
Abstract
To understand the role of symptom attribution in treatment-seeking behaviours, survey results of 1356 veterans (age = 38–72 years) were analysed. Controlling for symptom frequency, significant relationships were found for specialist and psychological-related consultations. Those who favoured psychological explanations for symptoms were more likely to attend specialist and psychology-related consultations and filled significantly more prescriptions than people who predominantly explained symptoms by situational factors (normalisers). Veterans who favoured somatic explanations attended more general practitioner consultations than normalisers. Attributional style should be considered part of the constellation of factors influencing healthcare usage. Normalisers, the predominant group, used fewest health services and filled fewest prescriptions; this may have important implications for healthcare considering their tendency to minimise or downplay symptoms.
Introduction
Experiencing health symptoms that could potentially be treated is very common (Burton, 2003), but the vast majority of symptoms are dismissed by sufferers as unnecessary of seeking medical care (Zola, 1973). Symptoms may be physical or psychological, but many symptoms are ambiguous in nature and subject to interpretation. There are a range of factors that influence a person’s decision to seek treatment for a particular symptom including psychosocial factors such as stress or interference with social activities (Cameron et al., 1995; Rosenstock, 1966; Zola, 1973), economic factors such as health insurance (Cameron et al., 1995; Dutton, 1986), demographic factors such as gender, socioeconomic status or geographical location (Cameron et al., 1995; Wang et al., 2005) and symptom characteristics such as rapidity of onset, perceived severity or perceived relevance (Cameron et al., 1995). But what about the perceived cause of the symptom?
While doctors use medical models of illnesses, patients have their own lay conceptions and health beliefs of both diseases and individual symptoms (Burton, 2003). These conceptions can influence health behaviours such as treatment seeking and even referral patterns of primary care doctors, which reflect the challenge of clinical management. How patients understand and interpret their symptoms has important implications for the type of healthcare and treatment decisions they make, that is, if they pursue treatment at all.
It has been proposed that attributional styles influence a range of behaviours and attitudes towards treatment such as self-care, propensity and delays to seek treatment, compliance, success in coping with illness, patterns of self-care and clinical presentation (Robbins, 1991; Wright et al., 2015). Attributional style refers to a pattern in how individuals view the likely cause of their symptoms. There are three different attributional styles: normalising (generally the most prevalent style, involving downplaying symptoms or attributing them to an environmental cause), psychologising (attributing symptoms to psychological distress or stress) and somatising (attributing symptoms to an organic or physical cause) (Robbins, 1991). Attributional style has been associated with changed symptom experiences; for example, psychologisers have reported more severe depressive symptoms (Parker and Parker, 2003), while chronic physical illnesses have been associated with somatisers (Robbins, 1991). Attributional style has been described as ‘moderately stable’, for while it has been characterised as an enduring tendency in individuals, there is evidence that it is also associated with past experience (Robbins, 1991).
Previous research investigated the relationship between symptom reporting and attributional styles in Australian veterans finding that psychologisers and somatisers demonstrated higher symptom reporting than normalisers (Wright et al., 2015). New symptoms and symptoms that persisted over time were also associated with changed attributional styles (Wright et al., 2015). This article extends this research by examining the relationship between attributional styles and treatment-seeking behaviours and referrals to gain a deeper understanding of how individuals interact with the healthcare system. Veterans are a population with increased healthcare needs (Agha et al., 2000; Ikin et al., 2004; Kelsall et al., 2004a, 2004b). Gaining more insight into why and how veterans do, or do not, seek treatment is of paramount importance to informing appropriate healthcare is available for veterans. While financial (Drapalski et al., 2008), social (e.g. public and personal stigma relating to mental health) (Stecker et al., 2013; Vogt, 2011), geographical (e.g. distance) (Buzza et al., 2011; Stecker et al., 2013) and socio-demographics (Lahiri and Xing, 2004; Nelson et al., 2007) have been investigated for how they influence veterans’ healthcare, the role of symptom interpretation is yet to be investigated. This is a particularly crucial investigation for veterans who experience ongoing, and often ambiguous, symptoms; for example, Gulf War veterans have been plagued for over two decades by chronic medically unexplained symptoms (Iversen et al., 2007) and multisymptom illness (Gwini et al., 2016; Kelsall et al., 2009). Symptoms, regardless of diagnostic status, are a major factor in health interpretation and health decisions (Khan et al., 2003). Thus, understanding this facet of veteran decision-making can help inform how best to provide adequate healthcare for veterans.
Previous research investigating attributional styles has found that a normalising style has been associated with less frequent general practitioner (GP) visits than other attributional styles (Sensky et al., 1996) and a somatising style with an increased likelihood to consult a GP or referral to a psychiatrist (Parker and Parker, 2003). In a population of fibromyalgia patients, those who did not seek treatment used the normalising style significantly more than those who did seek treatment (Gulec, 2008). Additionally, individuals report they would be less inclined to visit a doctor for what they interpret as symptoms with a psychological cause than those with a physical cause (Bishop, 1987). Beyond patients’ choices, symptom attribution has also been found to predict GP’s ability to identify depression and anxiety in normalisers (Kessler et al., 1999). Normalisers tend not to emphasise or complain about their symptoms, and it is therefore considered possible that screening instruments may not pick up their levels of distress (Parker and Parker, 2003). If patients are clear and insistent regarding explanations for symptoms, this can influence both the type of treatment they seek and their doctor’s interpretation and treatment options, including referrals, offered (McFarlane et al., 2008).
There continue to be evolving healthcare needs for contemporary veterans (Hoge et al., 2006; Seal, 2009). Multiple epidemiological studies have found that Gulf War veterans suffer from a range of medically unexplained symptoms (Kang et al., 2009, 2000; Kelsall et al., 2009; McKenzie et al., 2004; Schwartz et al., 1997; Unwin et al., 1999). Healthcare usage and barriers to care in military and veteran populations have received considerable interest in recent years. Predictors of healthcare utilisation in military or veteran populations include physical health functioning (Aspinall et al., 2009; Elhai et al., 2008), mental health functioning (Aspinall et al., 2009; Gray and Kang, 2006), insurance status (Aspinall et al., 2009) and mental health stigma (Hoge et al., 2006; Owens et al., 2009; Vogt, 2011). It is beneficial to understand how and when veterans seek treatment for their symptoms, both physical and psychological, to ensure that adequate and satisfactory care is available. An important aspect of this is to understand why some veterans seek medical care for symptoms, while others do not. However, to our knowledge, the role of attributional styles in veterans’ healthcare usage has not been investigated.
The literature regarding symptom attribution in health has largely focused on its influence on doctor’s ability to correctly identify distress and their interpretation of symptoms (Greer et al., 2004; Kessler et al., 1999), which in turn impacts on the specialist referrals made by the GP. Only a few articles have focused on the role of symptom attribution in an individual’s treatment-seeking behaviours (Gulec, 2008; Rief et al., 2004). Rief et al. (2004) explored attributions in patients with unexplained physical symptoms and found that after controlling for health conditions, organic (somatic) attributions were associated with a need for medical diagnostic examinations to verify diagnoses. Gulec’s (2008) study of fibromyalgia patients and healthy controls found that normalisers were less likely to be engaged in help-seeking behaviours. Another study of Australian men from the general community found that normalising styles predicted fewer medical and cancer checks (Brown and Bond, 2008). To our knowledge, none have examined this in a military or veteran population, which have different healthcare requirements and options (Hoerster et al., 2012).
Our previous research findings revealed a similar distribution of attributional style in Gulf War veterans and a military-era comparison group (Wright et al., 2015); thus, the two groups will be considered together for the present analysis. This article aims to better understand healthcare usage by examining the role of symptom attribution through the following research questions:
Are attributional styles and symptom reporting associated with the likelihood that veterans have sought treatment, and if so which types of treatment?
Are attributional styles and symptom reporting associated with the likelihood that veterans have had prescriptions filled?
Methods
Participants
The baseline Australian Gulf War Veterans’ Health Study, conducted in 2000–2002, recruited 1456 Gulf War veterans (1990–1991) (80.5% of eligible cohort) and 1588 (56.8%) of an military-era comparison group, who were largely composed of Naval personnel (Ikin et al., 2004). The same cohort of participants were followed-up in 2011–2012. Participation at follow-up involved two main components: a self-report questionnaire and consent to data linkage with Australian Medicare Benefits Schedule (MBS) data, Department of Veterans Affairs (DVA) health services data and the Pharmaceutical Benefits Scheme (PBS) and the Repatriation Pharmaceutical Benefits Scheme (RPBS) data.
After baseline, participants who had refused involvement in further research were identified as deceased or who had no valid mailing address located were removed, the recruitment denominators were 1330 for the Gulf War veterans and 1449 for the comparison group. Of those, 715 (54%) Gulf War veterans and 675 (47%) comparison group members participated. The self-report questionnaire was completed by 712 Gulf War veterans and 674 comparison group members. The analyses conducted in this article were restricted to males due to very low female numbers: 697 Gulf War and 659 comparison group members, a total of 1356. The majority of male participants (n = 1159, 85.5%) consented to DVA and/or MBS data linkage. Of those who consented to linkage, 956 were linked to MBS, 614 were linked to DVA and 720 were linked to PBS/RPBS.
Although participants from comparison group were matched on demographics with the Gulf War veterans at baseline, due to differential participation rates at follow-up, there were slight differences between the two groups. Gulf War veterans at follow-up tended to be slightly younger and more likely to have been in the Navy (Ikin et al., 2016).
Participants were between 38 and 72 years old, with a mean age of 50.1 years (standard deviation (SD) = 6.45), the majority were or had been in the Navy (77.3%), with 14.0 per cent Air Force and 8.7 per cent Army. Post the 1990–1991 Gulf War, 67.8 per cent of all veterans had deployed between 1991 and 2012 and 17.5 per cent were still serving in the Australian Defence Force (ADF) in 2012. Previous analysis found no difference between Gulf War veterans and the comparison group in predominant attribution style; normalising was the predominant style in both groups (Wright et al., 2015). It has also been previously reported that attributional style did not differ by active service status (Wright et al., 2015). Further analyses revealed no differences in predominant attribution style for age or service type (e.g. Navy, Air Force or Army).
Measures
The Symptom Interpretation Questionnaire (SIQ) was used to assess common attributional styles for causes of somatic symptoms: normalising, psychologising and somatising (Robbins, 1991). The SIQ consists of 13 common bodily symptoms and attached to each symptom are three possible explanations, each one corresponding to one of the three styles of attribution. Participants chose one explanation per symptom, giving each participant a possible score of 0–13 along each of the three attributional dimensions. Participants were classified as predominantly normalisers, psychologisers or somatisers if they scored seven or more on that scale; those who did not score at least seven for any style were categorised as no predominance (Kessler et al., 1999). As no predominance indicates a predominant combination of psychologising and somatising answers with some normalising attributions, this will be interpreted as a mixed attribution style. As normalisers have been identified as the predominant group (Wright et al., 2015), they will serve as the reference group in the analyses.
A 63-item symptom questionnaire, administered at follow-up, was used to assess the presence of symptoms in the past month, which were rated on a 4-point Likert scale from ‘Not at all’ to ‘Severe’. The questionnaire was adapted from that used by the King’s College Gulf War Illness Research Unit and included respiratory, cardiovascular, musculoskeletal, dermatological, gastrointestinal, genitourinary, neurological, neuropsychological or cognitive and psychological symptoms (Kelsall et al., 2004b). Previous work revealed a three-factor solution to grouping the 63 symptoms. The types of symptoms covered by the list included psychophysiological (e.g. nausea, difficulty speaking), cognitive (e.g. loss of concentration, avoiding things/situations) and neuromuscular (stiffness in several joints, loss sensation hands/feet) symptoms (Forbes et al., 2004). A count of the symptoms rated as moderate or severe was tallied.
Healthcare usage was defined in two ways: first, based on self-reported consultations with health professionals and second, drawing on data derived from record linkage on consultations with GPs and specialists and pharmaceutical prescriptions filled. Within the questionnaire completed at follow-up, participants were asked whether they had consulted a health professional (excluding time spent in hospital) for their own health in the previous 12 months. The list of 14 professions can be seen in Table 1, with the exceptions of hospital outpatient, emergency ward and day clinic attendance, which were excluded as they potentially relate to a different set of behaviours and health issues. For example, visits to the emergency ward are often driven by external factors and do not necessarily involve a choice to seek treatment. Additional data would be required to more fully investigate these types of healthcare usage, such as reasons for visits, but these data were not available in this study.
Attributional style and self-reported health professional consultations in the past 12 months.
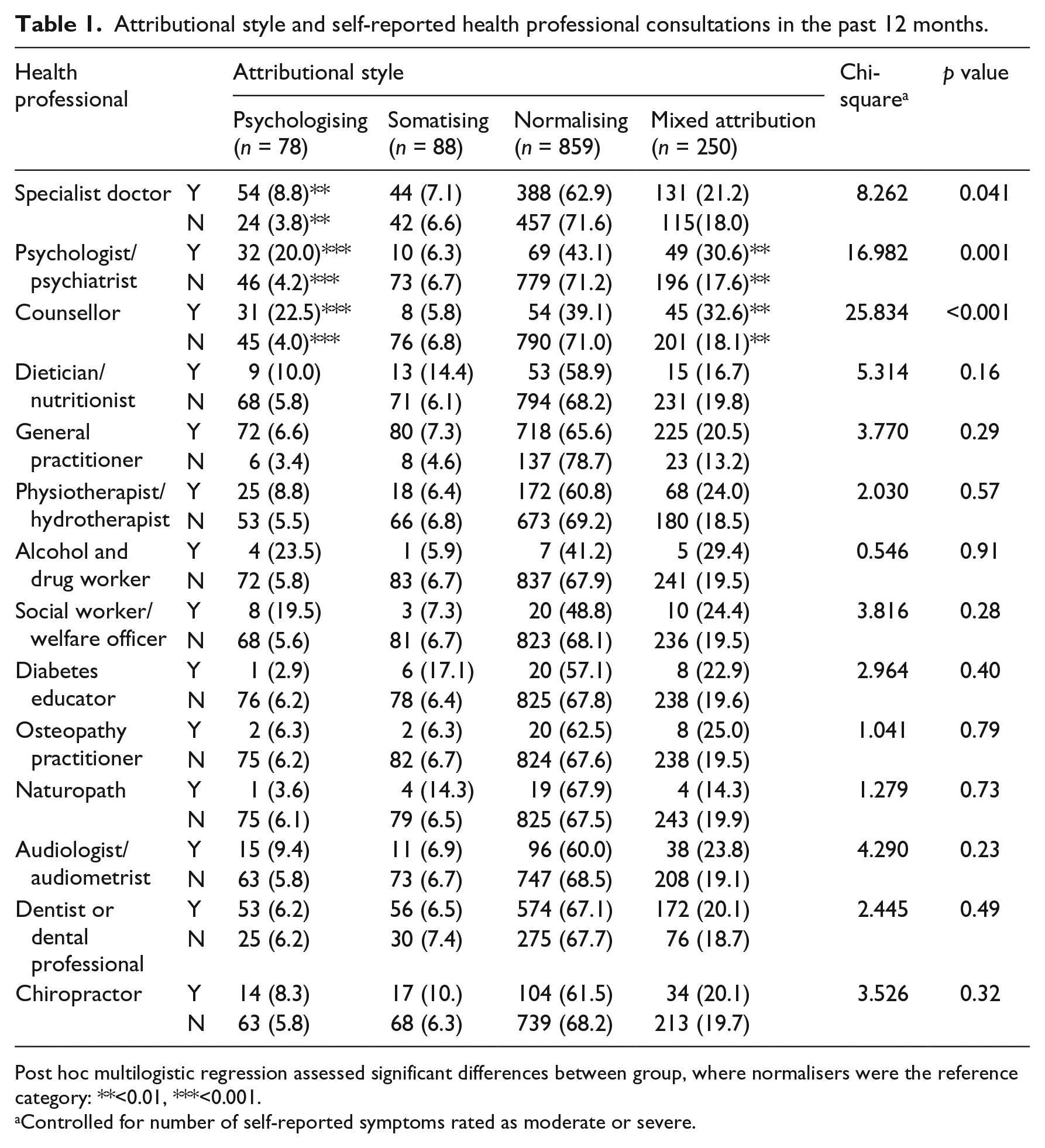
Post hoc multilogistic regression assessed significant differences between group, where normalisers were the reference category: **<0.01, ***<0.001.
Controlled for number of self-reported symptoms rated as moderate or severe.
Further to this self-report data, linkage with MBS, DVA-held health data, PBS and RPBS were utilised. Medicare Australia is an Australian government–funded national programme that covers a wide range of healthcare services. The MBS is a health publication listing services that are subsidised by the Australian government under the Medicare system. Linkage with DVA-held health data was conducted to obtain additional MBS data that were processed through the DVA system and thus were not captured through linkage with MBS alone. PBS data list payments to pharmacies after a PBS-listed medicine has been dispensed to a patient. The RPBS lists all medicines dispensed in Australia to eligible veterans at a DVA-subsidised price. The MBS, DVA-held health, PBS and RPBS data were obtained for the period 1 January 2001 to 15 August 2012. Each consenting participant’s identification information was linked with the above databases. Linkage with these databases provided a comprehensive picture of individual participants’ healthcare usage, as participants may have used either the general public health or pharmaceutical system or accessed care through the DVA health system.
Variables were derived from the linkage data relating to any GP consultations in the past 12 months and the total number of GP consultations in the past 12 months; any consultation with five specialist doctors (psychiatrist, gastroenterologist, neurologist, dermatologist and respiratory physician: chosen to reflect key health concerns in Australian Gulf War veterans) in the past 12 months and past 10 years; and any and the total number of pharmaceuticals dispensed in the past 12 months.
Statistical analyses
Bivariate analyses (chi-square) were used to test differences in categorical variables across attributional style. Significant differences were further investigated with multinomial logistic regression, controlling for frequency of symptom reporting, where normalisers were used as the reference group. The multinomial logistic regressions were used to analyse both main effects for attributional style and symptom reporting on the outcome variables. Differences in continuous variables across attributional style were explored using analysis of covariance (ANCOVA) controlling for symptom reporting, with post hoc Bonferroni tests. Data analysis was performed using SPSS version 21.
Results
The analyses found that attributional style demonstrated significant relationships with self-reported treatment-seeking behaviours and specialist consultations; however, the majority of variance was accounted for by the frequency of symptom reporting. After controlling for symptom reporting, significant differences were found for consultations with specialist doctors, psychologists/psychiatrists and counsellors; the results for adjusted analyses are displayed in Table 1. Further analyses using multinomial logistic regressions were conducted to identify which groups were significantly different. The pattern observed in these post hoc differences reflected that participants who consulted a specialist doctor were more likely to be psychologisers than normalisers and participants who consulted either a psychologist/psychiatrist or a counsellor were more likely to be psychologisers or mixed attribution.
The linkage data with the MBS and DVA-held MBS data were used to further explore these treatment-seeking behaviours in relation to specialists. The majority (86.5%) of participants had not consulted any of the listed specialists in the past 12 months, but a considerable number had consulted at least one specialist (12.3%), a small number had consulted two specialists (1.2%) and a fraction had consulted three (0.1%). There was a significant relationship between consulting any specialist in the past 12 months and attributional style, but this did not remain significant when symptom reporting was controlled for (p > 0.05).
In the past 10 years, almost two-thirds (64.2%) of participants had not consulted any specialist, 24.4 per cent had consulted one specialist, 8.0 per cent had consulted two specialists, 2.7 per cent had consulted three specialists and 0.7 per cent had consulted four. Similar to the results for the past 12 months, at 10 years, the relationship between any consultation and attributional style did not remain significant after controlling for symptom reporting.
When investigating differences in attributional style for individual specialists, psychiatrist consultations in the past 10 years were significantly different, but were not significant for the past 12 months, after controlling for symptom reporting (see Table 2). Participants who had a psychiatrist consultation in the past 10 years were more likely to be psychologisers, somatisers or mixed attribution than normalisers. Although there was a significant overall relationship between attributional style and gastroenterologist consultations in the past 12 months, no post hoc differences between attributional styles were revealed.
Attributional style and specialist consultations since 2001 based on MBS/DVA-held MBS data.
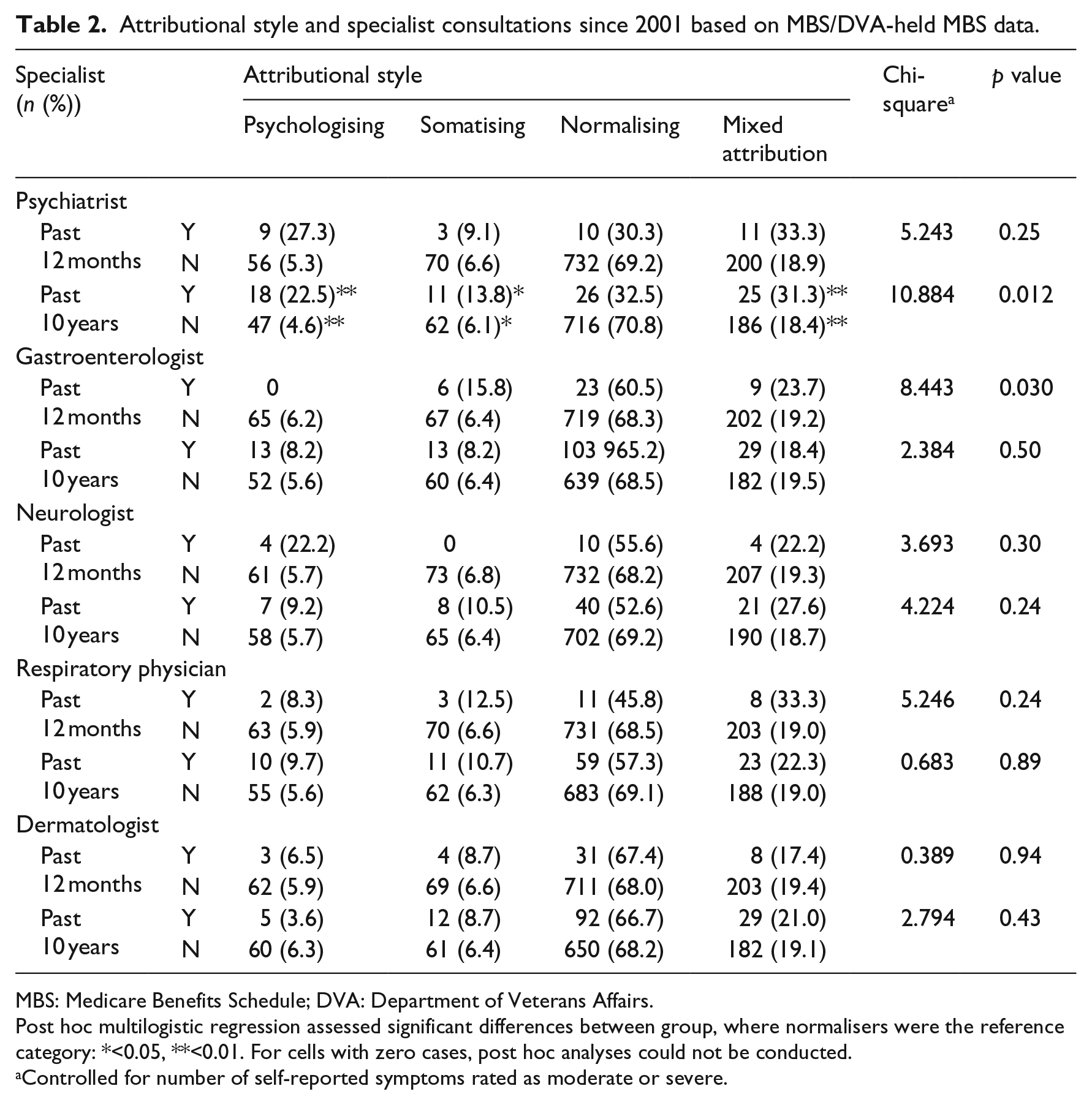
MBS: Medicare Benefits Schedule; DVA: Department of Veterans Affairs.
Post hoc multilogistic regression assessed significant differences between group, where normalisers were the reference category: *<0.05, **<0.01. For cells with zero cases, post hoc analyses could not be conducted.
Controlled for number of self-reported symptoms rated as moderate or severe.
Attributional style was investigated for any relationship with GP consultations recorded by MBS and DVA-held MBS data; the adjusted results are presented in Table 2. After controlling for symptom reporting, there was no statistically significant difference for attending any GP consultation in the past 12 months. However, the mean total number of GP consultations in the past 12 months differed significantly across attributional style (Table 3). Post hoc analyses revealed that normalisers had fewer consultations in the past 12 months than both somatisers (p = 0.001) and mixed attribution (p < 0.001).
Attributional style and general practitioner consultations in past 12 months based on MBS/DVA-held MBS data.
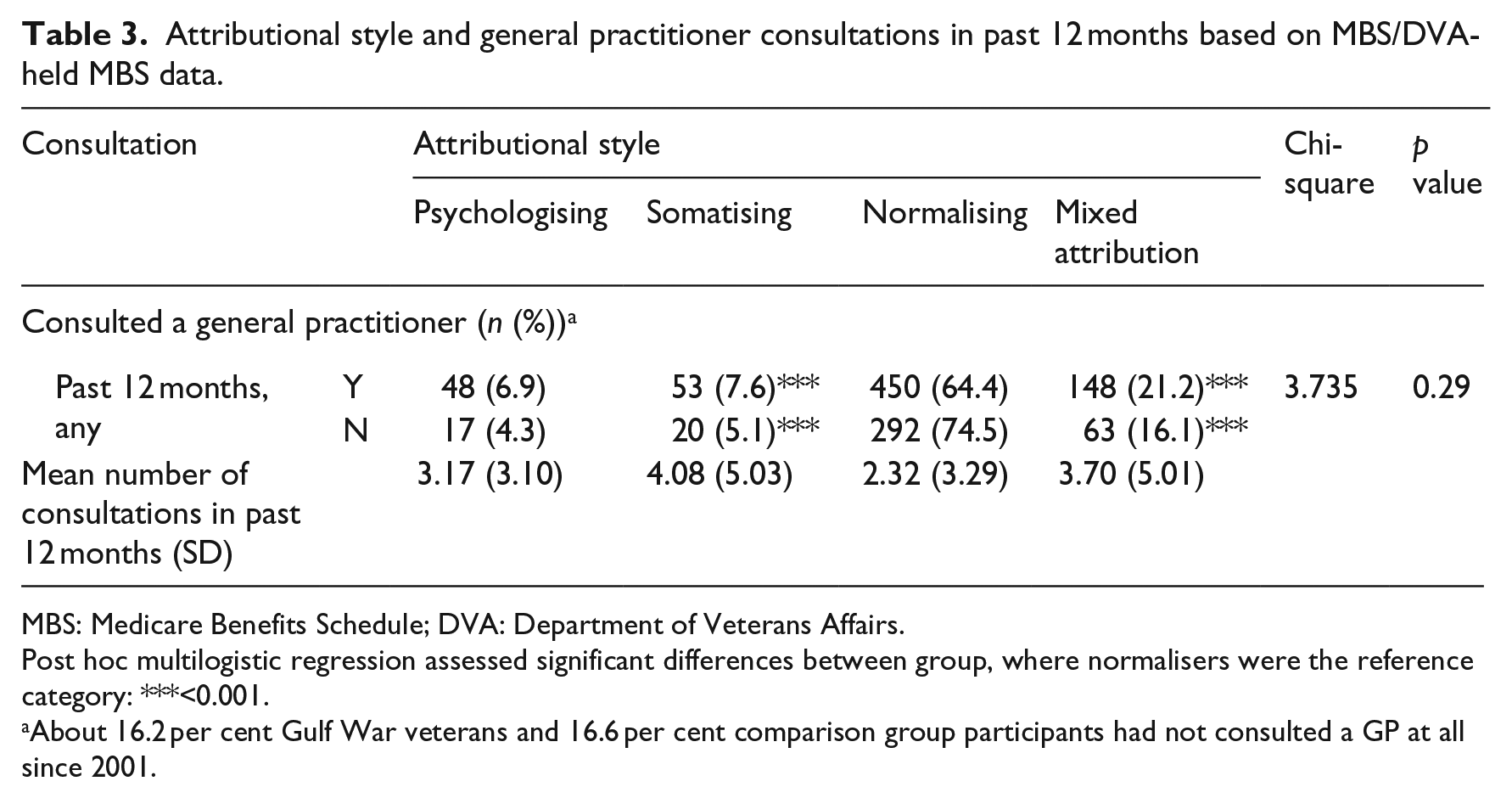
MBS: Medicare Benefits Schedule; DVA: Department of Veterans Affairs.
Post hoc multilogistic regression assessed significant differences between group, where normalisers were the reference category: ***<0.001.
About 16.2 per cent Gulf War veterans and 16.6 per cent comparison group participants had not consulted a GP at all since 2001.
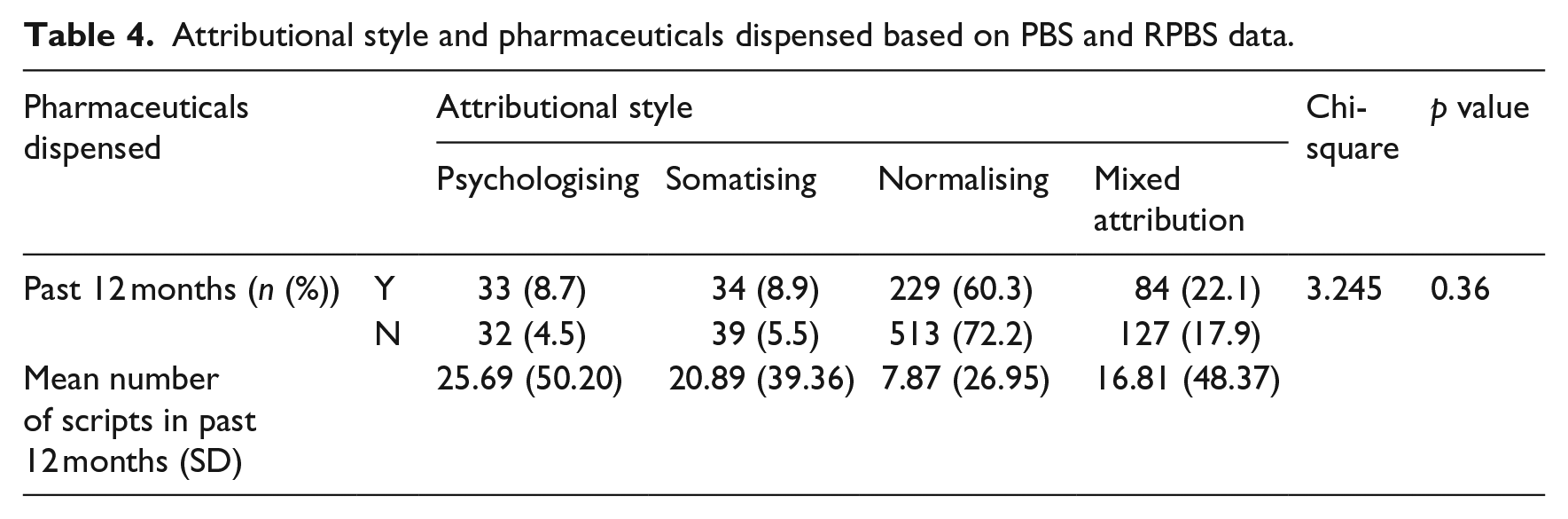
Combined data from the PBS and RPBS were used to indicate medication use: whether participants had at least one script filled in the past 12 months and the total number of scripts dispensed in the past 12 months. The mean number of scripts dispensed in the past 12 months remained statistically significant across attributional style, after controlling for symptom reporting (see Table 4). Post hoc analyses revealed that normalisers filled significantly fewer scripts than psychologisers (p < 0.001) and mixed attribution (p < 0.001). Somatisers were not significantly different from normalisers after controlling for symptom reporting and no other attributional styles were significantly different.
Attributional style and pharmaceuticals dispensed based on PBS and RPBS data.
Discussion
Above and beyond the influence of symptom reporting, different attributional styles had significant relationships with treatment-seeking behaviours. Attributional style was associated with self-reported specialist consultation, psychology-related consultations (self-reported and linkage), gastroenterologist consultations based on linked data, number of GP visits and the number of prescriptions filled. Psychologisers were more likely to attend specialist consultations and in particular psychologists/psychiatrists and counsellors, as well as having more pharmaceutical scripts filled. Mixed attribution demonstrated a similar profile to psychologisers with more attendance at psychiatrists and counsellors, more GP visits and more prescriptions. Somatisers attended more GP visits than normalisers. There was a clear pattern that normalisers used the fewest health services and had the fewest prescriptions filled.
Engagement with psychology-related consultations was similar across psychologisers and mixed attribution, who were more likely to engage with psychologist/psychiatrist and counsellor consultations both in the past year and over the past 10 years. Psychologisers and mixed attribution displayed similar treatment-seeking behaviours and specialist consultations throughout the results. Psychologisers may be more likely to attribute psychological explanations to their symptoms (Robbins, 1991) which in turn leads to requests for, or referral to, psychological treatments. This may also include psychologisers presenting their symptoms in a way that increases clinicians’ recommendation of psychological treatments. Findings show that a psychologising style can influence GP recognition of distress (Kessler et al., 1999), so their presentation style may also have a consequent effect on referrals and subsequent treatment options. For patients’ care, it is important to understand these interactions so that clinicians can make informed decisions about appropriate care and treatment options.
For engagement with regular healthcare, somatisers and mixed attribution had attended more GP visits in the past 12 months. Indicating that despite frequency of symptom reporting, these styles perceived a greater need for healthcare. Previous research suggests that somatising and psychologising styles involve more anxiety (Sensky et al., 1996); thus, the greater number of GP visits for somatisers and mixed attribution may be due to a tendency for them to worry more about their symptoms (Sensky et al., 1996). They are perhaps seeking reassurance or recourse to treatment. There may be difficulties for GPs to manage these patients and their anxiety about symptoms which may currently lead to more referrals. However, it is also important to note that in the Australian context, individuals are entitled to funded visits to a psychologist, but a referral must be obtained from a GP first. Therefore, it is possible that some of the visits are related to psychological concerns and the need for referrals. If GPs had more information about attributional styles, this could help them in how to best manage patients with different styles and concerns, including tendencies to promote particular symptom interpretations or conversely downgrade symptoms; this could have implications for referrals and treatment options.
Normalisers have been found to be the principal attributional style in populations studied thus far (Kessler et al., 1999; Robbins, 1991), including Australian veterans (Wright et al., 2015), so it is particularly important to understand the implications for healthcare usage of this group. Normalisers exhibited the fewest treatment-seeking behaviours throughout the results; previous results also found that normalisers in this population also report fewer symptoms across somatic, cognitive and psychological measures (Wright et al., 2015). Normalisers may dismiss symptoms as being unnecessary of treatment, or they may feel that medical treatment will not address or resolve the symptoms they experience (Gulec, 2008). Their lower level of treatment-seeking behaviours could be due to not seeking medical consultations in the first place as evident by their lower number of GP visits; however, they may also not attend follow-ups and referrals. Due to this tendency, healthcare professionals need to be alert to the relevance and significance of normalisers’ presentation of symptoms as their severity may be underestimated and opportunities for early intervention missed. Normalisers may also require more attention to medication compliance due to their tendency to dismiss health-related concerns.
Our finding that normalisers reported the fewest GP visits correspond with findings from a UK population in which GP patients who attended more frequently made fewer normalising attributions (Sensky et al., 1996). Similarly, findings from a study of fibromyalgia patients indicated that normalisers demonstrated long-term patterns of non-treatment seeking (Gulec, 2008); this study could indicate that normalisers under-utilise health services even when they require treatment.
The associations with pharmaceutical data indicated that normalisers filled significantly fewer pharmaceutical scripts compared to psychologisers and mixed attribution. But this finding must be interpreted with care; it may be that as they attend GP and some other consultations less frequently than other attributional styles, there were fewer opportunities for them to be prescribed medication. Alternatively, it could be that their symptoms were not identified by healthcare professionals as requiring medications. It is possible that normalisers were less likely to fill scripts that they were given but it was not possible to investigate this further based on the data that were available.
Furthermore, the majority of the analyses demonstrated significant differences between normalisers and other attributional styles before symptom reporting was controlled for; however, as has been reported previously, normalisers may underreport their symptoms (Wright et al., 2015). This underreporting may indicate that a lower symptom threshold could be necessary for normalisers, thus controlling for the current symptom levels could be clouding the relationships with treatment seeking. Although it was not possible to explore this possibility within the given data set, this could be an important area for future research. The results presented demonstrated that beyond symptom experience and reporting, attributional style still plays an important role in treatment seeking and healthcare usage.
Taken together, these findings indicate that normalising may need to be recognised and better understood by healthcare professionals to ensure that symptoms are identified and treated appropriately and not dismissed as inconsequential. This may be particularly pertinent for veterans and other populations, who experience a range of symptoms (Forbes et al., 2004; McFarlane, 2010) which are persistent (Kang et al., 2009), and thus may need ongoing care and treatment. Healthcare professionals need to be aware of the implications that attributional style has on presentation and reporting of symptoms, as well as the individuals’ treatment preferences and potentially their treatment adherence. The increased likelihood of consultation attendance by psychologisers, mixed attribution and, to a lesser extent, somatisers indicates that over and above the contribution of symptom experience, symptom interpretation and attribution drives health concerns that impact on the likelihood of healthcare attendance, frequency of attendance and the type of healthcare attendance.
While this study utilised a large sample size and considered the discussed relationships in a veteran population among a range of outcome variables, there are some limitations that should be considered. Some data on consultations with health professionals were based on self-report and thus may be subject to recall bias; however, linkage with national medical and DVA-held databases provided objective data for comparisons. Although GP visits were analysed, we do not know from the data available the nature of the visit and what it related to. Visits to the GP can relate to a range of issues from renewing prescriptions, to test results, to establishing a Mental Health Plan. Therefore, interpretation of these data should be done with care. Furthermore, the available data for specialist consultations differed between self-report and linkage data; specific medical specialists of interest that were not included on the self-report list, but were available in the MBS/DVA-held MBS linkage data, include neurologist, gastroenterologist, respiratory physician and dermatologist. Furthermore, it is important to note that the number of prescriptions recorded as dispensed may not be the same number as those written by medical practitioners nor the same as medications actually taken by participants and does not indicate medication compliance. Finally, although symptom reporting was controlled for, medical and psychiatric conditions were not. Diagnosed conditions may demonstrate different relationships with attributional style and healthcare usage; this should be explored in future research. The present research provides fresh insight into treatment-seeking behaviours in veterans and indicates areas of importance for further investigation in the general population. Future research would benefit from looking beyond dichotomised variables of consultations, to frequency or measures of relative consumption of health services, and the influence of attributional style on specific forms of medication use and compliance. Further research should investigate whether the level of treatment-seeking behaviours or follow-up is appropriate for normalisers or if they under-engaged with healthcare and potentially jeopardising their health. Our understanding of attributional style and treatment-seeking behaviours may be furthered by investigating these relationships over time. It is particularly important to measure attributional style over time, which was not possible in this study. This study included objective medical services and pharmaceutical use data for the period 2001–2012, allowing us to define both recent 12-month and long-term 10-year usage, and it is anticipated that further data linkage will be sought in the future to further elucidate healthcare usage over time.
Conclusion
In conclusion, there were clear patterns between attributional style and treatment-seeking behaviours above and beyond symptom reporting; psychologisers and mixed attribution demonstrated similar patterns and were more likely to attend psychology-related consultations than normalisers. Normalisers attended the fewest GP consultations and had the lowest number of pharmaceutical scripts dispensed. Overall, the results indicate that attributional style is important in relation to some aspects of treatment-seeking behaviours and should be considered part of the constellation of factors that influence healthcare usage.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical declaration
The Human Research Ethics Committees of Monash University, Australian Department of Defence and Australian Department of Veterans Affairs approved the baseline and follow-up studies; all participants provided voluntary informed consent. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This journal article has been produced using funding provided by the Australian Government Department of Veterans’ Affairs (DVA) (Applied Research Program project no. 0907). However, the views expressed do not necessarily represent the views of the Minister for Veterans’ Affairs or the Department of Veterans’ Affairs. The Commonwealth does not give any warranty nor accept any liability in relation to the contents of this work. The funding body had no role in the conduct of the study, analysis of the results nor preparation of this manuscript.