
Abstract
The rapid expansion of digital health technologies has prompted questions about their influence on cognition. This study investigates how physical activity, psychological well-being, technology readiness, and digital health innovations contribute to cognitive performance, with self-efficacy as a mediator and perceived usefulness as a moderator. A stratified sample of 1025 Chinese physical education students completed questionnaires, and Structural Equation Modeling was applied. SEM examined direct and indirect relationships, while mediation and moderation analysis examined how self-efficacy and perceived usefulness affected associations. Digital health technology engagement, self-efficacy, psychological well-being, and technology readiness improve cognitive outcomes. A mediation analysis suggests that self-efficacy influences digital health technology use, psychological well-being, and cognitive function. Moderation analysis shows that perceived usefulness amplifies relationships among technology use, exercise involvement, and cognitive outcomes. The findings suggest adding digital health tools, physical exercise, and self-efficacy support to physical education programs to boost psychological and cognitive engagement
Keywords
Introduction
Digital technology has impacted education, health care and wellbeing quite fast. Digital innovations, including wearable fitness trackers, health applications, and AI-based coaching assist in physical education by engaging and being more efficient (Lampreia et al., 2024). With the increased rates of sedentary behavior, obesity and mental health care issues, digital health solutions are needed to improve and ensure activity and wellbeing. in China, where humanity is becoming increasingly digital and emphasizing personal health, it is important to learn how digital health tools can influence physical education. The government programs assist in national fitness, technological assimilation in education and active health management (Morris et al., 2025). Exercise also has a positive impact on cognitive and emotional aspects, including students’ memory, attention, problem-solving abilities, and decision-making (Herbert, 2025; Song et al., 2025). Conventional physical education might require programs that are not customized and which lack innate motivation hence engagement decline (Pan and Hsu, 2025). Online courses with the ability to make learning adaptive, provide instant feedback, and achieve goal setting, motivate and enhance adherence.
Exercise is a key theme of physical activity that can greatly benefit the mental health of students, alleviating stress, enhancing mood and socialization (Hossain et al., 2024). Digital health products such as virtual coaching, game-based workouts, and measuring progress can make physical education more interactive and consequently more involved (Choi et al., 2025). The focus of adoption within an accessible technology context is more advantageous to those students that are tech-savvy, whereas among others, it might prove difficult due to the gap in skills or privacy matters (Schei et al., 2024). Engagement is also affected by what students think of utility, which shows that accessible and effective interventions are necessary (Li and Liu, 2024).
The case of Self-efficacy also determines participation in physical education. The students that believe more in themselves continue with struggles and advance on physical tasks (Lockyer et al., 2024). Self-efficacy is improved by digital health tools, incorporating action feedback, goal setting, and tracking of progress and reinforces engagement and wellbeing over life (Makda, 2025). Digital health innovations can also influence cognitive performance and mental health via their effect on self-efficacy. Digital integration of health is particularly timely because of the focus of increasing the technological development and educational changes in China (Deng et al., 2023). Smart classrooms, artificial intelligence solutions, surveillance systems are used by schools to improve results. In order to be efficient in integration, one will need to know how the technology, psychological, and instructional factors interrelate.
A coherent narrative pattern guides this research on the mental and cognitive consequences of digital health technologies in PE. Based on recent findings (Hong et al., 2024), the study first examines students’ psychological well-being and their use of digital health tools. It seeks to minimize stress, manage anxiety, and assess the effects of these tools on students’ mental health. Cognitive outcomes examine whether digital health devices improve memory, attention, and decision-making. Despite its extensive advocacy for cognitive enhancement, AI-assisted platforms and biofeedback devices have yet to be proven effective in organized PE contexts (Mitsea et al., 2024). This study illuminates these links in instructional sports. The study concludes by investigating self-efficacy as a psychological mechanism through which advances in digital health improve mental health and cognition. Digital technologies may indirectly improve results by boosting self-confidence, goal-setting, and self-monitoring (Min et al., 2022). This study investigates whether students’ mental health and cognitive capacities improve when they use digital health devices more and have stronger self-belief.
The study examines how digital health technologies in PE courses affect students’ mental health and cognitive capacities, not only grades. Research focuses on cognitive skills, including attention, memory, and decision-making, as well as mental health outcomes such as stress, anxiety, and psychological well-being. The research includes students at different academic and professional development stages to understand better how technology-based tools support learning, mental health, and cognitive engagement in physical education. A secondary objective is to explore how self-efficacy influences the favorable mental health and cognitive effects of digital health technology use. The study aims to determine whether students’ self-confidence underpins these links between digital technology use and benefits. The research seeks to examine how technical preparedness and accessibility affect the performance of digital health solutions. It seeks to determine if students’ digital health technology readiness moderates the relationship between digital health technology use and psychological well-being and cognitive performance in physical education.
Digital health technology can enhance physical education within China’s rapidly evolving educational system. This study examines the effects of these tools on students’ mental health and cognitive function, providing insights for policymakers, curriculum designers, and educators implementing health-focused programs. With rising academic pressures and lifestyle changes affecting student wellbeing, the findings inform strategies to leverage digital health technology to improve mental health. The research also highlights how digital interventions support learning and critical thinking, with self-efficacy mediating the relationship between confidence, personal belief, and academic achievement. Educators, psychologists, and technology developers can use these findings to improve physical education and classroom digital health tools. Overall, this study aims to help students in China benefit from technological advances and enhance both personal and academic outcomes.
Literature review
Digitalizing physical education may enhance students’ mental health and academic performance. Technological interventions, including virtual training, AI-powered fitness apps, and wearable devices, can improve psychological wellbeing, learning efficiency, and academic outcomes in Chinese students. Evidence shows that virtual coaching, wearable trackers, and AI-based programs support emotional stability, reduce anxiety, and increase motivation (Hu et al., 2024). Fitness-tracking applications reduce stress and foster engagement compared to traditional programs (Danković et al., 2023). Personalized digital guidance strengthens self-confidence and emotional regulation (Zhu et al., 2024). Digital health innovations also support cognitive performance. AI-powered modules enhance problem-solving and cognitive flexibility (Gkintoni et al., 2025). Virtual reality in physical education improves processing speed and multitasking ability (Wollesen et al., 2022). Gamified and immersive learning approaches reduce mental fatigue and academic burnout (Hou et al., 2025) and improve concentration and task-switching. Overall, technology-driven physical education positively influences students’ mental and cognitive development while promoting engagement and self-efficacy.
Numerous studies on online education have examined technology readiness as a key factor in students’ adoption and success with digital instructional resources (Robinson Jr, 2025; Veseli et al., 2025). Students’ classroom preparation indicates their technical proficiency, desire to try new things, and confidence with digital tools (Deng and Liu, 2025; Zhang, 2025). Research shows that online learning platforms, mobile health apps, and wearable tech benefit students who are more tech-savvy (Goel et al., 2025; Khlaif et al., 2025). Physical education students utilize activity monitors, fitness applications for mobile devices, and systems that track performance in cognitively and physically demanding exercises, making technology preparation crucial. Al-Emran et al. (2023) found that student readiness to use such technologies improves self-regulation, motivation, and activity-based learning. Consequently, this research views technological preparedness as an essential prerequisite that determines the nature of the relationship between physical education students’ mental health and their ability to think critically and solve problems. Based on the stated literature, the study’s first research hypothesis is as follows:
Digital health innovation and interest in teaching and learning strategies like interactive learning modules and real-time monitoring performance determine the mental health of students and their academic performance. One-to-one digital coaching increases the resilience and motivation to respond to stresses in academics (Polat, 2024). Online methods to gamify physical education increase emotional stability and decreased performance anxiety (Liu et al., 2025). There are physiological feedback systems and real-time analytics that foster cognitive engagement and wearable devices have already been indicated to make people more aware and faster in decision making (Hsu et al., 2023). Interactive programs based on AI technologies will make it more attentive and have higher learning ability (Alam and Mohanty, 2023), whereas adaptive training strengthen the memory and understanding process (Gligorea et al., 2023). Exercises done via motion sensors also enhance reaction time and spatial cognition (Yu, 2024). The study’s second research hypothesis is as follows, that is,
Digital health and engagement strategies affect psychological and cognitive outcomes, although self-efficacy and technological availability attenuates these effects. Self-efficacy, the belief that one can achieve goals affects students’ mental and emotional responses to digital health treatments. Bandura (1978) presented self-efficacy as a key psychological concept that boosts motivation and learning. Rohde et al. (2024) found that self-efficacy helped students use digital health applications. This is because these students were more resilient and stress-tolerant. Alrashidi and Alshammari (2025) argued that active participation in virtual training programs improved students’ cognitive results and self-efficacy beliefs. Lack of digital tools, inconsistent internet connections, and economic constraints may prevent students from fully engaging in technology-driven physical education programs. Zhang (2025) found that students with easy access to exercise apps were more mentally flexible and resilient. When institutions encouraged equitable access to digital health resources, Al-Motrif (2025) found that student’s mental health and cognitive engagement increased. The dynamic framework produced by self-efficacy, technological accessibility, and digital health technologies may help explain students’ psychological and cognitive outcomes. Technology accessibility ensures equal opportunities for all students, which moderates the link between digital health adoption and cognitive performance (Şahin, 2025). Self-efficacy mediates. Digital therapies offer great potential and demonstrate that students’ psychological attitudes and technical skills greatly impact their performance. The final research hypothesis is as follows:
Although the research on digital health, mental well-being, and cognitive performance expands, empty areas exist. Not many investigations take the impact of digital health tools on the cognitive ability of students in classrooms, with most of the article paying attention to the results of physical activity (Meng et al., 2025). There is a severe lack of research on the impact of gamification and personalized feedback and other engagement techniques on emotional stability and overall academic adaptation. In the vast majority of studies, the results are written over a short-term perspective, and their long-term consequences on mental and cognitive well-being remain unclear (Gutierrez et al., 2025). There is very little research in non-western settings and especially in China and this makes generalization hard as a result of cultural and institutional diversity. Person difference in terms of self-efficacy and access to technology is frequently overlooked, yet multiple studies have the capability of altering the effectiveness of the digital health program (Bao et al., 2022).
This paper fills these gaps by exploring findings related to the impacts of digital health tools on emotional stability, cognitive adaptability, decision-making, and academic engagement. It also takes into account the technology-based approaches to engagement and their impact on cognitive and mental outcomes. By placing the study in China, it allows the cultural and institutional issues on technology acceptance in the field of physical education. Such incrementation as self-efficacy and access to technology is a way to excavate a careful reflection of individual reactions to digital health interventions. Results will inform policy makers, educators and people involved in development of inclusive, effective, and culturally appropriate digital health programs to students.
Theoretical framework
This study is based on numerous well-established theories on digital health innovations, psychological wellbeing, and physical education cognitive performance. The Self-Determination Theory (SDT) emphasizes relatedness, autonomy, and competence for inner motivation and wellbeing (Deci and Ryan, 2013). SDT helps understand how technology-driven engagement and digital health tools increase students’ cognitive abilities and psychological resilience via tailored and interactive learning. Providing students with digital fitness applications, gamified physical education platforms, and AI-driven health treatments may enhance their mental health and academic performance. Cognitive Load Theory (CLT) is essential for understanding how digital health devices affect mental capability. According to CLT, optimal learning environments promote memory retention and problem-solving, whereas excessive cognitive load impairs learning and decision-making (Sweller, 1988). Through adaptive and interactive technology, digital health treatments in physical education classrooms may reduce cognitive overload and promote academic engagement. The Technology Acceptance Model (TAM) shows how freely available technology connects digital health improvements to mental and emotional wellbeing. Technology adoption is largely impacted by ease and usefulness, according to TAM (Venkatesh and Davis, 2000). Digital health technology can only help students’ wellbeing if adopted and utilized. Finally, Bandura’s Self-Efficacy Theory helps explain how students’ self-perceptions affect their digital healthcare interactions. According to Bandura’s theory, self-efficacious persons are less likely to give up on complex tasks, more likely to utilize technology to learn, and less likely to suffer psychological distress (Bandura, 1997). It is observed that students with strong self-efficacy were more likely to benefit from digital health innovations, which boosted cognitive flexibility and psychological resilience. Based on these theoretical views, Figure 1 shows the study’s conceptual framework. It shows the relationships between digital health innovations, psychological wellbeing, cognitive performance, engagement techniques, self-efficacy, and technological accessibility. Based on these theories, the study hypothesizes that digital health innovations greatly improve mental health and cognitive function (H1), engagement strategies amplify these associations (H2), and self-efficacy and technology accessibility mediate and moderate these effects (H3).
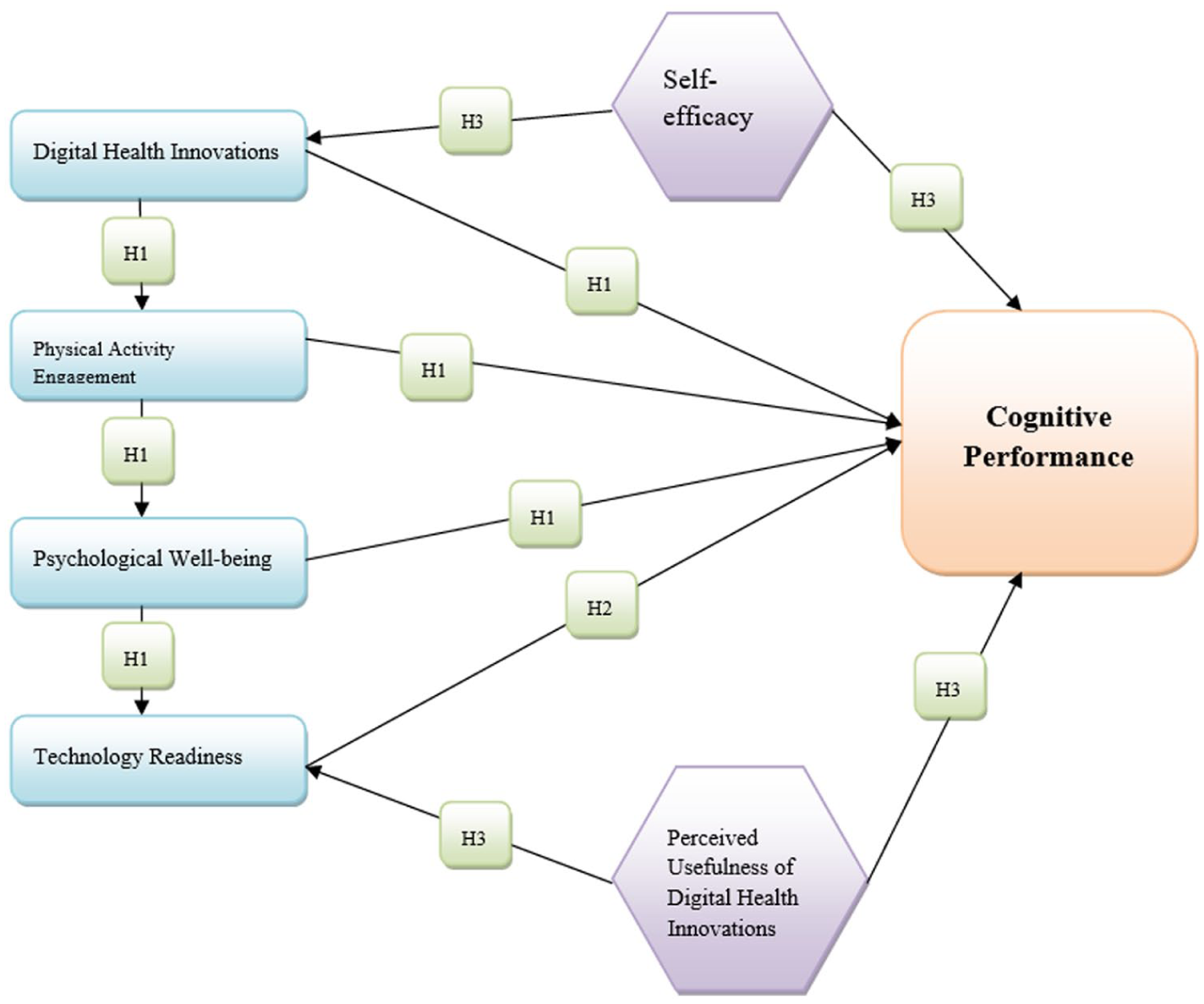
Theoretical framework.
Digital health innovations and physical activity integration (H1) promote psychological well-being and cognitive function since technology-driven treatments increase mental resilience and cognitive engagement. H2 predicts that digital engagement and individualized learning will improve intrinsic motivation, memory retention, and cognitive ability. Since self-efficacy regulates these relationships, those who believe in themselves have higher mental health and cognitive function (H3). Technological readiness (H3) may increase or decrease these effects depending on how open and adaptable PE students are to digital technologies. These aspects show how technological innovation might improve China’s physical education curriculum by improving students’ emotional and intellectual well-being. This research examines these theorized relationships to determine how to employ digital interventions to enhance students’ psychosocial and cognitive outcomes.
The study employed a structural equation model (SEM) grounded in psychology, cognition, and technology adoption theories to explain the relationships among digital health innovations, psychological traits, and cognitive performance in physical education. Self-Determination Theory underpins the model’s psychological processes. SDT bases excellent functioning and psychological well-being on relatedness, competence, and autonomy. Digital health technologies such as activity trackers and fitness apps may boost mental health and help people exercise longer by enabling self-monitoring and goal-setting, according to studies. Thus, the SEM hypothesizes that digital health, psychological health, and physical activity improve cognitive function. Bandura’s Self-Efficacy Theory strongly influences the SEM’s self-efficacy mediating function. According to the theory, self-confidence affects drive, determination, and productivity. Digital health technology could boost self-efficacy by providing real-time feedback, tracking progress, and rewarding success. This hypothesis posits that self-efficacy mediates the relationships among technological preparedness, digital health advancements, mental health, and academic achievement. Perceived utility may moderate the Technology Acceptance Model (TAM). TAM says technology adoption and success depend on how useful it is. The structural equation model (SEM) shows that perceived utility strengthens the linkages between digital health advances, physical activity, technological preparedness, and cognitive performance. If students value digital health tools for mental and emotional well-being, they will benefit more. Cognitive Load Theory underpins the links between digital health technologies, exercise, and mental sharpness. The CLT says instructional strategies that reduce extraneous information and improve processing enhance learning outcomes. Well-designed digital health solutions may enhance executive functioning, memory, and attention by arranging feedback and activity demands to encourage physical activity. According to the SEM, self-efficacy and perceived usefulness jointly predict that digital health and physical activity increase cognitive performance.
The study relies on the psychometric literature on complex models that combine digital, psychological, and cognitive health components (Cross and Alvarez-Jimenez, 2024; Galatzer-Levy and Onnela, 2023). Structural Equation Modeling is used to assess latent psychological features, cognitive processes, and technology-related perceptions while accounting for measurement error and construct interdependencies. Integrating digital health perspectives, psychological factors like self-efficacy and preparation, and cognitive performance indicators requires established multi-item measures, strong construct validity, and rigorous convergent and discriminant validity. According to digital health and cognition studies, associations rather than causal effects explain cognitive results, particularly in cross-sectional designs (Çöme et al., 2025; Franke Föyen et al., 2023). Psychometric validation methods, such as reliability estimation, mediation and moderation testing in structural equation modeling (SEM), and confirmatory factor analysis, has been used to model the relationships among digital health preparedness, psychological factors, and physical activity. This study uses these well-established psychometric concepts to evaluate multidimensional Cognitive-Digital Health frameworks in youth and physical education, following current methodological standards.
Methodology
In accordance with EQUATOR Network standards, this study used a cross-sectional survey design and reported its findings using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) criteria. To ensure transparency, reproducibility, and scientific rigor, all methodological components were documented. These included participant selection, measuring instruments, data collection, and statistical analysis.
This study examines physical education students in universities and colleges across multiple regions where digital health and physical education programs are active. The sample included participants from six provinces, that is, Beijing, Shanghai, Guangdong, Jiangsu, Sichuan, and Shandong, representing diverse educational and technological environments. Representative institutions included Beijing Sport University, Shanghai University of Sport, Guangzhou Sport University, Nanjing Sport Institute, Chengdu Sport University, and Shandong Sport University. The study chose these provinces because their physical education curriculum uses technology, and their educational environments differ. With 1025 completed surveys out of 1250, the dataset’s reliability increased. The sample size for significant populations was estimated using Cochran’s formula. With 95% confidence and a 5% margin of error, the lowest sample size was 384. The final sample was expanded to ensure robustness. Table 1 displays province-specific response distributions.
Sample size and response rate.
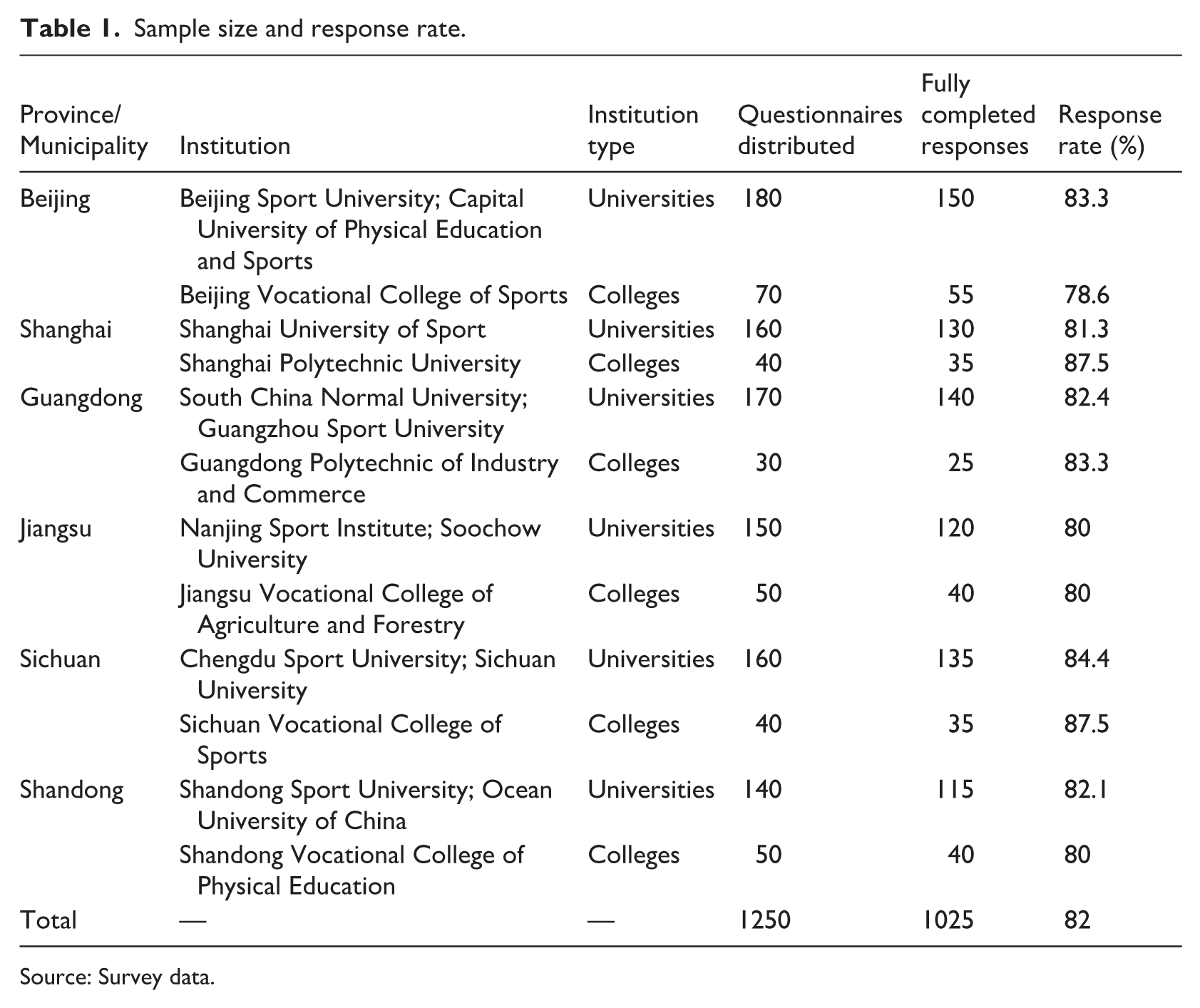
Source: Survey data.
The study targeted Chinese undergraduates, postgraduates, and Doctoral/Professionals in physical education from diverse regions. The curriculum included physical education, exercise science, sport science, and related professions that integrate academics with exercise. The study factors had to be relevant to schooling; thus, we excluded individuals from unrelated majors. The institution’s desire and accessibility determined whether a self-administered structured questionnaire was used online or in paper format. Academic coordinators sent questionnaires to students in class or via the school’s internet tools. All participants provided informed consent after finding the study’s goal. The final analysis included 1025 valid, complete surveys from 1250 students. Many efforts were taken to prevent bias or coercion. Participation did not confer any academic or motivational advantages. Second, respondents were assured anonymity and not asked for any identifying information. Third, participants were told their involvement would not influence their grade or academic standing. Data were collected using validated measurement scales, well-structured questionnaires, and consistent methodologies across institutions to reduce methodological bias.
The study employed stratified random selection to balance respondents from different regions and educational backgrounds. Tech adoption and digital health readiness dictated sample geographic stratification, not administrative boundaries. Selecting these provinces revealed the nation’s universities’ digital infrastructure, educational technology access, and utilization of health and learning tools. The selected areas differ in internet speed, smart-campus implementation, access to learning management systems, mobile health technology in PE, and institutional investment in digital pedagogical platforms. Sichuan, Jiangsu, Guangdong, and Shandong have highto medium-level technological penetration, with expanding innovative education and digital health infrastructure. At the same time, Beijing and Shanghai were included due to their advanced digital ecosystems and early adoption of health-related digital technologies. This stratification strategy allowed us to reduce regional technological homogeneity bias and to study better the relationships among digital health tools, psychological factors such as self-efficacy and readiness, and cognitive performance among physical education students. A structured questionnaire employing established scales from prior research ensured the validity and reliability of the measuring instruments. The study assessed all latent structures using multi-item psychometric measures. Each variable has five items to ensure construct coverage and measurement reliability. The items were rated on a five-point Likert scale, with 1 indicating strong disagreement and five strong agreements. Mental health and cognitive function were the dependent variables, whereas digital health innovations, physical activity integration, tailored learning, and digital engagement were the independent factors. The study includes self-efficacy and technical readiness as moderators and mediators.
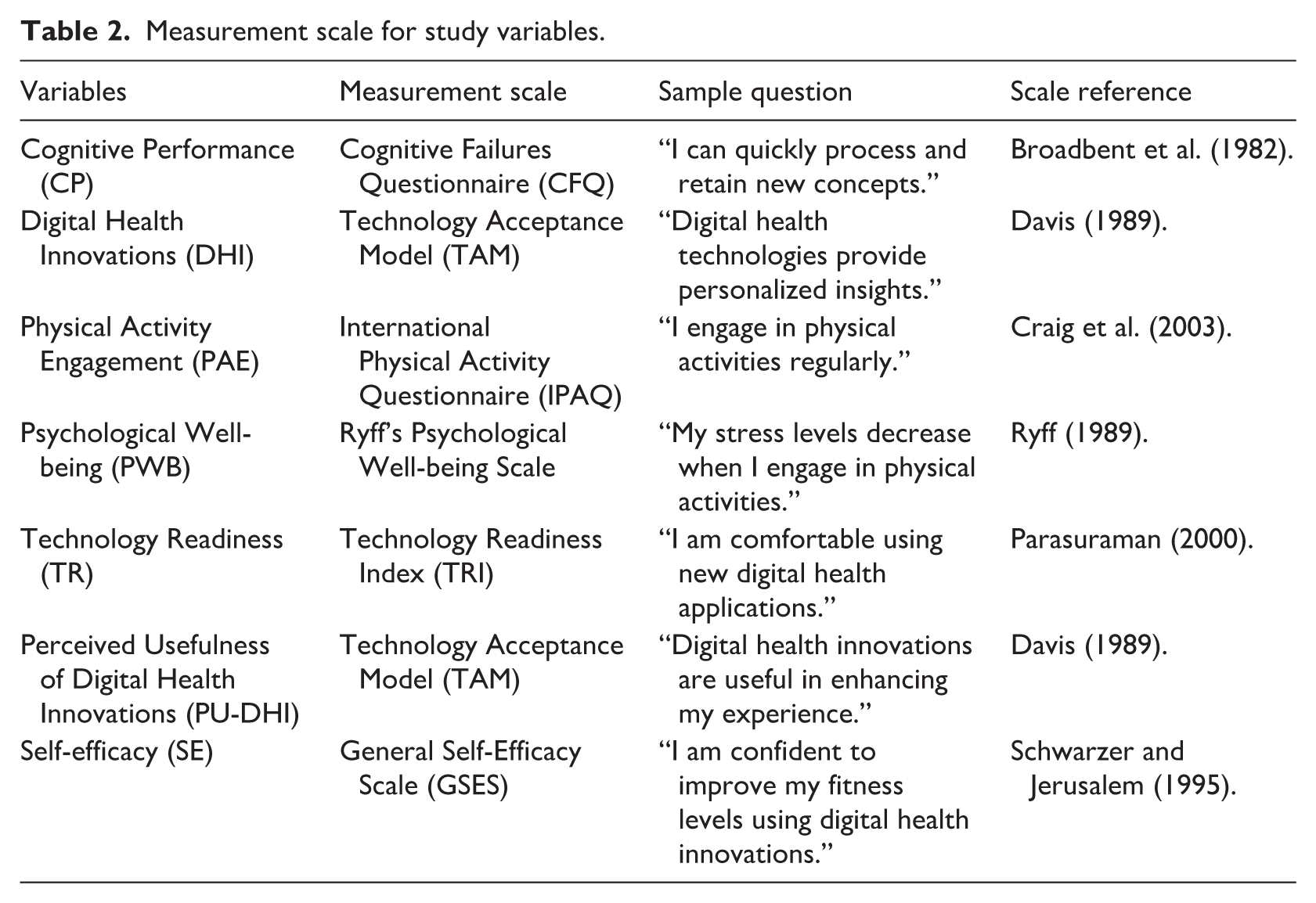
To assess cognitive performance, the study employed the validated self-report Cognitive Failures Questionnaire (CFQ), which evaluates the frequency of frequent cognitive failures rather than objective cognitive competence. To reflect daily cognitive problems, the CFQ measures attention, memory, perception, and action gaps. Lower CFQ scores indicate better cognitive functioning (fewer cognitive lapses), while higher scores indicate weaker cognitive functioning (more cognitive failures). The structural equation modeling investigations found links between digital health use, psychological traits, physical activity, and cognition to decrease cognitive failures, not cognitive performance. This interpretation is consistent with prior empirical applications of the CFQ in education and health research, as well as with psychometric recommendations. The General Self-Efficacy Scale (GSES) measures self-efficacy. The Psychological Well-being Scale was updated, and research connections were provided to assess mental health in education. Table 2 shows the scale measurements and the questions they asked. Table 2 shows the variables measurement scales and sample of asked questions.
Measurement scale for study variables.
A forward-backwards translation method was employed to translate English into Chinese. An expert in both English and Chinese translated the items into Chinese, and then another expert reversed the translation into English. It resolved inconsistencies to ensure conceptual coherence, cultural relevance, and semantic similarity. A pilot test with a small group of physical education students assessed item clarity, appropriateness of language, and contextual relevance. Based on participant feedback, minor language modifications were made before data collection.
To determine internal consistency of all measurement scales, Reliability analysis was administered with the help of Cronbachs Alpha. This 0.70 score is considered to be have a good reliability and any item, which decreased reliability, was changed or dropped. This gave a proper measurement of independent, dependent, mediating, and moderating variables. Confirmatory Factor Analysis (CFA) was conducted to calculate construct validity to determine the correspondence between the observable items and the underlying constructs. After testing the discriminant validity with the Fornell-Larcker criterion and Heterotrait-Monotrait ratio, the fact that the constructs are not overlapping was also tested.
The exploratory Factor Analysis (EFA) was used to describe the underlying structure of the data and code variables. Factor analysis adequacy was ascertained via the Kaiser-Meyer-Olkin which exceeds 0.70 and significant Bartlett-Test of Sphericity. Principal Component Analysis on Varimax rotation was applied to extract the components to minimize the cross-loadings and increase the clarity of factors. This was enhancing the model of measurement, and led to the framework of the study being increased.
The structural equation modeling approach examined concept validity using confirmatory factor analysis (CFA). Convergent validity is indicated by statistically significant factor loadings, composite reliability (CR) values above the specified thresholds, and AVE values above 0.50. Discriminant validity was verified using Fornell-Larcker criteria. The square root of AVE for each construct was bigger than its correlations with other constructs. These indicate that the adjusted measures are psychometrically sound for Chinese physical education. To suit strong conclusions, several metrics, including CFI, TLI, RMSEA, and SRMSR, were checked to model fit.
Hayes, PROCESS macro was used to carry moderation and mediation analysis. Moderation determined the impact of technology readiness on the relationship between digital health interventions and psychological well-being. In place of that, in mediation, self-efficacy had to answer the question of whether it was an indirect influence of physical activity integration on cognitive and psychological outcomes. The statistical significance of direct and indirect effects was determined using the Structural Equation Modeling framework, nonparametric bootstrapping with 5000 resamples. Since bootstrapping does not assume normality of the sample distribution, it is appropriate for indirect impact studies with non-normal distributions. Based on established methodological criteria, the study employs 5000 bootstrap resamples to obtain stable parameter estimates and believable bias-corrected confidence intervals. If 95% bias-corrected confidence intervals did not contain zero, effects were statistically significant. This strategy enhances inferential accuracy and reliability over normal-theory tests.
The structural regression results were used to assess the direct and indirect effects of digital health advances and the integration of physical activity on the mental health and cognition. Robust results were given by the use of significance levels, confidence interval, and adjusted regression coefficients. Such sophisticated analysis tools helped to elucidate the interdependence of the digital health technologies, physical activity, and student wellbeing, offering information to the study of education technology and physical education.
Ethical considerations
This study was conducted in accordance with the ethical standards of the 1964 Declaration of Helsinki and its later amendments. Ethical approval was obtained from an institutional research ethics board (Approval No. HU-REC/2023/1125). Informed consent was obtained from all participants prior to data collection. Participation was voluntary, and confidentiality and anonymity were strictly maintained throughout the study.
Results and discussion
Demographic data about participants in Table 3 is crucial to ensure the study’s findings represent the target population. The study’s 1025 participants were 54.6% male (n = 560) and 45.4% female (n = 465), indicating gender parity. The respondent age distribution is 45.9% (n = 470) were aged between 26 and 35 years, 37.1% (n = 380) were aged 19–25, and 17.0% (n = 175) were 36 years and above. Data shows that most responders were 19–35 years old, consistent with digital technologies in health and wellness initiatives.
Demographic characteristics of respondents.
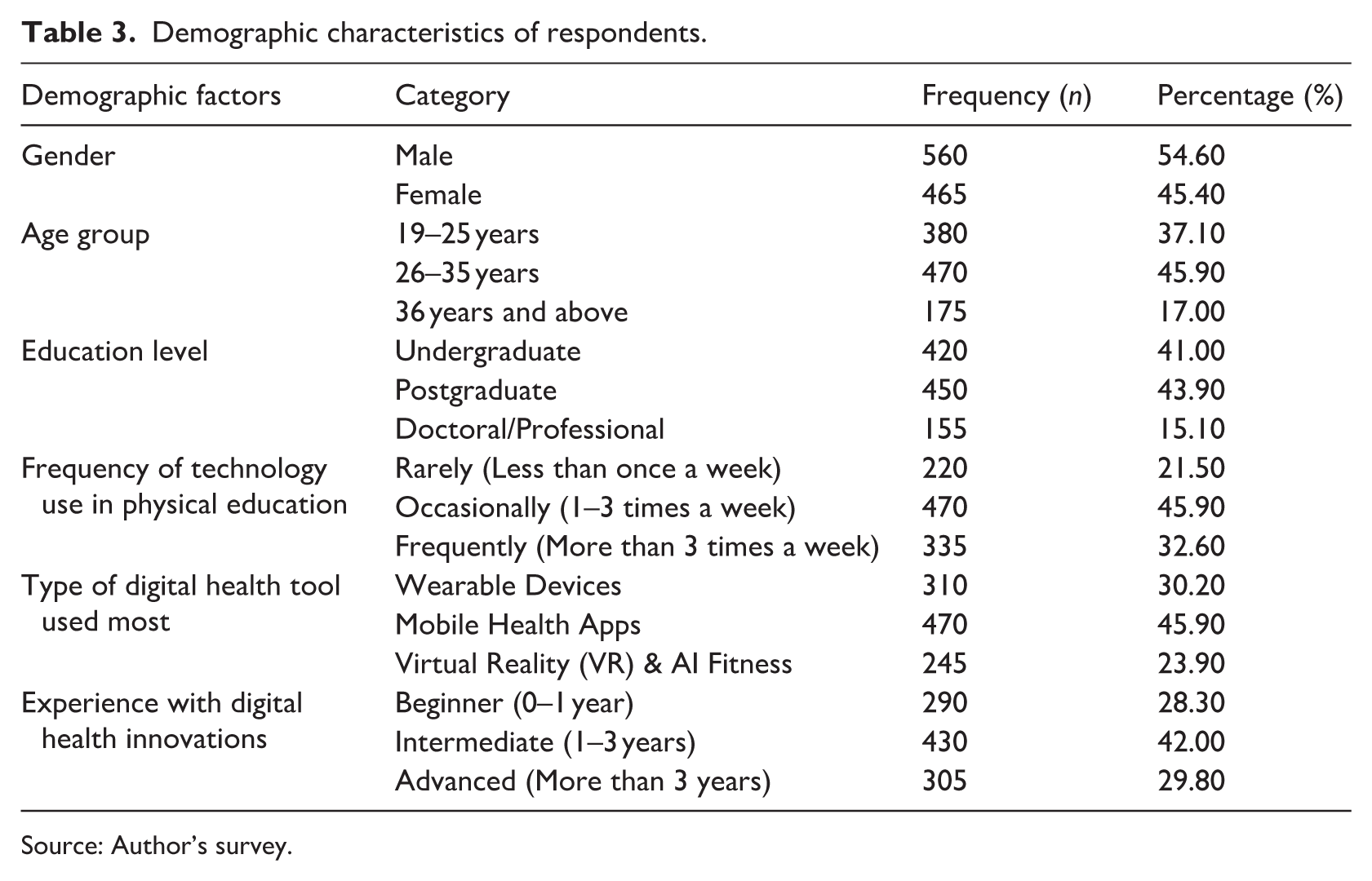
Source: Author’s survey.
According to their academic qualifications, most respondents were undergraduates (41.0%) or postgraduates (43.9%). Only 15.1% (n = 155) were doctoral or professional students. A significant number were graduate students in sport sciences, exercise physiology, coaching education, physical education pedagogy, and related subjects. Graduate students work with digital health technologies in their coursework, research, and applied training modules, as well as in physical education settings for advanced training and teaching. They complement the study’s focus on technology-facilitated PE and add depth by drawing on a range of academic levels within the same subject. Most participants had completed or were pursuing higher education and were familiar with digital health technologies in physical education. Technology use varied: 45.0% used it sometimes (1–3 times per week), 32.6% used it regularly (more than 3 times per week), and 21.5% rarely. Mobile health apps (45.9%, n = 470) were the most used tools, followed by wearable devices such as smartwatches and fitness bands (30.2%, n = 310) and VR/AI-based fitness solutions (23.9%, n = 245), reflecting accessibility and ease of use. Participants’ experience with digital health tools ranged from beginners (0–1 year, 28.3%) to intermediate users (1–3 years, 42.0%) and advanced users (over 3 years, 29.8%).
Descriptive statistics, reliability, and validity tests (Table 4) confirmed scale consistency. Mean scores ranged from 3.95 to 4.21, indicating positive perceptions of digital health innovations, psychological wellbeing, cognitive performance, self-efficacy, and technology readiness. Digital health innovations had the highest mean (4.21, SD = 0.72), while physical activity integration was lowest (3.95, SD = 0.68). Standard deviations ranged from 0.68 to 0.75, with psychological wellbeing showing the highest variability (SD = 0.75) and physical activity integration the lowest, indicating consistent responses in this area.
Descriptive statistics, Cronbach’s alpha, KMO measure, and Bartlett’s test of sphericity.
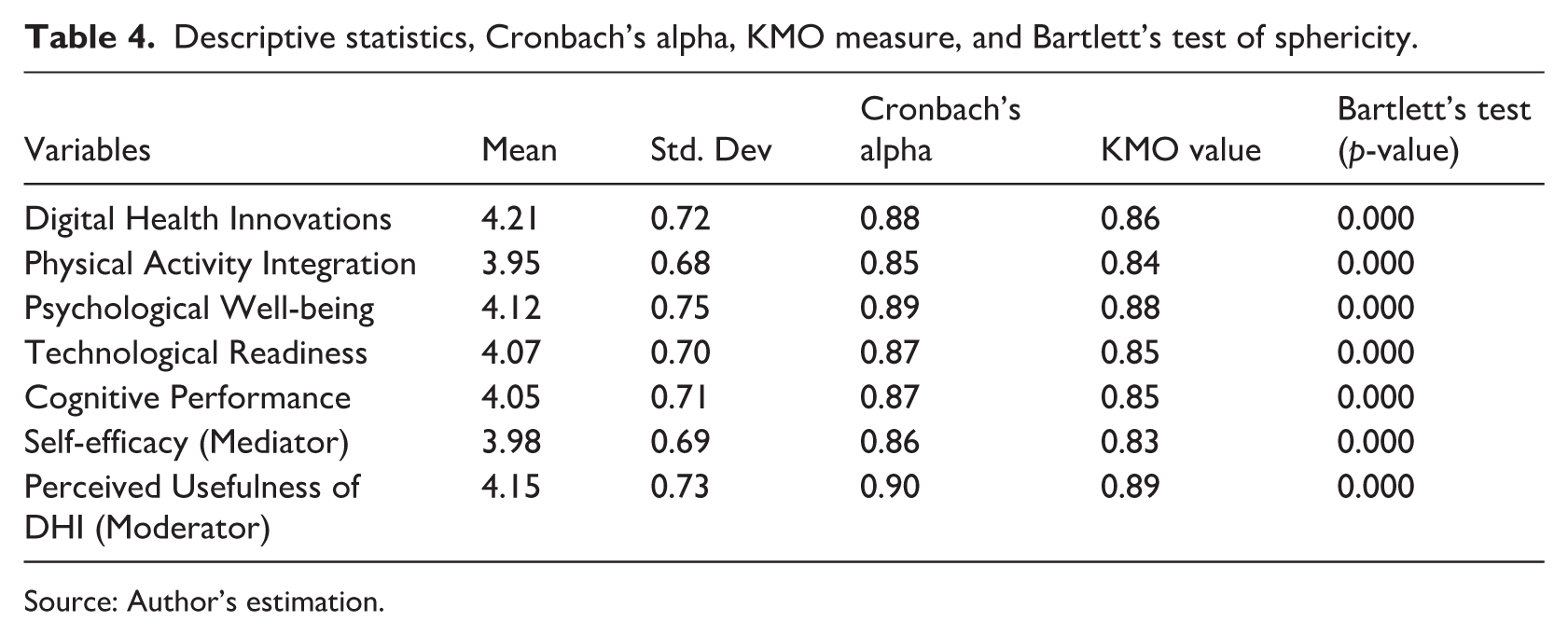
Source: Author’s estimation.
Cronbach alpha values of all constructs were above 0.80 and therefore the measurement scales were reliable. Most credible readiness indicator of digital health technology was Perceived Usefulness of DHI (α = 0.90). Cognitive performance (α = 0.87) and psychological wellbeing (α = 0.89) also exhibited good levels of reliability and physical activity integration scored 0.85 showing precision in measuring the construct in question. The factorability of the dataset Kaiser-Meyer-Olkin (KMO) values all its constructed factors, each having a value of over 0.80, which is much higher than the minimum set of 0.70. The KMO of the perceived Usefulness of DHI was undeniably the best (0.89), then digital health innovations (0.86), psychological wellbeing (0.88) and self-efficacy (0.83). The Test of Sphericity by Bartlett revealed that there is significant evidence of correlation contributes to factor analysis and made sure the matrices were fitting (p < 0.001).
The measurement model was confirmed by Principal Component Analysis (PCA) using varimax rotation (Table 5). The purpose of PCA was to guarantee latent structures and strong factor loadings. With the Kaiser criterion, eigenvalues above 1.0 were kept. Digital health innovations became the main element with an eigenvalue of 3.85 reflecting the 23.5% of variance proving the rising popularity of wearable products, mobile applications, and AI-operated technologies in the context of physical education and health. The second most significant factor was the integration of physical activity with an eigenvalue of 3.12% and 18.9% variance accounted probably. Items discrimination and loading of this construct were observed to range between 0.68 and 0.84 including the view of that the items successfully reflected the use of technology in the fitness program.
Principal component analysis (PCA) with Varimax rotation.
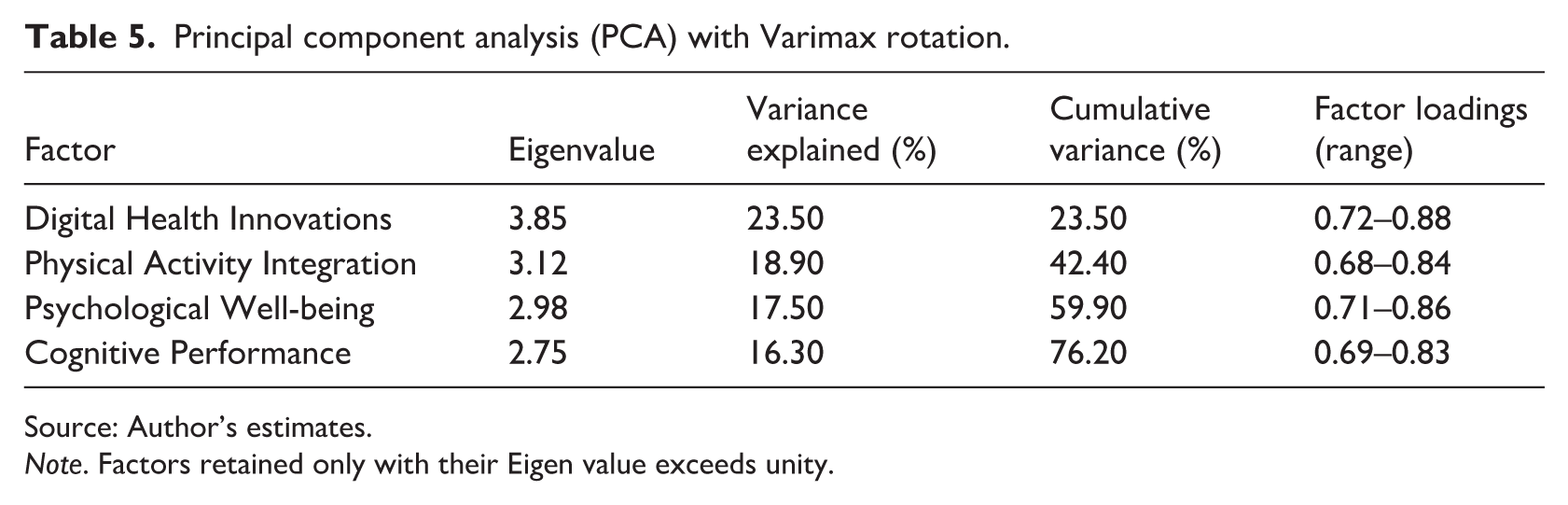
Source: Author’s estimates.
Note. Factors retained only with their Eigen value exceeds unity.
Psychological wellness is the third important component, with an eigenvalue of 2.98. This component explained 17.5% of the variance and 59.9% of the variation. The relatively high variance described by this component shows that digital health tools impact users’ mental and emotional well-being and physical activity. Factor loadings for this construct ranged from 0.71 to 0.86, indicating convergence. This shows that digital health experiences lower stress and boosts motivation. The fourth and final major component, cognitive performance, explained 16.3% of variation with an eigenvalue of 2.75, totaling 76.2%. This large cumulative variance indicates that the factor structure is durable and that the factors discovered account for a considerable portion of the dataset’s variability. The cognitive performance factor loadings (0.69–0.83) demonstrate a good link between the observable variables and the latent construct, validating its evaluation. All four retrieved factors explain 76.2% of the dataset’s variability, proving the factor model was appropriate. The primary factor loadings (range from 0.68 to 0.88), which reveal a well-defined structure with minimal cross-loadings, suggest that each component represents a different digital health interaction aspect. Varimax Rotation increases factor separation and constructs consistency, improving interpretability.
Table 6 shows the Confirmatory Factor Analysis (CFA) model fit indices to evaluate if the measurement model captures latent components. All indices exceed their cutoff values, proving the model matches the data. With a CFI of 0.934, greater than the specified threshold of 0.90, the proposed model explains the observed variables’ covariance structure.
Confirmatory factor analysis (CFA) model fit indices.
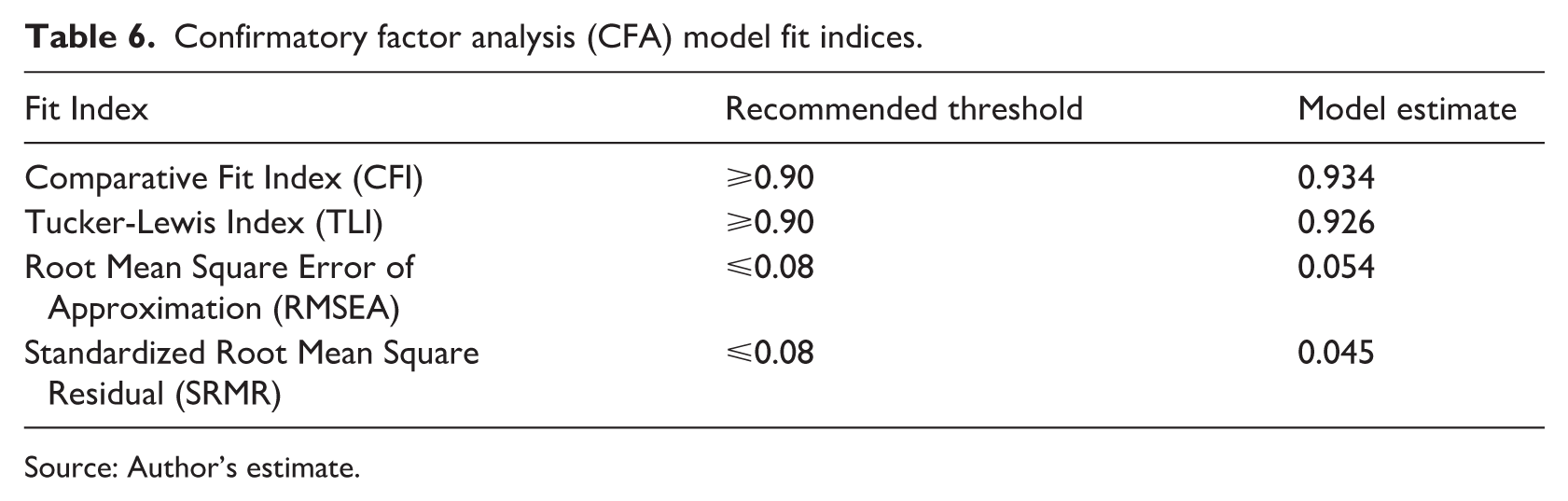
Source: Author’s estimate.
Tucker-Lewis Index (TLI), also known as the Non-Normed Fit Index (NNFI), shows that the model balances fit and parsimony, with 0.926 being its current value. The low RMSEA of 0.054, within the permitted range of <0.08, suggests no significant model misspecifications. The Standardized Root Mean Square Residual (SRMR) is 0.045, much below the standard requirement of 0.08, indicating minimal discrepancies between observed and anticipated correlations. These fit indices show that the CFA model is well-specified and captures the relationships between the study’s latent constructs.
Despite their widespread use and validation, the Cognitive Failures Questionnaire (CFQ), the General Self-Efficacy Scale (GSES), and the Technology Acceptance Model (TAM) have psychometric limitations. Since all evaluations are self-reported, response biases, such as social desirability or memory errors, may affect the findings. Even though their reliability has been proven to be high, the CFQ, GSES, and TAM scales may not be able to assess all aspects of people’s cognitive talents, self-confidence, and technology habits. To address these shortcomings, the study used confirmatory factor analysis (CFA) to assess the convergent and discriminant validity of all constructs. Fornell-Larcker criteria supported discriminant validity, whereas factor loadings and AVE values above 0.60 proved convergent validity for all constructs.
Table 7“s Fornell-Larcker criteria and HTMT ratio results demonstrate the study’s constructs” convergent and discriminant validity, ensuring the measurement model’s validity and reliability. Composite Reliability (CR) scores of 0.86–0.91 prove the structures’ internal consistency. These values are above Fornell and Larcker’s 0.70 thresholds. They are reliable because the constructs are internally coherent, and the indications used to evaluate each construct are closely related.
Fornell-Larcker criterion and HTMT ratio.
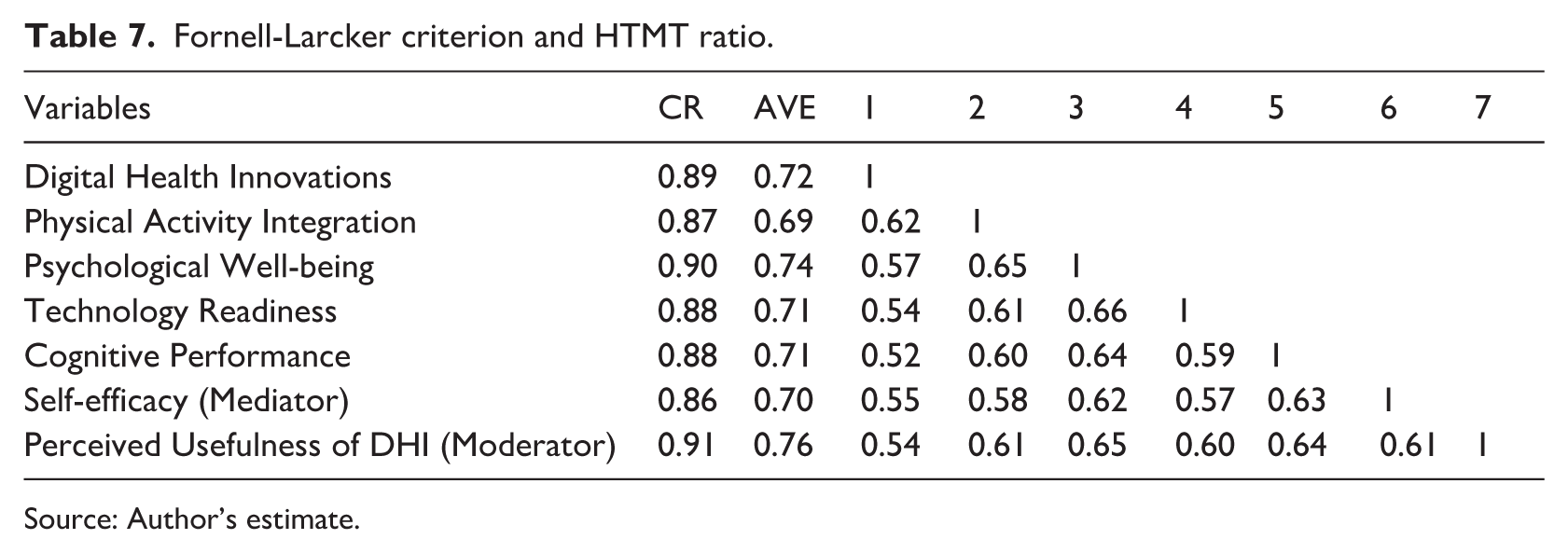
Source: Author’s estimate.
Convergent validity is supported by Average Variance Extracted (AVE) values over 0.50, between 0.69 and 0.76. The measuring approach is more resilient since each concept accounts for many variances in its indicators. Perceived Usefulness of DHI (AVE = 0.76) and psychological wellbeing (AVE = 0.74), which impact test results, had the largest variation. To assure discriminant validity, the Fornell-Larcker Criterion requires construct correlations to be less than or equal to their square root AVE. No multicollinearity or construct redundancy issues exist, and all Heterotrait-Monotrait (HTMT) ratios are below the conservative limit of 0.85, supporting discriminant validity. Psychological well-being and Perceived Usefulness of DHI are most correlated (0.65), showing a slight but positive association. The lowest inter-construct correlation of 0.52 shows that digital health innovations and cognitive performance capture different elements of digital health adoption and cognitive outcomes. The results demonstrate the measurement model’s discriminant and convergent validity and strong psychometric properties. The model’s internal coherence and ability to differentiate components make it suitable for structural equation modeling (SEM).
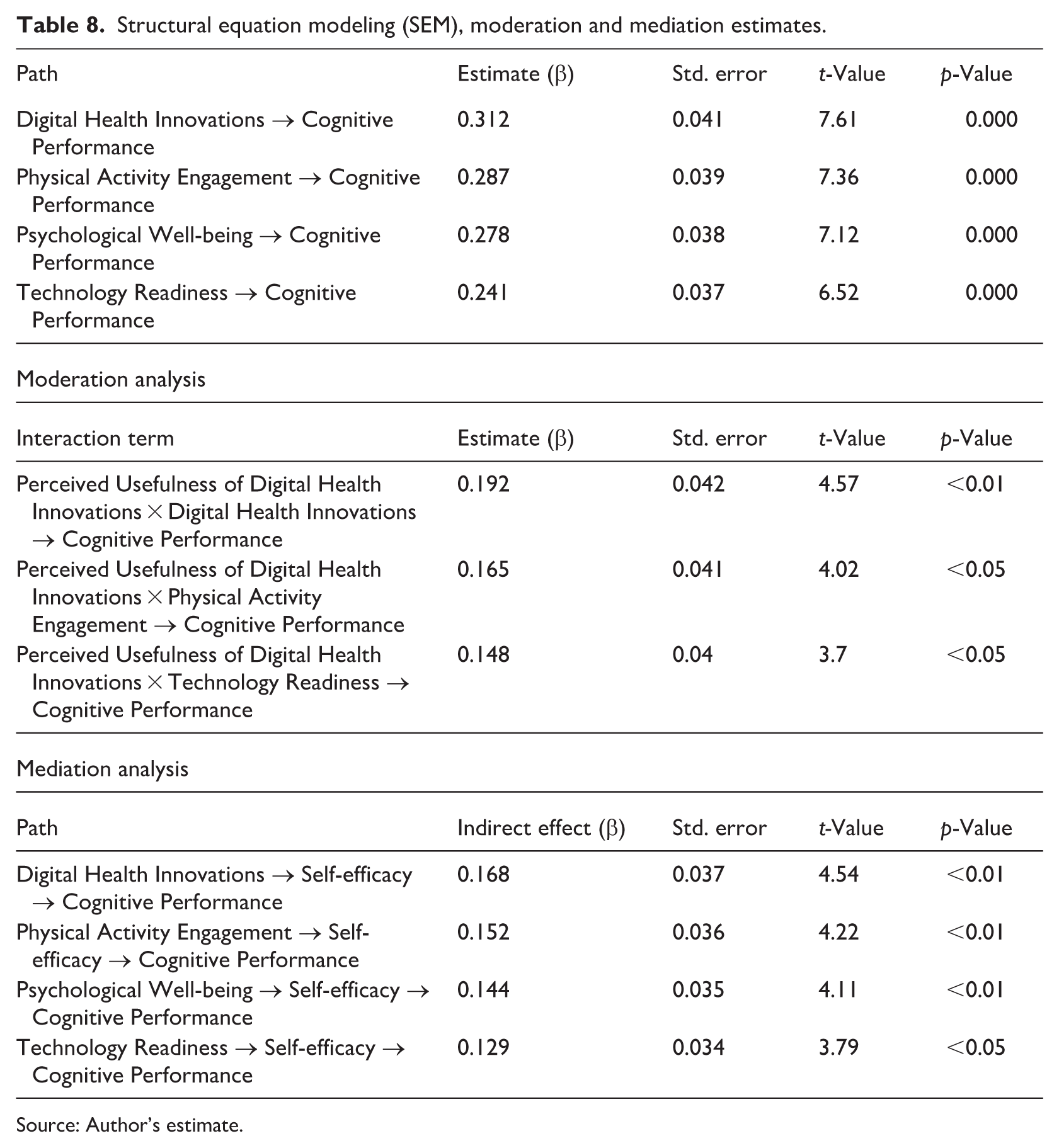
Table 8 shows the structural equations modeling (SEM), moderation and mediation estimates. The results show a positive correlation between digital health innovations and cognitive performance (β = 0.312, t = 7.61), indicating that increased use of digital health technologies significantly improves cognitive results. This supports earlier research that shows technology improves cognitive capacities, mainly via digital treatments that improve memory, mental agility, and executive functioning (Leung et al., 2022; Robledo-Castro et al., 2023). Technology acceptance and success improve users’ performance and cognitive abilities, according to the Technology Acceptance Model (TAM). According to cognitive load theory, digital health technologies enhance information processing and reduce cognitive overload, improving cognitive efficiency and higher-order thinking (Bahari, 2023). Empirical research shows that cognitive training applications, wearable health monitors, and AI-driven tailored health feedback improve cognitive adaptation (Onciul et al., 2025).
Structural equation modeling (SEM), moderation and mediation estimates.
Source: Author’s estimate.
Exercise has a good relation with cognitive ability since the correlation between cognitive ability and physical activity is significant (β = 0.287, t = 7.36). Motor coordination, cardiovascular stamina, and the capacity to efficiently utilize neural significance increases intellectual clearness, and physical education demonstrates these learning advantages in formalized sessions. The study provides support of exercise as a non-pharmacological treatment that prevents cognitive decline (Yorozuya et al., 2022). Cognitive performance (β = 0.278, t = 7.12) also depends on psychological well-being as emotional health benefits cognitive efficiency. The positive psychology states that decreased stress, chewing and resiliency increase cognitive flexibility, attentional control and the action of decisions. Individuals with balanced emotions have a quicker processing and executive functioning (Ma et al., 2023). According to self-determination theory, intrinsic motivation and cognitive engagement, retention, and problem-solving well-supported by psychological well-being will improve (Osei and Bjorklund, 2024). Mental health and mindfulness treatment of stress encouragement interventions are necessary to improve the mind. Cognitive performance has a positive relationship with technology readiness (β = 0.241, t = 6.52). As specified in the Diffusion of Advancements Theory, people with high levels of cognitive ability become more willing to adopt and utilize digital technologies (Norzelan et al., 2024). Knowledge on digital tools improves learning, addressing issues, and decision-making. Neurofeedback attitude novels, augmented reality education, and artificial intelligence-based training assist in the cognitive development (Piszcz et al., 2024). The findings show that virtual training platforms, performance-monitoring systems, mobile health applications, and wearable activity trackers are becoming increasingly important in the creation of physical education curricula. The emphasis on analytical and research-oriented involvement at the graduate level has increased the use of these technologies for skill development, self-monitoring, and personalized training. Digital health technology in physical education programs may increase students’ mental health, cognitive capacities, and physical training outcomes. The results suggest that curriculum designers should link technological tools with pedagogical aims to maximize digital health benefits for education and cognition.
According to the moderation analysis, Perceived Usefulness of DHI and the interactions with digital health innovations impact learning in a positive way (β = 0.192, t = 4.57, p < 0.01). This effect can be described by the Technology Acceptance Model because the perceived usefulness leads to improved cognition. This creates the necessity of digital health tools designed in a technologically efficient and friendly manner to maximize cognitive advantages. The connection between PU-DHI and physical activity engagement (β = 0.165, t = 4.02, p < 0.05) suggests that acknowledging the benefits of digital health innovations in encouraging physical activity enhances the cognitive benefits of exercise. According to the Self-Determination Theory (SDT), intrinsic motivation increases and individuals become more committed to the process and its consequences when they view their efforts as making a difference (Howard et al., 2021). Wearable fitness trackers, AI-guided workout regimens, and mobile-based health treatments promote physical activity and improve cognitive function. This discussion emphasizes the need for technology to monitor and optimize physical activity for cognitive function. When tech-savvy individuals see digital health advancements as favorable, cognitive benefits rise (PU-DHI × Technology Readiness, β = 0.148, t = 3.7, p < 0.05). This supports the Diffusion of Innovations Theory, which claims that individuals are more inclined to adopt and employ technological solutions they perceive to be advantageous. Digital cognitive training platforms improve memory, problem-solving, and adaptability. This is according to study on tech-savvy people who value digital health goods (Jeong and Nam, 2024).
Results of mediation analysis indicate that digital health tools improve cognitive performance by increasing self-efficacy, leading to an indirect effect. Cognitive training apps, telemedicine platforms, AI-assisted diagnostics, and other digital health therapies may enhance health and cognitive management trust. Self-efficacy increases continuous cognitive tasks, problem-solving, and adaptive learning, which may improve cognitive performance. Digital health developments have a direct and indirect effect on self-efficacy; thus, digital solutions must give tangible benefits and inspire confidence. Self-efficacy mediates the association between physical activity and cognitive performance, highlighting the psychological process of cognitive enhancement. According to research, daily physical activity improves brain function, and confidence in mental challenges (Caponnetto et al., 2021). When individuals feel they can exercise and keep it up, self-determination theory says their motivation to exercise and cognitive advantages grow. The significant mediation effect emphasizes the relevance of self-efficacy and cognitive performance interventions like physical exercise and psychological support. Higher psychological well-being correlates with stronger cognitive abilities due to increased self-efficacy, as confirmed by mediation analysis. A balanced psychological profile includes emotional stability, resilience, and stress management. Lowering cognitive load and enhancing attention control improve cognitive function. Study has connected strong self-efficacy to enhanced involvement in cognitive challenges, tenacity in problem-solving, and effective emotion control during complex cognitive processes(Rashid et al., 2024). This result underscores the necessity for comprehensive cognitive therapy with psychological support to improve self-efficacy and cognitive function. Finally, self-efficacy mediates the relationship between technology readiness and cognitive performance, indicating that tech-savvy individuals have better cognitive function due to increased self-confidence. This result supports the idea that self-efficacy is a critical psychological mechanism that turns technical knowledge into cognitive benefits (Kim and Lee, 2025). Explore innovative technology, digital learning experiences, and creative cognitive training methods to improve cognitive function.
Study limitation
Despite its strengths, the study has some limitations. First, since the research is cross-sectional, it cannot draw clear conclusions about the use of digital health technologies, self-efficacy, psychological well-being, and cognitive performance. Second, because the sample comprised only physical education majors, the findings may not apply to other fields. Third, self-reported survey results may be distorted despite measures to restrict pressure and ensure anonymity. Even though the study covered undergraduate, graduate, and doctoral/professional students, cultural, institutional, and geographical factors may limit generalizability outside the provinces tested. Different student groups, longitudinal designs, and objective performance or physiological assessments to augment self-reported data can help future studies address these limitations. Forth, since the sample includes students with access to digital devices and online platforms, the digital divide may introduce technical bias. Therefore, populations with less access to digital health solutions may not benefit. Fifth, model overfitting increases the likelihood that predicted linkages will be less robust when using complex Structural Equation Modeling (SEM) with a homogeneous sample. SEM allows the simultaneous examination of several correlations; thus, causation should be assigned with caution. Future studies could consider utilizing additional samples and methodologies to increase model generalizability and reliability.
Conclusions and policy recommendations
The research has shown that technological preparedness, psychological wellbeing, physical activity, and digital health innovation have a great impact on cognitive performance. According to moderation analysis, perceived usefulness, physical activity, and technological readiness enhance the correlation existing between digital health innovations and cognition. The use of mediation shows that self-efficacy also translates into cognitive performance and digital health innovations, psychological wellbeing, physical activity, and technological readiness with statistically significant indirect effects.
These results imply a number of policy implications. The policymakers must enable digital health technology in logic and strategy in learning activities by providing access in academic, care and business pieces. Digital application must promote individualized cognitive, mental-health, and exercise-coaching and achieve ethical standards, privacy levels, and quality. The cooperation between the academic community, medical organizations, and technology firms can lead to the creation of successful digital medications. There should be awareness creation on the use of digital health technology in cognitive functioning among the age groups and occupations, through campaigns. The brain functionality, neuro-productivity improvement, and health results should be attained through technology-based academic curricula (app-based) cognitive practice and company-sponsored wellness programs. Self-efficacy offered by policy should be advanced as well as mental health programs that incorporate digital health to vulnerable groups including students and seniors. Technological preparedness is initiable by public-private partnerships that are designed to maintain equity, provide balanced participation, and digital frontiers to access.
Although the study’s cross-sectional design and self-reported measures limit causal inference about cognitive outcomes, the findings clearly reveal features of cognitive performance.
Footnotes
Ethical considerations
This study protocol was reviewed and approved by the Ethical Committee of Henan University in accordance with the Declaration of Helsinki (Approval No: HU-REC/2023/1125). All participant data were collected anonymously, and no identifiable personal information was obtained.
Consent to participate
Participation in the survey was entirely voluntary. Informed consent was implied through completion of the questionnaire.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data.
Author contributions
Jichun Xie designed the study, conducted the survey, collected the data, and performed the statistical analysis. He also prepared the first draft of the manuscript and contributed to subsequent revisions. Ruilin Xu supervised the overall research process, validated the data and analytical procedures, and provided critical revisions to improve the quality and clarity of the manuscript. Both authors reviewed and approved the final version of the manuscript prior to submission.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the 2024 Annual Project of the Philosophy and Social Sciences Planning of Henan Province (2024BTY024) and the Graduate Education Research Project of Zhengzhou University (YJSJY202327).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data will be made available upon reasonable request.*