
Abstract
Dyadic developmental psychotherapy (DDP) is an attachment-focused therapy frequently used with adoptive and foster families. While the evidence base for DDP is building, national guidance has called for further trials and qualitative evidence. This study aimed to understand the experience of adoptive parents who have completed DDP therapy. Semi-structured interviews with 12 adoptive parents were analysed using interpretative phenomenological analysis. Four superordinate themes were identified: (1) increased understanding, (2) ‘It’s a different method of parenting generally’, (3) the DDP journey and (4) ‘It’s a shared kind of experience you go through and come out together’. Parents felt they had increased insight into their child’s mind and how to better support their child. They felt DDP was a good fit to their unique situations and it appeared to promote acceptance. The DDP journey started with parents feeling uncertainty and questioning the effectiveness of DDP. However, generally parents became committed to the therapy once they saw change and expressed fear and sadness at ending. Parents acknowledged the dyadic nature of DDP, feeling it helped build trust and security and supported co-regulation. Parents also acknowledged the therapist’s role in conveying the core DDP principles. Further implications for practice and research are highlighted.
Keywords
In 2015, the National Institute for Health and Care Excellence (NICE) outlined several interventions thought to be useful when supporting young people with attachment difficulties. However, due to limited good-quality evidence, NICE (2015) have recommended that randomised control trials (RCTs) and qualitative research are conducted into parent and children’s experiences of these therapies. One intervention specifically noted by NICE (2015) is dyadic developmental psychotherapy (DDP). DDP works with ‘a specific type of complex trauma that primarily focuses on the effects on a child who experiences abuse and neglect early in life at the hands of his or her parents or caregivers’ (Hughes, 2014, p. 2). This type of trauma is likely to have occurred for children who are fostered or adopted from care as they are more likely to come from families with disordered lifestyles (Golding, 2010), with increased risk factors, such as living with parents who experience mental illness, domestic violence or drug and alcohol use (McAuley & Davis, 2009). Attachment theory predicts how maltreatment can deeply impact an individual’s sense of self, affect regulation and their capacity to enter into mutually beneficial reciprocal relationships (Bowlby, 1988). There is ample evidence that early disruptions in care can lead to a range of maltreatment-associated psychiatric problems (Mikulincer & Shaver, 2013) and DDP aims to support families where these difficulties are present.
The primary treatment goal in DDP as a therapy is to facilitate attachment security between the child and parents. This is achieved by using here and now intersubjective experiences in the therapy room to discover positive qualities in the child, provide emotional regulation, and facilitate a new understanding of why the child has needed to use distrustful, defensive and controlling behaviours in order to keep safe. (Casswell, Golding, Grant, Hudson, & Tower, 2014, p. 20)
The therapeutic stance is one of playfulness, acceptance, curiosity and empathy (PACE), to bring elements of secure attachment to the interaction with the child to facilitate co-regulation and co-creation of past experiences between the parent and child (Hughes, 2014). DDP is one of a number of therapies reported to be widely used in UK adoption services including play therapies, filial therapy, theraplay, and dialectical behaviour therapy (Stock, Spielhofer, & Gieve, 2016). While DDP has a research base, using elements found in effective therapies and addressing evidential effects of maltreatment (e.g. Hughes, Golding, & Hudson, 2015; Turner-Halliday, Watson, Boyer, Boyd, & Minnis, 2014) and evidence for DDP-informed interventions for care-givers and adoptive parents are positive (e, g, Selwyn, Golding, Alper, Gurney-Smith, & Hewitt, 2016), to date there has only been one evaluation of the therapy (Becker-Weidman, 2006). Although positive in their findings, the study lacked robust methodology and so, at best, can only be considered promising (Becker-Weidman, 2006). Reviews of studies of psychosocial interventions for adoptive families consider the field of interventions for adoptive families lacking in more robust, methodologically sound studies of any intervention with DDP therapy being no exception (Harris-Waller, Granger, & Hussain, 2018). In seeking to develop the evidence base for DDP therapy, a stepped approach to understanding the effect of DDP has been initiated. Qualitative interviews with services using DDP therapy have been conducted to establish the provision of this intervention in the United Kingdom (Turner-Halliday et al., 2014) including economic viability analysis for an RCT of DDP therapy (Boyer, Boyd, Turner-Halliday, Watson, & Minnis, 2014). These studies concluded that funding a trial of this nature could be rationalised and supported. In recognition of the need for ‘theoretically informed outcome measurement’ of therapies for adoption (Harris-Waller et al., 2018, p. 17) and in line with the call by NICE (2015) for both qualitative and quantitative methods of DDP therapy, a qualitative study of the experience of receiving DDP therapy was seen as building the theoretical rationale for future quantitative studies including a potential RCT.
This study aims to understand the experience of adoptive parents, as co-participants of the therapy, who have completed DDP with their child. Although DDP is used frequently with both adoptive and foster families, it is felt that adoptive and foster parents may have different experiences of DDP since in adoption the legal relationship between child and birth parents is terminated and an equivalent relationship is made with the adoptive parents (Cullen, 2003). It is hoped that by studying adoptive parents in the first instance, as an homogeneous group, experience of parents with permanent legal responsibility for their child can be gathered and further research can be conducted with other groups receiving this intervention.
Method
Design
Semi-structured interviews with 12 parents from 12 separate families were analysed using interpretative phenomenological analysis (IPA). IPA allows for the interpretation of people’s lived experience and the personal meaning given to them (Smith, Flowers, & Larkin, 2009) and to allow for comparison, was the same methodology was used in a qualitative study of adoptive parents who received a DDP-informed parenting group (Hewitt, Gurney-Smith, & Golding, 2018). Given that the methodology aims to gather detailed interpretative accounts of individual transcripts, IPA allows for a small sample size to gain in-depth perceptions of a specific group as opposed to making more general claims (Smith & Osborn, 2004).
Participants
The following inclusion criteria were used to enhance sample homogeneity (Smith et al., 2009):
Adoptive parents who completed DDP with a certified DDP clinician or clinician becoming certified;
Who completed at least six DDP sessions;
Who completed DDP within 12 months of interview to ensure good recall;
Who had capacity to give informed consent as judged by the clinician and interviewer.
Participants were excluded if they were biological or foster parents or if their children were over 18 years old.
Measure
A semi-structured interview schedule was established in line with IPA (Smith et al., 2009) ensuring questions were open and expansive. A DDP clinician and an adoptive parent who was undergoing DDP reviewed the interview schedule to ensure relevant questions were included. This parent also underwent a pilot interview resulting in a number of the questions being reviewed to allow for more open responses. This interview was not included in the data.
Procedure
Recruitment
DDP practitioners were identified using the online DDP network. Clinicians were emailed about the project and asked to provide information to potential participants. Parents were able to opt in by contacting the researcher or clinician. If interest was expressed, the clinician gained the parent’s consent to pass on contact details to the researcher or the parent was able to contact the researcher directly. Participants were given at least 24 hours before they were contacted to allow the researchers to answer any questions. If parents were happy to partake, they were given a consent form. Participants were offered £10 for participation.
Interviews
The researcher conducted all interviews, lasting between 41 minutes and 1 hour 19 minutes (M = 57.85 minutes). Interviews were conducted via video call (n = 10) or face-to-face (n = 2).
Data analysis
Analysis was carried out in accordance with Smith et al. (2009). Each transcript was considered individually to ensure analysis remained idiosyncratic (Smith et al., 2009). Initial listening to and transcribing of recordings helped enter the participants’ world. Transcripts were read several times before notes were made against the data looking at language, content and providing comments on the individuals’ experience. Emergent themes developed by reducing notes into portions of data that represented key concepts. This process was repeated with each transcript and similar patterns across cases were noted. Themes that were not confirmed by other transcripts were removed or assimilated into other themes. Connections across themes were then mapped to produce a set of superordinate and subordinate themes. Convergences and divergences were recognised in line with the IPA principle that participants’ experiences have similarities and differences (Smith et al., 2009). Names were given to themes in an attempt to capture participant’s main concerns within interviews. This was, in four cases, felt to be most accurately captured by participant’s own quotes.
Reflexivity
IPA recognises that researcher biases, values and interests can impact interpretation. A bracketing interview was conducted prior to interviews to allow the researcher to bracket prevailing assumptions, biases and to understand how their subjective experience may impact analysis (Rolls & Relf, 2006). In addition, the researcher completed a reflexive log throughout.
Quality and credibility
Yardley’s (2000) quality criteria for qualitative research were followed. IPA supervision groups allowed for discussions on credibility and for peers to complete credibility checks on themes. The DDP clinician who reviewed the interview schedule also completed a credibility check. This supported triangulation, allowing different perspectives and interpretations of the data to be captured.
Ethical considerations
The Oxford Central University Research Ethics Committee approved the project. Participants were informed that the study was voluntary and that their care would not be affected by their decision around taking part. Participants were told the researcher may need to disclose information if there was concern of harm to self or other. Participants were given an idea of interview content and informed they did not have to answer any questions they did not want to. Support was offered post-interview if needed. Transcription omitted any identifiable information.
Results
Situating the sample
In accordance with IPA, a small, homogeneous sample of 12 adoptive parents (7 mothers, 5 fathers) were recruited. Parents’ demographics can be found in Table 1. Average age was 47 years (37–61 years) and the majority of parents were heterosexual and married (n = 8). Two parents were in homosexual relationships, one parent was a heterosexual widower and one was a single parent. Eleven parents identified as White British and one identified as Indian. Number of estimated sessions ranged from 8 to 43. Time since adoption varied from 1 to 12 years. One family had DDP support from the point of adoption and the longest period of time between adoption and the DDP referral was 11 years. Time since therapy ended to interview ranged from less than 1 to 12 months.
Participants’ demographic information.
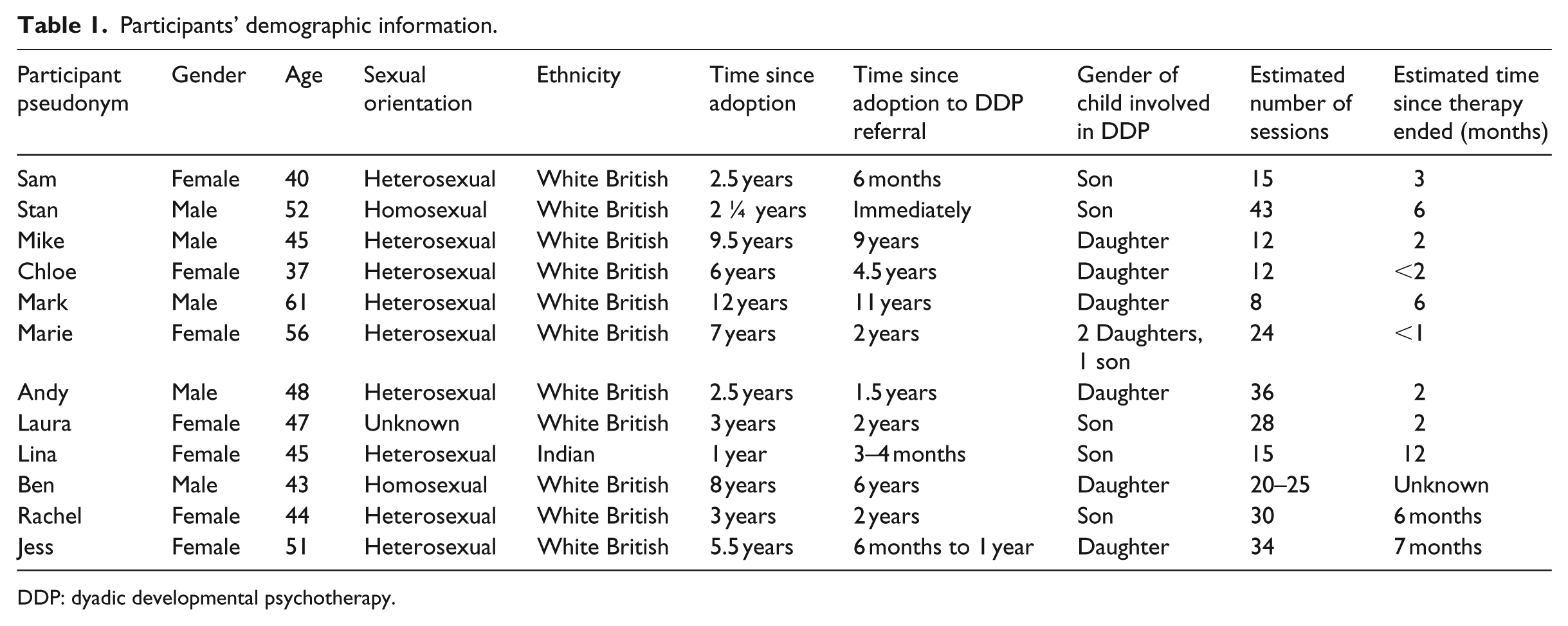
DDP: dyadic developmental psychotherapy.
Overview of themes
Analysis revealed 4 superordinate themes and 10 subthemes, seen in Table 2. The degree to which participants endorsed these is demonstrated in Table 3.
Superordinate and subordinate themes.
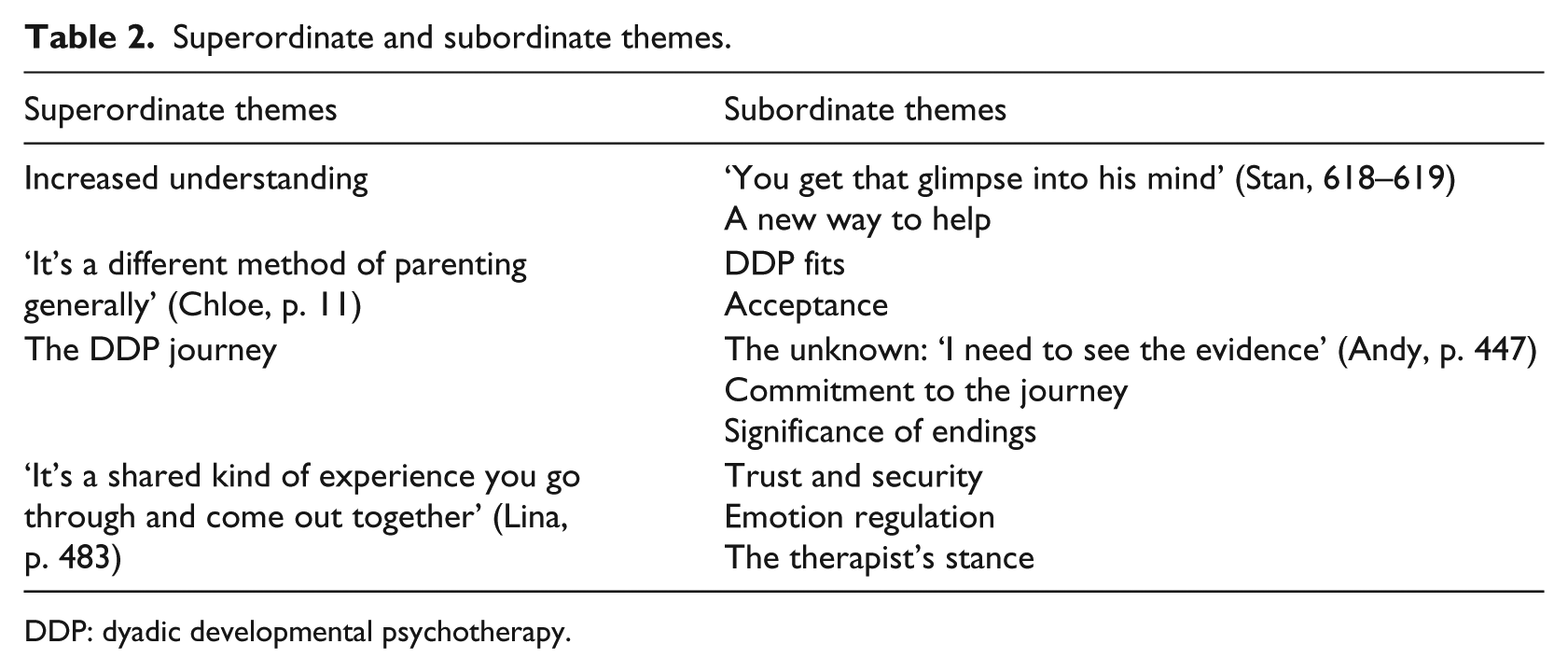
DDP: dyadic developmental psychotherapy.
Endorsement of superordinate (in bold) and subordinate themes by participants.
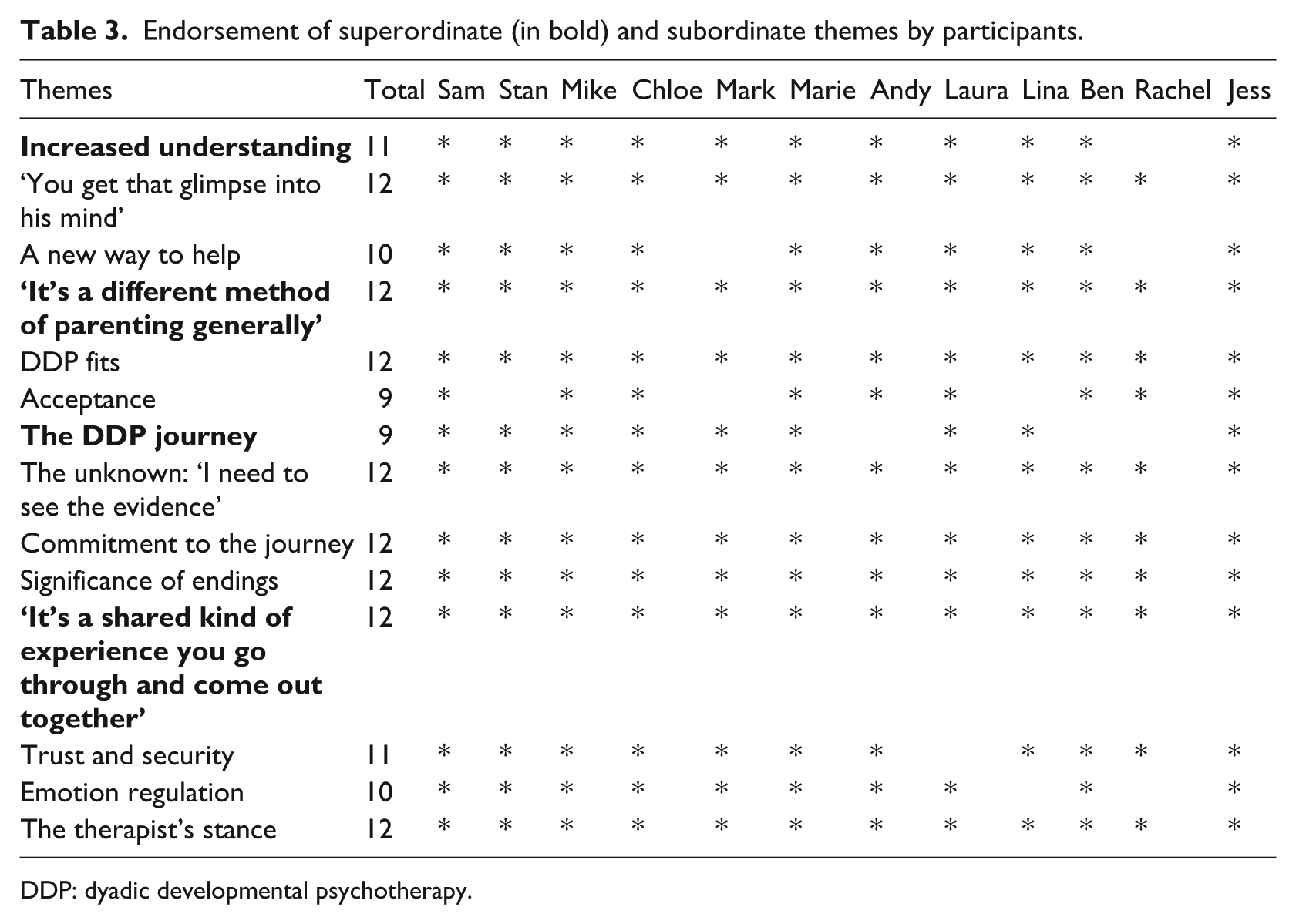
DDP: dyadic developmental psychotherapy.
Increased understanding
All but one parent described gaining a better understanding of their child and increased curiosity about their child’s mind. This fresh insight provided parents with a new way of working in terms of strategies, skills and techniques to support their child.
Part of it was understanding why Lilly was feeling the way she was feeling, why she was presenting the way she was presenting. . . Richard drew a picture of the brain and talked about the three parts. . . so we understood that actually, for the first time, that because of how Lilly’s brain is different, normal sort of parenting doesn’t work. (Mike, pp. 87–93)
Mike highlights how developing a deeper understanding of his daughter allowed him to be curious about what her behaviour was communicating. This curiosity may be something particularly prominent for adoptive parents who do not experience their child’s early life and so are left trying to understand their history and the impact. Sharing the neurodevelopmental effects of maltreatment appear to have provided a potentially more organic basis to explain some of Lilly’s behaviour, removing blame and helping Mike to realise he may need to respond to Lilly differently.
Parents linked increased understanding to a better awareness of their child’s pre-adoption history. In many cases, the significance of their child’s past was brought to light during DDP: But because she was 14 months when she came here, naively I thought she’d have no recollection necessarily of what went before and wouldn’t have experienced things that would cause her problems going forward, at first. (Chloe, pp. 185–188)
In Chloe’s case, understanding the past helped make sense of current ‘problems’. Parents spoke of assuming their child would not recall early experiences, perhaps due to difficulty accepting that they may still struggle with their trauma. It may also be that accepting the trauma means acknowledging more deep-rooted difficulties with longer term implications. For many parents, accepting and gaining insight into their child’s history helped them see how their child saw themselves: Luke’s biggest problem is that he doesn’t like himself. . . he thinks he has a dark heart, his heart must be black because they made him. (Sam, pp. 108–111)
For Sam, understanding how Luke saw himself enabled her to recognise that his difficulties may come from a place of self-loathing.
Exploring the child’s past relationships also helped parents make sense of the child’s current relationships, ‘the trauma was predominantly from his mother so he was very, has been very, very frightened of me at times’ (Sam, pp. 61–62). Sam identifies that their relationship can be difficult, due to the influence of Luke’s harmful relationship with his birth mother. Many parents also gained insight into what was missed in their child’s early life and the importance of trying to address this in therapy: And there’s quite a lot of pampering so, um, rubbing moisturiser into feet or hands or arms and stroking and combing hair and things. Lots of kind of, just, physical touching, sensory stuff and just the kind of things you might do to a baby. Um, to give her that sort of nurturing that she missed. (Andy, pp. 303–307)
It’s lovely to have a formula because we had nothing before . . . Whereas now there is, there is a bit of security as parents as well. You know, you’re just going along following how your parents were and how you’ve watched other parents and it don’t fit, it doesn’t fit our children. (Marie, pp. 94–99)
Marie’s use of ‘formula’ suggests having a useful solution to something that was initially incomprehensible. Knowing how to support her children also provided security for her, suggesting parents felt more contained. She describes responding to her children in the same way she had been responded to, but realising this did not fit her children, given their traumatic histories. Increased understanding allowed parents to stop, reflect and attempt to understand behaviour: It’s that ability to reflect, that ability to sort of stop, that ability to not, not assume that actually Katie’s just doing it to be a bit bloody-minded, that actually she can’t help herself, you know, this is pre-determined, this is about her own, her own early trauma and the impact that early trauma is having on her now. (Ben, pp. 527–531)
Here, Ben describes seeing Katie in a different light. By understanding her history, blame is reduced and he becomes more forgiving. Ben has been given the autonomy to stop and reflect rather than feel he urgently has to respond. Stan later describes this as different to how he responded before: For us, it was vital, it was vital for the success of this placement, you know? It gave us the skills and the tool sets we needed to understand Jack and try and help him on his life journey, you know? . . . and for us to remain sane really and to understand where he was coming from. (Stan, pp. 718–724).
‘It’s a different method of parenting generally’
This theme incorporates parents’ descriptions of DDP as different, experiencing a ‘eureka moment’ (Mike, p. 111) where something ‘clicked’ and DDP felt like a fit for their family. Parents cited acceptance as a key component, which made DDP different to other interventions.
Every parent described getting to a place where they felt Like trying to bang a square peg into a round hole. The only way it would work is if you smashed it so hard that you just turn the square peg into a round peg by breaking things off it and that’s not right. (Mike, pp. 539–542)
Mike describes discomfort at attempting to force-fit other approaches for Lilly using the brutal metaphor of banging a square peg into a round hole, whereas DDP was described as follows: a very natural approach. It felt as though it was very focused on our situation and the challenges we were facing, so it didn’t feel like something was being force-fit. (Mike, pp. 8–10).
This description feels much less forceful and natural, describing DDP as personal to the families’ difficulties.
And realising that when they’re having a meltdown it’s not a matter of telling them ‘stop having a meltdown’, it’s about sitting next to them and being very sorry that that’s how they are feeling. . . and going through the PLACE. To start off with it was not my style, at all. I wanted to put a band-aid over it and say ‘come on lets go and sing’. . . let’s make everything fun. (Marie, pp. 541–548)
Marie describes realising that trying to stop distress was not helpful and learning to validate and sit with her children’s emotions, supporting them with playfulness, love, acceptance, curiosity and empathy (referred to as PLACE). Some parents described feeling initially uncomfortable about not reassuring their children straightaway. Children were also described as seeing themselves differently but starting to accept themselves: Katie is better able to tackle life day-to-day, she’s more open and she is um, she has a better understanding of who she is, of her own identity and how she works. And actually she knows that in certain situations she will freeze but actually that’s ok, these are the strategies she can use to be able to move on from that. (Ben, pp. 590–594)
Here, Ben notices his daughter’s increased insight into who she is and that this has helped her accept that she is ‘ok’. She is described as more open, possibly because she feels safer to express herself, knowing others can support her. Child self-acceptance also emerged when children gained insight into how their parents saw them: He knows we know that story and we know everything and we’re still there and we still love him (Marie, pp. 335–336)
Overall, increased acceptance allowed challenges to become a part of family life rather than a struggle: It’s about accepting it for what it is and not trying to make it something different. You’re just trying to make it feel better for everybody. And until we got to that, I think all this other lovely stuff has come from it. . . As opposed to ‘I will make that happen because that’s going to be lovely’ it was more ‘oh this is happening and it just is lovely’ and that spontaneity has just become a really big part of our family now. (Chloe, pp. 794–801)
Here, Chloe describes accepting life with her daughter as she is and eventually struggling less with trying to always ‘make it feel better’. This ethos appears to have disseminated into everyday life.
The DDP journey
Most parents described undergoing a ‘journey’. Parents described initially knowing very little about DDP and questioned its validity initially. This phase seemed to come to an end when parents saw evidence of its progress, becoming committed, despite difficulties. All parents also spoke about having significant feelings about ending treatment.
And we were sceptical for a while, until something clicked. . . We went willingly, feeling very lucky that we got access to it, we didn’t let our cynicism, scepticism, whatever it is, sway us. (Mike, pp. 72–76)
Mike’s scepticism may be linked to the experience of other approaches that had failed them before or more general cynicism associated with therapy. Despite this, Marie highlights the vulnerability in making a decision about what help she needed: We would have jumped off the Empire State Building if someone had told us it would have worked for them. (Marie, pp. 151–152)
All but one parent felt that after some time, progress became evident. This was in the way their child started to feel about themselves and others, their improved ability to manage emotions, increased empathy, openness and sense of security. These changes led to more tangible progress such as improved sleep, less behavioural difficulties, placement stability and better peer relationships. Progress led a handful of parents to conclude that DDP ultimately kept the family together: The placement would have likely broken down because I don’t think I could’ve coped with it having no understanding what was going through his head. (Stan, pp. 300–302)
However, one parent, Rachel, still felt she hadn’t seen the progress she had hoped for at the end of therapy. Rachel later questioned whether DDP had been the right approach for her and the needs of her son: I realise that I’m a fixer, I want to fix things and I understand that the treatment wasn’t ever to fix these things but to bring them up and kind of explore them. . . but ultimately the issues that we had are the same, they haven’t changed. (Rachel, pp. 312–315)
She put this down to wanting a ‘fix’, which contradicts the feelings of acceptance that other parents identified.
I’ve got a demanding job and finding time in the diary, to, to do this amidst all else was challenging but worthwhile. (Mark, pp. 145–146)
Mark highlights that the therapeutic process takes time, linking back to the idea that there is no ‘quick fix’ for attachment difficulties, given the ‘fix’ is likely to be relational. A number of parents also described some discomfort during sessions, learning to speak to their child in a different way and completing therapeutic activities, which felt odd and unnatural to certain parents, ‘I think some of the things we were kind of having to do did feel quite unnatural’ (Lina, pp. 185–186).
DDP was also described at emotionally difficult for both parent and child during and after sessions: We’d both be exhausted afterwards, you know? I’d keep him off school afterwards because he’d just be so upset. . . And I found it really hard seeing how difficult it was to hear from another person, the stuff that had failed him (cries). I found that really, really hard. (Laura, pp. 582–596)
Here, Laura highlights how emotionally exhausting DDP was for her son. Laura also highlights how difficult it was for her. Some also described how difficult it was to acknowledge their own attachment histories and to be reappraising themselves as parents. Despite the difficulties, all but one parent stated that DDP was worthwhile: You’ve got to stick with it. Because whilst it may not seem to be going anywhere or may not seem to be right, it’s preparation that’s well worth investing in. (Mike; pp. 250–252)
Like an investment, Mike suggests that commitment and trust in the process are required to get a profitable return. Furthermore, it seemed that the hard work continued after sessions as described by Ben’s swan analogy: I use that swan analogy that our children do glide through, um, and everybody goes ‘they’re so wonderful, they’re so engaging, they’re so brilliant’ and you go ‘you have no idea how hard the legs are going underneath to be able to, just to be able for them to keep up’. (Ben, pp. 254–257)
The Do you know it was really nervy because you get used to knowing you’ve got that sounding board, knowing that she’d always impart a gem of wisdom. . .and just knowing we were going it alone almost was a little bit daunting. But very quickly you then get home and you realise that you’re the master of your own destiny and you just crack on. (Chloe, pp. 671–675)
Here, Chloe describes anxiety possibly linked to feeling that the ‘therapist’s wisdom’ may have not become internalised. Parents perhaps lacked confidence in their ability to progress alone. However, Chloe soon realised she is a ‘master’ in her own way and takes control: So it’s not just the therapy happens in that room, the therapy happens, not continuously. . . I’m not that good, you know what I mean (laughs). . . but it happens more generally through our lives. (Laura, pp. 53–55)
The therapy appears to have been focused on families’ day-to-day lives and therefore could be continued even once the sessions ended. In some cases, the therapist was mindful of the impact of endings and treated them as a celebration, providing the child with a positive experience of ending a relationship. Most parents were also mindful that their children may require therapy in the future and that DDP provided a good grounding for this, ‘DDP ain’t the end, that’s the thing as well, DDP is the beginning’ (Marie, p. 848).
‘It’s a shared kind of experience you go through and come out together’
Parental involvement appeared important to all, mainly because it enabled strengthening of the parent–child connection and allowed parents to support children. However, the therapist was also identified as an important part of the process and relationship.
Well, I think there are very specific issues faced by adopted children aren’t there, to do with attachment . . . and it affects behaviour, attitudes towards relationships. . . so finding that security in relationships is doubly important really. (Mark, pp. 386–401)
Mark senses that attachment is at the core of his daughter’s difficulties, realising that the remedy is in their relationship. He felt that as their relationship improved, so did his daughter’s sense of security with others: My hunch is it’s because she feels more secure with me, that she feels more able to be relaxed and out-going towards others. . . I think it’s her feeling of security which enables her to open up and to blossom really. (Mark, pp. 367–371)
Mark describes his daughter building a safe base with him, providing a security from which she can flourish. Lina describes how such trust was built during exercises: He had to jump off the cushions into Will’s (adoptive father) arms and my arms or whatever. And that might seem like fun but there was an element of risk there for him, you know? He’d kind of get through and see you know, actually they will be there for me and catch me. (Lina, pp. 302–305)
Lina describes how her son physically had to let go and trust his parents but that this transcended into beginning to trust them emotionally.
I want them to recognise they’ve been heard and because I’ve just done that and I’ve just articulated to Bella that I totally get what she’s just been feeling and what she’s described to me, but I’m not fixing it, it means she feels she’s at one with me, so she is there with me. (Chloe, pp. 875–878)
Chloe and others described that children’s expression of emotion could feel extreme, unpredictable or even ‘shut off’. However, here she notices that her children need to feel heard, possibly because they have had experiences of not feeling heard in the past. ‘Fixing it’ did not seem to help but confirming the emotion, sitting with it and managing it together did. In addition, parents described gaining better insight into their own emotional reactions and how this affects their child: The adrenaline goes up and the natural instinct is to shout at them . . . And it’s reining that back and it takes a lot of self-control. . . And again Sonya was able to teach a lot of techniques, you know? Singing nursery rhymes, yes it calms him but it actually calms yourself as well. (Stan, pp. 181–186)
Stan notices that the therapy has also helped him. He becomes aware that he can be quick to react and implies that his daughter is affected by this heightened emotion. Better understanding of his own reactions helped with self-control, and this was truly a shared experience in that emotion regulation techniques were effective for both parent and child.
Every parent spoke about Tina was quite skilled at pitching it at a level that Eloise wouldn’t find too threatening because, of course, if someone’s defended the last thing you want to do is challenge that defendedness too early. So she was very good at making it um, including sort of playing of games and making it fun really and Eloise responded to that. (Mark, pp. 126–130)
Mark highlights how difficult it was to accept and openly discuss Eloise’s early life. It was therefore important that Tina made the environment safe and playful. Jess describes how the therapist’s curiosity helped enhance her own curiosity about her daughter’s mind: So if I watch Jade talking to Jasmine I can see that she’s genuinely trying to think of why she’s thinking, why she’s feeling like that, which made me think why is she feeling like that, why is she thinking like that? (Jess, pp. 363–365)
Parents also spoke about the therapist being an important support for them. Chloe describes how her therapist’s non-judgemental attitude helped her feel reassured about her parenting: Very accepting and non-judgemental, which we had hoped for but not necessarily expected. . . she never made us feel in any way that we weren’t competent parents. (Chloe, pp. 517–522)
Other parents described that having another separate mind helped them to think: But I mean the main thing is, it’s somebody sitting outside, so, you know, we’re too close to it and we’re trying to react to our child, and we don’t have the brain space, I suppose. (Andy, pp. 329–331)
Andy describes the therapist as someone able to think when his thinking became clouded by emotion.
Discussion
This study aimed to understand the experiences of adoptive parents who completed DDP with their child. Four superordinate themes were revealed. These included parents feeling DDP gave them increased understanding of their child and that DDP was different to anything they had tried before. Parents alluded to their feelings about DDP shifting and developing, like a journey. Finally, DDP was reflected on as a shared experience. Although the sample and interventions varied in terms of time since adoption and length of DDP treatment, relatively consistent experiences were described. Below each superordinate theme is considered in relation to theory and research. Finally, limitations are considered and implications for policy, care and research discussed.
All but one parent explained that DDP helped give them a better understanding of their child. Caregiver’s understanding of the child’s mind and emotional state is characteristic of many attachment-based interventions and is consistent with the DDP approach (Hughes, 2011). It is hypothesised by Goldfinch (2009) that increasing parents’ understanding of their child can reduce blame and ‘increase their effectiveness in managing the behaviour. . . helping the child learn to calm down and better regulate emotions’ (pp. 292). This is echoed in parents’ experiences in that better understanding helped to remove blame and help parents know how to best help their child. Luke, Sinclair, Woolgar, and Sebba (2014) note that interventions are most likely to be effective when they focus on developing relationships and understanding and it appears that this effective component of therapy was highlighted in parents reports of DDP. Parents also acknowledged feeling that their child’s brain was ‘different’ and this fits with the DDP approach, which emphasises an understanding of the neurodevelopmental effects of maltreatment on autobiographical memory (McCrory et al., 2017), threat processing (McCrory et al., 2011) and emotional regulation (McCrory et al., 2013). Difficult attachment relationships are also known to have an impact on self-worth and developing self-cohesion (Mikulincer & Shaver, 2013) and parents spoke about getting a better insight into how their child saw themselves, allowing them to empathise but also respond to their child effectively.
Parents experienced DDP as a very different approach to anything they had tried before. This fits with DDP’s development, where Dan Hughes identified that a different approach was required for treatment of developmental trauma (Hughes, 2014). Traditional behavioural approaches are not considered to accommodate the neurodevelopmental effects of maltreatment (e.g. Casswell et al., 2014). Parents described DDP ‘fitting’ their situation and suggest DDP has face validity for them. Acceptance in DDP was a key concept noticed by parents, which they found different to other approaches they had experienced. Parents spoke about acceptance of the origin of their child’s distress and not trying to ‘fix it’ immediately. This is consistent with other therapeutic approaches, which place acceptance at their core, such as mindfulness or acceptance and commitment therapy (Baer, 2015).
The therapy was described as ‘a journey’ which began with an initial ‘cry for help’, linking to the emotional, behavioural and relational difficulties we may expect to see in children who have experienced difficult or disruptive early attachments, which are felt by their adoptive parents (Harris-Waller, Granger, & Gurney-Smith, 2016; Mikulincer & Shaver, 2013). Parents identified with feeling so overwhelmed they were willing to try DDP despite it being relatively unknown to them. This fits with recent research showing that although adoptive parents report increased stress and perceived child difficulties, very few were receiving service input (Harris-Waller et al., 2016). In the same way, parents initially felt sceptical about how DDP could help and with a limited evidence base to date for DDP therapy (Turner-Halliday et al., 2014), it is reasonable that at this stage, parents and therapist will have had little information about this to discuss before treatment began. This theme is also reported by Hewitt et al. (2018) in adoptive parents completing a DDP informed group.
Over time, all but one parent felt DDP was suitable to their needs and led to positive change. The DDP logic model (Turner-Halliday et al., 2014) identifies a number of long-term attachment goals and many of the ways in which parents recognised progress link with the goals identified in the model. For example, joint affect regulation, acceptance of comfort, feeling better able to manage conflict, making sense of the child’s experiences and gaining insight into the child’s history. In many cases, this led to parents feeling committed to the DDP ‘journey’, which may have resulted in families receiving a more effective intervention, with Luke et al. (2014) reporting that high levels of commitment to the approach can enhance efficacy. Alternatively, in one case, Rachel felt she did not see the progress she had hoped for. This may be explained by the diverse range of complex needs experienced by looked after and adopted children, meaning there is still not complete certainty about who is most suitable for DDP (Turner-Halliday et al., 2014). As with all psychotherapy, one size will not fit all (Roth & Fonagy, 2013).
Parents also referred to DDP being emotionally challenging but worthwhile. Parents reported that DDP brought about difficult emotions for their child, emphasising the importance of the therapist maintaining a ‘therapeutic window’ to avoid either insufficient or overwhelming activation of affect (e.g. Casswell et al., 2014). In addition, given that DDP encompasses resolution of caregiver attachment strategies before supporting the child with theirs and involves the active participation of the parent as the attachment figure (Hughes, 2014), it is unsurprising that DDP fostered emotional engagement for parents. The majority of parents spoke about joint emotion regulation. This is another key element of DDP, referred to as co-regulation (Hughes, 2011). It is important since theory suggests that when parents’ stress levels rise, they can lose their capacity to provide ‘empathic, attuned caregiving’ (Casswell et al., 2014, p. 22), described as ‘blocked care’ by Hughes and Baylin (2012). DDP therefore aims to support co-regulation of affect through parent–child attunement, which is crucial to developing self-regulation (Schore, 2001). This also supports the DDP logic model, in which increased co-regulation is one of the core mechanisms of DDP (Turner-Halliday et al., 2014). This was also found in a qualitative study of adoptive parents who received a DDP-informed group (Hewitt et al., 2018). This may be a common mechanism to examine in future qualitative studies of both DDP therapy and practice. Clinically, this reinforces the practice of DDP to ensure the regulation of the parent is considered in this work and that parents feel supported before and during therapy as described in similar transactional and dynamic approaches (Mackler et al., 2015).
Each parent also spoke about having significant feelings about ending treatment. Anxiety experienced could be due to parents feeling ill equipped to continue the work, concerns about availability of other support/services in adoption or their sadness might have reflected a more general struggle with ending relationships. Parents may have also come to accept the longer term nature of attachment difficulties as shown in research, which suggests that although many adoptees ‘catch-up’ with their peers in terms of physical growth, they may have more attachment insecurity and disorganisation in the longer term (Van IJzendoorn & Juffer, 2006). This finding was also mixed with most parents also describing a readiness and acceptance of the need to move on with family life and to embed the approach at home.
The shared experience of DDP was relevant to every parent’s story. This fits with the significance of ‘intersubjectivity’ within DDP to create a shared, reciprocal experience that is often missed in early neglectful or abusive relationships (Casswell et al., 2014). An environment in which trust and security between parent and child could develop was crucial to the process, supporting the idea that the child’s relationships are key to helping them (Turner-Halliday et al., 2014). There have been concerns in previous writings that attachment-informed therapies may encompass practices to establish adult authority, such as holding (Mercer, 2015). Such practices were not reported by any of the parents and indeed many identified DDP as being child-led, meeting the needs of their family with good results and in a climate of safety.
Finally, parents spoke about the importance of the therapist creating safety, modelling PACE and being a ‘separate mind’ when parents became overwhelmed. Mikulincer and Shaver (2013) suggest that if attachment insecurities are risk factors for psychopathology, then creating a sense of security, especially within attachment relationships, is important for improving resilience and mental health. Parents’ experiences of therapists creating a safe environment highlights a setting within which secure relationships could flourish possibly assisting their regulation to remain engaged with their children. Connecting with an emotionally available and responsive other allows a child to see that naming and showing emotions is acceptable (Mikulincer and Shaver, 2013). The therapist was considered to be someone with the ‘brain space’ as termed by one parent in the study, to support the child with this when parents became overwhelmed. The therapist was also seen as being able to help children manage difficulties through PACE, with the intention for this to become part of the family’s approach for relationship repair and affect regulation (Casswell et al., 2014).
Findings have a range of clinical implications. They support Casswell et al.’s (2014) suggestion that there is a need for different, relational approaches for attachment difficulties, as opposed to traditional, behaviour-focused interventions. DDP should therefore be an accessible option for families who do not respond to more widely available approaches. Parents identified that DDP actively involved them in the process unlike other therapies, which either child or parent had experienced individually, and this was at times challenging for them. Parents could be given advice about the level and impact of active participation before therapy begins and as DDP usually involves initial parent sessions, it may be helpful to ensure this is a standard element of these, using this study to discuss with parents what can be involved emotionally and practically.
There are also implications for future research. This study provides some further evidence to support a large-scale RCT, as recommended by NICE (2015), given parents’ generally positive experiences matching those practising DDP with families in services across the United Kingdom (Turner-Halliday et al., 2014). It also supports the idea that outcome measures may want to focus on both relational and behavioural change. NICE (2015) have recommended including measures of attachment, parental sensitivity (knowledge, understanding and emotion regulation), placement disruption and behavioural problems, all of which are supported by parents’ experiences in this study. Given acceptance was also a significant part of the experience; this may also be an important outcome to be measured. As identified by Boyer et al. (2014), it would be difficult to find an instrument that measures all the elements of DDP and therefore a variety of measures will be needed. Furthermore, there was variation of between 8 and 43 therapy sessions. This does not permit an understanding of how many sessions may be needed for any potential changes to be realised. This will need to be addressed in an RCT of DDP given that some positive changes were reported for most participants.
Although much effort was made in this research to ensure maximum reflexivity, quality and credibility, there are some limitations inherent to a qualitative study of this kind. The sample may have consisted mostly of parents who had ‘good’ experiences of DDP since clinicians may have put forward ‘successful’ therapy cases and by requiring only those who had completed enough sessions to qualify for having had DDP therapy, this may suggest the sample were likely to have had better outcomes. Also we did not collect data for those, if any, who may have declined when approached by their DDP therapist. One parent did not report such positive outcomes however suggesting these potential biases did not mitigate their inclusion. Understanding how treatment content varied was not addressed. Although DDP as a therapy is described in detail in a manual (Hughes, 2011) and there is strict guidance on content of trainings in DDP (DDP Network, 2014) as well as the practicum (DDP Network, 2011); this remains an area which could be addressed in future studies. In addition, the sample was not particularly diverse, including mainly White British, married (or co-habiting) parents between 37 and 61 years, though these are typical of adoptive parents domestically adopting in the United Kingdom (Department of Education, 2016). In this way, it would be useful to conduct the study with other groups such as foster carers who have received DDP therapy but who may differ in their demographics and specific needs to inform methods of measurement and response in any future quantitative DDP study. Other demographics such as social-economic status, level of education, length and stability of relationship and children’s pre-adoption histories were not captured and may have impacted on how parents and children responded to the therapy and should be controlled for in future quantitative research.
In conclusion, in the first direct study of participants who have received DDP therapy, an interpretation of adoptive parent’s experiences of DDP therapy found four superordinate themes encompassing increased understanding of the adoptee’s mind and how to help. There were consistencies in the DDP model with the experience of parents including the importance of acceptance and active participation in the therapy. Parents spoke about DDP as a journey, starting with some uncertainty but once parents experienced evidence of change, they became committed to, what some described as, a difficult journey. Finally, DDP was seen as a shared experience, which was crucial in building trust and co-regulation. The therapists’ stance was also an important part of the experience. There are implications for clinical practice and future quantitative research arising from this qualitative study which generally supports the promise of DDP therapy as effective and worthy of further investigation.
Footnotes
Acknowledgements
We would like to thank all of the parents and clinicians who participated in this research.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Ben Gurney-Smith is Research Co-ordinator for the DDP Institute.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was completed in partial fulfilment of Dr Megan Wingfield’s Doctoratal Thesis at the Oxford Institute of Clinical Psychology Training.