
Abstract
As the opioid overdose crisis in the US persists, governments have coordinated with drug companies to propagate the overdose reversal drug naloxone (Narcan) as a ‘kinder/gentler’ state response, deriving from a supposedly progressive harm reduction ethos. Drawing on Derrida’s deconstruction of pharmakon, I show how Narcan is rendered paradoxical and terminal, diverting attention from the structural antecedents of opioid addiction and resources for drug treatment while reproducing corporeal suffering in those revived. I further highlight how Narcan is positioned in a wider array of regressive governing practices that legitimate the state’s punitive drug war and demonization of drug users. Narcan thus provides a useful opening between the state and contemporary biomedicine to theorize how harm reduction and public health unfurl in insidious and corrosive ways.
Even the best of intentions to help or to serve the socially vulnerable can also simultaneously perpetuate—or even exacerbate—oppression, humiliation and dependency of one kind or another (Bourgois 2000: 168–169).
In May 2019 paramedics, firefighters, and police responded to a 911 medical emergency at the transit bus depot in downtown Appleton Wisconsin, where 47-year-old Ruben Houston was found unresponsive. Paramedics determined Houston had suffered an opioid overdose and administered two doses of the overdose reversal drug naloxone (Narcan). The first dose reestablished breathing. The second restored consciousness. After walking himself off the bus, Houston told paramedics he used some of his wife’s prescribed morphine for knee pain and declined their suggestion to seek additional medical care. The situation escalated from routine medical protocol when police questioned the just-revived Houston and attempted a pat-down for weapons before allowing him back on the bus. Rebuffing their search attempts and backing away, Houston drew a gun and fired at the questioning officer, who retreated. Other police on the scene returned fire and chased Houston, who fired again, fatally shooting a firefighter and wounding an officer before being shot multiple times by police and taken into custody, dying later at an area hospital. Twenty-four total shots were fired in a 30-second event so frenzied a bystander was also shot twice by police and hospitalized (Yang, 2019). Roughly a month following the tragedy, officials released body camera footage of the incident and held a press conference where the county district attorney confirmed police use of deadly force was justified. The tandem press conference and body cam footage release generated an extended round of media coverage and went viral, featuring on the extreme sports forum mixedmartialarts.com titled ‘Junkie kills firefighter (RIP)’, and the gun enthusiast site tactical-life.com titled ‘WATCH: Appleton police kill suspect who suddenly shoots, kills EMS’.
The story also featured in the Officer Safety section of lawofficer.com which identifies as ‘the only major law enforcement publication and website operated by law enforcement, for law enforcement’. The user comment thread below the story revealed an inchoate resistance to, and palpable disgust with, Narcan as currently structured. For some commenters, its propagation reflects a naive, misplaced empathy for opioid users. In this view, Narcan saves those unworthy of living while condoning drug abuse, addiction, and resulting harms. The following comment sequence is illustrative:
COMMENT 1: What a piece of shit lowlife drug user . . . I am glad he is gone. I worked in a hospital for years and honestly . . . sad to say, but drug users are a major pain in the ass and should be left to fend on their own and stop costing tax payers when they just keep repeating the same old crap . . . Drug and alcohol abusers do NOT have a disease . . . it’s a lame excuse. COMMENT 2: All frequent fliers, on their third strike need to be let go to the other side. Communities will improve, homeless rates would decrease, drug houses will go back in the market to be gutted and rebuilt, and the people who actually need Narcan, like the first time drug doers or the folks who were going through rough times and took too big of a hit, will get it, rather than it being wasted on these ‘scum of the earth, just looking for a fix while never contributing to society’ ass people!!!! P.S. I am a first responder and frequenters need to be left to GOD. Chasing that dragon has one inevitability. Death is the highest high so let them reach it and be with the lord.
While the tragedy of the Appleton case combined with the felt-anonymity of the internet may have emboldened commenters to express their frustrations in especially brutal terms, similar sentiments have been articulated for years in the US by legislators and police. In June 2017, a Middletown Ohio city councilman proposed a ‘three strikes’ policy for overdose reversals with Narcan. The policy would have required first- and second-time patients to complete community service work equal to the cost of emergency medical response. On a third overdose, Narcan was to be withheld. Justifying the proposal as necessary to manage budgetary strains, he stated: ‘I want to send a message to the world that you don’t want to come to Middletown to overdose because someone might not come with Narcan and save your life’ (Bacon, 2017). That same year an Ohio sheriff in an adjacent county generated a windfall of controversy in explaining how, in the context of record-level opioid overdose deaths, his officers do not, and would not, carry Narcan. ‘It’s very dangerous’, he said. ‘We’re not winning this battle and Narcan is not the answer’ (Pack, 2017). And in 2018, Maine governor Paul LePage vetoed legislation that would make Narcan available at pharmacies without a prescription. Explaining the decision, he wrote:
[Narcan] does not truly save lives; it merely extends them until the next overdose. Creating a situation where an addict has a heroin needle in one hand and a shot of [Narcan] in the other produces a sense of normalcy and security around heroin use
In order to consider not only the ‘cold indifference and resignation’ apparent in how Narcan is disavowed by some police and lawmakers (Linnemann and Medley, 2019: 151), but also the cruelties reflected in its propagation and deployment, in this article I engage a critical reading of Narcan as emergency medical interruption of opioid-induced overdose to uncover its contradictions. In Ruben Houston’s case, it was the application of Narcan—not to restore breathing and transport to hospital, but to restore consciousness—that transformed the situation from medical to criminal. As Narcan is lauded as a biomedical intervention that is at once rational, humane, and effective, it provides fertile ground to engage the politics of harm reduction as construed in the current neoliberal moment. Although critical of Narcan propagation as an almost singular response to the US opioid crisis, my aim here is not to trivialize those suffering opioid addiction, nor to dismiss those whose breathing was restored following an overdose. Rather, I argue it is important to complicate Narcan’s logic as a biomedical technology that offers those revived the opportunity to become ‘resilient subjects’ who ‘bounce back’ and ‘fight another day’. Mark Neocleous (2015) argues that as both a personal/subjective attribute and ‘neoliberal ethic’, resilience lays the foundation for ‘subjectively dealing with the uncertainty and instability of contemporary capital while it simultaneously masks the fact that resources are far from equally shared’ and bouncing back not equally possible. While giving a ‘shot’ of Narcan may be understood as a ‘magic bullet’ operating on the brain’s opioid receptors, it is also one of a number of technologies emblematic of the precarity of late capitalism that obfuscates fundamental inequities such as lack of comprehensive healthcare. Narcan therefore provides an opening between the state and contemporary biomedicine where broader critiques of US drug policy can be extended. I first situate Narcan within a particular model of medicalized neoliberalism. Following this I highlight how Narcan works to reproduce and reaffirm the taken-for-granted cruelties of the present social order.
Narcan as biomedical panic
Moral panic has been the traditional, if not de facto, theoretical lens employed to examine historic and contemporary drug discourses. Initially developed to theorize overwrought media reaction to deviant youth subcultures, in incipient form, moral panics were framed as regressive, ultimately mobilizing legislators to enact policies that would reestablish control over those ‘folk devils’ believed to embody a problem (Cohen, 2002 [1972]). Moral panic has since been subject to extensive theoretical revision, with analysts highlighting how, in a late-modern risk society, issues of social concern do not adhere to a mediated ‘top–down model’, but are ‘catalyzed by real-world events’ (Ungar, 2001: 277). Per Beck (1999), the intrapsychic condition of the risk society constitutes a ‘peculiar, intermediate state between security and destruction, where the perception of threatening risks determines thought and action’ (p. 135). Reformulations have attempted to diffuse the concept to account for so-called ‘good’ moral panics (Cohen, 2011) that function as ‘normatively ambivalent operations of power’ and respond to social suffering through ‘technical modes of rational governance’ (Hier, 2008: 181). Predicated on actuarial forms of risk management and responsibilization (Garland, 2001; O’Malley, 1996), contemporary (good) moral panics exist in a circumstance where the state—recognizing the limits of its own sovereign power—does not endeavor to control the general population by promoting ‘moralising discourses, but instead, ‘stages its own retreat into a kind of populist, lowest-common-denominator technocratic stewardship’ in a way that ‘allows us to persist in a normal condition of anxious complacency’ (Horsley, 2017: 88–93).
Foucault has long highlighted how liberalism’s sustenance is contingent on the nurturing of anxieties about various dangers. Constantly striving for permanent security and social order, the state is never able to fully resolve proliferating risks that are at once diffused, omnipresent, perpetually evolving, yet knowable and with the potential to be mitigated by application of scientific expertise. A recurring theme in Foucault’s writings on biopolitics and governmentality, beginning with Birth of the Clinic (1963) and continuing through his later work on ethics (1979) describes the state’s proclivity to intervene in the life of its subjects through a preoccupation with a ‘politics of health’ (birth and death rates, diseases and epidemics, mastery of the physiological constitution of populations and sub-populations). In contemporary manifestations of biopower, Nikolas Rose (2007) has theorized the expansion of a Foucauldian ‘politics of health’ to a neoliberal ‘politics of life’, where individual action is guided or led by an expert culture that folds in the healthcare system, private nonprofits, and biotech multinationals that market drug technologies to keep consumer-subjects alive and productive. In a politics of life, danger and harm become fundamental to capital, and are central to pharmaceutical companies’ push to biomedicalize risk through investment in therapeutic interventions. Governing at a distance, the state serves as middleman for these entities, allocating tax revenue and workers, ‘promoting the agenda’, and monitoring results through data collection and reporting.
In a politics of life, the contemporary opioid crisis and tactics to manage its most serious harm—death—may then be viewed as a paradigm example of a ‘good’ moral panic. Prompted in part by a raced/classed framing of the opioid crisis as uniquely ‘ravaging white communities in the Northeast and Midwest’ (Seelye, 2015), the state has altered its approach to drug problems, pivoting from a ‘tough on crime/drug war’ approach to a supposedly ‘kinder/gentler’ tack that folds in pharmaceutical technology and emergency response. Here the medical industrial complex seizes on the overdose crisis as a market opportunity (Denvir, 2017), inviting both professionals and lay citizens to partake in the benevolent responsibility of managing its highest value community—life itself (Rose, 2007). The state assists, appropriating millions in tax dollars to get Narcan into the hands of not just first responders- defined here as emergency medical technicians (EMTs), paramedics, firefighters, and police- but to diffuse constituencies of actors such as librarians, teachers, gas station employees, friends and family of opioid users, and users themselves. While Narcan propagation may signal a beneficent shift in the state’s approach to drug harms, it is also illustrative of an adaptive criminal justice system that has co-opted medical and treatment discourses to expand its reach. 1 Indeed, most police agencies do not equip their personnel with Narcan (Quinn, 2019) and although officers respond to overdose calls in an expanded role as first responders, their principal commitment is to threat management.
From harm reduction to war on overdose
First approved by the US Food and Drug Administration for reversing opioid overdose in 1971, naloxone was kept tightly limited by organized medicine before being gradually extricated by harm reduction activists in the mid-1990s (Campbell, 2020). Adopting various tactics from distribution of naloxone via Reddit forums, partnering with patient advocacy groups, to lobbying local officials, naloxone distribution was placed on the legislative agenda only after state officials realized that visible, rising overdose deaths were a political liability. By 2017 policy and innovation had changed such that naloxone was effectively ‘tamed’—‘on the way to becoming just another pharmaceutical ‘product’; ‘addicts’ were consumers; and access issues no longer seemed to have social justice implications’ (Campbell, 2020: 294).
This trajectory, though abbreviated, is also broadly illustrative of other harm reduction initiatives in that what began as ‘bottom–up’ social movements morphed into ‘top–down’ policies, with a ‘saleable emphasis on medical benefits’ (Roe, 2005: 245). Critics of top–down harm reduction argue it is ‘a safety net, not a strategy’ (Miller, 2001: 177) and that by assuaging the worst effects of drug problems such as overdose death and blood-borne disease transmission, as a ‘brand’,
2
harm reduction technologies like Narcan overlook the structural and cultural antecedents of drug crises (Bourgois, 1998; Moore and Fraser, 2006):
‘Mature’ medical harm reduction . . . is characterized by a dangerous acceptance of the present situation of drug users, fatalism towards the prospect of larger change, failure to challenge the contradictions of licit and illicit drug use, and a continuation of the assumptions of addiction and morality that underlie abstinence and enforcement (Roe, 2005: 248).
Rejecting such criticisms, Keane (2003) argues that harm reduction’s amoral stance and technical/medical approach to the acute management of drug harms is in itself radically disruptive of normative understandings of drug use. ‘Bottom–up’ initiatives such as peer-administration of Narcan have indeed been framed as a pragmatic harnessing of neoliberal imperatives for progressive ends that ‘empowers’ drug users (e.g. Faulkner-Gurstein, 2017). While Campbell (2020) similarly describes Narcan as a ‘technology of solidarity’, she also cautions that—as a ‘biopolitical therapeutic regime’—state-sponsored harm reduction programs risk alienating both serious long-term opioid users and the activists who worked to make Narcan available in their communities long before it became a surging institutional fad (e.g. Anderson et al., 2010; Best, 2006).
Philadelphia city’s response to its opioid crisis reflects some of these tensions. In 2017 the overdose mortality rate for Philadelphia was higher than any major city in the US at 77 deaths per 100,000 persons (DEA, 2018). Established in 2017 in response to a problem that had been accelerating for years, the city’s ‘Opioid Task Force’ initially moved to address the problem by emphasizing the responsibilization of citizens via Narcan propagation. Figure 1 shows a screen capture from the Task Force’s website.
Medicalization via responsibilization.
As seen in Figure 1, the Task Force endorses a ‘call for help—revive—call for more help’ model of medicalization through taking ‘action’. 3 Contemporary biomedicine and the state share a commitment to particular modes of problem-solving that address complex social ills like drug addiction through reliable, quick-fix outcomes (Bourgois, 2000). Narcan propagation is emblematic of this emphasis, especially given the neoliberal norm of governments contracting with private companies to provide market-based solutions to problems.
As the national opioid problem grew, prices for Narcan rose sharply, with the cost for intranasal versions having increased 129% since 2012 (Denvir, 2017). Presently Narcan costs about $150 for two nasal-spray doses, and newer, easier-to-use versions can cost up to $4500. Recently the multinational pharma giant Emergent BioSolutions completed its acquisition of Adapt Pharma, maker of the Narcan nasal spray, for $735 million, ‘expanding the company’s presence in the public health threats market’ with the aim of ‘boosting and diversifying its product development’ (Zacks, 2018). Emergent also boasted that ‘[s]hares . . . have surged 30.15% this year, against the industry’s decrease of 14.5%’ since the acquisition. As local and sta governments are by far the largest purchasers of Narcan, we may observe a neoliberal, marketized response to the opioid crisis, predicated on the ideal of responsibilization, logically addressed by ubiquitously marketing the latest drug device.
Consistent with neoliberal ideals of individualism, Narcan propagation as harm reduction tactic imbues dying bodies with a new and sudden corporeality. It is corporeal reanimation that holds the promise of transforming those (still) suffering opioid addiction through the opportunity to engage in self-help and treatment seeking—a second chance at life. However, as with drug treatment services in public and private domains, Narcan does not claim to ‘cure’ persons of addiction (Iacobucci and Frieh, 2018). 4 Rather, it reanimates bodies. Once the threat of death is quelled, the problem is no longer defined as medical emergency. From then, medical care is predicated on individual choice and one’s personal resolve to seek treatment. Narcan quite literally offers a ‘wake-up call’. Treatment and therapy are not in its purview. 5
Data indicate the number of overdose deaths in Philadelphia fell by 8% in 2018. The 1116 total fatalities represented a decline of 101 deaths from the prior year when the Opioid Task Force was established. Although Philadelphia still had the highest overdose death rate of any major US city, and in fact had declared a ‘disaster emergency’ in one of its most severely afflicted neighborhoods, city officials credited the bulk-purchase and distribution of Narcan as driving the modest decline and hosted a formal event in celebration (Whelan, 2018). However, a more nuanced parsing of the data reveals a contingent decline that did not extend to the city’s most vulnerable. While total overdose fatalities declined from the 2017 peak, drug deaths among homeless Philadelphians increased between 2016 and 2018, with overall homelesss deaths having tripled in the last decade (Whelan, 2019). 6
Narcan as resilience in a politics of life
In a politics of life, human beings are ‘somatic individuals’, and personhood is synonymous with corporeality (Rose, 2007). Faced with the inevitability of corporeal death, the urgency to derive meaning in life must be negotiated against the ‘constant threat of nonbeing and numbness’ (Hoffman, 1998: 16). To understand how this tension is reconciled, it is useful to recall Franco Berardi’s The Soul at Work (2009; also see Adams, 2016). In theorizing the organization of late capitalist labor relations, Berardi describes a capitalist culture that has harnessed biomedical tactics of desensitization, aggressively marketing prescription drugs to neutralize the feelings of pain and existential lack that are symptomatic of the present order. In the US case, a ‘psychotropic reformatting’ (Berardi, 2009: 88) is accomplished through the prescribing of opioids like Vicodin (for somatic pain), benzodiazepines like Xanax (for anxiety), or stimulants like Adderall (for attention deficit). As a ‘kind of labor of the neoliberal entrepreneurial self’ (Neocleous, 2015), this psychopharmacological imperative is sufficient to return the subject back to a ‘deadened, efficient productive state’ (Berardi, 2009: 88), ‘recycling the pains created by capital into a resource that can then be used by capital’ (Neocleous, 2015).
In a moral panic over rising overdose deaths, the drug user’s body becomes an intensely governed body and intervention at the biochemical level is the imperative. As an opioid antagonist, Narcan restores corporeality by destabilizing an opioid’s grip on the receptors of the brain. It provides a partial or full overdose reversal. A ‘partial’ reversal restores breathing. In hospital settings, naloxone is administered initially in a low dose, then titrated to optimize reversal of opioid-induced respiratory depression (Lynn and Galinkin, 2018). Out of hospital, titrating naloxone to optimal effect is impractical and so a standardized dose deployed in an emergency ‘rescue’ context is the propagated form. In its newest intranasal formulation, Narcan offers a ‘full’ overdose reversal (consciousness restoration), and may be understood critically as a form of corporeal discipline.
The street advertisement in Figure 2 is illustrative. In a ‘concentrated 4-milligram dose’, it boasts the ‘highest available concentration of naloxone for individual use in the community’. The advertised 4-milligram dose is 10 times stronger than the initial intramuscular injectable version and five times stronger than the first intranasal device. The ad further emphasizes the product’s ease of use over more primitive formulations like intramuscular, intravenous, or subcutaneous naloxone. Equipped with the 4-milligram intranasal version, the responding citizen will always be ‘prepared to act’ without regard to ‘additional preparation’ or other medical training. Here Narcan is positioned as technology of resilience, orienting subjects to a future emergency beyond their control, but one that they will be equipped to manage and bounce back from (Neocleous, 2015). Although a ‘slow push’ to restore breathing is medically recommended, the advertisement in Figure 2 promotes administering a powerful concentrated dose. The fine print contains disclaimers, noting that: (1) administering Narcan is not intended as a substitute for professional medical care; and (2) one should consult the product monograph for contraindications, warnings, precautions, adverse reactions and drug interactions.
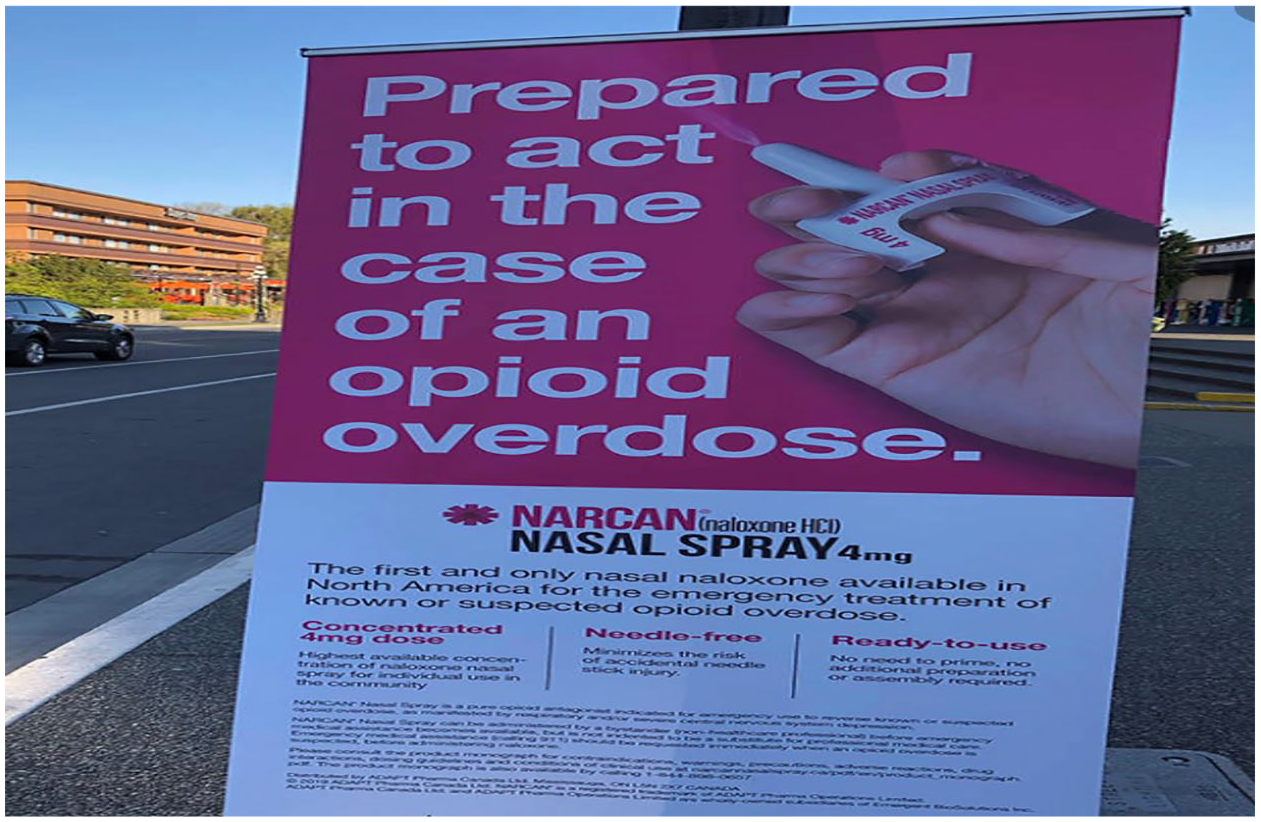
Narcan 4mg nasal spray advert.
Politics of life, politics of harm
In order to position Narcan within a broader regime of biopower and further illustrate its contradictions, it is useful to recall Jacques Derrida’s Dissemination (1981), where his deconstructive move takes up a reading of Plato’s Phaedrus, foregrounding the ancient Greek word for drug: pharmakon. Here Derrida traces its ambiguous and contrary meanings to connote: remedy, poison (toxicon), drug, recipe, charm, medicine, substance, and spell. Highlighting the philosophical concept of indeterminacy and as a metaphor for discourse, pharmakon becomes something particular only in context, depending on how it is deployed. We may then consider Narcan as pharmakon through a reading of how its medical and cultural forms are rendered paradoxical or terminal.
Narcan as iatrogenic, treatment as punitive
While not residing in the US federal drug schedule, naloxone, whether in intramuscular, subcutaneous, or intranasal form, is a prescription drug. 7 As with other drugs—prescribed or prohibited—adverse effects are common. Minimized by drug manufacturers with the softer phrasing side effects, adverse effects are ‘iatrogenic’—harms generated by the medical treatment itself, or by the misapplication of a treatment by a person (paramedic, EMT, police officer, friend, relative. . .) acting in the capacity of a healthcare professional (Illich, 1975). ‘Common’ adverse effects of Narcan are listed as: flushing, dizziness, tiredness, weakness, fever, chills, shortness of breath, body aches, diarrhea, stomach pain, nervousness, restlessness, and irritability. More ‘serious’ adverse effects include: agitation, abnormal brain function due to hypoxia, 8 seizures, coma, or death (Cunha, 2019). Those more ‘common’ adverse effects are associated with heroin and opioid withdrawal—a condition Narcan itself induces. Although infliction of pain in the process of an overdose reversal is by no means an inevitability, as Narcan’s potency has increased with the propagated 4mg nasal spray, precipitated withdrawal 9 has become routine to its application. Defined by brain destabilization and somatic suffering, Narcan is ‘linked as much to the malady as to its treatment’ (Derrida, 1981: 99), achieving both repair of the subject (in corporeal revival) and abuse of the subject (in withdrawal sickness). While Narcan-induced withdrawal symptoms like anxiety, nausea and agitation are knowable internally to the sufferer, they are also external and visible to others. Somatic suffering, then, becomes embodied evidence of Narcan’s success—a ‘politics of life’ in action.
The dominant mode of addictions treatment in the US further reinforces the exercise of biopower (e.g. Meyers, 2014). For example, medication assisted treatment in the form of opioid maintenance therapy with buprenorphine (brand name: Suboxone, Subutex, Sublocade) has long been considered the ‘gold standard’ for treating opioid use disorder. In the US context however, formal treatment programs are rife with conditional requirements that create disincentives to enrollment and retention. In addition to geographic and other resource-driven barriers to access, criteria for program enrollment are often punitive. Mandating surveillance of enrollees with urine screenings where submitting a ‘hot piss’ is addressed through sanction, restrictions on other medicines for co-occurring mental health issues, or the absence of cognitive-behavioral therapy, are defining characteristics. Punishment for relapse includes program de-enrollment and coordinating with doctors to blacklist rule violators from accessing buprenorphine. Alienated subjects then opt to acquire buprenorphine illicitly, return to heroin use, and experience a general cynicism toward formal addictions treatment (Kavanaugh and McLean, 2020). 10
The cruelty of first response
As poison and remedy, pharmakon requires a patient-subject who is held up as the exemplar of a biomedical offering, but who is simultaneously the locus of failure and deception, or scapegoat (the pharmakos). Also translated as druggist, poisoner, wizard, magician, or sorcerer, we may extend the concept of pharmakos from patient-subjects to the first responders who administer Narcan. As the process of rescue induces consciousness along with somatic pain, revived bodies may become unpredictable and in need of extra-medical discipline. Threats, and interpretations of them, are further complicated in that first responders span at minimum four professions (paramedics, EMTs, firefighters, police). Variability in managing revived subjects often reflects the medical knowledge of a given profession. Paramedics have the highest levels of certified training. EMTs are certified at a ‘basic’ level. Firefighters and police are generally not certified, but sometimes take courses on recognizing an opioid overdose and administering Narcan. Accordingly, paramedics are more likely to correctly identify adverse effects like confusion, agitation and combativeness as resulting from hypoxia, whereas those with less training are more apt to interpret such behavior as anger about Narcan having ‘ruined their high’.
Reflecting on possible policy changes in response to overdosed persons following the tragedy in Appleton where multiple persons were shot after police attempted to detain and question just-revived Ruben Houston, one agency head commented: ‘We just wasted their money, essentially, on whatever drugs they took … We took away whatever euphoria they were in’ (BeMiller, 2019). Flipping on its head the classic view of medicalization as transforming subjects from ‘badness to sickness’ (Conrad and Schneider, 1992 [1980]), Narcan is also capable of re-inscribing ‘badness’ onto subject bodies. Its promise is also its threat. As the Ruben Houston case shows, the questioning and detainment of those revived who are viewed as suspicious, and if necessary their subjugation, is the police prerogative. To mitigate the ‘badness’ created by Narcan, Wisconsin police agencies have proposed handcuffing overdosed persons before administering it, despite acknowledging that complications like agitation result from giving doses larger than medically necessary (BeMiller, 2019):
Before the Appleton shooting, the Menasha Police Department was already preparing to restrain people who are unconscious and suspected of overdosing. Chief Tim Styka said the department began using a higher dose of Narcan, which can make people even more volatile.
Rather than innovating a paradigm shift in the governance of drug users, Narcan may then be viewed as one of a number of technologies in a reconfigured and re-declared drug war, repackaged as a ‘war on overdose’, but ultimately reflecting the state’s commitment to governing ‘through’ its various drug problems (McLean, 2018; also see Linnemann, 2013).
In addition to misunderstandings deriving from lack of education, the modes of stress-management employed by emergency medical personnel can exacerbate the feelings of numbness that are endemic to late capitalism. In The Soul at Work, Berardi (2009) describes how increased exposure to the stimuli and technological overload that define contemporary modes of work results in a ‘deadening of the psychic crust’ and diminished capacity for in-feelings. We may also apply this characterization to first responders. Emotions are not useful in a no-nonsense rescue context where life is on the line. The nature of such work necessitates a cool detachment to both perform effectively and to ward off traumatic stress that might be triggered by feelings of empathy (Regehr et al., 2002). Figure 3 illustrates the oft-grim humor EMTs employ to manage the stress of their work. Such memes are widely circulated on popular first responder-themed social media platforms (i.e. #worstresponders), as a darkly absurd way of managing the intrapsychic pain deriving from repeated exposure to the dead or dying. The first sequence shows the restoration of breathing with Narcan followed by transport to hospital. The second shows responders loading a body bag onto a gurney. This form of ironic distancing—deriving laughter from the overdosed dead—somehow renders the dystopian present where drug overdose deaths remain at record high levels, more livable.

Narcan meme circulated by first responders.
We may also view such sentiments as reflecting what Neocleous calls a ‘training in resilience’ (2012: 189; also see Linnemann et al., 2014). Akin to Berardi’s (2009) notion of late capitalist labor relations resulting in a deadening of the psychic crust, symbolic displays of resilience work to harden both first responders and the public to the seeming intractability—indeed, banal normality—of the current opioid crisis. Though Figure 3 makes light of the dead, it also functions as critique. In the context of an overdose death rate that remains among the highest in the world, we may also read in-jokes like Sometimes Narcan, Sometimes Narcan’t as problematizing the state’s response to its protracted drug problems with a medical technology aimed at the level of the bio, but which is unable to keep pace with innovations in illicit drug markets.
While Figure 3 highlights the increasing uncertainty of Narcan’s success in a heroin market characterized by the ubiquitous presence of synthetic fentanyl, the image in Figure 4 laments those Narcan has revived.
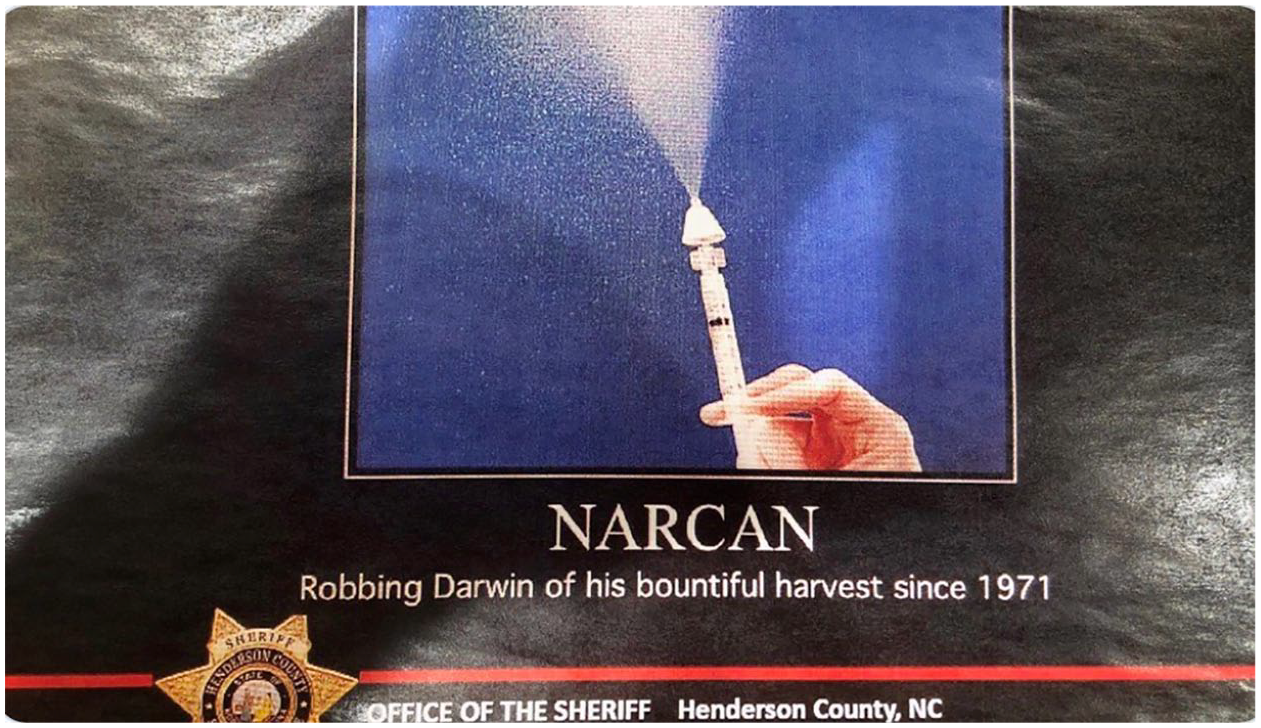
Narcan meme circulated by North Carolina police.
Circulated in an email chain by an unnamed employee of the Hendersonville North Carolina Sheriff’s Department in the spring of 2017 when US drug overdose deaths were nearing their peak, the meme was submitted to the press that December by an anonymous whistleblower (KIRO7, 2017). The objectionable sentiment expressed in the image was addressed by Sheriff Charles McDonald:
Regarding the offensive slide, there is no excuse for it regardless of the intention. I’m told it was an attempt at dark humor, but it was in no way humorous, and I know it does not reflect the true heart of the actual sender, or that of our staff and volunteers. I am aware that every person saved is someone’s child, parent, spouse, neighbor or employee caught in a desperate web of addiction from which I am certain they desire to be free.
However, as seen in the comment thread below the ‘lawofficer.com’ publication on the Appleton Wisconsin shooting tragedy, in first responder comments to the press on that same incident, as well as remarks by both legislators and police from Ohio to Maine, Darwinian ‘survival of the fittest’ sentiments are not exceptional among state actors. Rather, in policing’s ‘uncontrolled image’ (Linnemann, 2017a), we may observe revived subjects framed not as ‘sick’ and deserving of medical response—but as irresponsible and deserving of death. Despite official walk-backs intended to neutralize bad press, the principal lament is not for opioid users, nor their intimates, but for resources expended on reviving undeserving hedonists who ‘already made their choice’ (Pack, 2017), and then have the gall to become combative toward those who ‘ruined their high’ (BeMiller, 2019). Therefore, we should not dismiss the circulation of imagery wishing death on opioid users as ‘an attempt at dark humor’ that ‘does not reflect the true heart of the actual sender’, but instead understand it as evidence of the everyday cruelty of police and their reluctant service in a drug war reconfigured as a ‘kinder/gentler’ quasi-medical war on overdose.
Narcan as image work
As a metaphor for discourse pharmakon constructs a play of oppositions, signifying in myriad ways such that its meaning is overdetermined. Ambiguous and prone to manipulation, for Derrida, discourses possess the maleficent potential to distort truth by offering a simulacrum, which, presented as an addendum or supplement, is communicated as true and read as true by audiences. It is in police discourses where Narcan most aptly reveals this power of ‘maleficent penetration . . . that dangerous supplement that breaks into the very thing that would have liked to do without it’ (Derrida, 1981: 110).
While the sentiment expressed in Figure 4 was publicly disavowed by the agency head, in other instances Narcan is purposed as the latest tool in police–public relations work. Premised on ideals of community policing, Narcan has become one of a number of ‘best practices’ incorporated piecemeal into the police repertoire, and reflects the creep of police ever-further into the mundane functions of the social state. In this regard Narcan functions as a symbol, reminding citizens and communities that police are not some violent inimical force, but emphasizes their beneficent duty to protect, serve, and save. The following excerpt is illustrative:
A police officer in [Texas] helped save [a life] when he responded to a 911 call . . . A mother reported finding her son . . . unresponsive. Sgt. Morehouse said he used naloxone, commonly known as Narcan, to revive the man from a heroin overdose. This came just two months after the patrol officer received training on how to use the nasal spray on someone. ‘It was amazing to see this particular medicine . . . take someone that in years past we may not have been able to save,’ Sgt. Morehouse said, ‘but this person’s going to be able to move on for another day and hopefully get the treatment and help that they need’ (DuPree, 2019).
The story excerpted here, and others like it, may be read as part of an ideological project that redirects public attention from critiques of policing and its fundamental violence, to acknowledging it as a social and civic good. In their newly publicized role as lifesavers, attention is redirected from those suffering overdose back onto police, who themselves become pharmakos—the personification of sacrifice; the stoic sufferers who save, cleanse, and reorder (Girard, 1986). Storytelling through pharmakos foregrounds the ‘special case, the distinct, ennobled individual who . . . conveys cathartic suffering to the audience or readers’ (Herlinghaus, 2013: 22). Stories of the benevolent officer who allows overdosed subjects the chance to ‘move on for another day and hopefully get the treatment . . . they need’ function as a velvet glove strategy, obscuring that Narcan is a sometimes-tool of police existing on a continuum with the more familiar powers of arrest, taser, and firearm.
Although fatal shootings of just-revived subjects are rare, ‘saves’ that morph into arrest or subjugation upon revival—what critical police scholars Correia and Wall (2018) call ‘pain compliance’—are more common. In February 2020, Philadelphia police responded to an overdose call in a Rite-Aid parking lot where Narcan was administered by a pharmacist prior to their arrival. The dose restored consciousness, and the revived man began vocalizing unintelligibly and ‘striking parked cars and the ground with his body’ before being punched in the head with a closed fist by one officer as other police attempted to handcuff him (Palmer, 2020). Following this, the subject died en route to hospital. As the revived subject constituted an ‘immanent threat’, officers assumed their familiar role as threat managers, enacted as a ‘duty to protect’ life (gathered bystanders), and private property (parked cars). Although the incident remains under official investigation, the subject’s revival, subjugation and death marks another example of how those reanimated with Narcan often exist in the eyes of police as Others deserving of violence (e.g. Linnemann et al., 2014). Although police may respond to overdose events, we should recall that most officers do not carry Narcan, and that those who do rarely use it (Quinn, 2019). For example: New Mexico consistently has the highest rate of opioid overdose fatalities of any US state in the regional West. In an attempt to stem this rising tide, 2017 legislation required all New Mexico police officers to carry Narcan. The state’s largest agency—the Albuquerque Police Department—purchased 80 Narcan kits at $150 per kit, and as of 2019 had deployed it just three times. The remaining 77 kits have since expired. 11 Statewide, police deployed Narcan just seven times in a two-year period (Wilham, 2019).
While Narcan may be harnessed as a form of counterinsurgency in manufacturing the image of a kinder/gentler police officer, or to normalize violence against unruly subjects, in other instances it is purposed to highlight the purported dangers inherent in fighting a perpetually evolving drug war increasingly characterized by ‘illicit’ fentanyl, linked to clandestine Chinese laboratories and foreign Others (Kennedy and Coehlo, 2019). Always endeavoring to control its own image by communicating its inseparability from safety and order (Linnemann, 2017a, 2017b), police discourses around the opioid crisis adapt familiar neoliberal rhetorics of ‘emergency’ and ‘crisis’ to bolster security aims and reproduce police power.
News stories of police succumbing to opioid overdose via passive fentanyl exposure began going viral in 2017 when an Ohio officer was reported to have brushed fentanyl powder from his uniform and lost consciousness before being revived with Narcan by another officer. Although transdermal toxicity is not medically possible (Herman et al., 2020), such reports distinguish the fentanyl used by medical professionals to treat pain from the ‘illicit’ fentanyl found in street heroin (Kennedy and Coehlo, 2019). Following the incident, the American College of Medical Toxicology (2017) issued a public statement clarifying: ‘it is very unlikely that small, unintentional skin exposures to tablets or powder would cause significant opioid toxicity, and if toxicity were to occur it would not develop rapidly, allowing time for removal’. Despite this, reports of incidental overdoses from passive fentanyl exposure were noted in at least 551 news reports across 48 US states through December 2019 (Beletsky et al., 2020), including Vermont, where a state trooper reportedly became sick and collapsed in a parking lot after handling a small quantity of heroin, before being given Narcan by another officer. Prior to the completion of toxicology testing (negative for fentanyl), the state police director issued a press release:
Now there is a new threat that we’re seeing up close: the risk of exposure to powerful drugs that can kill in even tiny amounts . . . Were it not for the immediate availability of Narcan and the quick actions of his fellow troopers and medical personnel, we might be speaking today about the death of a trooper in the line of duty . . . I’m angry at how close we came, and relieved that the situation was no worse than it was (Meyn, 2019).
Such claims, articulated repeatedly and despite evidence to the contrary, underscore the importance of folklore in the construction of drug scares, as well as the theatricality and drama police engage in to exaggerate drug dangers. Here Narcan serves a useful purpose: as inoculating agent that keeps both police and citizen-subjects secure from dangerous new substances, and reaffirming police ownership of drug problems—even those that have been partially medicalized. Taking its cue from the US Drug Enforcement Agency, who issued several hyperbolic reports and onerous recommendations on the handling of ‘dangerous’ drug evidence (DEA, 2016), we may observe law enforcement’s ability to exploit the opioid crisis in a way that pivots from a kinder/gentler concern for the opioid user to one highlighting the ‘extraordinary work’ police do on behalf of citizen-subjects (Linnemann, 2017b: 62), the prioritizing of police safety, and the re-centering of punitive drug control policy through novel fear appeals.
Conclusion
My aim in this article was to stimulate a wider debate on the implications of Narcan as a treatment drug that is central to the state’s reconfigured drug war and to highlight its various harms—principally precipitated withdrawal or exposure to violence among those experiencing overdose as well as its novel positioning by police and state actors in drug war discourses. Narcan is on one hand the subject of a beneficent quasi-medical vocabulary of ‘patients’, ‘saves’, and ‘warm handoffs’ while on the other hand it is cast as a ‘moral hazard’—a perverse safety net that emboldens opioid users, fueling a backlash against those ‘frequent fliers’ who are revived multiple times (Campbell, 2020). As we have seen, this portends a circumstance where enthusiasm for Narcan’s lifesaving capability diminishes, and ‘shades of the persistent othering that have haunted drug users in the past’ are foregrounded (Campbell, 2020: 294). This is the essence of pharmakon—that of an ambivalent ‘poisoned present’ (Derrida, 1981: 77). While I do not dismiss out-of-hand the pragmatist position that Narcan propagation in the state response to the opioid crisis has delivered some genuine good, I have endeavored to show how it also functions maleficently—dehumanizing the overdosed dead and living addicted and representing some of the limits of ‘mature’ medical harm reduction.
Ever-flexible, the neoliberal state’s response to its overdose crisis through Narcan propagation is on one hand panicked and reactive, akin to a ‘good’ moral panic. On the other hand, it demonstrates an inability to effectively integrate social with biomedical interventions for drug rehabilitation (Campbell, 2020). It purports to reduce cost, but does so by using a version of Narcan powerful enough to reanimate bodies, thus lowering the likelihood of hospitalizing opioid users who lack private health insurance. It therefore lowers expenditures only by suspending opioid users in a permanent state of precarity, and administers punishment if revived subjects are not sufficiently docile. Narcan, then—like other harm reduction initiatives such as opioid maintenance therapy and safe injection sites—may be viewed as another ‘hostile exercise in disciplining’ (Bourgois, 2000: 165). Narcan should be understood critically and paradoxically—as pharmakon. Narcan is poison, cure, symptom, and more. It saves lives as it perpetuates suffering. Narcan is sadistic in its organization because it requires suffering as evidence of its effectiveness, and necessitates additional cruelties to quell the suffering it induces.