
Abstract
Contemporary health research often examines patient objectification, patient self-objectification, and good patient performance as separate concerns. Treating them in isolation makes it difficult to see how they combine to shape what patients feel able to express in clinical encounters. To address this gap, this study examines how cancer survivors describe objectification, internalization, and performance within oncology care. Through this analysis, we develop a unified analytic account of these three experiences. In doing so, we reframe the “medical gaze” in existential terms as the “medical look,” by drawing on Sartre’s account of how becoming visible to another reshapes lived experience and existence. We interpret clinical visibility as a structure that unfolds across encounters, rather than as isolated interactional events. Drawing on 29 interviews with cancer survivors, our findings show that being positioned through clinical routines, adopting those framings as self-measures, and calibrating self-presentation in anticipation of clinical judgment were lived as connected movements within one structure of visibility. Recognizing this continuity clarifies communication pressures and constrained agency in oncology, and identifies points where clinical practice may ease the conditions under which patients manage how they appear.
Keywords
Introduction
Across qualitative and sociological research, two major strands of scholarship have examined how clinical encounters shape patients’ thoughts and behaviors. One strand, drawing on Foucault’s theory of the medical gaze, analyzes how routine clinical procedures objectify patients as cases and how these objectifications are internalized over time (Mol, 2002; Timmermans and Berg, 2010). A second strand investigates how patients attempt to present themselves as “good” or credible in order to be taken seriously, emphasizing how cooperation and deference influence whether clinicians judge them as trustworthy or compliant (Dudley et al., 2024; Matthias et al., 2010).
Although each body of work has advanced understanding in important ways, a central gap remains. Research on objectification and internalization and research on being a good patient have developed in parallel without an analytic link between them. Without such a link, the relationship between objectification and patient self-presentation remains analytically underdeveloped.
To address this gap, the present study examines how cancer survivors describe experiences of objectification, internalization, and patient performance within oncology care. Through this analysis, the study reframes the medical gaze in existential terms as the medical look. The analysis traces how these three movements unfold and interrelate across clinical encounters over time. Drawing on Sartre’s (1943/1956) existential account of the look, in which becoming visible to another alters one’s mode of being, the study interprets performances of doctorability as emerging from prior experiences of objectification and internalization, rather than as isolated interactional strategies.
Literature review
This review draws together bodies of research that address how clinical encounters – broadly considered – shape patients’ visibility, credibility, and agency, before narrowing to oncology as the context of the present study. Section “Objectification and internalization under the medical gaze” examines studies of the medical gaze, which show how institutional routines objectify and reorganize patient experience (Mol, 2002; Wolf et al., 2012). Section “Doctorability, credibility work, and the performance of being a good patient” turns to research on doctorability and credibility work, which examines how patients manage self-presentation to secure recognition within clinical settings (Dudley et al., 2024; Matthias et al., 2010). Section “Cancer survivorship, communication pressures, and convergence” then considers communication scholarship in cancer survivorship, where the identified pressures often converge and intensify under surveillance and time constraints (Li et al., 2020; Smith et al., 2024). Finally, section “The unresolved gap” brings these strands together and clarifies the unresolved gap addressed by the present study.
Objectification and internalization under the medical gaze
Qualitative and ethnographic work has shown how diagnostic categories, documentation systems, and workflow constraints organize patient encounters in ways that translate persons into manageable cases (Bishop and Waring, 2019; Mol, 2002; Wolf et al., 2012). Routines of measurement and templated reporting can narrow what becomes visible, while related work on digital self-tracking shows how data practices may also generate algorithmically mediated identities (Lupton, 2019). Radiology and laboratory studies further illustrate how protocols render experience into coded data, which reshapes what clinicians can register as meaningful (Rogers et al., 2023).
These dynamics do not remain external to patients. A growing body of work shows that objectification can migrate inward and influence self-understanding and expectations for care (Davidsen et al., 2023; Tjernström et al., 2024). Telecare and digitally mediated settings can intensify this process, encouraging forms of responsibilization or acquiescence to clinical framings (Heavey et al., 2019; Pols, 2012). Phenomenological scholarship further clarifies how clinical practice makes the body salient as an object for scrutiny and interrupts ordinary modes of orientation (Carel, 2016; Grīnfelde, 2023; Leder, 1990, 2022; Zeiler, 2010).
Although this work demonstrates consistent patterns of objectification and internalization, it rarely traces how these movements structure the later performances patients adopt in response. The result is a detailed account of how patients come to inhabit clinical categories, but an incomplete account of how they subsequently act within them.
Doctorability, credibility work, and the performance of being a good patient
A second body of research examines how patients calibrate their conduct to remain credible within institutional expectations. Conversation analytic studies show that patients design narratives to present troubles as medically appropriate and to avoid disrupting clinical agendas (Heritage and Robinson, 2006; Kushida et al., 2020). In domains marked by diagnostic uncertainty or mistrust, such as chronic pain, patients work to appear responsible and non-demanding to avoid dismissal (Matthias et al., 2010, 2014). Ethnographic work conceptualizes these adjustments as credibility labor, that is, the ongoing work of sustaining legitimacy under clinical and moral scrutiny (Dudley et al., 2024; Werner and Malterud, 2003).
Furthermore, these performances are often anticipatory. Patients regulate emotion, suppress concerns, or reshape accounts of symptoms anticipating how clinicians will interpret them (Pols, 2012). Communication studies observe that such strategies can constrain disclosure when patients fear damaging rapport or appearing difficult (Kushida et al., 2020).
Despite its depth, this literature typically takes performance as its starting point. It examines how patients present themselves, but rarely asks how such performances become necessary in the first place. As a result, credibility work is treated as a strategic response rather than part of a larger experiential trajectory.
Cancer survivorship, communication pressures, and convergence
Cancer survivorship provides a setting in which these pressures consistently converge. Follow up care involves surveillance scans, structured appointments, and time constraints that reinforce expectations of optimism and compliance (Miller, 2012; Smith et al., 2024). Survivors often withhold concerns or reshape narratives to fit these norms or to conserve limited clinical time (Li et al., 2020). Other studies describe how being reduced to recurrence risk scores or scan results influences the language survivors use to describe their bodies and symptoms (Rogers et al., 2023; Shilling et al., 2017). In sum, this work shows that survivorship carries persistent communication pressures shaped by both institutional routines and expectations for self-management.
The unresolved gap
Even with these contributions in view, the literature still does not fully explain how these pressures relate to one another across encounters. Research on objectification and internalization demonstrates how clinical categories and routines reshape patients’ self-understanding, but it does not follow how these shifts inform later self-presentation. Studies on credibility and doctorability examine how patients manage their appearance as cooperative or credible, yet rarely trace how these strategies emerge from earlier experiences of being positioned as objects within clinical routines. Communication scholarship in cancer survivorship shows that these pressures converge in practice, but it has not yet provided a framework for understanding them as interconnected movements within a single experiential arc. The literature therefore still lacks a theory that treats objectification, internalization, and the performance of being a good patient as interconnected movements across encounters.
The present study addresses this gap by examining how cancer survivors describe transitions from being objectified, to internalizing clinical framings, to performing as cooperative or credible patients. Through this analysis, the study reframes the medical gaze in existential terms as the medical look. By bringing these strands into a single conceptual account and employing a phenomenologically informed qualitative method, the study clarifies how institutional routines, surveillance structures, and credibility expectations combine to shape what patients feel able to say and do.
Conceptual framing
Before turning to the methodological approach, we first clarify the conceptual framework of this study. Our investigation draws on Sartre’s (1943/1956) analysis of the look (le regard), which names a shift in being that unfolds when I apprehend myself as visible to another. In what follows, we briefly outline the look as Sartre develops it in its general, existential sense. While Sartre identifies multiple different ways to experience the look, we focus on three ways or expressions of the look that are most relevant for the present study. These are objectification, internalization, and performing. After clarifying these three expressions in their philosophical form, we then show how these philosophical ideas provide the conceptual framework for our qualitative investigation of clinical visibility.
First, objectification names the moment in which an other’s (≈ another person’s) perspective is imposed upon me and defines how I appear. Sartre describes this first moment as the awareness of being looked at – of realizing that the other now defines how I appear. In this instant, I sense myself as seen through the other’s eyes rather than my own. I am no longer simply the one who acts or speaks, but someone who can be examined, known, or handled (Sartre, 1943/1956: 358–362). What changes is not what I see, but who I am. To be looked at is to undergo a transformation in being – to find oneself defined from outside.
For Sartre (1943/1956), this shift means that “the self exists at the same level as worldly objects” (p. 349). Under the look, the person becomes something observed, measured, and interpreted within it. More specifically, the look makes me an instrument for the other. As an instrument-object, my possibilities are no longer self-given. Instead, they are assigned from without. I am no longer the one who determines what I am capable of doing or being. Like any implement, my use is set by the one who employs me – here, the other. I am to be used toward the other’s ends, and my possibilities are conferred by that use (Sartre, 1943/1956: 366). Simply stated, Sartre’s conclusion is that my entire being is taken up within the other’s projects – interpreted, positioned, and deployed as a functional element in the pursuit of ends that are not my own.
This first expression of the look names only the initial imposition, where the other attempts to make me an object. According to Sartre, the transition to a second expression occurs when the other’s view no longer stays outside, but is taken up from within, that is, when I accept and internalize the other’s definition of myself and my abilities as an instrument-object. In this acceptance and internalization, I see myself as the other’s instrument and understand my possibilities and abilities as those conferred by the other. Sartre (1943/1956) thus straightforwardly writes, “I learn of my possibilities from outside and through [the other]” (p. 361). Here, the external gaze becomes an internal horizon through which I interpret myself and my agency (Sartre, 1956: 374, 388).
Finally, Sartre identifies a further expression of the look that arises once objectification has been accepted inwardly. After being apprehended through the look and having taken that framing into myself, I may try to regain a sense of control by perfecting the object the other has defined me as. Sartre calls this expression “vanity,” though this paper will more neutrally term it, “performing” for the look.
This expression of performing does not stand apart from objectification and internalization, but rather extends them. Once I have been objectified and have taken that objectification into myself, a new kind of activity can arise within the same mechanism. When performing for the look, I may act freely, but that freedom is bound to the framework of my objectification. My efforts confirm and sustain the same image that first diminished me. After accepting how I have been seen, I begin to refine that image, striving to embody it completely and convincingly. I thereby reclaim a sense of control, but only by becoming the best possible version of the instrument-object the other has made me out to be. For Sartre, this is the contradiction at the heart of performing for the look. The contradiction Sartre identifies is not between freedom and subjection as separate forces, but within the same action. Freedom turns back upon itself, exercising agency through the very image that binds it.
In our current society, the reason Sartre calls this expression “vanity” becomes clear when placed in the context of beauty. In a case where the other objectifies a person as beautiful – if that person is “vain” – they may then seek to present themselves as beautiful as possible in hopes of gaining favor or approval (Sartre, 1943/1956: 394). This example helps to clarify that when performing for the look (or for Sartre, in vanity), freedom shows itself through submission. The person does not escape the look, but performs within it, thereby sustaining the very structure that first defined them.
Sartre’s theory of these three expressions of the look can help clarify how visibility reorganizes self-relation at the level of lived experience. The present study extends this account into the clinical domain by examining how such visibility is lived within medical encounters. Critical to note here is that Sartre’s emphasis on lived transformation differs from dominant analyses of clinical visibility that focus primarily on institutional arrangements of knowledge and power. Indeed, clinical visibility is frequently examined through Foucault’s account of the medical gaze (le regard médical), which analyzes how medical institutions historically produce a field of observation in which bodies are classified (Foucault, 1973). Foucault’s concern lies with the formation of regimes of knowledge and authority. By contrast, the present study examines what occurs in self-relation when one apprehends oneself as visible within such a clinical field. Whereas Foucault clarifies how medicine produces visibility, the present analysis investigates how visibility is inhabited. We accordingly appropriate Sartre’s “look” (le regard) as the term “medical look” throughout the rest of this paper to emphasize the experiential and existential dimension of clinical visibility, rather than its institutional formation. The following section outlines the methodological approach through which this account was developed.
Methods
Design
This interview study employed a concept-led qualitative design (Byrne, 2026a, 2026b). The purpose of the design was to examine how cancer survivors describe clinical encounters when interpreted through a defined conceptual framework. The study was not structured as hypothesis testing – nor did it proceed through inductive theme generation. Instead, the design began from specified existential distinctions and examined how those distinctions were expressed in participants’ accounts of care.
The conceptual framework for the study was Sartre’s (1943/1956) analysis of the look. In the present investigation, the look was specified in three expressions: objectification, internalization, and performing. These distinctions did not function as variables to be tested. They functioned as orienting concepts that structured interview construction and guided analytic attention.
In order to examine the existential dimension of clinical visibility, the study adopts a phenomenological-existential method. Specifically, we investigate the medical look by employing the method, “Phenomenologically Directed Qualitative Research” (PDQR; Byrne, Under Review). PDQR begins from clarified existential concepts and distinctions to orient the research question and structure the design (Byrne, 2025a, 2025b; Køster and Fernandez, 2023; Stilwell et al., 2025). In this sense, PDQR treats phenomenology not just as a method applied to data, but as the generative ground from which inquiry itself begins. In what follows, we outline the central tenets of PDQR and explain how this method directed our study.
PDQR takes its methodological point of departure from the phenomenological distinction between the invariant basic conditions of life and the varied expressions through which these conditions are lived (Heidegger, 1927/1962: 81–83).
These basic conditions – which Heidegger calls “existentials” – constitute the fundamental structures that make any relation to the world possible. Basic conditions are not mental states, behavioral tendencies, or social constructs, but the structural arrangements that make any experience possible. For instance, agency refers to the basic condition of being able to act – to initiate, respond, or resist (Heidegger, 1927/1962: 95–105). Another example of a basic condition is spatiality. Human life always unfolds in a world already organized by nearness, distance, direction, and possibility (Heidegger, 1927/1962: 134–147). The present study centers on one such basic condition – the look. Although the look may initially seem to demarcate a particular encounter, we take the look as a constant structure of existence. We understand the look as the way in which one becomes aware of being seen and thus of oneself as visible. Far from being a fleeting event, we believe that the look is a persistent dimension of life that shapes how selfhood is lived and exposed to others. Indeed – according to Sartre (1943/1956) – the other need not be physically present for one to experience the look (pp. 380–383, 386). The mere apprehension of oneself as visible to another is sufficient to provoke this shift (Toombs, 1993: 58).
While the basic conditions of life form the enduring framework of existence, they never appear in a single or uniform way. Instead, there are varying expressions of these basic conditions. Each basic condition is expressed within the shifting realities of social, spatial, and institutional life. PDQR treats basic conditions as dynamically lived via their expressions, rather than theoretically fixed. PDQR emphasizes that their significance always arises in and through context (Heidegger, 1927/1962: 172–181; Køster and Fernandez, 2023: 153). The experience of agency, for instance, may be expressed as expansive in moments of freedom, yet expressed as constricted when circumstances impose limitations (Sartre, 1943/1956: 482–500). Spatiality, likewise, can be expressed as opening onto a larger world or expressed as a feeling of enclosure, depending on how one inhabits the world (Heidegger, 1927/1962: 136–145). The look, too, takes different shapes: it can be experienced as objectifying from without, as objectifying from within, or as that under which one performs. Although the present study draws on Sartre’s account of these expressions as objectifying, alternative phenomenological interpretations have argued that the other’s look need not always be objectifying in this way (Leder, 1990: 94–95). Our aim here is not to resolve that broader theoretical question, but to clarify the objectifying forms of visibility that were most salient in participants’ accounts.
As an empirical method, PDQR examines how basic conditions become apparent through their expressions in lived encounters. PDQR does not treat these expressions as traits to locate in transcripts. Instead, PDQR uses clarified distinctions as an orienting framework for interview design and analytic attention. Interview questions for this study were therefore structured to invite accounts of moments when expressions of the medical look became salient, whether imposed from outside, taken up from within, or enacted through calibrated self-presentation.
Study context
This study was conducted within the United States in the context of contemporary biomedical oncology. All participants received care within the American high-income oncology system. Oncology carries structural features that may intensify the dynamics examined here. Cancer diagnosis relies heavily on imaging and staging practices that render the body as lesion or progression. Treatment is often invasive and prolonged, and prognostic communication frequently centers on survival statistics. Cancer can also involve visible bodily change, chronic pain, and explicit confrontation with mortality (Byrne et al., 2025b). These conditions may heighten experiences of objectification, internalization, and performance within clinical encounters. Oncology is therefore not treated as a neutral example of medical care in general, but as a domain in which the medical look may be especially pronounced. Whether similar structures emerge in other specialties remains an open empirical question.
Recruitment and sample
Participants were recruited using purposive sampling with convenience access points and snowball extension. Initial recruitment took place through three institutional access points in one Midwestern region of the United States. Flyers were distributed at in-person meetings of a Cancer Research Advocacy Group – which is led by one of the authors – and were also placed in two oncology clinics at two hospitals. Interested individuals contacted the research team by scanning a QR code linked to an intake form, which assessed eligibility, including age 18 years or older, self-reported cancer diagnosis at any stage, and fluency in English. No restrictions were placed on cancer type or treatment status. Participants also referred others who met eligibility criteria, extending the sample across multiple U.S. states, although all recruitment remained within U.S. oncology settings.
Data collection
Each participant completed a brief demographic questionnaire followed by a semi-structured interview conducted over Zoom or in person – depending on participant preference and accessibility. Interviews focused on concrete clinical encounters in which participants described how they were seen, how they understood themselves, and how they adjusted their conduct in anticipation of clinical response. The semi-structured guide used broad, concept-oriented prompts, with follow-up questions used flexibly to clarify and deepen participants’ descriptions. Representative interview questions are provided in Supplemental Material 1. Interviews lasted between 45 and 90 minutes, were audio-recorded and transcribed verbatim, and were conducted between January and August 2025.
All identifying details were removed during transcription. Each transcript was checked against the original audio recording for accuracy by two members of the research team. Audio files and transcripts were stored in a password-protected Box folder on the Unviersity of Illinois Urbana-Champaign’s system accessible only to the research team.
Analysis
Data were analyzed using PDQR (Byrne, 2026b; Charmaz, 2004; Køster and Fernandez, 2023; Stilwell et al., 2025). Rather than generating themes inductively, transcripts were examined in light of the defined expressions of the medical look – objectification, internalization, and performance – to determine how these structures appeared and shifted within participants’ accounts
After de-identification, each transcript was read holistically and then event-by-event by team members trained in PDQR. Analysts wrote brief memos identifying passages in which visibility, recognition, or objectification became salient and articulating the shift in self-relation evident in the text. These memos documented interpretive decisions.
To render judgments intersubjectively examinable without reducing them to thematic codes, we applied a focused set of sensitizing markers aligned with the three expressions. Objectification was marked when participants were positioned as cases or body-objects through measurement or protocol. Internalization was marked when participants adopted those frames as self-measures. Performance was marked when narration oriented toward anticipated recognition – adjusting self-presentation to appear credible or cooperative. Each marker was accompanied by a brief written warrant.
Interpretive meetings reviewed warrants, refined distinctions, and returned to transcript language to adjudicate boundary cases. Cross-case displays tracked how expressions emerged within encounters and across participants. Findings are presented as interpretive developments grounded in exemplary passages, rather than thematic categories.
Researcher positioning
The research team approaches this study from a background in existential phenomenology and prior work using PDQR. All analysts had completed advanced training engaging Husserl, Heidegger, and Sartre. This shared formation informed analytic sensitivity and shaped the kinds of interpretive questions brought to the transcripts. Such training was not a formal requirement of PDQR, nor does the method presuppose mastery of specific canonical texts.
Philosophical concepts were not treated as presumptively confirmed in the data. Interpretive meetings focused on whether and how the defined expressions of the medical look were demonstrably present in participants’ accounts. When prior commitments risked extending beyond the data, alternative readings were considered and adjudicated through close return to transcript language. The aim was not philosophical verification, but examination of empirical expression.
Ethics
The study was approved by the Institutional Review Board at the University of Illinois Urbana-Champaign (Protocol #IRB24-2216). Prior to participation, individuals received written information outlining the study purpose, procedures, and voluntary nature of involvement. Written informed consent was obtained before interviews began.
Given the sensitive nature of discussing cancer care experiences, participants were reminded that they could decline to answer questions or withdraw at any time without consequence. Interviewers were attentive to signs of discomfort and paused or redirected conversation as needed. At the conclusion of each interview, participants were provided with information for national and local cancer and mental health support services.
Findings
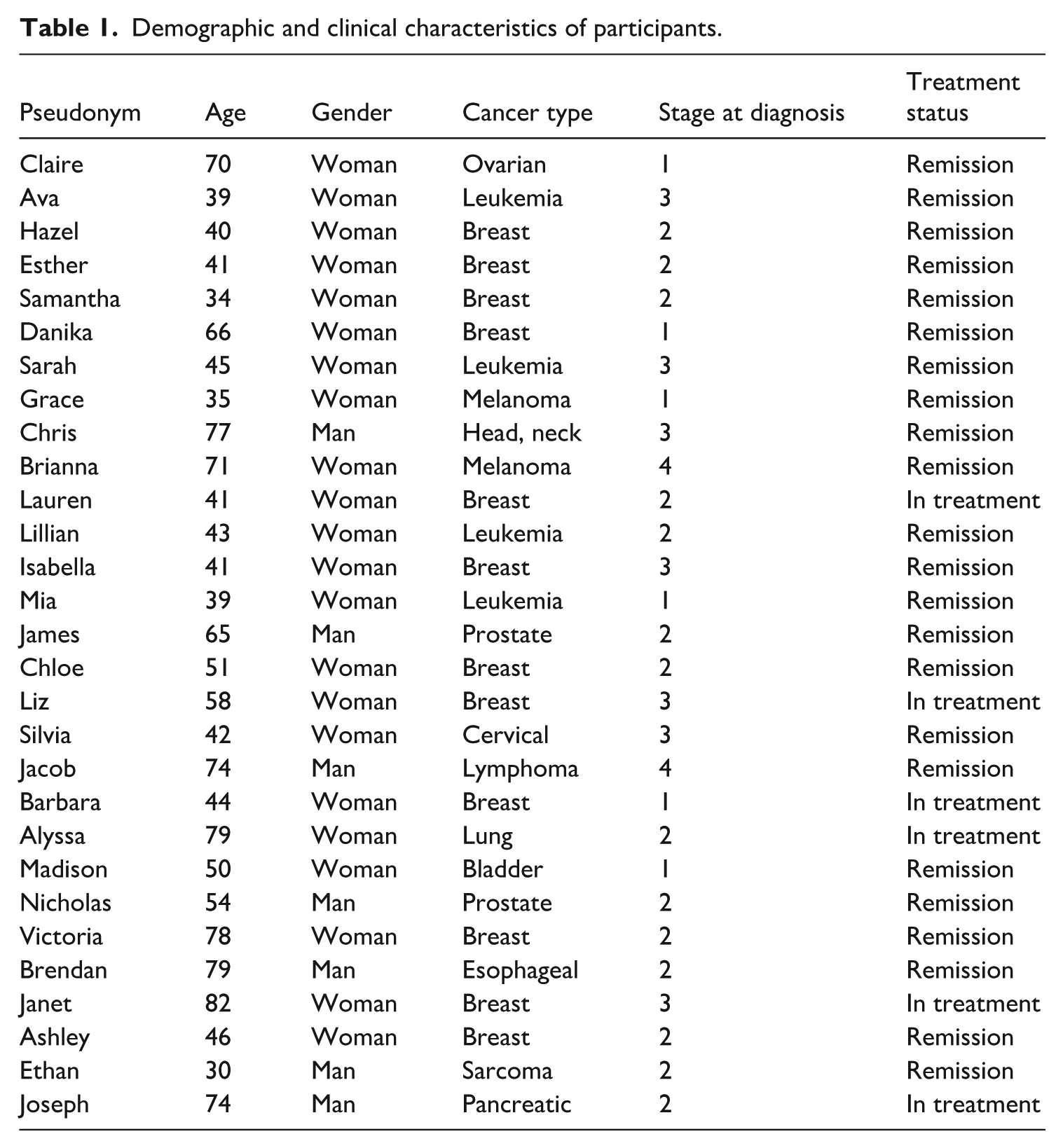
Twenty-nine individuals completed both the demographic questionnaire and the in-depth interview and are included in the analysis. The sample included individuals across stages of diagnosis, treatment, and survivorship. Participants were predominantly White and middle- to upper-middle class. While snowball sampling increased geographic range, socioeconomic diversity remained limited. For full details concerning demographic and clinical information, see Table 1.
Demographic and clinical characteristics of participants.
The following findings present participants’ descriptions as interpreted through Sartre’s account of the look (Byrne et al., 2025a; Køster and Fernandez, 2023: 161–163). Objectification, internalization, and performing function here as analytically distinct yet interconnected expressions of what Sartre identifies as a single structure of visibility. These expressions are not treated as discrete empirical categories, but as manifestations of one clinical dynamic – the medical look – as it was lived within oncology care.
Among the 29 participants, 22 described experiences consistent with at least one expression of this structure. Several also described collaborative, person-centered encounters not organized by the medical look. The analysis that follows reflects the predominant pattern rather than all clinical situations.
Objectification
Sartre’s account of the look provides the analytic lens for understanding how the medical look was first lived by participants. The first expression – objectification – refers to becoming visible as something perceived and positioned within the clinical field, rather than as the one directing the encounter. Participants described being assessed, measured, and arranged within institutional routines in ways that shifted their sense of agency. Seventeen of 29 participants narrated experiences consistent with this form of objectification, often as a sudden awareness of being positioned as something perceived rather than as someone who perceives. Several described unambiguous, even extreme, forms of this expression. As a first example, “Esther” (pseudonym) recounted being apprehended not as a person, but as a pathology – the fixed object of the clinician’s view: Because, again, I felt like [the doctor] was treating me as if I were just another tumor. Just a tumor. He was already on to the next step while I was still talking. And I remember thinking. . . just, okay, I’m the tumor today.
While Esther’s description plainly captures the first expression of the medical look, as Sartre emphasizes, the one who is looked at does not become just any object, but an instrument. “James” (pseudonym), for example, recalled his biopsy as one step in a coordinated chain of procedures, describing how he felt treated less as a person than as a component in an operational system: When I was going for the biopsy, there’s this long line of stretchers. All these guys getting biopsies the same day because the doctor only does them one day a week, fifteen minutes each. So it’s like, okay, next, next, next. A biopsy assembly line . . . They don’t really even talk to you [about the biopsy] personally. They just show you a video of what the biopsy is. And we [all of the patients in the line] were all watching it at the same time . . . It was a little bit dehumanizing.
A still more explicit instance of this instrumental relation appeared in “Lillian’s” (pseudonym) account. Her oncologist not only defined her actions, but positioned her as someone to be directed and controlled – an implement within the physician’s own project of treatment, rather than an agent in her care: I was told to do [a treatment] 5 times a day. I saw no justification for why five times a day. And I have a hard time remembering twice daily medications, and I was like 5 seems like a lot. I thought it through and couldn’t see justification for that. And I said I think this is burdensome and my oncologist said, and I quote, my doctor told me, “You’re a cancer patient, you’ll do whatever I tell you.”
Together, these accounts illustrate the first expression of the medical look: becoming visible as something observed, assessed, and incorporated into clinical routines as an instrument-object. These experiences also structured how participants would later assess themselves and act within care.
Internalization
The second expression of the medical look – internalization – occurs when the look is no longer experienced as merely imposed from outside, but is taken up within self-understanding. In Sartre’s terms, the other’s evaluation becomes a reference point through which I come to interpret my own possibilities. The clinical frame is not only applied to the patient, but adopted by the patient.
In participants’ accounts, internalization appeared when medical classifications, measurements, or prognostic judgments began to shape how individuals understood their own bodies and capacities. Participants described evaluating themselves through diagnostic language, doubting perceptions that diverged from clinical results, or deferring to medical interpretations over their own lived experience. What began as external positioning became a mode of self-relation.
Thirteen of 29 participants narrated experiences consistent with this expression. For example, when experiencing pain that contradicted her test results, “Mia” (pseudonym) subordinated her own perception to the clinician’s interpretation, accepting the medical account as more authoritative than her lived experience: He [the doctor] told me like, “Your labs look fine.” I was like in so much pain, but the results had always been right before, so I like told myself that it must be ok. I thought he knew what he was doing.
“Victoria” (pseudonym) offered a closely related account, describing how her doctor’s directive not only silenced her curiosity, but also reshaped her sense of self. By identifying with the compliant patient her physician preferred, she came to experience submission as a kind of safety: When she [my doctor] said to me, “Don’t Google things; that just confuses you,” I just stopped reading about it. I felt like I wasn’t like qualified to know about it. And honestly, it made me feel safe to trust her.
Across participant accounts, the medical look operated through the meanings patients applied to themselves. Clinical interpretations and evaluative standards became part of how participants oriented to their bodies and futures. This shift provides the background for the third expression, where persons act in anticipation of how they will be perceived.
Performing
A third expression of the look – performing – arises when objectification has been accepted inwardly and becomes the basis for action. In Sartre’s account, once I have taken up the other’s framing of me, I may attempt to reclaim agency by perfecting the image through which I am seen. Performing does not break from objectification and internalization. Rather, it intensifies them. Agency is exercised, but within the terms already set by the look. In many accounts, this performance did not appear as overt self-assertion, but as the active enactment of passivity. Participants often described trying to appear calm, cooperative, and non-disruptive, thereby refining and sustaining the very role into which they had already been positioned.
In clinical encounters, performing appeared when participants sought to manage how they were perceived by their clinicians. After being positioned as cases and adopting that framing, some described adjusting their conduct to align with medical expectations. Rather than resisting the doctor’s authority, they worked to appear cooperative, credible, and disciplined. Participants described striving to embody the “good” patient in hopes of securing stability, approval, or more attentive care.
Nine participants narrated experiences consistent with this expression. The pattern was especially clear in “Claire’s” (pseudonym) account, where conformity became a deliberate strategy for securing care. She explained that she believed compliance would be rewarded – that if she appeared calm, trusting, and easy to treat, she would be viewed more favorably and receive better care. In performing this composure, she sought control not by resisting medical authority, but by managing how her objectification was perceived: I just put it in his [my doctor’s] hands and I did whatever he said. My sort of philosophy was he [the doctor] knows what he’s doing and I’m just [going to] sit back and let him do whatever. I thought that if he knew I trusted him, he would help me more and give me the best things [the best treatments]. And now that I know more . . . it’s not that I would necessarily change what happened, because it was very straightforward. I’ve definitely felt I wasn’t in control. But I would never voice that to anybody, to not make a scene. But yeah, I didn’t [feel in control]. I felt out of control in so many different ways.
Another instance of performing, closely resembling Claire, appeared in “Chris’” (pseudonym) account. His effort to make treatment easier for his doctors was a way of maintaining a sense of control within dependence, guided by the belief that appearing agreeable would lead to attentive care. Yet, this very effort left him uninformed about key aspects of his treatment and unprepared for its consequences: I didn’t ask much at first. I didn’t want to be a patient who slows things down or asks too many questions. I figured the best thing I could do [was] just let them do what they needed to do. I thought that if I stayed quiet, they’d see me as good and take good care of me. But after surgery, they told me they’d taken out all these lymph nodes. And I had no idea that was even part of it [the surgery]. . . . My neck swelled up, I could barely swallow water, and the burns made it hard to sleep or even move.
While such behavior may appear counterintuitive, many participants justified such performances by pointing to the pressures of contemporary medical care. They emphasized that doctors see an overwhelming number of patients each day, and that being an ideal patient felt like the only way to stand out or receive attentive treatment. “Danika” (pseudonym) expressed this version of conformity in especially clear terms: Well, you know your situation. They’ve seen it [her specific kind of cancer] like 5,000 times by now, and they’ve treated, you know, 10,000 people. And you’re just like another data point that’s gonna go in their chart. So I try to make it easy for them. . . . Have everything written down, don’t take too much time, don’t complain. I, well I believed, if I come across as organized and respectful, well yeah, I just didn’t want to be a patient they dread seeing.
These accounts reveal the paradox Sartre describes: freedom exercised through submission. Having internalized the medical look, participants acted within it, performing as ideal patients to secure attention or care. In performing for the medical look, participants found control only by perfecting the conditions of their own objectification.
Discussion
Research on the medical encounter often describes objectification, internalization, and performance as distinct processes. Work on objectification shows how clinical routines and diagnostic categories position patients as objects to be managed (Carel, 2016; Leder, 1990). Studies of internalization describe how these external framings can migrate inward as patients adopt medical interpretations as their own (Dolezal, 2015). Research on credibility work and being a good patient examines how people adjust their narratives and demeanor to remain legible within clinical expectations (Gill and Maynard, 1995; Jutel, 2017). These literatures identify important dimensions of clinical life, yet they typically treat them as separate mechanisms. The findings above demonstrate that participants experienced them as connected expressions of a single condition of visibility – the medical look.
The analysis clarifies how this continuity unfolded in practice. Participants did not report objectification as a single moment. Instead, they described shifts in how their bodies and uncertainties became defined through clinical categories that carried institutional authority. Earlier studies have shown how diagnostic labeling, surveillance, and categorization reshape self-understanding, but they often do not show how these changes become tied to a patient’s own interpretation of risk or possibility (Carel, 2016; Dolezal, 2015). The interviews here show how internalization arose through this interpretive vulnerability. Participants reported that once their bodies were framed through clinical trajectories, they began to understand themselves in those terms even when this conflicted with felt experience. This continuity extended into performance. Research on good-patient behavior often treats performance as a strategic response to expectations (Gill and Maynard, 1995). Yet, participants described it as an attempt to maintain stability in encounters where visibility already carried risk.
Seeing these movements as expressions of one structure – the medical look – provides a different account of why communication pressures persist even when clinicians encourage openness. Studies of patient-clinician interaction show that reassurance or open-ended questions do not always change what patients feel able to disclose (Heritage and Robinson, 2006; Stivers, 2005). The findings here help explain why. When visibility is experienced as a condition in which one’s self-understanding is already shaped, disclosure is not simply a matter of trust. It becomes a moment in which misinterpretation feels possible. Many participants calibrated how they presented concern, gratitude, or symptom severity because they sensed that appearing composed or efficient would secure recognition. The resulting performances were purposefully enacted, yet the terms of action were set by earlier encounters that had already redefined how they could appear. This continuity draws attention to how patients navigate conditions that shape what becomes expressible.
These insights suggest directions for clinical and system-level reflection. Because objectification often began early in the encounter, small shifts in how openings are structured may alter how patients are positioned at the start. Early diagnostic framing could be delayed briefly so that the patient’s account shapes the initial orientation. Documentation practices could also preserve a distinct patient voice by ensuring that their own descriptions remain visible in the record rather than being absorbed into clinical categories (Blease et al., 2020; Walker et al., 2019). Finally, near-perfect concordance with clinical plans might be interpreted cautiously. Research on shared decision-making notes that agreement does not always indicate understanding (Elwyn et al., 2017; Montori et al., 2022). A person-centered approach may also help counteract the dynamics described here by beginning from patients’ lived needs, rather than only from clinical routines. In practical terms, this means not treating calmness, agreement, or efficiency as transparent signs that the encounter has been experienced as supportive. It also means creating space for patients to describe concerns in their own terms before those concerns are translated into clinical categories.
Limitations and scope
The study’s interpretive claims are supported by explicit analytic safeguards. Trustworthiness was supported through an audit trail, analyst triangulation, negative-case analysis, and reflexive documentation of prior commitments. Dependability and confirmability were strengthened through preservation of the decision record and consideration of alternative readings. Transferability rests on thick description of exemplar passages (Lincoln and Guba, 1985; Miles et al., 2014).
At the same time, the study has limits that shape its scope. Interview questions were designed to elicit moments in which objectification emerged through interpersonal visibility within clinical encounters. Other phenomenological sources of objectification – including bodily disruption in illness (Leder, 1990: 92–99; Toombs, 1993: 70) and technologically mediated alienation (Carel, 2016: 220–221) – were not systematically examined in this investigation.
The study also did not explicitly distinguish between reductive and supportive forms of objectification. Svenaeus (2017) argues that some forms of objectification remain compatible with acknowledgment of the lived and expressive body. Our conceptual framing, however, drew primarily on Sartre’s account of the look, which presents interpersonal visibility in predominantly conflictual and destabilizing terms. Because the interview questions were oriented by this framework and focused on moments of tension and constraint, participants primarily described objectification as limiting. Although participants in the present study primarily described objectifying visibility as limiting, this pattern should not be taken to settle the broader phenomenological question of whether all forms of being seen by another are necessarily objectifying or constraining.
The sample was predominantly female, predominantly White, and limited to English-speaking participants. These features may have shaped how visibility and performance were described. Normative expectations concerning gender, language, ethnicity, and other social positions may influence how the medical look is internalized and enacted, as well as what patients feel able to express within clinical encounters. Excluding non-English speakers may also have omitted important forms of clinical vulnerability.
One author’s prior role as leader of a Cancer Research Advocacy Group also represents a possible source of influence, as some participants knew that author before entering the study. To maintain appropriate separation, that author did not interview participants, but prior familiarity may still have influenced recruitment. Interpretation therefore relied on team-based analysis and repeated return to transcript language, rather than on any one researcher’s impressions alone.
Supplemental Material
sj-docx-1-hea-10.1177_13634593261446988 – Supplemental material for The medical gaze reframed: A phenomenological investigation of patient visibility in oncology
Supplemental material, sj-docx-1-hea-10.1177_13634593261446988 for The medical gaze reframed: A phenomenological investigation of patient visibility in oncology by Thomas Byrne, Susan E. Leggett, Aaryanna Zapata, Fanny Smithing, Joshua MacLeod, Zekun Xiao, Liangtong Wu and Jack Pickert in Health
Footnotes
Ethical considerations
Ethical approval for this study was granted by the University of Illinois Urbana–Champaign Institutional Review Board (IRB24-2216).
Consent to participate
All participants provided written informed consent prior to completing the demographic questionnaire and interview.
Author contributions
Thomas Byrne: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Supervision; Writing – original draft; Writing – review and editing. Susan E. Leggett: Conceptualization; Investigation; Writing – original draft; Writing – review and editing. Aaryanna Zapata: Conceptualization; Investigation; Methodology; Formal analysis. Fanny Smithing: Conceptualization; Investigation; Methodology. Joshua MacLeod: Conceptualization; Investigation; Methodology. Zekun Xiao: Conceptualization; Methodology. Liangtong Wu: Conceptualization; Methodology. Jack Pickert: Conceptualization; Methodology.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data are available from the corresponding author upon reasonable request. Because the dataset consists of qualitative interview materials, access is limited to ensure participant confidentiality.
Supplemental material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.