcomes is presented in a companion paper (McCullough, Gordon-Jones, Last, Vaughan, & Burnell, this issue).
Footnotes
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.