
Abstract
This article investigates how the practice of drinking kombe (drinking washed off Qur’anic verses) informs subjectivities in the nexus of ‘religion’, ‘medicine’ and their Swahili approximations dini and dawa. Situated in Zanzibar, it is mostly referred to as dawa ya kiislamu, bringing ‘medicine’ and ‘religion’ together and providing space for multiple enactments of subjectivities. Most prominently, Christians’ use of kombe requests a different engagement with kombe and accentuates the ambiguity of drinking kombe as an embodiment of Islamic scripture conveyed by Islamic connotations of the Qur’an that heals, on the one hand, and drinking kombe as treatment irrespective of ‘religious’ affiliation, on the other. This becomes particularly pertinent in the discourse justifying drinking the Qur’an against anticipated criticism. These justifications enable the practice of drinking kombe to reveal different implications for the formation and cultivation of subjectivities with respect to the flexible ground of enacting dawa ya kiislamu.
Bi Mwaltima, a middle-aged female healer, works in a dispensary of mainly herbal treatments that I regularly visited in Zanzibar Town. During one such visit in 2014, we were engaged in exchanging the latest personal news when we passed the dispensary’s courtyard, in which buckets with kombe – Qurʾanic verses written with saffron ink and dissolved in water to be drunk for medicinal purposes – are stored (see Figure 1). I did not see the familiar transparent buckets so I asked her about them. She opened one of the other buckets and pointed out that kombe was in there. We both looked inside and saw a liquid, but because the bucket was not transparent it was impossible to determine the colour. To prove that it was kombe, Bi Mwaltima bailed out a little with a white cup and I recognized the characteristically pink colour of kombe. I confirmed that now I certainly could see that this was kombe and Bi Mwaltima, instead of pouring it back, nonchalantly set the cup to her mouth, drank the liquid and continued the conversation.

Buckets of kombe in the dispensary’s courtyard, Amani, Zanzibar Town, March 2014. © Photograph: Hanna Nieber.
What does this seemingly mundane event reveal about how kombe is drunk and the people who drink it in Zanzibar? How can a study of kombe be used as an entry point to understand the formation of religious subjectivities? How does Bi Mwaltima’s being Muslim relate to the framing of kombe as treatment? How do the English words ‘religion’ and ‘medicine’ relate to their Swahili approximations dini and dawa and how do the gaps of their correspondences matter when negotiating and justifying subjectivities? A focus on the body and its interaction with the material world through particular practices informs this contribution. To study subjectivity in terms of the body in society involves grounding oneself in manifold developments within social and cultural anthropology. 1 Questioning the primacy of meaning in the humanities (Geertz, 1993[1973]) was crucial for the wide reception of an understanding that subjects ‘have’ and ‘are’ bodies (Merleau-Ponty, 2012) and that the relationships between people who have and are bodies form practices – or a habitus, to use Bourdieu’s term (for example, 1977) – that take part in shaping ‘religious’ subjects (Asad, 1993; see also McGuire, 1990). There is a distinction between verbalized and procedural knowledge and while the first pertains to discourse, the second refers to bodily practices that may not be easily identifiable as ‘religious’. In this article, via a study of drinking kombe (a practice of ‘religious’ healing), I explore how the conceptual boundaries between ‘religion’ and ‘medicine’ as distinct domains of knowledge and practice become blurred. I further trace how in this case practice and discursive rationale are entangled in specific co-relations to the effect that these categorizations matter, despite the blurred boundaries.
The correspondence of a certain kind of subjectivity with its practices is often taken for granted. However, as this article aims to show, subjectivities do not develop from an easy co-relation of the procedural and the discursive or the bodily and the material. This correspondence relies on processes of doing, and may arise after much tension and (mis)alignment. The practice of drinking the Qurʾan, often glossed as dawa ya kiislamu (Islamic medicine), must be ‘made to matter’ – as my interlocutors in Zanzibar do – by relating it to certain types of subjectivities, some of which become pertinent vis-à-vis anticipated verbalized and doctrinal criticisms.
Although the practice of drinking the Qurʾanic liquid kombe (a more detailed description follows below) is widely spread around the Islamicate world, in most academic literature that mentions it, it merely appears as an incidental remark rather than as a topic that bears potential to be investigated in its own right, 2 as Katharina Wilkens (2013: 243–244) has observed and explained in terms of disciplinary foci. She herself has analysed kombe using the methods of comparative religious studies. Wilkens (2011) shows the spatial juxtaposition to Marian faith healing practices in Dar es Salaam and highlights the comparability to medieval Christian practices of swallowing the Madonna (Wilkens, 2013). An earlier study, and widely perceived, is El-Tom’s article (1985) on the phenomenon that he terms ‘erasure’. He focuses on the relation between the written verse and the affliction for which it is taken amongst the Berti in Sudan. Annemarie Schimmel (1994) approaches the topic briefly through the perspective of Sufism. Travis Zadeh (2008a, 2008b, 2009, 2014) takes a historical perspective and traces early theological contestations and justifications of drinking the Qurʾan in the area of what is today Iran, and Eleanor Abdella Doumato (2000) and Joyce Burkhalter Flueckiger (2006) describe how the Qurʾan was and is drunk in Saudi Arabia and Hyderabad, India, respectively. The most prominent engagement with kombe in the Swahili context is Allyson Purpura’s PhD (1997) thesis, in which she situates kombe within the context of knowledge configurations in Islamic Zanzibar over history. More recently, Janet McIntosh (2009) has mentioned kombe in her work on the Giriama and their relationships with the Swahili. These scarce exceptions to the otherwise non-existent engagement with kombe in academic literature are highly informative about the practice’s embeddedness in larger temporal and spatial frameworks. While some of these authors note that kombe is part of a medical pluralism that is employed by all kinds of people, including non-Muslims, these studies do not engage with the question of how drinking the Qurʾan as ‘Islamic medicine’ affects people’s negotiations of who they are and become by drinking kombe. Despite a quite literal embodiment of the Qurʾan, little has been written about how drinking the Qurʾan influences engagement with subjectivities in the nexus of ‘religion’, dini and dawa.
I conducted ethnographic fieldwork for 13 months between 2013 and 2015 on drinking kombe in Zanzibar Town. In my research, I traced the practices related to the preparation and consumption of kombe in Zanzibar mainly through participant observation and followed discourses of its permissibility in interviews conducted in Swahili. I examined its materiality and engaged with its contextual situatedness: kombe is framed as dawa ya kiislamu (Islamic medicine) in Zanzibar, an island group situated in the Indian Ocean just off the Tanzanian mainland to which it politically belongs. With a population of predominantly Muslims of the Sunni Shafiʿi school and historical ties to Oman, Zanzibar’s connection to the Indian Ocean world is vibrant and continuously shapes an awareness of regional embeddedness (see Figure 2). Groups of Ibadhi, Shiʿi and Wahhabi-influenced Muslims, Roman Catholic, Anglican and various Pentecostal Christians, as well as Hindus form a numerical minority. With these people the awareness of regional entrenchment is strengthened. 3 Furthermore, ascribed or actual descent from Persia, ‘Arabia’, the East African mainland, Goa, or Gujarat not only plays an important role for Zanzibar’s social order, but also amplifies positive value judgement of belonging to the Indian Ocean region and distinction from the African mainland.

Map of part of the Indian Ocean region showing areas to which people in Zanzibar ascribe their origins. © OpenStreetMap contributors, openstreetmap.org.
The ascription of kombe as dawa ya kiislamu (Islamic medicine) and the concomitant categorization of drinking kombe as a practice of dini (‘religion’) and dawa (‘medicine’) resonates with Zanzibar’s situatedness as part of the Tanzanian state but, unlike the Tanzanian mainland, with a dominant Muslim majority oriented toward the Indian Ocean. Drinking kombe and talking about drinking kombe give rise to tensions between practices that are easily claimed to belong to the ‘religious’ realm and their enactment in a ‘medical’ realm. The consequential differences in the subjectivities formed through this practice (in terms of its attribution to dini/‘religion’ and/or dawa/‘medicine’) matter for a discursively expressed desire to conciliate these differences and portray coherent subjectivities.
According to Hakimu Saleh (2013, personal communication), who describes himself as an Islamic healer and is visited by patients from across Zanzibar to receive spiritual guidance and medication, ‘medicine’ usually refers to something that is practised in the governmental hospital and is attuned to the visible body. 4 Dawa, he says, is more inclusive and, in addition, involves treatment in the realm of the unseen or the ‘spiritual’. Dini, he states, encompasses the realm in which God acts, so everything can be attributed to dini, including dawa. Hakimu Saleh explains that the Western concept of ‘religion’ includes a multiplicity of different religions. He cannot reconcile this concept of religion with Islam since Islam is not one religion amongst others but, for him, the only singular and all-encompassing dini. He thus uses ‘dini’ and ‘Islam’ interchangeably. 5
Farouk Topan (2009) states that dini is conventionally explained in juxtaposition to mila (customs) whereby the separation between ‘Islamic’ and ‘African’ practices is stressed. I agree with Kjersti Larsen’s (2009) critique of it in which she observes that rather than being dichotomized, dini and mila need to be understood by what they share: frameworks to preserve the well-being of the individual and of the community. Dawa – ‘medicine, in the broadest sense of the word’ (Langwick, 2011: 41) – is part of dini: it is part of preserving well-being. In contrast to ‘medicine’, it does not carry an exclusively positive connotation, but is also used for substances that poison (see also Wilkens, 2011: 180) and hence could be thought of as encompassing a wide range of ‘potent’ substances. Most importantly, dawa includes measures against afflictions that biomedicine 6 does not see, such as problems with spirits. According to Walter Bruchhausen (2006), the two terms ‘religion’ and ‘medicine’ and, in particular, their separability from each other are intimately tied to particular Western developments. Bruchhausen glosses these developments as secularizing and institutionalizing processes (p. 482). He thus sees these two terms as unfit to describe African healing phenomena. 7 Although the terms dini and dawa might not be easily translatable to ‘religion’ and ‘medicine’, my fieldwork, in contrast to Bruchhausen’s rejection of the terms, suggests that the separability of the Western concepts and the inseparability of the Swahili-language concepts interact in contemporary Zanzibar. The correspondence of dini with ‘religion’ and of dawa with ‘medicine’ and the gaps of these correspondences matter in particular when negotiating and justifying subjectivities, as I will show here.
In this article, I proceed to explore both the preparation and the drinking of kombe as specific material processes. I then describe how kombe is perceived by different people to act on patients’ bodies and on their emplacement in Zanzibar. The distinctions and connections between the domains of dini, dawa, ‘religion’, and (less so) ‘medicine’ take shape in relation to practices of people as subjects that have bodies and are bodies (Hardon and Posel, 2014; McGuire, 1990) that can ingest Islamic scripture. These conceptual distinctions become pertinent when Christians’ use of kombe (of drinking the Qurʾan) is scrutinized. The multiplicity of how drinking kombe relates to the subjectivities of those who ingest it is opposed to a more rigid discourse that strives towards a coherent narrative. I argue that, by utilizing the relations between dini, dawa, ‘religion’ and ‘medicine’, the kombe drinkers’ engagement with anticipated contestations fundamentally invokes the ambiguous nature of subjectivity. It serves to complicate the attribution of practices as markers of a particular kind of subjectivity and also shows how contestations are embedded in entangled 8 notions of multiplicity and its perceived ‘gaps’.
Kombe in its materiality
Paper/plate and ink
When kombe is prepared, the paper or ceramic plate on which Qurʾanic verses are written must be plain: neither lines nor floral designs nor anything else may interfere with the plainness of the paper or plate. Often the good quality of old Chinese porcelain that had arrived in Zanzibar through prosperous trade relations across the Indian Ocean is stressed in contrast to today’s more easily available plastic plates (also from China). Although the ceramic plates used today are mostly not antique, they evoke a connection to a glorified past. On these plates, or on plain paper, the verses are written with zafarani (saffron) used as ink (see Figure 3). Although mostly food colouring imported from India is used, naming it zafarani when bought and used for the purpose of preparing kombe attaches worth to the ink and refers to saffron’s healing properties. 9 In his study of the Masowe apostolics who reject material things as hindrances to the relationship with God, Matthew Engelke (2005) draws attention to different degrees and kinds of materiality and, in doing so, refers to Miller’s (2005) conceptualizations of the relativity of materiality. The plate (or paper) and the saffron ink matter; their materiality is given value by commenting on certain specificities (plainness, value) and their importance for the preparation of kombe. Other materials receive less attention since they matter differently.

A plate with Qurʾanic verses ready to be washed off (Amani, Zanzibar Town, January 2014). © Photograph: Hanna Nieber.
In order to write kombe, Hassan, Abdul or Tufa, all of whom work with Bi Mwaltima and are considered fit for this task, take the plate and put it on their laps. While Hassan usually opens the Qurʾan (at random), Tufa uses a book in which the verses are ordered according to affliction; to Abdul, the verses come as inspiration. After taking a sharpened twig, the size of a pencil, into their right hands (all of them are right-handed) and steadying the plate with their left hands, they dip the twig into the ink in a cup that is regularly refilled for this purpose. Sometimes they adjust their sitting position and move the cup with the ink so that they can comfortably reach both the plate and the cup with their right hand. The chosen verses are then written while the hand moves along the lines and constantly goes back to the cup to ensure the twig carries enough ink. After the writing is finished, the twig is left in the cup with the remaining ink to be used by the next person. With both hands, the plate is picked up from the lap and given to somebody else either to hold it for a second while the books are stored away or to wash the verses off.
Water
Washing off the verses is a decisive moment for the preparation of kombe. The water that is used to contain the verses is mostly non-descript or described as neutral. Occasionally, the preference for zamzam (water from the spring at the Kaaba) is articulated but, as it is difficult to obtain, the use of rainwater (which must not have touched anything else before) is suggested. Mostly, however, tap water or water from the nearest well is used and with this water the previously written verses are washed off. 10 Despite recommendations for differentiating various kinds of water, in practice, water’s neutrality matters, allowing for the use of unspecified (though not polluted) water. In the context of religious healing, water’s neutrality is often invoked as it then becomes ‘chargeable’. Wilkens’ (2011: 75) study on Marian faith healing in Dar es Salaam describes the ‘water service’ in which patients are showered with blessed water mostly to exorcise spirits. She comments on the convenience of blessed water being easily perpetuated, as a small amount of blessed water can be multiplied by adding more – neutral – water and certain prayers. In a different manner, Engelke (2005: 134) also stresses water’s neutrality. As different people imbue water with different meanings and as water is ubiquitous, it has acquired a neutrality which for the Masowe apostolics gives it a different material quality. In the case of kombe, water is a neutral carrier that can contain Qurʾanic verses with all their power and carry it to the afflicted body. Its neutrality protects the verses and leans water towards the immaterial.
The water containing these verses is filled into bottles to be given to the patients (see Figure 4). The bottles are either brought by the patients themselves or supplied by the practitioners. Unless they have contained something alcoholic, the bottles do not matter much. This chain of practices involving different material entities with their traces forms the ‘practice bundle’ of preparing kombe. Depending on the context, the practitioner’s body and the room of preparation also receive attention, being protected in specific ways, or, in other contexts, left as unimportant.
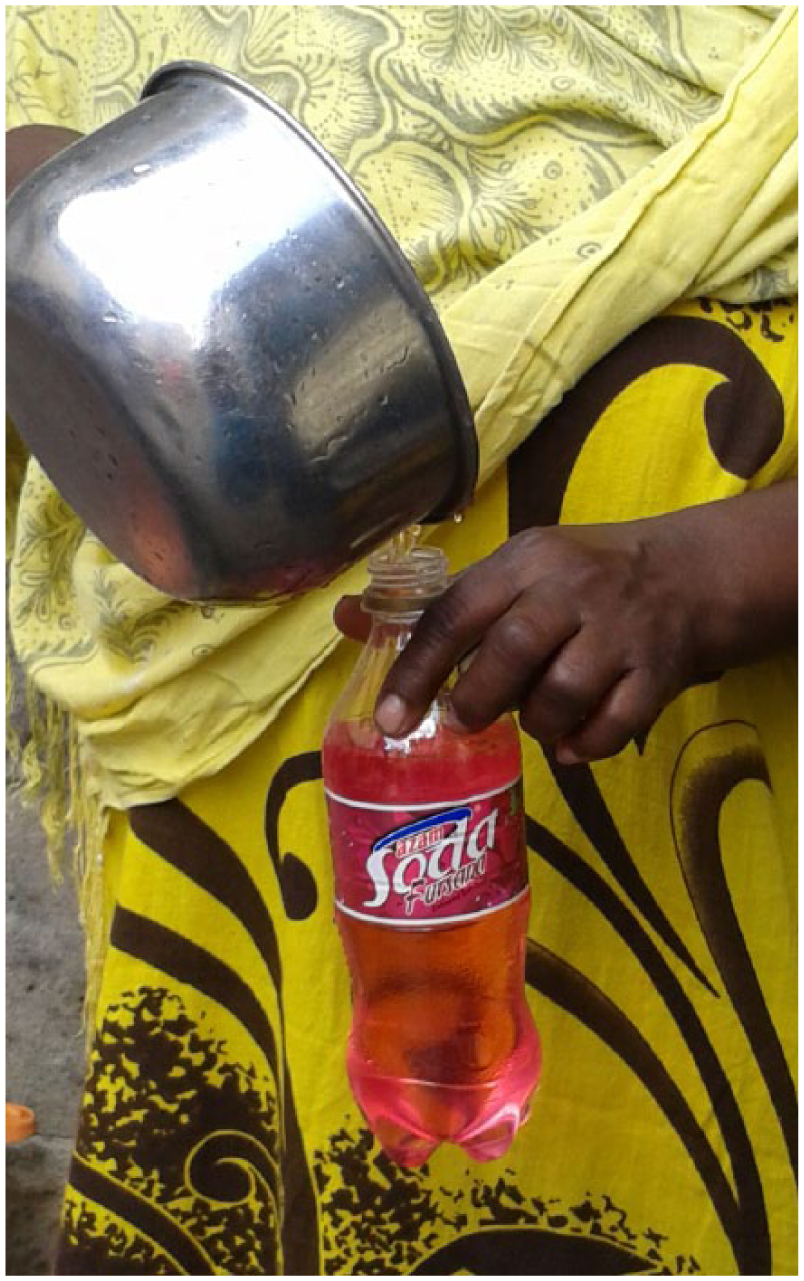
A bottle being filled with kombe to be given to a patient, Amani, Zanzibar Town, August 2014. © Photograph: Hanna Nieber.
As Miller (2005) posited, some things are more material than others. The plate, the ink, the water and the bottle all matter to different degrees. We now turn towards the verses, the materiality of which is given much weight.
Qurʾanic verses
The procedure of choosing the appropriate Qurʾanic verses (and possibly supplements such as praise particles, names of protective jinn, or the Solomonic Seal) 11 depends on the person who is doing the writing. Some practitioners make an array of calculations to ground these decisions, for instance, Hakimu Saleh does this while others such as Bi Tufa look up the affliction in a separate book that matches afflictions to appropriate verses. Still others, such as Abdul, use their inspiration from God and, for others, the choice of verses does not matter as any verse of the Qurʾan can provide healing.
The preparation of kombe entails the transmission of these Qurʾanic verses from a msahafu (a physical codex of the Qurʾan) to a liquefied drinkable version. The msahafu (material ink in a particular form on paper, as God’s word equipped with specific rules denoting its handling) is read and copied by the practitioners. The practitioners need to ensure that the forms they draw resemble those of the printed version and keep their characteristics so that the zafarani text remains the same text as in the msahafu, and thus constitutes the Qurʾan. As Stacy Langwick (2011: 98) points out: ‘Writing kombe … does not require literacy in Arabic’ but at least in Zanzibar Town it does require the ability to carefully copy the forms of the Arabic letters. Once the zafarani has been dissolved in the water, however, it loses the form that defined the letters and made it readable with the eyes. It loses its form, but not its empowering Qurʾanic content. The power of the Qurʾan persists, even though the text may not be readable with the eyes anymore.
Karen Barber (2007: 212) points out that texts are embedded and entangled in the material world: ‘Though all texts are made to be iterable and detachable from context, they are also ambiguously bound up in context.’ Barber, whose understanding of text goes beyond written words and includes orality, pays attention to texts’ relations to the situation of their occurrences. With scripture, the question of its materiality leads to the celebration, the acceptance, or the repudiation of particular practices in this material world and thus to the enactment of scripture. The Christians who don’t read the Bible (Engelke, 2009), for example, mark the importance of immateriality through practices in the material world whereby ‘materiality is a matter of degree and kind’ (p. 136). 12 Of course, the Bible as the Protestant’s scripture is inherently different from the Qurʾan as the Muslim’s scripture, not least because the Protestant understanding of the Bible that foregrounds meaning differs completely from Muslims’ dedication to the material Qurʾan as the presence of God’s word. Nevertheless, the question of the materiality of scripture matters in particular with the justifications of drinking kombe, as will be explored below.
The Qurʾan is more than written text. 13 As God’s word it is held to go beyond its existence as a written text and a dissolution of the written letters transforms this particular substantiation of the Qurʾan but does not destroy it. Once given a material existence in writing (or in recitation, but this is not the focus of this article), its form can be changed into a liquid or into smoke (see Flueckiger, 2006): its physical properties can be altered. The transformation of the written Qurʾanic verses into a liquid – a liquid that carries the ink that had formed the determinative letters – renders the Qurʾan’s healing properties accessible to the body.
Ingestion
After kombe is written, washed off, filled into a bottle, stored, sold and transported, it finally needs to be drunk by the patient – it needs to be ingested to unfold its Qurʾanic healing properties inside the body. The bodies that people are and have (McGuire, 1990) become the material form in which healing through the Qurʾan takes place. In accordance with the range of ways in which the verses are chosen and how kombe is prepared, the practice of drinking kombe equally differs amongst the patients. The case of Mama Sue and her new-born baby Tarnim will serve as an example here before I continue to inquire into the relation between the ingestible Qurʾan and the body.
Mama Sue, her husband and two children form a not particularly pious Muslim family and occupy one of the rooms of the shared flat that I was also living in for two months. She gave birth to her third child in the period that I was there and I accompanied her to see a healing practitioner when she had the feeling that her new-born child Tarnim was not well. She chose to visit yule bibi (‘that woman’) who had helped her before and who was known to treat conditions that others, in particular biomedical practitioners, might not notice. Sleeping difficulties are among the afflictions that might not be visually detectable in the body. The 40 days of staying at home with the child that most Muslim mothers try to (and are expected to) observe had not yet passed. Next to concerns for her new-born baby, the visit to the healing practitioner was also a welcome diversion from her household chores. Baba Sue, who drove us to the practitioner, negotiated a better position in the waiting line and then resorted to waiting outside. Unlike the few other visitors, who clutched documents from previous visits to other medical places, Mama Sue held nothing in her hands except her baby; I was carrying her handbag in which she had additional cloths for the baby as well as her purse and phone. When it was our turn, the practitioner touched Tarnim’s stomach and diagnosed ‘gas’ (flatulence). Since Tarnim was too small to directly drink anything but breast milk, Mama Sue was to drink the prescribed dawa (‘medicine’) and thereby pass on its quality via her breast milk. Along with some wooden sticks to be simmered in boiling water and later cooled and drunk, Mama Sue was also given kombe. She had brought an empty bottle which was filled with kombe that had been written and kept in stock beforehand. Both the decoction and the kombe were to be drunk by Mama Sue regularly and thus passed on to Tarnim: one small tea cup in the morning and one in the evening for seven days. 14 On our way home, Mama Sue used the opportunity of being in a car and asked Baba Sue to stop twice in order to do some shopping. Whereas Tarnim had been sleeping on our way to the practitioner, she grew hungry on our way back. At home, Tarnim was breastfed and we started cooking. The water with the wooden sticks was put on the charcoal grill just after the food was ready. After eating, Mama Sue drank her medicine: both the decoction, which was very bitter and therefore had to be gulped down quickly, and the cup of kombe, which fortunately did not taste bitter but rather non-descript – like water. She went to bed early that day. Although the bottle of kombe was meant to last for seven days, it was already empty after three. Mama Sue noticed this with indifference and a day later decided to also stop drinking the decoction. Although she continued to complain about her difficult situation with Tarnim who continued to have ‘gas’ and therefore wouldn’t sleep peacefully, she evaluated the treatment she received as successful and went back to the practitioner irregularly to receive more treatment (based on my field notes, 2013).
Of course, this account of how Mama Sue drank kombe cannot be generalized – others might portion the bottle more carefully to last for seven days, or they might say ‘bismillahi’ in praise of God before swallowing kombe. But the account of how Mama Sue took kombe is not exceptional and offers an appreciation of how kombe can be drunk as part of a treatment ya asili (‘original’/‘traditional’). 15 Mama Sue’s way of ingesting the Qurʾan was not framed as ‘religious’ and was not incorporated in a practice bundle that would render it as part of practising this ‘religion’. For her, kombe and the decoction belonged together as they were received together from yule bibi, the practitioner that she chose in order to receive treatment ya asili. Furthermore, they were prescribed for the same time span and the early finishing of the bottle of kombe prompted her to also finish the treatment with the decoction a day later. The bitter taste of the decoction and the smell that pervaded the kitchen cannot be discounted in making it unpalatable for Mama Sue. (She also needed the pot in which the decoction was prepared for the daily preparation of meals.) With some hesitation, Mama Sue evaluated treatment with the decoction to be only effective with the accompanying ingestion of kombe. Co-occurring with the decoction, the transformed Qurʾan is made to unfold its healing effect in the body. Mama Sue received the decoction as dawa ya asili (‘traditional medicine’) and kombe as dawa ya kiislamu (‘Islamic medicine’) and, although each has an independent rationale as to how it works, Mama Sue treated them as having a relation of dependency: they are both dawa, but the efficacy of dawa ya asili is dependent on the dawa ya kiislamu. Here, the dawa ya kiislamu is coupled with the sense of dini that is encompassing, relevant for all aspects of life, and includes the realm of all dawa. Mama Sue joins the drinking of the two liquids, each imbibing particular healing qualities and each constituting a specific type of dawa, into one practice bundle. She thereby renders her drinking holistic in the sense of dini without incorporating it in practice bundles of ‘religion’ and thereby without marking it as ‘religious’. Thus, drinking kombe in this case is part of the formation and cultivation of Mama Sue’s (and Tarnim’s) ‘medical subjectivities’ in a holistic sense influenced by dini, and very concretely substantiated to fight affliction in and through the body.
Bodily practice
Specified as dawa ya kiislamu, drinking kombe co-exists with many other curing options that an afflicted person in Zanzibar can choose from – biomedicine, Chinese medicine or, as in Mama Sue’s case, ‘traditional’ (ya asili or ya kienyeji) medicine – that are often combined with kombe. The body concepts that are mobilized through these different medicines are, in various combinations and degrees, also taken to the kombe practitioners’ places (i.e. X-ray pictures brought to the kombe practitioner’s healing room). Equally, the body containing the Qurʾan travels to other medical settings: the body containing and reacting to the Qurʾan is at the same time the body that in the governmental hospital can be depicted in X-ray or ultrasound images, consisting of bones, blood vessels and organs. It is the same body that gets hungry and tired, that gets dressed, veiled, that enters public transport and carries children, that prostrates itself during prayers, that potentially is the seat of a spirit, that hurts, and so on. It is the same body differently enacted in the different instances. Warnier (2001) makes a related point when he stresses that the body and its material surroundings can never be separated and that sensori-motor culture is ‘propped’ by its interactions with material culture. This body in its various facets is the body that the subject is and has – and ‘not a seamless whole’ (Hardon and Posel, 2012: S6). As Annemarie Mol (2002: viii) puts it, ‘the body is “multiple” … In practice, the body and its diseases are more than one, but this does not mean that they are fragmented into being many.’
The ingestion of kombe into this ‘body multiple’ incorporates the materiality of the Qurʾan into the body. It acts affectively on the patients to counter affliction, which varies depending on the person and situation, but this multiplicity manifests in the one body. A stomach ache, for example, occurs in the body that is a biomedical body with a stomach that reacts to bad food. Simultaneously, the stomach ache occurs in a body through which jealousy materializes as affliction and in a body that is taken care of to be reproductive. Despite the differences in the interpretations of why certain symptoms appear, the body is not fragmented, but rather a body in, through, and to which afflictions occur and in, through, and to which treatment practices are directed. Kombe caters to this multiplicity by being instilled into this body multiple without fragmenting it. The body that people are and have is the body through which religious subjectivity is lived. Instilling it with kombe, however, does not necessarily render drinking kombe a ‘religious’ practice. Furthermore, this simultaneity of the body’s unity and multiplicity provides room for questioning, possibly resolving, or allowing for ambiguities of how kombe’s efficacy is influenced by a subject being and having a ‘body multiple’.
In Swahili, the body is mostly referred to as mwili. Mwili is the living body that is ‘visible with the eyes’. The Islamic healer Hakimu Saleh further illustrated that mwili is that which can ‘undergo operations in the governmental hospital’.
16
Mwili is entangled with nafsi (‘self’/soul), roho (spirit/soul), moyo (heart), akili (mind/intellect) and tumbo (stomach) (Hakimu Saleh, 2014, personal communication; see also Kraska-Szlenk, 2014: 99–107). When kombe is drunk, the Qurʾan is made part of this mwili, and this means that the Qurʾanic text is quite literally embodied (see also Ware, 2014). Talib Ali, who is a scholar on Islamic matters in Mombasa, Zanzibar, heard about my research about kombe and offered to be an interview partner for me. Responding to my inquiry about how kombe unfolds in the body, he argued that while kombe enters the stomach and travels from there, it can only be effective if the heart has embraced it prior to the material ingestion:
When you drink this medicine [kombe], it passes here [points to the stomach]. It passes through the stomach, right? And then it circulates. But before that, you know, the afflicted person has an imani (belief/faith/trust) – which belief? The belief that it will help them. So, the information was already given to them. It is already in the heart and has started circulating before it reaches the stomach. (Talib Ali, 2014, personal communication)
For Talib Ali, the heart’s belief and trust are constitutive for the unfolding and efficacy of the embodied Qurʾan to work against affliction. When seen in this light, drinking kombe could be understood as a practice that presupposes and requires a body with a heart in which belief/trust in the Qurʾan’s efficacy are situated – a heart that understands. Jacques Mercier (1997), in his work on healing art in Ethiopia, also investigates the relation between faith and materiality. He states that ‘faith [is made] the foundation of the images’ effectiveness. The material object, and above all the body, is nothing by itself … For faith, fugitive as it is, can achieve anything, including the real presence of holy intercessors, health, and healing’ (p. 84). Despite Talib Ali’s foregrounding of belief/trust and many similarities between the Ethiopian scrolls and kombe, I argue that the Qurʾan is different from the ‘art’ that Mercier describes. The Qurʾan’s healing power is, as we will see, ambiguously linked to faith and to the ‘religion’ Islam – and these ambiguities matter.
From my observations of how Mama Sue went about integrating the ingestion of medication in her daily routines, she did not drink kombe because she and her baby are Muslim and she did not take her affiliation to Islam as a precondition for evaluating the treatment as successful. In fact, she found my inquiries in this direction rather strange. However, based on their verbal testimonies and actions, respectively, both Talib Ali and Mama Sue regard kombe as treatment, as a way of betterment. While Talib Ali emphasizes betterment through belief as part of dini, Mama Sue situates the chances for betterment in the realm of dawa – entangled with dini. This entanglement of dawa and dini, however, does not always merge into a coherent account. When drinking kombe as an embodied treatment of affliction, neither is dawa always embedded in conceptualizations of dini nor does Talib Ali’s preconditioning of belief apply to all patients. Most prominently, Christians’ use of kombe prompts a different engagement with kombe as dawa ya kiislamu.
Christians drinking kombe
‘Even Christians come here!’ Tufa, a practitioner who works with Bi Mwaltima in the herbal dispensary, once proudly told me. ‘Yes, they also receive kombe and it helps them’ (2013, personal communication). Bi Mwaltima overheard our conversation and added: ‘Well, you see, they all just want to get healthy. Dawa does not have a religion’ (2013, personal communication). Many Muslims also take kombe without making an explicit connection to their religious affiliation, such as Mama Sue. However, often Christians’ use of kombe is discursively highlighted to stress that ‘dawa does not have a religion’. Despite imbuing the body with the Qurʾan, in this context kombe is primarily framed as treatment that affects bodies that need medical attention.
Tufa’s and Bi Mwaltima’s statements resonate with what Allyson Purpura (1997) encountered in the 1990s. She quotes Mzee Chuma, an Islamic practitioner in Zanzibar:
‘The power of the Qurʾan is not about religion’, he [Mzee Chuma] explained. ‘If it was, we wouldn’t be able to cure people with religions different from ours. Even though Christians were not given the Qurʾan, we can still use the power of the Qurʾan to cure them. It can cure anyone with a problem. Whether or not you are a religious person, you will still be cured.’ (p. 307)
Through the body, affliction is treatable. The afflicted body, here, is a material entity distinct from the person’s religious affiliation; however, the religious affiliation is simultaneously embodied. The body that the subject has, and is, inhales frankincense in a church or prostrates during prayers. It is the body multiple that is medically treated and with which (religious) subjectivities of all kinds find material expression.
Many Muslims, talking about Christians, find several reasons why Christians choose to receive dawa ya kiislamu, although Christians themselves are very covert about it. One of the most prominent reasons is the type of affliction. Having a Muslim spirit bother you (for example, by rising to your head and using your body to move around crazily to then be soothed by Qurʾan recitations) is an affliction that everybody including Christians can suffer from and that is often treated with dawa ya kiislamu. 17 The Islamic healer Hakimu Saleh explained: ‘Because, you see, the spirits don’t choose people according to their religion – and if you have a Muslim spirit, even if you are a Christian, it is best to treat this condition with Islamic dawa’ (2014, personal communication). ‘Having a spirit’ (kuwa na sheitani/kuwa na jini) is usually framed as a ‘spiritual’ problem that biomedicine fails to treat and that therefore needs ‘alternative’ or often more specifically ‘Islamic’ treatment. Thus, recounting cases of Christians being afflicted with Muslim spirits leads to the logical conclusion of Christians’ recourse to dawa ya kiislamu. For ‘having a Christian spirit’ they would go elsewhere. For most people in Zanzibar, Christians resorting to dawa ya kiislamu in case of affliction does not contest their being Christian. Rather, Christians’ choice to receive treatment with dawa ya kiislamu highlights their situatedness in Zanzibar, that is, their making use of and submitting their bodies to which dawa is locally available, locally known to be effective, and associated with the orientation to the Indian Ocean that is of local importance. Treating kombe as dawa underpins Christians’ attempts to observe the distinction between purely ‘medicinal’ practices and practices that foster their ‘religious’ subjectivity. Interestingly, this separation of the practice of drinking kombe into the domains of ‘religion’ and dawa is also used by Muslims for themselves as justification against anticipated criticism (see below). It also makes possible an alignment of practices of drinking kombe as dawa within a verbalized, doctrinal theological framework.
For some people, drinking kombe as dawa ya kiislamu can be part of deliberately forming a ‘religious’ subjectivity (pertaining to a doctrinal domain of ‘religion’). Drinking kombe can be viewed, felt and narrated as a practice of piety, as observing one’s religious duties, and as confirming oneself as a subject of Islam. Dawa ya kiislamu can be connected to an encompassing Islamic notion of dini. As subjects are and have bodies, fighting affliction through bodily practices is also related to the formation and cultivation of religious subjectivities, much in line with what Talib Ali pronounces. However, discursive elements and bodily practices do not always match in this framework of dini. With my inquiry about kombe, it became a topic to be described, talked about, made pronounceable sense of. This prompted some people to see an ambiguity of patients’ behaviour: their multiple practices did not yield a coherent narrative about their subjectivities free of contradictions. Jean-Pierre Warnier (2001), building on Gregory Bateson (1987), approaches the juxtaposition of possibly contradictory practices and discourses with the ‘cognitive gap’ between verbal statements and the sensory-motor experience (see also Mohan and Warnier in the introduction to this special issue). This ‘cognitive gap’ accounts for the co-existence of statements with logically conflicting practices. With respect to drinking kombe in Zanzibar, this argument could be translated into the ambiguity of drinking kombe as an embodiment of Islamic scripture, on the one hand, and drinking kombe as treatment irrespective of doctrinal or normative affiliation, on the other. The verbalized knowledge of kombe’s healing remedies ‘to those who believe’ (Qurʾan, 17:82, Abdel Haleem, 2008: 180) appears to stand in contrast to the practice of Christians drinking kombe as dawa. In the latter instance, drinking kombe does not seem to challenge the state of being ‘Christian’. Is this a ‘gap’? With the ‘body multiple’, these gaps do not matter neither in the sense of its value nor its materialization. However, entangled within broader discursive power relations, this gap does matter.
For most people in Zanzibar, the ambiguity of Christians embodying Islamic scripture without challenging their status as Christians only matters with regard to a Zanzibari engagement with an anticipated criticism by an authoritative ‘other’. The arguments that are brought forward in this context are concerned with justifying a corporeal application of this specific re-materialization of the Qurʾan that is pertinent to everyone. This accounts not only for the ambiguity of the practice’s domain (especially when Christians are involved) but also expresses a desire to align the perceived tensions: closing the ‘gap’ especially matters when a coherent justification vis-à-vis an authoritative discourse is sought. The repercussions of this engagement feed back into the conceptualizations of ‘religion’, dini and dawa, and respective categorizations of subjectivities, reflecting both the ambiguity and the desire to resolve it.
Anticipating criticism as aligning tensions
‘Yes, of course, there are these people who don’t like kombe. You have to be careful who you talk to’, I was advised several times.
Some sheikhs say that it is not good to use the Qurʾan like this, but doesn’t the Qurʾan itself say that it is healing? And don’t we have hadiths that tell us that even Muhammad used the healing power of the Qurʾan? Some sheikhs say it is not good to have the Qurʾan in your body, because you should not take the Qurʾan to the toilet or pollute it otherwise. Some sheikhs say … (Hakimu Saleh, 2013, personal communication)
18
Arguments like these are put forward by people like Hakimu Saleh who are not against kombe as treatment but who attribute these argumentations to a discursively made ‘other’. I briefly contextualize the two points that Hakimu Saleh has attributed to ‘some sheikhs’ and his justifications. The first point, using the Qurʾan ‘like this’, alludes to an intellectual approach to the Qurʾan that requires reading and interpreting as the most important practices with the Qurʾan. In his justification, Hakimu Saleh refers to the first part of the verse 17:82: ‘We send down the Qurʾan as healing and mercy to those who believe; as for those who disbelieve, it only increases their loss’ (Abdel Haleem, 2008: 180). This is also one of the most commonly used verses for the preparation of kombe. While the second part is mostly omitted, 19 the Qurʾan saying about itself (in the first part of the verse) that it is healing is a strong argument for the use of the Qurʾan as medication to counter affliction. The argument that the ‘other sheikhs’ are said to make is not a contestation of this verse, rather a contestation of its literal application. ‘The Qurʾan heals, but not by being ingested without an intellectual encounter’ is the rationale attributed to these ‘other sheikhs’. Hakimu Saleh then provides a second justification to this first point which revolves around a hadith contained in the collection of Bukhari, in which it is recounted how the Fatihah (the opening sura of the Qurʾan) was recited over water and used to cure by the Prophet Muhammad. 20 Again, in the anticipated criticism of ‘some sheikhs’ the hadith itself is not challenged, but rather the implications it has for today’s practices. While ‘some sheikhs’ are said to only recognize water that the Qurʾan was recited over as medicinal water, kombe la kuandika (written kombe) is justified as it is the same Qurʾan that is transmitted to the water and in its written version it is less susceptible to noise pollution. The second point that Hakimu Saleh attributed to ‘some sheikhs’ follows up on the issue of pollution. While a msahafu, a codex of the Qurʾan, is liable to a number of rules including that it cannot be taken to the toilet, the ingested Qurʾan will necessarily be brought there eventually. Hakimu Saleh does not give a direct justification for this point in the above quote; however, this argument was often used to delineate what those ‘other sheikhs’ say and mostly put aside with a short laugh. It was explained to me once that kombe enters the body like good food that you also would not take to the toilet before eating, but which would unfold its effect in the body even if you go to the toilet eventually. Inside the body (and in fact already in their liquefaction) the verses do not constitute a msahafu anymore.
These ‘other sheikhs’, as they are often glossed by people who then enrol in a discourse of justifications, are said to be found amongst the people whose practices of Islam are influenced by what locally is perceived as Wahhabism.
21
Interestingly, those people who are believed to reject kombe are mostly indifferent about it when directly asked. Felicitas Becker’s observations explain:
The question of Qurʾanic or ‘book’ healing, uganga wa kitabu, into which many Tanzanian Muslims put much trust, focused many of the ambiguities Muslim reformists ran into … Despite their initial condemnation of every religious practice not explicitly sanctioned by the Qurʾan, the stance of the Ansuari [locally referred to as Wahhabi] on therapeutic uses of the Qurʾan was muted and unclear. On one hand, the use of the scripture as a means of protection was not in principle considered innovation. The notion of the Qurʾan as a panacea even had a certain resonance with Islamist ideas. On the other hand, the mixture of objects and substances with religious elements in uganga wa kitabu [to which she attributes kombe] smacks of shirk, the sin of idolatry, and the focus on the materiality of the scriptures runs counter to the reformist emphasis on intellectual engagement with them. By and large, the Ansuari dealt with the uncertainty by not pushing the point. (Becker, 2007: 28)
The few people who did voice their concern about kombe and were not indifferent about it did not justify their unease in a way predicted by those people who endorse kombe. The main issue amongst these exceptions was that the Prophet Muhammad is not reported to have written and drunk kombe and thus these practices depart from following the Prophet’s exemplary way of living.
Nevertheless, the arguments attributed to the Wahhabis circulate as anticipated criticism. The engagement with these arguments points to a perceived dichotomy between the practice of drinking kombe and a strict (kali) way of practising Islam attributed to Wahhabism with their claims to theological authority. Attributing scepticism to this ‘other’ that makes claims on theological authority reveals an awareness of the dominant discourses about the cultivation of a pious subject. At the same time, it shows the need to align scripture practices that even Christians make use of with spoken-about concepts rooted in an engagement with authoritative Islamic influences – to bridge the ‘cognitive gap’. The ‘others’’ arguments, together with justifications that then become relevant, show the tensions between the ‘sensory-motor experience’ that facilitates healing through dawa ya kiislamu (which even pertains to Christians) and the ‘verbal statements’ about contestations of kombe’s permissibility even amongst Muslims. The discourse in which this ‘gap’ matters does not provide room for multiplicity, but seeks coherence. The set-up of these bilateral issues is grounded on matters of materiality. Practices of and with the Qurʾan, the materialization of the Qurʾan and its incorporation into living bodies are problematized and entangled with the discriminability and overlaps of dini, dawa, and ‘religion’. Kombe being dawa justifies a use of the Qurʾan that might be contested by ‘religion’. Kombe being dawa ya kiislamu differentiates it from ‘medicine’ with its biomedical bias. Simultaneously, it specifies this dawa as ‘Islamic’. This specification shows a shift of a conceptualization of an all-encompassing, singular dini towards an understanding of ‘religion’ that inherently includes multiplicity. The anticipated criticism, along with its justifications, forges the discourse about the practice of drinking kombe to unfold different implications for the formation and cultivation of subjectivities with respect to the flexible ground of enacting dawa ya kiislamu.
Conclusion
Drinking the Qurʾan, drinking kombe, is in the projections of its materiality regionally embedded as a practice that from the Tanzanian coast relates to a Muslim Indian Ocean world. It thereby interacts with the nexus of dini, dawa and ‘religion’. Kombe incorporates the overlapping fields of ‘dawa’ and ‘religion’/dini in being termed dawa ya kiislamu. This discursive delineation provides space for multiple enacted emphases in this realm, including Christians’ use of kombe as dawa attuned to their ‘medical’ approach to health and disease. However, narratives about this way of drinking kombe struggle with this multiplicity as incoherent and ambiguous. Christians’ use of kombe accentuates the ‘cognitive gap’ between drinking kombe as embodiment of Islamic scripture conveyed by Islamic connotations of the Qurʾan that heals and drinking kombe as treatment irrespective of ‘religious’ affiliation. Despite their small numbers, Christians as patients who drink kombe challenge the conceptualization of dawa ya kiislamu as intrinsically connected to an Islamic notion of dini.
The anticipated criticism – accredited to a discursively made ‘other’ – questions the permissibility of drinking the Qurʾan on ‘religious’ grounds and requires the practices to be scrutinized. Subsequent justifications stress the effect of experiencing healing and are equally expressed in ‘religious’ terms. Attributing kombe to dawa, in particular dawa ya kiislamu, encompasses an anticipation of a sceptic ‘religious’ discourse about it while at the same time permitting Christians to take part in this practice and for anyone to cultivate a variety of overlapping subjectivities in this realm of dini, dawa and ‘religion’.
Bi Mwaltima complicates this picture. When she drank the cup of kombe in passing it was not related to practices of forming and cultivating her Muslim self. Nor was it required as treatment or part of a ‘medicalized’ practice bundle. Her drinking of the Qurʾan is partly informed by her situatedness in a Zanzibari herbal dispensary where the practice exists, kombe is produced, where she works and has access to it. It is also informed by Bi Mwaltima being a Muslim and could be read as a prophylactic measure but, most of all, Bi Mwaltima drank kombe as a result of the situation, spontaneous and random, as a kind of bodily habitus.
Footnotes
Acknowledgements
The research is part of the project ‘Habitats and Habitus: the Politics and Aesthetics of Religious World Making’ chaired by Birgit Meyer. I wish to express my deepest gratitude for being part of her project and for her insightful comments during the evolution of this article. I also wish to thank Kristina Dohrn, Benedikt Pontzen and Markus Fiebig, as well as Urmila Mohan and Jean-Pierre Warnier for their close readings and the fruitful exchange. Furthermore, I would like to thank the participants of the conference ‘The Bodily and Material Cultures of Religious Subjectivation’ for the lively engagement. Last, but not least, the two anonymous reviewers have provided much food for thought and immensely improved this article.
Funding
This research was funded by the Anneliese Maier Prize (Humboldt Foundation) awarded to Birgit Meyer and there is no conflict of interest.