
Abstract
In recent years, the organisation of healthcare in many welfare states is gradually moving towards an individualised and responsibility-driven self-care and use of healthcare services. Departing in this restructuring of care, this article explores how bodies are experienced and how care is sough, by socially disadvantaged cancer patients. Based on repeated ethnographic interviews with 10 socially deprived cancer patients in Denmark, the article illustrates that socially disadvantaged cancer patients often experience their bodies and move between feeling fine and feeling sick in a disjunctive manner engulfed by the practicality of getting through the day. From a critical phenomenological perspective, we argue that this way of being in the world appears counterfactual to welfare expectations of proactive attention to the body, and contemporary moves towards increased individual responsibility for preventing serious disease and monitoring the body.
Keywords
Background
This article derives from years of empirical engagements with the dilemmas and complexities of social inequality and health (e.g. Merrild et al., 2016) and an increasing sense of concern, sparked by the changing politics of responsibilities currently taking place in emergent neo-liberal landscapes in Denmark (Hedegaard, 2016). In Denmark, where our research is based, the introduction of neo-liberal values is evident across the healthcare system, concretised in the move from institutionalised care and prevention to a more individualised, responsibility-driven care of the self (Mattingly et al., 2011). People assume still more responsibility for caring for their own health, and ‘being in good health’ is culturally and politically merited (Ludvigsen, 2016). As argued by others before us, shifts in care provision thus entail shifts in material as well as social care resources (Wilkinson and Kleinman, 2016). An example of this reorganisation is the way that follow-up for cancer patients is moving away from routine surveillance strategies in the secondary sector to an emphasis on individualised follow-up, positioning patients as key actors in identifying potential signs of recurrence and post-surgery and treatment needs. In addition, although cancer incidence has increased by 19 per cent for men and by 13 per cent for women since 2007 (Danish Cancer Registry (Canceregisteret), 2018), fewer people suffering from cancer are hospitalised when undergoing treatments (outpatient treatments for cancer have increased by 40% from 2007 to 2014), and hospital stays are shortened (from an average of 6 to 5 days) between 2007 and 2014 (Danish Health Authority (Sundhedsstyrelsen), 2016)). These transitions take place in a context of relatively high levels of cancer morbidity and mortality in Denmark compared with the northern neighbours (Coleman et al., 2011). They are at the core of what has been identified as an emergent global paradigm of successful ageing, which involves a concerted effort on behalf of governments to lessen the burden on the healthcare system through the promotion of health and active living among senior citizens (Lamb, 2014; Ludvigsen, 2016). This is also reflected in the institutional sentiments in Denmark, where public discourse and policy in subtle ways frame vigilance and awareness as proper ways to embody citizenship (Offersen et al., 2016). Also, once people have fallen ill, it is increasingly difficult to access long-term social benefits, perhaps suggesting how the poor and the sick are gradually made more responsible for their own misfortune (Mik-Meyer and Silverman, 2019).
In anthropology and related disciplines, a wide range of studies have been devoted to explaining how socially marginal and institutionally relegated groups are more inclined to suffer from chronic disease, and how sufferings intensify as forces of social stigma, material deprivation and social injustice join together (Das and Das, 2007; Farmer, 1999; Kleinman et al., 1997; Wilkenson and Kleinman, 2016). In contrast, the Danish welfare society is rich and governed by principles of egalitarian. As implied in the above, there is, however, also a growing need for a commitment to understand health in socio-political terms in neo-liberal landscapes of the Global North. As others and we have argued, political–economic forces are increasingly implicated in the extent to which health problems manifest and are experienced by those living at the margins of ‘welfare’ (Merrild and Andersen, in press; Mik-Meyer and Silverman, 2019). In terms of cancer, this is backed by epidemiological evidence, showing that ‘multi-morbidity’ is more prevalent among people living with cancer than among those who have not had cancer, a tendency that increases with social disadvantage (Hovaldt et al., 2015). In addition, there are significant social differences in how people with diverse social backgrounds manage after being diagnosed with cancer (Dalton et al., 2019; Hovaldt et al., 2015).
With reference to the socio-political backdrop of neo-liberal transitions, the aim of this article is to explore how the increasing expectations towards individual bodily awareness or sensitivity may conjoin with the increasing challenges of social inequality in both morbidity and mortality (Marmot et al., 2008). More specifically, we explore how people living with cancer in disadvantaged social situations experience their bodies and how they engage with the healthcare system when moving back and forth between feeling fine and feeling sick. Following theoretical conversations in what has been referred to as anthropological phenomenology (Desjarlais and Throop, 2011), and understanding embodied experience as temporal and disjunctive, we learn that people do not always understand and attend to their bodies in an unfolding, forward-looking manner, that corresponds with the scales of institutionalised healthcare. Institutionalised healthcare involve timescales and values that promote ‘efficiency’ and ‘awareness’. People may appropriate such values, but these values do not necessarily fit the ways that people can or wish to prioritise the social projects that dominant their life worlds (cf. Whyte, 2019).
Experiencing the body and care seeking
As others and we have argued care seeking is an embodied, highly situated practice, and how people experience and articulate bodily distress or alterations varies across different social groupings (Merrild et al., 2016; Offersen et al., 2016). Inspired by critical phenomenological approaches to sensory experience, where the body is understood as deeply conditioned by its situation in the world (Desjarlais, 1996, 2003; Throop, 2003, 2010), this article explores the ways that experiences of the body are shaped in close interaction with ‘the lifeworld – that domain of everyday, immediate social existence and practical activity’ (Jackson, 1996: 7). Our empirical focus is on how people, who are sick and suffer from degrees of deprivation, experience their bodies and seek care. Such modes of existence are frequently shaped by poverty, transience and contingency, which are conditions that increasingly characterise lives lived on the fringe of post-industrial society (Desjarlais, 1996: 89). From a more structural and politically engaged perspective, research on social suffering (Kleinman et al., 1997, Wilkinson and Kleinman, 2016) and structural violence (Farmer, 1999) has addressed and examined bodily experiences of pain and distress, as conditioned and moderated by social context. While drawing our inspiration from these perspectives on social inequality and injustice, our quest in this article is to understand how people experience their bodies and engage with the healthcare system in the context of the welfare state, when life is difficult, not only due to serious disease, but also due to social and material hardships. We suggest that the lives of socially deprived people may be characterised by what Desjarlais (1996) termed ‘struggling along’. The idea of struggling along depicts a way of existing and engaging with the world that focusses on the temporality and instability of everyday life when living in fragile, uncertain situations. According to Desjarlais, the notion of struggling along also serves as a commentary on academic conversations on the nature of experience. From a phenomenological perspective, the living body is the existential point of departure from which our various engagements with the world depart (Desjarlais, 1996). For this reason, exploring the embodied or sensorial aspects of suffering is not limited to focussing on subjective experience. It is a response to calls to study the pragmatics of sensing and to focus on the political, moral and temporal dimensions of sensorial experience (Desjarlais, 2003: 343) and care seeking in lives shaped by pain, illness, uncertainty, poverty and the sense that the rug might be pulled from under one’s feet at any time.
While tentatively applying the concept of struggling along as the lens through which we understand our interlocutors’ experiences of their bodies, we remain humble in the face of the destitute situations of Desjarlais’ homeless informants living in a Boston shelter. The lives of the people we worked with in Denmark bear little resemblance. Our interlocutors were not homeless. They were, however, sick and lived at ‘the bottom’ of a welfare society, in many ways struggling along in the sense that temporality, transience and uncertainty of what tomorrow might bring shaped their lives. Financially deprived, they toiled to get through the day, many of them also enduring social and psychological problems. Perhaps this mode of engaging with the world can be described by what Throop (2003, 2010) coined as disjunctive modes of experience. By disjunctive modes of experience, Throop turns our attention to the incoherent or fragmented nature of what we think of as experience. ‘By paying careful attention to the temporal orientation of our informants when engaged in, recollecting, or anticipating social action’ (Throop, 2003: 235), he states, may be a way to gain some insight into how different orientations engender differing varieties of experience. At times, the temporal organisation of attention and experience is turned towards the immediate and the present, in a more fragmented and disjunctive manner, and at times towards the more coherent, conjunctive and future-oriented mode of engaging with the world, thus guiding our attention forward and backward, according to our situation in the world.
Methods
In continuation of previous fieldwork carried out among different social classes in Denmark (some of whom were also living with cancer), Merrild did a longitudinal interview study among socially deprived cancer patients. A total of 10 persons, five men and five women who had been diagnosed with various forms of cancers, were identified through their general practitioner (GP), who contacted them based on the following simple selection criteria: short or no education beyond primary school, low income and living with a cancer disease. Initially, the GPs were asked to identify people who were no longer in a hospital follow-up programme, but this proved to be too difficult to carry out in practice. Hence, we ended up with a group of people who were suffering from various stages of cancer at the time of the study, which meant that the disease affected them differently. Originally intended as a fieldwork study that involved following participants in their everyday lives, the initial study design had to be altered due to the severity and fragility of their health and condition, into a design based on multiple interviews instead, and the participants, therefore, came to be regarded as Merrild’s interlocutors. This attests to the well-established point that working with people, who are frail and sick can be challenging, and that the research design must remain particularly flexible and adaptable to their needs and current condition (e.g. Cannon, 1992). The interviews did indeed turned out to be challenging, ethically complex undertakings. Sometimes, our interlocutors were clearly feeling very bad, although they insisted on completing the interviews. Sometimes, they were emotionally affected by the topics discussed, and sometimes, they had difficulties remembering why Merrild was there or what was being discussed. Hence, decisions constantly had to be made about whether to continue the interview, set up new appointments or even terminate the research project, based on a continuous reassessment of the participants’ condition. Using this approach meant that two interlocutors were only interviewed once due to the severity of their physical and mental health (one died and one was diagnosed with a new cancer). The rest were interviewed and visited 3 to 5 times during a period of 6 months. On average, the interviews lasted around 1 hour and focussed on various aspects of living with cancer. Sometimes, however, the interviews lasted longer; sometimes they were shorter, which, like the intensity of the interview, had to be assessed from time to time and always depended on the interlocutors’ state on the given day. All of the interviews took place in the interlocutors’ homes, except one, where the interlocutor chose to do the first interview at the cancer society, but subsequent interviews and visits also took place in his home. In addition to the formal interviews, Merrild also visited those whose health permitted, accompanying them to everyday activities, for instance, grocery shopping or spending time with friends. However, the lack of movement, energy and interest in life was a common feature among the interlocutors, as most of them could not get out of the house (due to their bad health), and in most cases, they did not really want to either. Hence, their lives were shaped by stillness, which turned out to be somewhat difficult to work with ethnographically.
Formal interviews were recorded and transcribed verbatim, and Merrild wrote down field notes immediately following informal conversations and field visits. Subsequently, interview transcripts were read and reread to identify emerging themes, which led to a thematic coding strategy focussing on experience of the body and care seeking. In the following analysis, we draw on examples from four cases: Simon, Karin, Liz and Jeffery, presented here in anonymised form using pseudonyms. We selected these cases as they particularly vividly illustrate some of the complexities of living life with cancer along with multiple other social, physical and mental challenges, complexities that were shared among all the interlocutors. It is not our intention to suggest that our interlocutors represent the lives of all cancer patients who live in socially disadvantaged situations. In line with our ethnographic approach, we want to point towards the ways that experiences are shaped and constructed, and thereby, through the cases and theoretical discussion, illustrate more general characteristics of how the body and care seeking is practised (Figure 1).
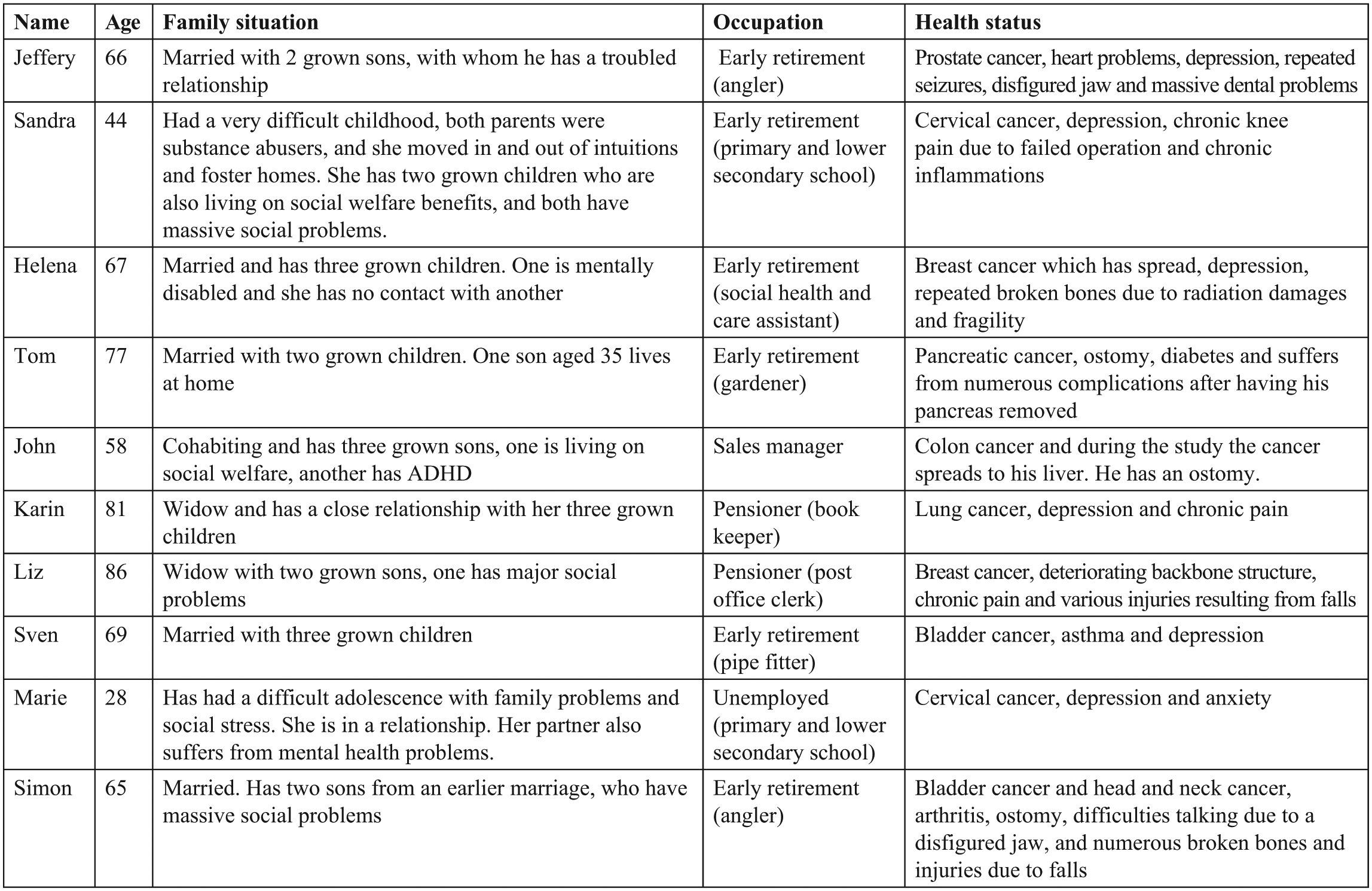
Overview of interlocutors.
Temporal orientation of experience
Karin usually greets Merrild at the door with a blanket around her shoulders. She is somewhat hunchbacked as she moves slowly with jerking movements, leading the way into her small house. Karin is one of Merrild’s key interlocutors. She had half a lung removed due to lung cancer. After the operation, she underwent chemotherapy for more than 2 years, travelling back and forth every week between her home 20 km outside the city and the hospital in the centre of town. The cancer went away, but Karin is still not well. She struggles with shortness of breath because as she says, ‘I’m missing half a lung’. Her voice is hoarse and she coughs a great deal, which pauses her speech and forces her to wait until she is able to return to the conversation. ‘Let’s sit in kitchen today’, Karin suggests, leading me to the small table at the end of the combined kitchen and living room. Merrild helps her set the table with the plates and cups. Karin leans on the table when she reaches for the cups, taking them one at the time and careful not to drop any, perhaps in an attempt not to overestimate her strength. She tells me that she phoned earlier to tell me not to bring any cake as her son (who she refers to as the baker) had been by the day before and he always brings so much cake that she has a tonne of leftovers. She often talks about her children, who play a large role in her life. Her son Patrick, who lives in Texas, is very worried about her. They talk on the phone at least once a week, she says with a smile on her face. Her daughter is also concerned, particularly about the fact that Karin still smokes, and about Karin not getting any exercise. When Karin talks about her daughter, she sometimes starts to cry, for example, if she describes a fight they have had or when she explains how her daughter gives her a hard time about her cigarettes.
Karin has a terrible back pain. She has taken her morphine as usual, but the pills have evidently not done their job today. She is moving with more difficulty than usual, as if every single jerking movement is causing her pain to increase. The difficulty in moving around stems from a combination of chest pain and a fall she had on her bicycle 2 years ago, where she hurt her back, which seemed to have set off an avalanche of health-related problems, such as a failing heart, depression and general weakness. Since the fall, she has not been able to move around like she used to, and now she does not even want to go outside. She is highly medicated, but most of the days, Merrild visits her or talks with her on the phone, neither her antidepressants nor her daily use of morphine and regular painkillers seem to have much effect. Over the past couple of months, Karin has been ailing. On most days, she struggles just to get out of bed and she is in constant pain. Particularly, her chest pain and her cough have gotten worse, and while drinking our coffee Merrild asks Karin what she does when her pain increases:
Well, I was told that I’m allowed to come [to the hospital]. And that I can have radiation, which can take the pain away. But, uhm, they can’ remove it. And then I feel that instead of rushing in there and back again, that I would rather just take the morphine pills. And they say that they’re not that strong. That’s something that Patrick [her son] found out. That this kind is not that strong. Many people in the States use morphine.
Ok, yeah. So, he checked out the morphine. That’s good.
Yeah and, uhm, he has made an appointment with my doctor later this month, so I am going down there for that. I think that it has to do with Patrick wanting to have a follow up done. He wants me to have it checked out again – that rib where my pain is.
He does?
I think that’s it, but I don’t know.
But are you just going down there at your own convenience then?
No, my doctor said that he had made an appointment for me – that I have been referred by Texas … [smiling].
[Laughing]. He said that? Well, that’s great. Then you’ll have to wait and see why you are going down there. When you got sick, was he already living in the US?
Yeah, he’s lived there for 20 years.
Karin no longer attends regular follow-up appointments for her cancer. Initially, the cancer went away, but she continues to worry about it, particularly when she can ‘feel it too much’. However, when we discuss her experiences of her body, she does not seem to be talking about her cancer as much as the pain it causes. Unlike her son Patrick, she does not seem to act on what could potentially be symptoms of relapse, that is, coughing and pain. During their regular phone conversations, he hears her hoarse voice and worsening cough, which he immediately associates with her cancer and directs her to her GP, with concerns about a potential relapse. He is actively involved in her care seeking. Although he is physically far away, he corresponds directly with her GP and vigorously engages in the management of her condition. After being ‘referred to her GP by Texas’, Karin was sent to a lung scan, which showed no radiological changes: I guess I should be happy about that … But it’s hard to believe that it might disappear. I don’t believe that anymore … I guess I have to let them know if it gets any worse. She, the doctor [at the hospital], told me that I should just come back if there was anything … But I don’t think they can do anymore. Except for the pills.
It is not that she does not worry about her cancer. In fact, she hangs onto it still being there and that nothing more can be done. However, her main concern is getting through the day and managing her pain and her more immediate health problems. She often complains ‘My legs, they are so heavy. And my whole body, it just hurts’. When describing her bodily distress and concerns, she does not refer to the cancer, unless directly asked. She seems to experience her body and organise her attention in a disjunctive mode, reflecting how in the context of extreme forms of suffering, it is often the case that individuals have little other choice than to deal with their immediate immersion in the present moment (Throop, 2010: 268). Her disjunctive attention to, and experience of, her body, health and illness override what may be described as a subjectively bounded experience of a long-term illness. As she puts it, ‘I guess I might be too lenient with all that [potential cancer symptoms]. I get so tired of the disease. Also because there’s been so much, right? … I kinda feel like, what’s the point?’ Karin’s temporal attention and experience of her body are tied to the here and now, and she organises her attention in a process resembling what Throop (2003: 234) calls a dynamic structuring of foregrounding and backgrounding. For Karin, this refers to the process where her experience of pain and her daily struggle foregrounds attention to her aching body and encourages her use of morphine to keep the pain at a tolerable level. Her attention to her cancerous body is backgrounded, maybe because there is nothing more to be done and maybe because her pain and daily struggle take up all of her energy and attention. Understanding the temporal orientation of experiences of the body as disjunctive draws our attention to how the immediate concerns, which for Karin may be the constant pain and bodily distress, result in bodily experiences of changes as ‘episodic sequences of events’ (Desjarlais, 1996), more than the unfolding experience of potential relapse symptoms in a cancer trajectory. This is also evident in the way that she responds to temporally oriented questions about the unfolding of her disease. She is unsure about the sequence of her disease-related bodily experiences and does not relate to her bodily decay in a temporally unfolding fashion. Her pain is here and now, demanding her attention. Her own experience of her body does not lead her to engage proactively with bodily changes that might indicate a relapse because in her world of daily struggle, ‘What’s the point?’.
Struggling through everyday life
One central aspect of Karin’s case is the fact that her children play an active role in relation with her care seeking, with her son, for example, organising an appointment for her with her GP. Karin has resourceful children, but many of the interlocutors had less advantaged relatives who also played a decisive role in the management of their care seeking. This was the case for Jeffery, another key interlocutor, who struggled with a wide range of different diseases. Some years back, he suffered what may have been a stroke or an epileptic seizure. His memory has failed him ever since, making him strongly dependent on his diary and his wife, Susan, to keep track of his countless medical appointments. In an average month, he has five to six medical appointments and he is never really sure what they are about. Susan, however, knows and manages his schedule, which means that most of the times Merrild asks him about a medical appointment or visit to the doctor, he has to consult her. Medicated for depression and heart problems, he was diagnosed with prostate cancer 3 years ago and most of his appointments are with specialised hospital departments. When asked about the role his GP plays in his illness trajectory, he says: Well, he was the one who found out that I had cancer. I guess he’s all right. I don’t use him that much because I am not ill, you see. Well, I’m not, so I only use him when I have to use him … I use the hospitals; they are really good. I have to go straight to the hospital if anything happens.
After his stroke, Jeffery stopped working and getting sick has changed him. A large, robust man, he used to work as an angler and spent long periods at sea. He swears a good deal and likes to tell stories about what he has done in life. Most of them refer back to when he was still working on large trawlers but also the time he worked as a town hall keeper. The first interview with Jeffery lasted almost 3 hours. He talked about his illness history, his work life and his troubled relationship with his wife and sons. In contrast to his explicit and detailed explanations about concerns and trouble in many areas of his life, he comments that ‘the cancer alone wasn’t so bad, I was lucky that I went to see my general practitioner that day’. In fact, his experience of living with prostate cancer does not seem to figure much in his mind. Presently, one of his biggest concerns is his constant tiredness and lack of energy as well as the pain and difficulties caused by his teeth. He had an accident on a motorbike at age seventeen, where he broke his jaw and damaged all his teeth. Recently, in the attempt of correcting his jaw, he had massive dental surgery to remove his few remaining teeth. Unfortunately, his new dentures do not fit properly, which means he has only been able to eat liquids for a long period. His biggest concern, however, is his lack of interest in life, being unable to do what he used to do. Like most of the people Merrild interviewed, he seemed to have lost his spark. When he describes how he spends most of his days at home, he speaks in a distant, somewhat irritated, tone, but he lights up when he talks about how he still goes down to the harbour every morning. And twice a week, he has ‘a meeting’ down there, with a bunch of other old men, some who used to fish and some who still do. Down at the harbour, he enthusiastically shows Merrild the small shack where his old nets, hooks, rain gear and oilskin clothes are hanging on the wall. He seems excited when he explains the use of the nets, rods and other equipment. A picture hanging on the wooden wall shows Jeffery far out at sea, holding up a large fish, dressed in orange rainwear, wet and smiling, looking proud and satisfied. He has no desire to be on the ocean anymore, he sighs ‘I don’t feel like it’. Perhaps he is afraid that he will be unable to manage physically. Perhaps he worries that he will not be able to remember what to do, or perhaps he just simply does not feel like it.
Jeffery is not preoccupied about the cancer. It is gone for now and he does not concern himself with it. When he finished his cancer treatment, they told him that if it came back, he would have to return to the hospital. When asked how he would know if it came back, he explains,
Well I have blood tests all the time. I still do. Also at my GP’s, and they also do it at the hospital. I am out there [at the hospital] all the time. Well, not all the time, but I’m out there often enough.
When referring to his blood tests, Jeffery describes how he is tested for all of his medical conditions. He does not feel that he has to worry about potential signs of cancer – he does not trouble himself with that: [B]ecause they [the hospital] keep an eye on me, they do. But all that [the cancer] was part of what made things bad for me. The worst thing is that I’m used to doing a great deal. I have no energy … I can’t even go fishing. It’s terrible. I don’t have the energy and I ought to do some exercise, but I don’t have the strength, I want to but …
Due to his medical affiliations with various departments, it is not clear who is keeping an eye on him and who is regularly taking blood tests. Different departments seem to be performing specific tests with different objectives and diseases in mind. It is all the same to Jeffery, however. Knowing that ‘they keep an eye’ on him, means that he does not have to bother with bodily experiences, which could indicate potential cancer relapse. Understanding Jeffery’s bodily experiences, from the perspective of struggling along, draws our attention to how the urgency of life muddles, or downplays, the experience of a long-term cancer disease trajectory. In accordance with Throop (2003), we argue that understanding ‘the organisation of attention according to the dynamic structuring of what is foregrounded and backgrounded in awareness’ (p. 235) may help us better understand how experiences of the body do not always correspond with what, from an institutionalised healthcare perspective, is considered important. For many of the people Merrild worked with, the bodily experiences that most significantly influenced the practice of their everyday lives, like Jeffery’s teeth, somehow overshadowed attention to the cancerous body. In the midst of struggling along, our interlocutors often appeared to actively disengage from their cancerous bodies because someone – the healthcare system – was overseeing the issue.
Disengaging with the cancerous body
Our interlocutors suffered from various stages and forms of cancer, which means they received different types of follow-up after their initial treatment. However, they shared the same low socio-economic situation regarding income and education, and they were living with cancer while simultaneously suffering from a number of other health problems. Thus, they mirrored the general socio-economic profile, where socially disadvantaged cancer patients are more likely to suffer from additional comorbidities than their more well off cancer peers (e.g. Hovaldt et al., 2015). This meant that they had frequent contact with the healthcare system, for one reason or another. Still, they did not really fit the profile of proactive healthcare seekers, who are expected to take on responsibility for their own illness prevention and management. Instead, their care seeking appeared to be reactive, somewhat contrasting contemporary neo-liberal framings of the independent, productive, self-supporting individual (Bruun et al., 2016). 1 The expectations surrounding proactive care seeking and individual responsibility for preventing disease were not lost on our interlocutors. For instance, when describing the care seeking trajectory that led to a cancer diagnosis, they all stressed the notion of timeliness. When Karin describes her initial care seeking prior to her cancer diagnosis, she repeatedly points out how she waited a long time before contacting her doctor about her cough. When she talks about this, she frowns, shakes her head and almost shudders apologetic and embarrassed. Whether this is an expression of self-blame, guilt or a feeling of failure was unclear, but it underlines the moral and ethical implications of managing the body proactively and attentively. According to Lamb (2014), ‘[O]ur ideas about what it is to be a successful human being over the life course arise out of and are shaped by profound cultural–political visions of who we are as human beings and how best to live’ (p. 51). Our interlocutors were suffering. They were tired, depressed and they seemed disengaged with their cancerous bodies, either because somebody else (the hospital or relatives) kept ‘an eye on’ them, or because getting through the day required all of their attention. When living with cancer, identifying potential signs of recurrence is vital to optimising the prognosis and reducing the risk of adverse disease outcome (Rubin et al., 2015; Weller et al., 2012). However, as already suggested, in the face of pain and illness, people often ‘have little other choice than to deal with their immediate immersion in the present moment’ (Throop, 2003: 234). Liz, an 86-year old retired postal worker explained ‘A disease like cancer wears you out’. Liz’s last breast cancer operation was in 2014 and she underwent radiation treatment again last year. She has a pile of invitations to various follow-up tests and exams at the hospital. Her son helps her with her medical appointments and tries to keep track of when she has to go to the hospital. ‘I don’t know how I would deal with all this without him’, says Liz, who is disabled by her deteriorating backbone, a situation made worse when she fell in her bathroom a few years back. She broke part of her spine and she still suffers from exhausting, chronic pain. Most days, she sleeps at lunchtime and when Merrild visits, she forgets about the appointment and opens the door looking dazed and confused – woken up by the doorbell. Liz does not know if the cancer is gone and that worries her. As with many of the other interlocutors, it is often hard to make out whether Liz is talking about cancer, her back pain or her swollen lymph nodes, the bulge of skin growing under her arm or the lumps in her breast, when she describes her health problems. It is all a blur, which yet again prompts the question of how people who are sick and suffering experience their bodies and how this corresponds with proactive healthcare seeking.
Let us introduce our final case, namely that of Simon, who was first diagnosed with bladder cancer 5 years ago. He went through a long, difficult recovery, but almost immediately after he got through it, he was diagnosed with tongue cancer. Although it is all gone now, the cancer has left him with a radically changed body. He has an ostomy, a hole in his jaw, less than half of his tongue and a single pointy yellow tooth raising up from his lower jaw. With the exception of the ostomy, his bodily disfigurements are due to radiation treatment, he says, drying a bit of protein shake from his chin, which drips from the corner of his mouth every time he takes a sip. ‘He is unable to keep food in his mouth, and he is waiting for reconstructive surgery’, explains his wife Anna, looking slightly embarrassed. His speech is slurred, making it difficult to understand him. Anna has to translate much of what he says or render it understandable, and she often helps him remember. ‘Before the cancer he was never ill’, she says. ‘He was always the kind of man who went to work even if he had the flu’. We are sitting in their small, sparsely lit apartment at the kitchen table, which is set with cups and small plates. Anna has made coffee and there is a lavish amount of cake and chocolate, all of which is apparently for Merrild as Anna does not eat anything, and Simon sticks to his protein shake and a can of beer. Simon used to work as an angler, then as a bricklayer, later a scaffolder followed by a range of other odd jobs. But now he does not socialise anymore. Many of his relations were grounded in his work life, and he does not want to leave the apartment, as he worries that his ostomy might leak. The massive changes in his body due to cancer-related surgery and radiation therapy have left Simon with a disfigured body. After having fed on a liquid diet for a long time, he has lost a lot of weight and he has trouble moving around. It is hard to imagine that the small, weak, hunched up man sitting across the table has performed hard manual labour his whole life. When asked to tell his story, Simon begins by sighing, ‘Well, there’s been a bit of a price to pay over the past year’. Encouraged to explain, he embarks on a long narration of all the accidents and bad luck he has had, starting with a broken thigh bone when he fell in the bathroom last year. The hospital was unable to fix it properly, which means it remains broken and is not correctly attached. Unable to help him, the hospital explained that it had to grow back at its own pace, which means it is still unhealed and continues to hurt terribly. He is reluctant to take painkillers to numb the pain, but sometimes, he has to do it: ‘I’m not fond of it [taking painkillers]. I’m okay but … Well, there’s been so many accidents’. Simon exhales as he describes how he was caught between the sliding doors of a bus 7 weeks ago on the way to the dentist. He hurt his knee, hip and finger, and ended up with a cast for 6 weeks. Anna elaborates, I got off the bus before him and, well, usually he gets off the bus on his own, right? When I turned around, there he was, lying on the ground by the door. The driver, he came running out. Luckily the emergency room was right nearby.
There is a surplus of stories like this in the narrations of Simon and Anna. Despite a persistent effort to focus the conversation on Simon’s cancer, Merrild has difficulty in doing so. It seems like the questions asked in the attempt to learn more about what life is like after being diagnosed with cancer do not really resonate with Simon; they seem somehow out of place. Simon and Anna’s preoccupation with the urgency and desperation of Simon’s broken body somehow makes the cancer seem secondary. Simon is struggling along. And like Liz, Jeffery and Karin, his bodily experiences appear fragmented and disjunctive, caught up in the here and now. Unfortunately, Merrild never gets the opportunity to go back and follow-up on her questions, find out how the reconstructive surgery went and spend some more time with Simon and his family. About a month after this interview, Merrild calls him up and his son answers the phone, ‘My dad is very ill, and he is only awake in the morning’. Merrild tries to call back in the morning a few times, but with no luck. Suddenly, his phone is disconnected and it remains turned off. After enduring a long life of hard manual labour and two rounds of specialised cancer treatment, his body is now apparently succumbing to side effects, accidents and disease.
The bodies of Simon, Karen and others who live on the fringe of the welfare society were destabilised and shaped by temporality and haphazard episodes, like being caught in the sliding doors of a bus or falling on the bathroom floor. Being poor, sick and moving towards the end of life may be conducive to a way of being in the world and experiencing the body where the struggle to get through the day requires all the energy and attention one can muster. To paraphrase Desjarlais (1996: 87), a good day for someone who is struggling along might be one where no accidents happen, where one is left in peace to rest and where the pain is endurable. Lives such as these are many times unknown, or perhaps unrecognised, and rarely understood, by the dominant, mainstream middleclass. The way of talking, the body language, the narration of the haphazardness and unfolding of unfortunate events, the social and family-related problems stimulate an odd feeling of familiarity. Merrild recognises the world that Simon and the other interlocutors live in. She has encountered his world before, many times, in previous work with lower working-class Danes. It is a world that is as far removed as one could possibly imagine from that of early disease detection, proactive attention to the body, health promotion and illness prevention. A world which is sometimes overlooked by the good intentions of the welfare state, where increased individual responsibility for maintaining good health, preventing (deterioration of) illness and maintaining the body, requires self-monitoring and early, proactive care seeking. Perhaps what Susan Whyte refers to as scaling can assist us when we try to understand. Drawing on her work with disability in Uganda, Whyte (2019) describes what she coins the temporality and scale of lifetimes. Lifetimes are human scale – informed by life projects, values and hopes, and constrained by the possibilities of situated persons. The situatedness of human scales, Whyte argues, are sometimes contrasted in the scales of the episodic time of interventions, broad shifts in historical time, or in this case, the values of progressivity, optimisation and urgency of early diagnosis and institutionalised healthcare.
Conclusion
This article feeds into ongoing discussions on the changing politics of responsibility in the context of neo-liberal welfare (Merrild and Andersen, in press). In the context of the growing expectations of proactivity placed on the individual patient, we argue that the ways in which people who are sick and suffering experience their bodies and seek care do not resonate with the scaling of awareness and timeliness represented by institutionalised healthcare. Drawing on the example of the changing organisation of cancer follow-up, where patients, in close collaboration with their GP, are expected to play a key role in identifying potential signs of recurrence, we suggest that people do not always experience their bodies in a linear, forward-moving process, but in a disjunctive manner, largely influenced by the practicality of getting through the day. They leave the management of their cancer in the hands of significant others, saving their strength for what is right in front of them. Our interlocutors’ engagements with their bodies and with the healthcare system may perhaps best be described by a sense of pragmatism, as alluded to by Wilkinson and Kleinman (2016) who argue, [T]here is little doubt that while struggling to relieve bodily pains and discomforts individuals are compelled to examine and revise their behaviours and forms of interaction with others. Managing experiences of illness and physical impairment tends to absorb people in the overwhelming practicality of life. (p. 128)
The suffering of people like Simon, who are traumatically affected from cancer, who are poor and unable to continue their work life, intricately reflects how physical, mental and social aspects intermesh. Simon’s pain and his ability to speak and partake in meals (the latter a social signifier in Danish society) are not easily separated from the shared pain that he and Anna experience due to a pending loss of life. Considering experiences of the body as episodic sequences of events draws attention to how the perspective of struggling along may help us better understand what it means to live with illness-ridden bodies in difficult social circumstances. The notion of struggling along brings forth the temporality and instability of everyday life when living in fragile, uncertain situations. It teaches us about the urgency, destitution, pain and suffering that shape experiences when being sick and poor, which is essential knowledge for practitioners working in healthcare systems that move towards individualised and responsibility-driven care of the self.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research for this article was financially supported by the Danish Cancer Society, grant number: R137-A8773-00-S3.