
Abstract
This study investigated how wheelchair-using individuals with paraplegia and chronic pain make sense of the factors associated with quality of life based on interviews using photo-elicitation and interpretative phenomenological analysis. Three superordinate themes emerged in the analysis: experiencing quality of life through the perception of self and identity, interpersonal relationships as facilitators and barriers to quality of life and life in a wheelchair: pain experience and management. Quality of life for those living with paraplegia and chronic pain is experienced as a complex interaction across several life domains. The use of photographs may improve the communication of pain-related experiences and understanding by healthcare staff.
Spinal cord injury (SCI) affects over 40,000 people in the United Kingdom (BMJ Best Practice, 2015) and 276,000 in the United States (National Spinal Cord Injury Statistical Centre, 2015). Depending on the location and nature of SCI, individuals may experience a partial or a complete loss of function and/or sensation to their lower limbs but may retain upper limb and/or trunk function and sensation (‘paraplegia’) or experience paralysis to all four limbs and trunk (‘tetraplegia’) (NHS Choices, 2014). Quantitative research has illustrated that individuals with SCI can experience poor quality of life (QoL) resulting from medication (Celik et al., 2012), psychological factors such as being unwilling to accept disability or a perceived lack of empathy from others (Summers et al., 1991), the impact of SCI-related pain on common daily activities (e.g. maintaining an active social life; Ravenscroft et al., 2000) and the chronic pain itself (Gutierrez et al., 2007; Modirian et al., 2010).
There are a number of limitations to traditional quantitative and function-focussed approaches to the exploration of QoL (Burton et al., 2017; Hammell, 2007). Despite a vast range of measures, many fail to be adequately checked for reliability and validity (Wilson et al., 2011), and many are criticised by those with SCI for failing to adequately capture QoL experiences (Whitehurst et al., 2014). Qualitative research can, however, overcome some of the limitations of quantitative approaches to exploring QoL (Burton et al., 2017). For example, a systematic review of qualitative research highlighted several psychosocial factors associated with QoL for those with SCI, such as the environment (physical, economic, political, legal and social), the renewed importance of relationships and continuity of biography, while the experience of pain was only briefly considered as one of many problems associated with an impaired body (Hammell, 2007). This lack of consideration is surprising given that chronic pain impacts large numbers of individuals with SCI (Gironda et al., 2004; Modirian et al., 2010), with greater intensity linked to worse QoL (Gutierrez et al., 2007), and the potential for a greater impact on QoL than SCI itself (Summers et al., 1991). How pain impacts on QoL requires more in-depth investigation in this population (Burton et al., 2017).
Despite around 69 per cent of individuals with paraplegia reporting chronic upper limb pain due to the use of a wheelchair for mobility (Gironda et al., 2004), there remains a lack of interpretative phenomenological analysis (IPA) research exploring the experience of living with pain in this population. For example, one study conducted focus groups with 24 individuals with SCI and chronic neuropathic pain (CNP) (Henwood and Ellis, 2004). Four themes were identified through constant comparative analysis: the nature of pain, including onset, unpredictability, increasing severity over time and intensification due to physical and emotional factors; methods for coping with pain, including physical and cognitive approaches with varying levels of success; ineffective medications and their associated side effects; and the physical and psychological impact of pain including a desire to maintain functional independence, grief related to losses caused by SCI and frustration with a perceived lack of understanding by healthcare professionals. This study provides some insight into the experience of CNP and SCI specifically, however a broader range of pain types are experienced by this group (Modirian et al., 2010). The use of IPA offers the opportunity to uncover how pain experiences relate to understandings of day-to-day QoL in those with SCI.
Previous qualitative research into SCI and QoL has employed semi-structured interviews or focus groups using researcher-devised schedules (e.g. Boswell, 1997; Dickson et al., 2008; Duggan and Dijkers, 2001; Mann and Chad, 2001), leading to an inevitable power imbalance in the research–researched relationship (Gough, 2003; Yardley, 2000). In addition, standardised self-report measures of QoL have been criticised by those with SCI (Whitehurst et al., 2014) and for focussing on function over other important domains such as personal meaning-making and life context (Blaxter, 1990; Carr and Higginson, 2001). These approaches have illustrated a link between SCI, chronic pain and poorer QoL but restrict the exploration of personally relevant experiences and meaning-making. Approaches that empower participants to lead discussions are needed to ensure in-depth nuanced understandings of QoL. The lived experience of chronic pain has drawn interest in the IPA literature. IPA’s commitment to exploring the lived experience of phenomena is particularly well-suited to this ‘complex, ambiguous and emotionally-laden’ topic (Smith and Osborn, 2015: 41). To date, IPA researchers have explored experiences of individuals living with chronic pain without an identifiable organic cause or associated co-morbidities, illustrating how pain has detrimental impacts on perceptions of ‘self’ and ‘identity’ (Hellstrom, 2001; Osborn and Smith, 1998, 2006; Smith and Osborn, 2007).
Some alternative data collection approaches incorporate creative methods. For example, due to the challenges describing the concept of pain, drawings have been employed to explore pain experience in IPA research (Kirkham et al., 2015). Drawings can facilitate the expression of experience and provide deeper explanations of the sensory, psychological and social impacts of chronic pain (Kirkham et al., 2015). Another avenue for prompting lived experience discussions is photo-elicitation (Collier, 1957; Harper, 2002), also employable alongside IPA (e.g. Rodham et al., 2012). The taking of photographs is less-dependent on artistic creativity than hand-drawn images while still allowing participants to describe experiences and articulate their personal meanings and sense-making (Burton et al., 2017).
This study aimed to use photo-elicitation and IPA to explore the lived experience of people with chronic pain and paraplegia to identify issues which influence their QoL. This approach can uncover the domains of QoL that have the most personal relevance for those living with paraplegia and chronic pain and how these domains function to facilitate or reduce QoL. Furthermore, an idiographic approach enables exploration of experiential features central to QoL that may be overlooked by traditional quantitative QoL measures.
Method
Design
A qualitative interview study was conducted to ensure a participant-led understanding of the QoL experience when living with paraplegia and chronic pain. Photo-elicitation (Collier, 1957; Harper, 2002) was employed to enable participants to take control of the research agenda. This meant that the participants were able to direct the discussions towards those elements of their experiences which they felt contributed to and were part of their QoL as represented by photographs and encouraged the discussion of detailed contextualised stories regarding their daily experiences (Radley and Taylor, 2003), which were analysed using IPA (Smith et al., 2009).
Recruitment and participants
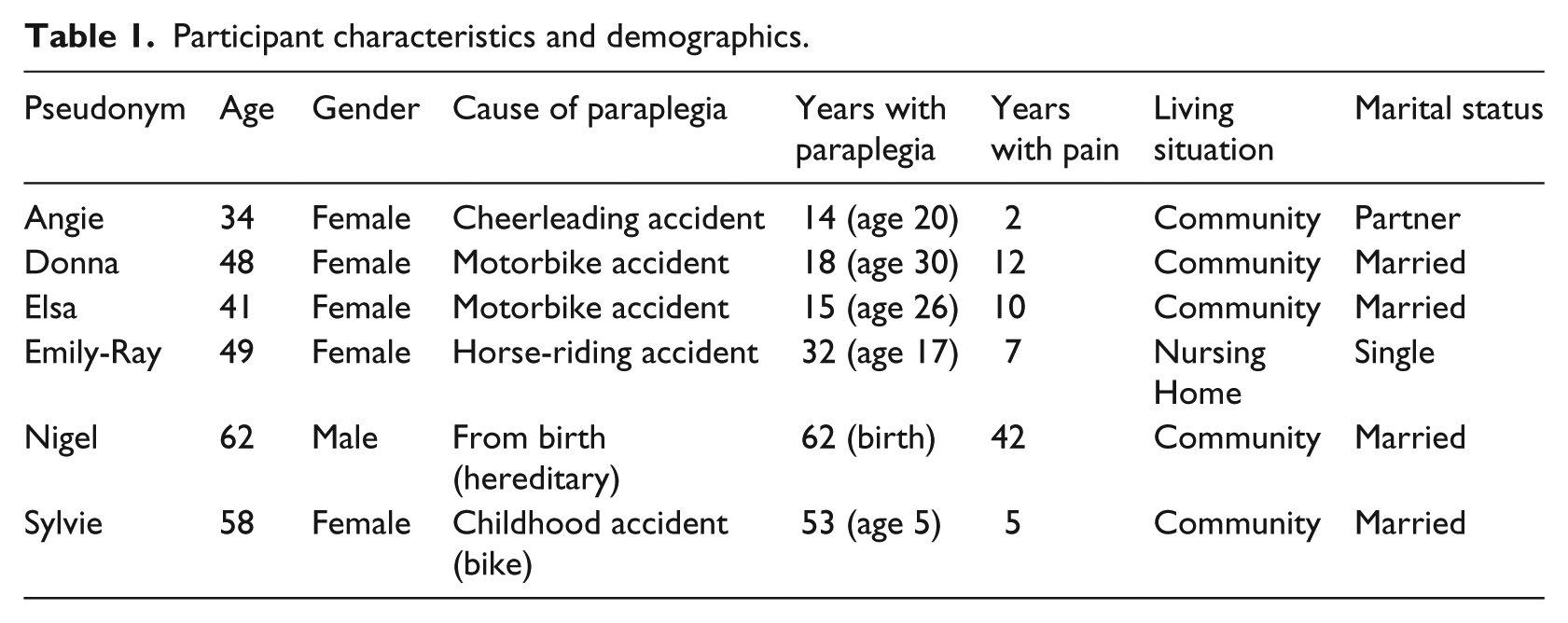
Institutional ethical approval was granted prior to recruitment by the Department of Psychology, Staffordshire University Research Ethics Committee. Inclusion criteria required participants to be English speaking adults, aged >18 years, living with paraplegia, using a wheelchair for mobility and self-reporting chronic pain. Advertisements were placed on online forums and distributed via an email list. The first six volunteers meeting the inclusion criteria (one male, five females; age 32–64 years, mean 49.5, standard deviation (SD) 10.61) were recruited in line with sample size recommendations for IPA (Smith et al., 2009). Written informed consent was obtained and participants provided descriptive data relating to age, sex, length of time living with paraplegia, chronic pain duration and marital status (see Table 1 for demographic information).
Participant characteristics and demographics.
Data collection
Participants spent 7 days taking photographs of things that gave their life quality or reduced their QoL. No further definition of QoL was provided to ensure the discussion was participant-led. Participants chose six or seven photographs that best represented their QoL experiences. This number was chosen as it enabled participants to represent a ‘typical week’ and ensured detailed discussion of each image could take place during the interview. This was guided by recommendations for the use of 6–10 open questions in interviews lasting between 45 and 90 minutes for IPA research (Smith et al., 2009).
Due to geographical variability telephone interviews were required. Despite limitations of this approach in terms of rapport-building (Kvale and Brinkmann, 2009), this method produces sufficiently detailed data for IPA analysis (e.g. Cox and Faithfull, 2015). Interviews began by exploring the background to the participant’s paraplegia (e.g. ‘please tell me a little about your disability’), then generic prompt questions were used to discuss each photograph in turn (e.g. ‘If we start with the first photograph, can you tell me why you chose this picture’, ‘What does it represent in terms of your quality of life?’). Interviews were audio-recorded, and anonymised verbatim transcripts were produced. Participants chose their own pseudonyms.
Analysis
We followed Smith et al.’s (2009) guidance for conducting IPA. IPA involves a ‘double hermeneutic’ in which the researcher aims to make sense of the participants’ making sense of their world and so employs an interpretative epistemology to uncover detailed understandings of ‘lived experience’ grounded in participant accounts rather than exploring a priori scientific constructs (Smith et al., 2009). As QoL is a challenging concept to define (e.g. Blaxter, 1990; Carr and Higginson, 2001), participants’ narratives were employed to guide and develop an understanding of the concepts central to QoL for this group without being limited by pre-existing models or constructs (Burton et al., 2017).
The analysis began by attending to each individual case; line-by-line annotations were made identifying descriptive, linguistic and conceptual features to develop an in-depth understanding of the individual accounts (Smith et al., 2009). Emergent themes representing issues central to QoL were identified by the second author (A.E.B.) and cross-checked and agreed by the third author (R.C.D.). Themes were tabulated and sorted according to the image that prompted each discussion. While not necessarily standard practice for IPA, our use of multiple analysts enforced the need to justify our interpretations of the participants’ experiences of QoL through regular discussions between the authors with repeated reference back to the transcripts, which ensured that our interpretations were grounded in the data. Cross-case comparisons of theme clusters by all authors were used to develop a narrative of superordinate themes capturing the lived experience of issues relating to QoL. Underneath these superordinate themes were a range of life domains associated with QoL.
Results
The participants highlighted a range of life domains central to achieving and maintaining QoL (Supplementary Tables 2 and 3 detail the photographs selected by participants and the QoL domains linked to these images). Each image prompted a range of positive and/or negative reflections on QoL domains, representing the spectrum of QoL experiences as discussed by the participants. None of the domains were mutually exclusive; all images prompted discussion of multiple domains illustrating the complex and intertwined lived experience of QoL. How QoL domains functioned to make up the overall experience was captured within three superordinate themes: (1) experiencing QoL through the perception of self and identity, (2) interpersonal relationships as facilitators and barriers to QoL and (3) life in a wheelchair: pain experience and management.
Experiencing QoL through the perception of self and identity
Discussions of factors promoting or reducing QoL were frequently related to concepts of self and identity, including the reflection on past, present and future selves. For example, Donna chose a photograph of her husband’s gift of a wall-mounted ‘I’m with Stupid’ mural, which highlighted how negative self-perceptions could be detrimental to a sense of QoL. Donna presented unease, wrestling with the possibility that the mural represented her husband’s actual thoughts about her (‘it is something [my husband] bought for me but I think he’s referring to me […] I can relate to it though’). Donna’s ability to relate to the image highlighted incidents of self-depreciation: I laughed [when taking this photograph] because I just see myself a dimwit, but at the same time I felt sad cause it’s sad when you feel that way about yourself and you think others see you that way too. It just sums up how I feel I am seen by people ‘cos no one cares anymore… no one comes near, it’s a lonely sad place…. I guess it’s just how I feel about myself being in the chair and not as I used to be. (Donna)
For Donna, being unable to equate her current identity with positive self-perceptions had important implications for QoL, fuelling negative emotions and a sense that others were choosing not to get close to her. While aware that these were her own perceptions and not necessarily the thoughts of others, Donna was unable to overcome the possibility that others also perceived her in this way and this became her only accessible explanation for the loneliness she was experiencing. This example illustrates the interrelated nature of the QoL experience with Donna discussing perceptions of self, interpersonal relationships and her wheelchair, all discussed further in later themes.
Reminiscence was also often incompatible with holding a perception of a current self with good QoL: It’s frustrating because I remember living without this pain and life was sweet you know. I was a different girl. I was not miserable. […] now a new girl has arrived in town and I have to deal with her. It’s hard. (Angie)
Despite reporting having paraplegia for 14 years and chronic pain for only two, Angie equated the onset of disability with the beginning of her pain experience. This illustrates how paraplegia, pain, self-perception and identity became interwoven constructs within the QoL narratives. There was a reluctance among participants to identify with their new disabled-selves, who were presented as external ‘others’ (e.g. ‘I’ vs ’her’). Participants’ memories of themselves prior to paraplegia typically prompted frustration with the current self who was viewed as inferior and was associated with a sense of poorer QoL.
Perhaps unsurprisingly, some of the participants valued opportunities to become a ‘different’ self to improve their QoL. For example, Sylvie chose a picture of the view from inside a car, which represented her independence and improved mobility which gave her access to relationships, positive emotions and pain management. Each of these QoL elements were bound up in Sylvie’s perception of her changed identity: I am lost in the wheelchair, even though it’s been my legs for 53 years, there’s no greater importance than feeling you don’t need that chair. Yeah, I might only get out of it to sit in the car, but the car takes me places my chair can’t. I am considered a fire hazard when I’m in my chair, I’m not in my car. I am me in the car, not a woman in a wheelchair, and the freedom takes away my feelings of pain. If only for a short while. (Sylvie)
The car enabled Sylvie to feel comfortable in herself and regain an identity (‘me’) she equated to a feeling of equalness. This account weaves together experiences of physical and psychological freedom; physically, journeys in the car meant a break from the wheelchair, while psychologically the car removed the visible indicator of Sylvie’s disability, something which was highly valued especially as the wheelchair represented a loss of Sylvie’s preferred identity. Other participants also valued opportunities to escape and experience freedom: This [photograph of nature] reminds me of freedom from pain and disability. Sometimes I can take myself spiritually out of the chair and pretend I am free […] ‘cos I can’t get out much to enjoy it, I have to think of the times I could. (Nigel)
Memories of being free from pain were also considered as a means of escape from pain and the current disabled self, at least mentally if not physically, and a way of becoming more resilient and maintaining QoL. Due to experiencing paraplegia from birth, unlike the other participants, Nigel’s self-comparisons related to when he developed additional illnesses and chronic pain that restricted his freedom. The biggest issue for Nigel was the impact of these changes in his identity on his relationships, which is discussed further in the next theme.
Interpersonal relationships as facilitators and barriers to QoL
The participants’ sense of self and identity were shaped and reshaped through their relationships, which had both positive and negative implications for their QoL. For some, a sense of a forced dependence on others led to feelings of guilt, anger, frustration and poorer QoL. For example, Nigel had paraplegia from birth but in recent years developed several health issues, including a stroke, minor heart attack, rheumatoid arthritis, chronic obstructive pulmonary disease and mental health difficulties, which further worsened his pain and negatively affected the relationship with his wife. In response to photographs of his medication and his wife’s bedroom he explained, Because of the medication I am on I can’t be left alone now. My wife can never leave me. That’s so pissing frustrating you know, I’m like a child … being baby sat. […] At night is when my pain is worst so I’m downstairs screaming up to my wife for help, so she is being disturbed […] seeing my way of life now to what it was is sad isn’t it? I don’t get to be who I want to be. I have changed my wife’s life and most days I sit feeling sorry for myself without thinking of her. (Nigel)
Nigel viewed the changed relationship with his wife as one of a carer-care recipient, which he likened to childcare, rather than one of equal partnership. Nigel’s additional health complications, which led to an inability to use a stair lift resulting in him sleeping alone downstairs, further compounded this changed identity and relationship. Nigel had a complex and conflicted emotional response to these changes; his concern for his wife but also guilt at the perception that he was a burden and that he was placing his own priorities and challenges first. This account illustrates how perceptions of changes in identity influence emotional responses to changed relationships, which in turn serve to reduce perceptions of QoL.
Those participants who struggled to find their own value in relationships, and felt like a burden to others, experienced stronger feelings of guilt for being dependent. Others could counterbalance feelings of being a burden against the benefits of engaging in meaningful relationships for their QoL. When discussing an image of a locket containing photographs of her parents Elsa explained, When I was injured and through everything that happened to me my mum has been there no matter what. I lost my dad to cancer and I know with my disability as well it’s been tough on her but I couldn’t live without her […] I feel guilty that I lean on [my Mum] […] but we help each other and it helps her too I reckon she doesn’t say it but she never complains about looking after me so I think she enjoys it. […] Family give me quality of life cos they are there for me, okay they can’t heal my pain, but they certainly take my mind off it and make me feel like I’m worthwhile which is amazing for me cos when I’m alone that’s when I think a lot but my mum and husband help me through the dark thoughts. (Elsa)
For some participants, acceptance of social support and spending time with family gave life purpose and meaning, provided a distraction from pain and ‘dark thoughts’, and enhanced their QoL. Elsa also portrayed reciprocity in her relationship with her Mum describing value in the support she could offer while adjusting to a shared bereavement, a stark comparison to Nigel’s inability to see his personal value in his altered relationship with his wife. Unlike Nigel, Elsa could find a valuable role within her relationships providing a sense of autonomy and independence that was beneficial for her QoL.
For others, a solution to the problem that family could not fully understand their experiences was to seek relationships in other ways. Angie and Nigel both achieved this through companion animals who could provide an escape from negative perceptions of post-disability identities and enhance their QoL. Angie explained, [My dog] makes my life better, she’s not judgmental at all, and she takes me for who I am which is great for me. […] When I am cuddled up with my dog on the bed, I am not the person in the chair who has to fight to pick things up or even go the toilet, she makes me feel how I used to be. She is just a tonic I want forever. (Angie)
Adult human relationships were often perceived as tainted by perceptions of difference or underlying stigma (‘people stare because I’m not walking like them’, Donna). In contrast, relationships with children (‘I don’t look normal do I so to have [my great nephew] accept me is a dream. I just wish the rest of society could do that’, Emily-Ray) and animals (‘[my dog] sees I need someone there, I talk to him, tell him how I’m feeling, we watch tele’ and I tell him what I think is crap on TV, he listens ya know?’ Nigel) were viewed being as non-judgemental of the participants’ new identity and untainted by the participants’ former selves, and so could facilitate a sense of satisfaction, acceptance and QoL.
None of the participants discussed in-person relationships with others with paraplegia, but some highlighted the value of support and companionship afforded by online relationships. These were a significant source of understanding and a means to relieve frustration: I can talk to so many people [using my laptop] who are like me… people who understand and will listen to me without prejudice. (Emily-Ray) Being lonely in a disability is the worst feeling in the world, so to have others, who you can share things with, that know where you’re coming from, is a great benefit to me and my family, cause then I’m not moaning to them all the time cos I do feel that’s all I do. […] there are people out there [on the internet], and like I said when we have been to see a doctor and feel we haven’t been listened to, then having others to tell is relief cos again you’re not alone in that. (Elsa)
Companionship and understanding provided by online relationships helped participants make sense of their own experiences, share coping strategies and provided an avenue for airing feelings and frustrations without the guilt associated with burdening family. Computer-mediated interactions were also beneficial when pain prevented participants from leaving the home by giving them the opportunity to engage in meaningful social interactions, which was beneficial for maintaining a positive sense of QoL.
Life in a wheelchair: pain experience and management
Some perceived QoL facilitators and barriers related to physical environments and mobility, and were discussed in relation to both physical and psychological pain. These were typically interpreted in terms of how wheelchairs and medical interventions could enhance or restrict QoL by both causing and relieving pain. Several participants selected a photograph of their wheelchair for discussion, illustrating its important role in their QoL. Some saw their wheelchair as an aid to better QoL and pain management: It’s my saviour. I would be housebound if I didn’t have my chair. It’s my best friend and when I’m busy in it like going out if I can it’s a kind of pain blocker. Okay, I don’t choose to be in it but it’s the way it is […] I am free in my chair but pain does have a say in it though. (Elsa)
For Elsa, the wheelchair was essential for QoL as it enabled independence and mobility that distracted her from pain. Despite acknowledging that a wheelchair is not her ideal solution, Elsa’s personification of her relationship with the chair helped her to resolve her experience of pain and emphasise its benefits for her QoL. However, it was evident that this relationship was complex, with pain still ‘having a say’, and this contradiction of both contributing to and reducing QoL could be challenging to resolve. For example, Emily-Ray conceptualised her wheelchair as a force that repelled others, causing her further pain: I got on the horse that day as me, free, able to walk, use the toilet, very independent, to a cripple mess that I am today. I am not taken seriously in life anymore, people stare, people are cruel… well those who don’t know me. They see my chair and it’s like a force is drawing them away from me as if they are going to catch my disability. With that I get psychological pain which then makes my physical pain worse. (Emily-Ray)
Again, identity plays an important role in understanding conceptualisations of QoL. Emily-Ray compared her current self with memories of her former pre-accident self, with the current self viewed as being less worthy and unable to function. Perceptions of how others reacted to Emily-Ray’s disability, which were interpreted through her dependence on a wheelchair, reinforced the discrepancy between her current identity and her past self. An inability to resolve and cope with this change in biography created barriers to relationships and increased psychological pain which in turn worsened physical pain symptoms and negatively impacted on QoL.
Other complaints regarding wheelchairs included problems navigating home environments, sleeping in separate rooms from partners and difficulties with basic personal care. These were all a source of frustration, pain and sometimes embarrassment, as Emily-Ray explained when talking about a photograph of her bathroom door: It’s a room within my apartment that I can’t use and I should be able to. I feel the pain when I have to go down the hall to use a bathroom, especially when I have to wait in a queue. When you’re keeled over with shoulder and back pain that’s the last thing you need. […] having a room that is there but you can’t use is frustrating, painstaking and, well, wrong. (Emily-Ray)
Emily-Ray’s room in the nursing home contained a bathroom, however it was not suitably modified for her wheelchair and instead she had to rely on shared facilities. As maintaining hygiene standards was important for Emily-Ray’s personal sense of QoL, this experience became a source of embarrassment and a contributor to her physical and emotional pain. The wheelchair in these instances was viewed a barrier to a good QoL by denying independence, especially the ability to take basic care of oneself, when in reality it should provide freedom and autonomy, an experience which became frustrating for many participants. The participants saw the use of wheelchairs as contributing to the experience of their pain as much as its management, which was another challenge for maintaining a sense of positive QoL.
Similar to the wheelchair, medications and healthcare professionals (HCPs) were viewed as a potential source of pain relief but also a source of further pain and frustration, especially the experience of medications failing to alleviate pain and feeling misunderstood by HCPs. For example, Nigel felt that it was impossible for the nurses who supported him in his home to understand his experience of pain: Look, I know [the nurses] mean well, some days I am miserable cos I am in so much pain … so they deserve medals really … I don’t think they, well, how can they know my pain and how bad it is? (Nigel)
There was a general sense that as HCPs did not fully understand the nature of the participants’ pain this lead to the prescription of numerous and inadequate medications, often accompanied with unwelcome side effects, contributing to a mistrust of HCPs. Challenges in communicating pain to HCPs, and finding the appropriate medication to manage pain, negatively influenced the participants’ perceived QoL: Doctors don’t listen. They have no idea what to say to me really. They try, bless them, but how can they know the pain? Although, it would be nice if they could actually try to listen instead of throwing meds at me […] I am on way too much medication, but they say it’s better I have the amount. I am not so sure, I am doped up most days on morphine which leaves me unable to function but it helps my pain, so for that I am thankful I suppose. (Donna)
Despite the perceived lack of understanding and pessimism about HCPs’ abilities to ever understand the nature of the participants’ pain, there was still some gratitude for medical support. Many participants had pessimistic views about medical interventions and medical advice as they had an experiential understanding of their own pain which HCPs did not fully comprehend or consider in their interventions. This combination of feeling misunderstood, poor communication with HCPs and negative experiences with medication had a cumulative effect in reducing the participants’ sense of QoL especially as all these factors, in addition to the wheelchair, should have significantly reduced their pain and improved their QoL.
Discussion
This study used a photo-elicitation approach to guide participant-led discussions exploring how individuals with paraplegia and chronic pain made sense of their QoL. Life in this context can be challenging for maintaining QoL and participants highlighted interacting constructs across eight life domains: pain, independence, mobility, relationships, hygiene, home environment, emotion and identity. These domains were never mutually exclusive and interacted within everyday experiences with participants drawing on issues relating to identity, interpersonal relationships and life in a wheelchair to make sense of their QoL. The domains and issues discussed by participants resembled those featured in traditional measures of QoL, including physical and psychological health, level of independence, social relations, environment and personal beliefs (WHOQOL Group, 1998), and those highlighted in previous qualitative research (Hammell, 2007). However, the participants’ accounts also illustrated how changes in self and identity played a central role in explaining how these domains either enhanced or reduced their QoL, something that has been explored in detail in IPA work with individuals with chronic pain (Osborn and Smith, 1998).
Our participants discussed struggles to form a coherent identity and provided clear examples of ‘biographical disruption’ (Bury, 1982), seeking to find meaning in their past and their future and come to terms with becoming disabled and experiencing chronic pain. Some experiences were similar to those reported in other chronic pain research which included examples of social comparison (Osborn and Smith, 1998). However, rather than downward-comparison reported by general chronic pain samples to improve self-perception (Osborn and Smith, 1998), our participants used upward self-comparison considering their current self as inferior to their pre-disability selves. These upward self-comparisons could damage QoL by restricting possibilities for the successful resolution of ‘biographical disruption’. Despite the proposition that individuals are able to adapt to biographical disruption over time (Bury, 1982), some participants remained unable to accept their new identity many years after the disruption occurred, with additional changes (e.g. sleeping downstairs) creating new disruptions. There is a clear need for ongoing rehabilitation strategies that assist individuals with chronic pain and paraplegia to interpret and repair this disruption.
One of the challenges of identity acceptance was a complicated relationship with wheelchairs. Wheelchairs were accepted as an aid for improving QoL by providing independence but were also a frustrating source of public stigma and pain. The struggle to resolve this ambivalence and confusion may result from differences in implicit and explicit cognitions. For example, Galli et al. (2015) found that individuals with SCI explicitly prefer other wheelchair users but implicitly prefer outgroup members without disability. The requirement placed upon wheelchair users to rearrange their identity from ‘able-bodied’ to ‘wheelchair user’ is at odds with the automatic reactions engrained in the cultural and educational dimensions of the able-bodied self (Galli et al., 2015). Our participants rarely discussed relationships with other wheelchair users, highlighting that opportunities to form a positive perception of their new in-group and new identity were lacking.
Social support has been associated with higher life satisfaction after SCI (Van Leeuwen et al., 2010), better health outcomes and improved functioning (Müller et al., 2012). Some of our participants discussed the benefit of online relationships which held promise for enhancing QoL and may hold particular value for those with paraplegia and chronic pain who have limited mobility (Mattar et al., 2015). Creating opportunities to engage and share experiences with others should be considered a priority within rehabilitation work as it has potential to promote QoL through an opportunity to be understood and facilitate positive perceptions of those with disability, which could contribute to the resolution of biographical disruption.
Participants frequently equated physical challenges when using their wheelchair with experiences of physical and psychological pain, helping to explain why pain has been shown to have a greater impact on QoL than SCI itself (Summers et al., 1991). Like Henwood and Ellis (2004), our participants highlighted that one of the barriers to pain management, emotional wellbeing and QoL was a perceived lack of understanding of pain by HCPs. One avenue to improving communication is the use of photographs or other creative outlets like drawings, to better allow users to discuss their pain experiences (Kirkham et al., 2015; Padfield et al., 2015). Improving communication has the potential to reduce the need for unnecessary medication and help those with SCI find beneficial pain coping strategies.
A strength of this work is the use of photo elicitation which has enabled an exploration of the factors that contribute to QoL for our participants, how these factors are understood in relation to day-to-day experiences and reduce or facilitate QoL. However, it is possible that our participants represent individuals who, in their willingness to discuss their own experiences, may be better functioning and have qualitatively different and less severe experiences of pain in comparison to others in this population. The use of audio telephone interviews in this study should be considered as a limitation and may have hindered the exploration of the content of the photographs, although both the researcher and participant had the photographs to hand during the discussions. Future research may consider using video conferencing technologies to facilitate rapport-building when conducting photo elicitation interviews.
Conclusion
This qualitative photo elicitation study has confirmed the existence of common QoL domains and has illustrated how these issues interact for a sample of individuals living with paraplegia and chronic pain. Our work highlights the importance of perceptions of identity and the role of supportive interpersonal relationships in aiding perceptions of good QoL. Rehabilitation interventions which help individuals to adjust to living with paraplegia and chronic pain are needed to improve QoL. Our work has illustrated how the introduction of creative visual representations of individuals’ pain experiences can uncover personally relevant elements of QoL. Photo elicitation could be used to improve the quality of healthcare communication to facilitate greater trust and reduce stress caused by complex pain management regimes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.