
Abstract
Background
In Australia, access to Alzheimer's disease (AD) therapeutics requires apolipoprotein E (APOE) genotype testing and disclosure, yet the feasibility, acceptability and tolerability of APOE disclosure in an Australian context remains unknown.
Objective
This pilot study evaluated a researcher-delivered, videoconferencing-based APOE disclosure protocol in cognitively unimpaired (CU) Australian adults with dementia family history.
Methods
The DISCLOSE-APOE protocol, informed by prior expert approaches and Australian consumer preferences, was piloted in fifteen CU adults aged 40–70 (8 ε4 carriers, 7 non-carriers). The protocol comprised 7 online sessions, including mood/suicide risk assessment, education, and psychological readiness evaluation. APOE genotype was disclosed 1:1 via videoconferencing using a standardized interaction procedure. Existing data and online questionnaires assessed participant characteristics and outcomes pre- and post-disclosure. Paired-samples t-tests examined within-group mood changes, and independent-samples t-tests compared post-disclosure test-/event-related distress between carriers and non-carriers.
Results
All participants (M age = 60.8 (±6.4), 60% female) completed the pilot, and no adverse events occurred. Baseline mood was equivalent across groups. Anxiety decreased post-disclosure in both ε4 carriers and non-carriers. Depressive symptoms increased slightly but not significantly in ε4 carriers and remained sub-threshold. Test-related distress was moderately higher in ε4 carriers post-disclosure.
Conclusions
Researcher-delivered and remote APOE disclosure via videoconferencing resulted in no attrition nor clinically-significant short-term psychological distress, with pilot data providing preliminary evidence of feasibility, acceptability and tolerability in this cohort. Findings will inform the development and implementation of culturally-appropriate and scalable APOE disclosure protocols in research and clinical settings to facilitate delivery of anti-Aβ therapies in Australia.
Introduction
Apolipoprotein E (APOE) ε4 carriage is the strongest genetic risk factor for sporadic Alzheimer's disease (AD) dementia. 1 APOE ε4 heterozygosity and homozygosity confer a 2–3 and 12–15-fold increased risk of AD dementia, respectively. 1 In adults with AD dementia, ∼60% carry at least one ε4 allele, 2 with ε4 carriage associated with earlier and greater amyloid-β (Aβ) accumulation, 3 and earlier symptom onset. 1
Although risk for AD associated with ε4 carriage is well-characterized, 1 APOE genetic testing in clinical practice is not recommended.4,5 This recommendation was based on concerns by physicians, geneticists, policy makers, and patients regarding the clinical utility of knowing APOE-related risk when there is no treatment for AD dementia.5,6 However, with recent approval of anti-Aβ therapies in the United States (US), Europe, Asia, and now Australia, attitudes are changing. 7 While the availability of AD pharmacotherapies is a positive development, enthusiasm is diminished somewhat by observations that ε4 carriers treated with anti-Aβ therapies are at higher risk of adverse events, and that cognitive benefits appear weaker in ε4 carriers.8–11 These two characteristics of disease management increase the importance of APOE testing and disclosure in clinical contexts for adults with symptomatic AD. 12 Additionally, as treatments become focused at the preclinical stage of AD, some prevention trials use APOE testing as a case-finding method, or include samples comprising mostly ε4 carriers.13,14 Consequently, in preclinical AD trials, APOE status is often disclosed. 13
Validated protocols show that ɛ4 disclosure is feasible and well-tolerated.15–17 For example, the US-based Risk Evaluation and Education for AD (REVEAL) trials demonstrated that in-clinic disclosure did not increase anxiety or depressive symptoms.15,16 Later studies showed that telephone-based APOE disclosure caused no negative outcomes. 18 However, in-clinic and telephone-based approaches rely heavily on expert genetic disclosure methods. While expert care is optimal, increasing demand for ε4 genotyping will require greater access, and scalable methods are needed. Systematic reviews of telehealth-based genetics services report high participant and clinician satisfaction and greater equity of access, but also highlight the need for context-specific evaluations.19,20 Current approaches may also be culturally-specific and constrained by region-specific healthcare and insurance systems, norms and potential for social stigma. 21 Consequently, the extent to which disclosure protocols developed and validated in the US can be applied in other countries with different healthcare systems and societal expectations, should be examined.
The feasibility, acceptability, and tolerability of APOE disclosure developed in the US 22 using in-clinic, telephone, and telehealth-based methods have begun to be examined in Asia4,23 and Europe, 24 however, to the best of our knowledge, not in Australia. Various geographic, social and workforce constraints provide compelling rationale for developing novel disclosure approaches in Australia. For example, one third of the Australian population reside regionally or rurally, 25 where access to genetic counseling is limited. This is compounded by an aging population, with 16% of the population aged 65+ 26 —a group more likely to require future APOE testing and disclosure. Simultaneously, a 2023 Human Genetics Society of Australasia survey found that ∼90% of respondents reported genetic counselor shortages, with almost all anticipating growing demand. 27 These factors create an environment where more scalable models of genetic disclosure, including those incorporating researcher-led and telehealth delivery, could expand access and reduce demand on limited specialists. This has become increasingly important with recent (2025) regulatory approval of anti-Aβ therapies in Australia, including mandated ε4 testing and disclosure to evaluate treatment eligibility among individuals with symptomatic AD.
This pilot study aimed to evaluate the feasibility, acceptability and tolerability of researcher-delivered, videoconferencing-based APOE disclosure in a well-characterized sample of cognitively unimpaired (CU) middle- to older-aged Australian adults with dementia family history, before initiating a larger-scale study in the general Australian population, including clinical populations. This group was selected because individuals with dementia family history are at elevated AD risk, are more likely to seek AD risk information, 28 and because midlife is a critical life-stage for primary prevention. 29 The first aim was to describe the characteristics of those willing to learn their APOE genotype in a remote research context. The second aim was to describe protocol feasibility and acceptability, including implementation outcomes. The final aim was to assess protocol tolerability, by examining within-group pre- and post-disclosure mood differences in ε4 carriers and non-carriers, and between-group differences in test-related distress post-disclosure. The first hypothesis was that anxiety and depressive symptomatology will be higher but will not exceed pre-defined clinical significance thresholds, following APOE disclosure compared to pre-disclosure in ε4 carriers, but not non-carriers. The second hypothesis was that that event- and test-related distress will be higher but will not exceed pre-defined clinical significance thresholds, in ε4 carriers compared to non-carriers following disclosure.
Methods
Participants and design
Fifteen CU adults aged 40–70 with dementia family history participated in the DISCLOSE-APOE pilot. Participants were recruited from the Healthy Brain Project (HBP; healthybrainproject.org.au) or BetterBrains Trial (BBT; betterbrains.org.au), had APOE status available, and indicated in a prior survey that they want to know their APOE genotype. The HBP is a cohort study observing midlife AD risk factors in CU Australian adults. 30 The BBT is a randomized controlled trial testing the effectiveness of personalized risk factor modification in preventing cognitive decline in CU Australian adults. 29 At time of recruitment, BBT participants had concluded the trial. Randomization status was blinded to investigators and not included in any analyses. See the Supplemental Methods for full inclusion criteria. A target sample of 15 participants was determined a priori, dictated by available staffing and funding constraints, and our conservative approach to undertaking this study, which included piloting the developed methodology in a small sample before considering scale-up in a larger future study. As such, recruitment and enrollment were monitored carefully to ensure meaningful variation in key characteristics, including an approximately even split of ε4 carriers and non-carriers, and representation across gender and age. Monash University Human Research Ethics Committee (number: 40227) approved the study in accordance with the Declaration of Helsinki. Participants provided written informed consent prior to participation and were provided a small honorarium (AUD$20) at study completion.
Protocol for researcher-delivered, videoconferencing-based APOE disclosure
A standardized protocol for researcher-delivered, videoconferencing-based APOE disclosure appropriate for an Australian context was developed to deliver consistent information, support and resources to participants. It was informed by US-developed methods 4 and Australian consumer preferences for APOE disclosure (details to be published in a subsequent article). The protocol consisted of 7 components: 1) eligibility screening, 2) education and knowledge assessment, 3) psychological readiness assessment, 4) disclosure, 5) post-disclosure follow-up, 6) follow-up assessment, and 7) post-study interview. The protocol also allowed for optional inclusion of a study partner. The study procedure is outlined in Figure 1 and is described below.
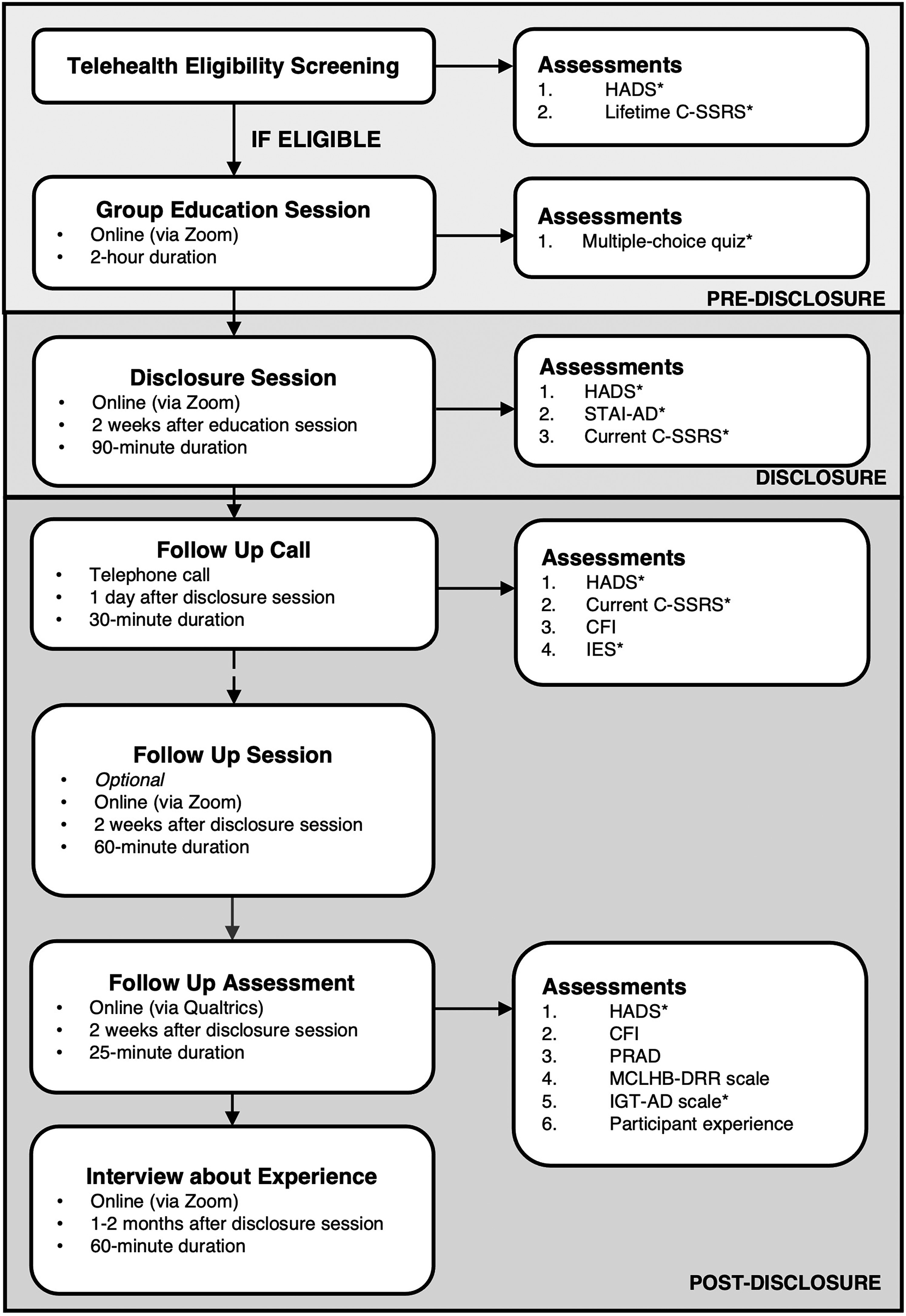
Flowchart summarizing the DISCLOSE-APOE study procedure, sessions, and assessments. Only certain assessments were included as outcomes in this study, with those included in this study indicated by the presence of a *. HADS: Hospital Anxiety and Depression Scale; C-SSRS: Columbia-Suicide Severity Rating Scale; STAI-AD: Short-Form State-Trait Anxiety Inventory for Adults; CFI: Cognitive Function Instrument; IES: Impact of Events Scale; PRAD: Perceived Risk of Alzheimer's Disease questionnaire; MCLHB-DRR: Motivation to Change Lifestyle and Health Behaviours for Dementia Risk Reduction Scale; IGT-AD: Impact of Genetic Testing in Alzheimer's Disease Scale.
Procedure
Potentially eligible participants (N = 27) were invited to participate via email between July–August 2024. After reading an explanatory statement and providing written consent, eligibility screening with a trained research assistant assessed participant mood and suicide risk. Participants were ineligible if Hospital Anxiety and Depression Scale (HADS) subscale scores 31 were >11 or if historical suicidal ideation or behavior was identified on the lifetime Columbia Suicide Severity Rating Scale (C-SSRS), 32 and a letter was sent to their general practitioner outlining this.
Eligible participants attended a group education session approximately two weeks after eligibility screening with the research coordinator and research assistant with APOE expertise. Topics included: 1) welcome/study overview, 2) introduction to dementia, 3) introduction to APOE, 4) potential risks, limitations, uncertainties, and benefits of APOE disclosure, 5) brain healthy lifestyle tips, and 6) question time. Participants received digital information packs including presentation slides, handouts, and mental health support services to review prior. Participants needed to complete and score ≥80% on a short multiple-choice quiz reviewing session content. Participants scoring <80% could review answers with a research assistant and retake the quiz to proceed to disclosure. The quiz ensured participants demonstrated adequate evidence-based APOE knowledge, including implications associated with each genotype for future AD risk.
Disclosure was a one-on-one session with the research coordinator (referred to as the APOE test result communicator). Disclosure was contingent on psychological readiness assessment at session commencement. Disclosure could occur if participants scored <17 on the Short-Form State-Trait Anxiety Inventory for Adults (STAI-AD), 33 <11 on the HADS subscales, 31 and did not endorse any current suicidal ideation or behavior on the recent C-SSRS. 32 A standardized interaction procedure was developed, including wording for disclosing results and providing genotype-specific information. Results were disclosed verbally and via a personalized handout discussed on-screen (Supplemental Figure 1). Participants received a digital copy of this handout after the session.
The post-disclosure protocol included a telephone call the day after disclosure with the APOE test result communicator. Participants were asked about wellbeing and completed mood, impact of events, and subjective cognition assessments. As additional support, participants were offered an optional follow-up Zoom session approximately one week after disclosure (to be scheduled two weeks after disclosure). Two weeks after disclosure, participants were emailed a link to complete the online follow-up assessment for completion within two weeks. This assessed mood, subjective cognition, perceived AD risk, impact of genetic testing, motivation to change lifestyle, and participant study experience.
Measures
As part of prior HBP or BBT participation, participants completed demographic, health, and AD risk assessments. Existing pre-disclosure data assessing demographics were obtained from participants’ most recent HBP or BBT assessment and used as baseline data. Baseline mood data (HADS) was obtained from eligibility screening. Post-disclosure measures were obtained from data collected within the follow-up wellbeing call (one day post-disclosure) (time 2) and follow-up assessment (two weeks post-disclosure) (time 3) (Figure 1).
APOE genotyping
APOE genotypes were obtained from previously collected saliva samples conducted via HBP or BBT participation.29,30 Participants were mailed a Genotek Oragene (OG-500) 2 ml saliva kit to complete. Samples were sent for processing and analysis to the GenoFIND Serviced laboratory (Salt Lake City, Utah, USA) to extract specific single nucleotide polymorphisms such as that for APOE: rs429358, rs7412. The six possible APOE genotypes were recorded as: ε2/ε2, ε2/ε3, ε2/ε4, ε3/ε3, ε3/ε4, ε4/ε4.
Mood
Mood was assessed using the HADS 31 and short-form STAI-AD. 33 HADS includes 14 items. Seven items were summed to create an anxiety score (HADS-Anx), and seven items were summed to create a depression score (HADS-Dep). Higher scores indicate greater anxiety and depressive symptomology. Clinically significant symptoms correspond to sub-scale scores >11. 31 The short-form STAI-AD included 6 items. All items were summed to create a STAI-AD score (lowest score = 6). Higher scores indicate greater trait anxiety. Clinically significant trait anxiety was categorized as scores ≥17 based on prior protocols.4,33
Test-related distress
Distress associated with learning APOE results was assessed using the Impact of Events Scale (IES)34,35 and the Impact of Genetic Testing in Alzheimer's Disease (IGT-AD) Scale. 36
The IES can be anchored to specific life-events and includes 15 items and two subscales (Intrusion, Avoidance).34,35 Seven items were summed to create an Intrusion score. Eight items were summed to create an Avoidance score. Total subscale scores were summed to create a total stress score. Higher scores indicate greater test-related distress.
The IGT-AD includes 16 items and two subscales (Distress, Positive). 36 Twelve items were summed to create the Distress score, while four items were summed to create a Positive score, and this subscale is reverse-scored. Total subscale scores were summed to create a Total scale score. Higher Distress, Positive and Total scores indicate greater test-related distress.
Data analysis
Analyses were conducted using RStudio (Version 2023.06.1 + 524), 37 and packages: ggplot2, psych, gmodels, car, tidyr, dplyr, readr, stringe, tidyverse, ggpubr, cowplot, emmeans, coin, matrixStats, and rstatix.
To describe demographic, genetic, and mood characteristics, descriptive statistics were computed for the total sample, ε4 carriers and non-carriers. Characteristics were summarized using the mean (M), standard deviation (SD), and range for continuous variables, and number (N) and percentage (%) for categorical variables.
To describe protocol feasibility, acceptability and implementation outcomes, including session completion rates, ineligibility/withdrawal rates, quiz completion rates and accuracy, and adverse events (incidence of suicidal ideation or behavior), descriptive statistics were computed for the total eligible sample who did not withdraw after screening, the final sample, ε4 carriers and non-carriers. Characteristics were summarized using M/SD for continuous variables, and N/% for categorical variables.
To examine tolerability (within-group pre- and post-disclosure mood changes), descriptive statistics (M, SD, range) summarized pre- and post-disclosure anxiety and depressive scores in ε4 carriers and non-carriers. Pre- and post-disclosure differences were assessed between two timepoints, namely, between time 1 (pre-disclosure) versus time 2 (post-disclosure; follow-up wellbeing call) and time 1 versus time 3 (post-disclosure; follow-up assessment) (primary outcome). To describe pre- and post-disclosure mood differences, a change score was calculated as the mean difference for each group (Equation 1):

QQ plots were visually inspected for normal distributions in change scores for ε4 carriers and non-carriers. Shapiro-Wilk tests showed that change score distribution did not significantly deviate from normality for both groups at both time comparisons (time 1 versus 2, time 1 versus 3) for most variables, with exception of non-carriers HADS-Anx scores at time 1 and 2. Scores were moderately left-skewed with most values clustering toward the higher end of the scale. To improve normality, a reflected square root transformation was applied (Equation 2):

Paired samples t-tests evaluated within-group differences in mean pre- and post-disclosure scores for ε4 carriers and non-carriers. Event and test-related distress (available post-disclosure only) was summarized using M, SD and range. A series of ANOVAs assessed between-group differences.
Statistical significance was set at p < .05. No corrections were applied for multiple comparisons as this research is novel in Australia and is largely exploratory and descriptive. Potential for Type I error was minimized by computing Cohen's d for within-group comparisons, used to contextualize results. Effect sizes were classified as small (0.20), moderate (0.50) or large (0.80). 38
Results
Pre-disclosure demographic characteristics and APOE status
Pre-disclosure demographic and genetic characteristics of the total sample and by APOE group (8 ε4 carriers; 7 non-carriers) are presented in Table 1. On average, participants were aged 60.8 (±6.4) years, had 16.9 (±3.3) educational years, were predominantly female (60%), and Caucasian (93%) (Table 1).
Pre-disclosure demographic and genetic characteristics (APOE Status) of the total sample (group level) and stratified by APOE status.
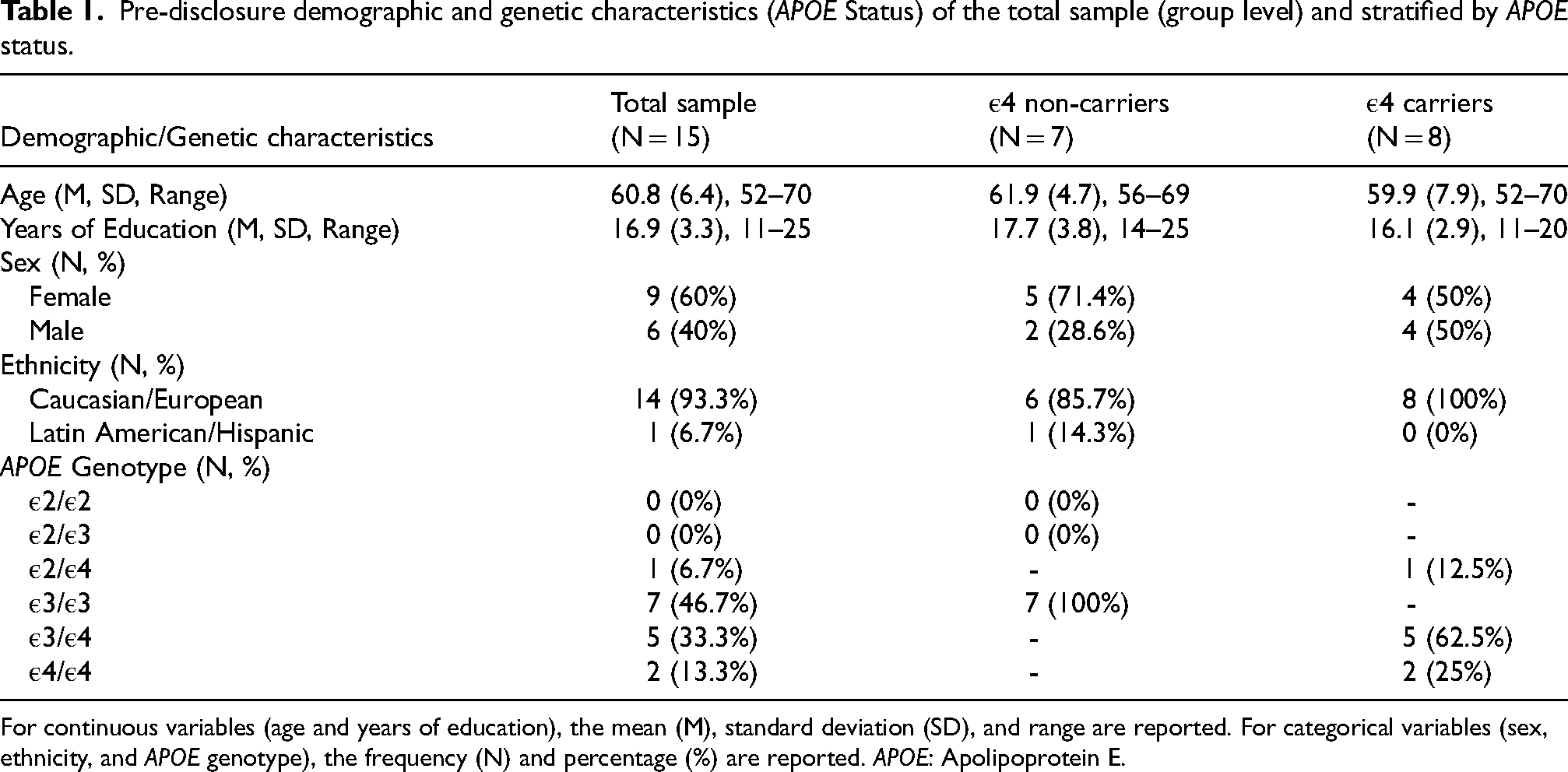
For continuous variables (age and years of education), the mean (M), standard deviation (SD), and range are reported. For categorical variables (sex, ethnicity, and APOE genotype), the frequency (N) and percentage (%) are reported. APOE: Apolipoprotein E.
Pre-disclosure mood
A summary of pre-disclosure mood symptomatology of the total sample and by APOE group are presented in Table 2 and described briefly below.
Pre-disclosure mood symptomatology of the total sample and stratified by APOE status.
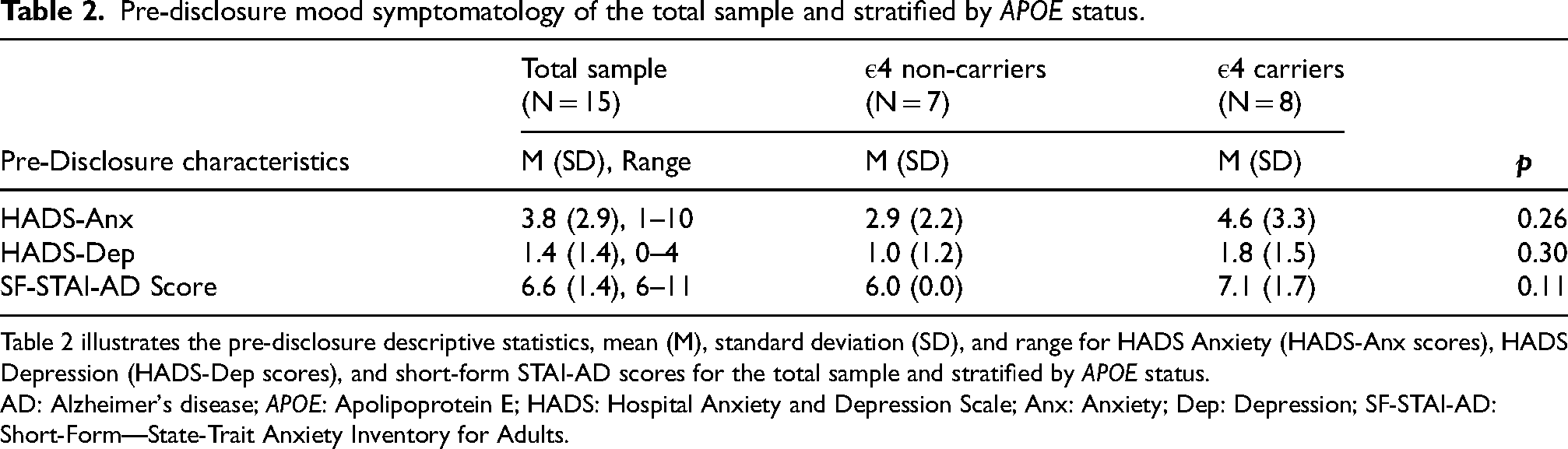
Table 2 illustrates the pre-disclosure descriptive statistics, mean (M), standard deviation (SD), and range for HADS Anxiety (HADS-Anx scores), HADS Depression (HADS-Dep scores), and short-form STAI-AD scores for the total sample and stratified by APOE status.
AD: Alzheimer's disease; APOE: Apolipoprotein E; HADS: Hospital Anxiety and Depression Scale; Anx: Anxiety; Dep: Depression; SF-STAI-AD: Short-Form—State-Trait Anxiety Inventory for Adults.
Anxiety and depression as measured on HADS, and short-form STAI-AD, did not differ significantly between groups pre-disclosure (Table 2). Pre-disclosure anxiety and depression scores for both groups were well below pre-defined cut-offs indicative of clinically significant mood symptomatology (Table 2).
Feasibility and acceptability of DISCLOSE-APOE protocol
Figure 2 illustrates study session completion and ineligibility/withdrawal rates. Briefly, 21 participants consented to participate. Of these, 20 completed screening and 18 (85.7%) were eligible (Figure 2). Seventeen participants completed the education session and quiz (81%), and 15 participants (71.4%) underwent APOE disclosure, forming the final enrolled sample (Figure 2). Only 1 participant included a study partner.
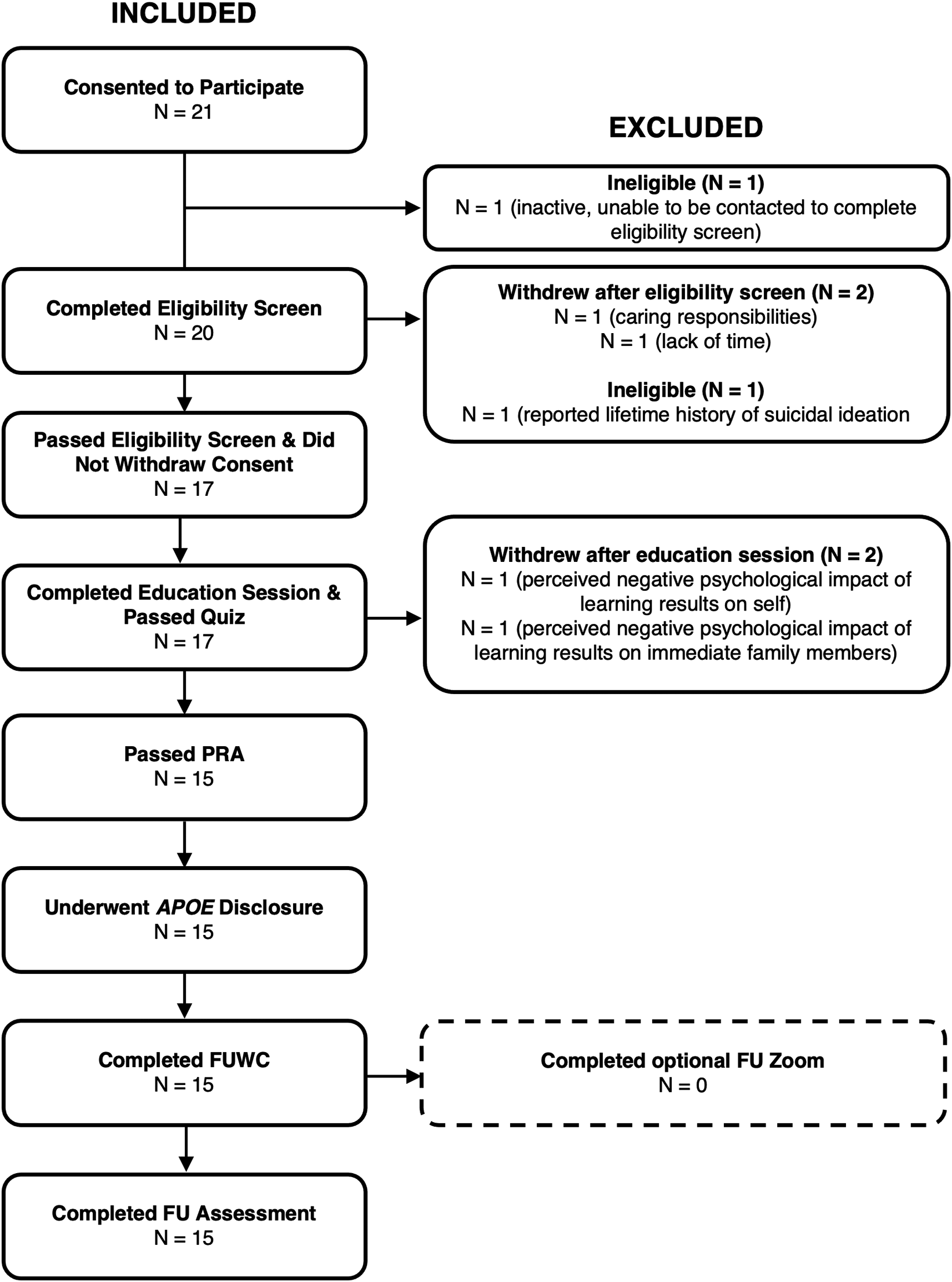
Flowchart illustrating session completion and ineligibility/withdrawal rates.
Table 3 summarizes implementation outcomes for the screened sample, final enrolled sample, and APOE groups.
Description of implementation outcomes, including quiz completion and accuracy rates, and adverse events.
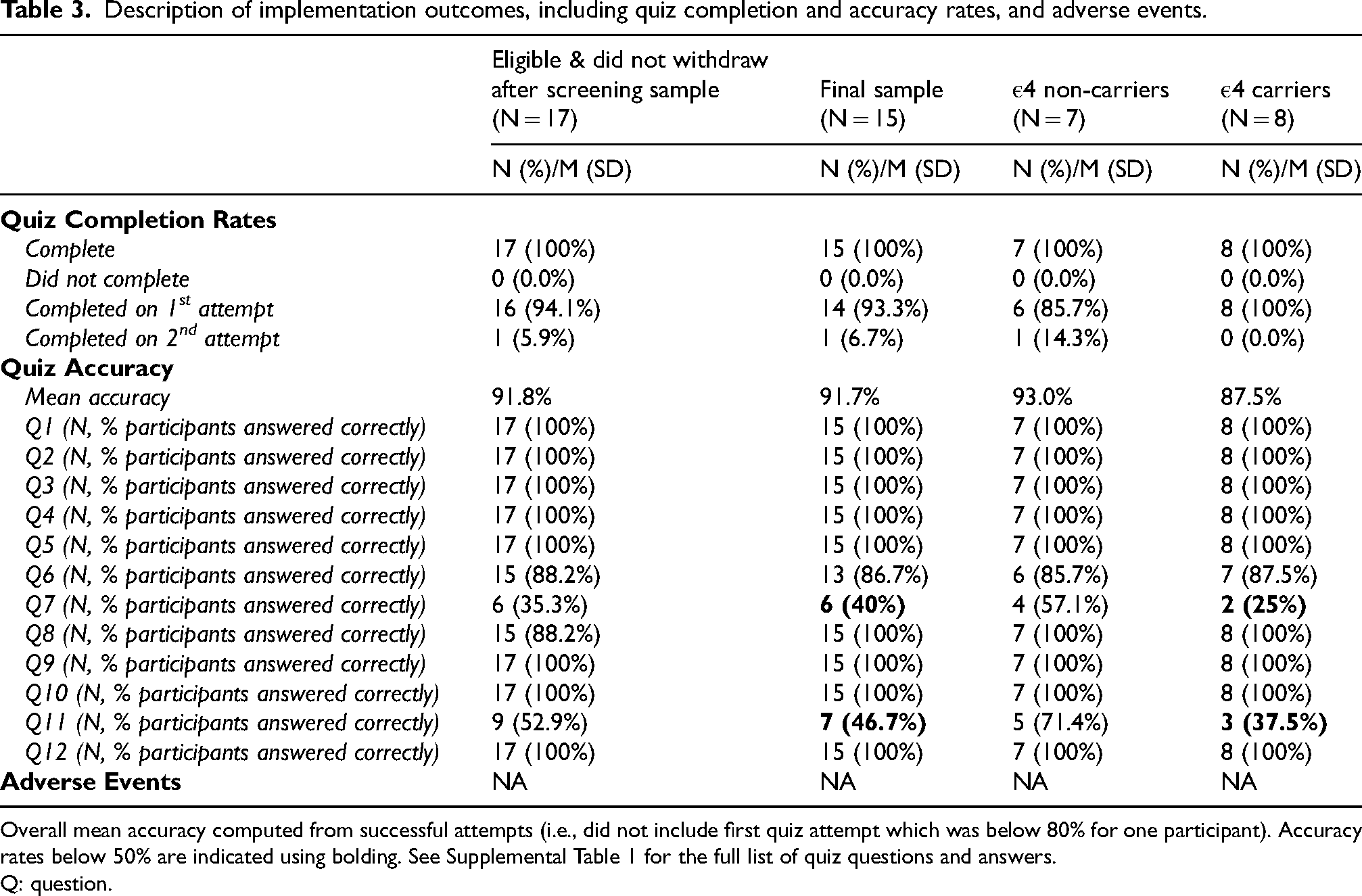
Overall mean accuracy computed from successful attempts (i.e., did not include first quiz attempt which was below 80% for one participant). Accuracy rates below 50% are indicated using bolding. See Supplemental Table 1 for the full list of quiz questions and answers.
Q: question.
Seventeen participants completed the quiz assessing APOE knowledge, with high accuracy (Table 3). Fourteen participants in the final enrolled sample completed the quiz on first-attempt (N = 1 on second-attempt and without re-review of content as participant knew where they went wrong), also with high accuracy (Table 3). Compared to non-carriers, ε4 carriers demonstrated lower mean accuracy (Table 3). Accuracy was particularly low for questions 7 and 11 (<50% of total enrolled sample answered correctly; Supplemental Table 1 for questions), driven largely by ε4 carriers (Table 3).
Adverse events
Crisis protocols were not enacted as no adverse events were reported (Table 3). No participant reported suicidal ideation or behaviors (Table 3).
Tolerability of DISCLOSE-APOE protocol
Within-group pre- and post-disclosure differences
Table 4 presents mean pre- and post-disclosure mood scores, change scores and paired samples t-tests results. A significant reduction in anxiety scores was observed in ε4 carriers from pre- to post-disclosure (time 2) and from pre-disclosure to follow-up (time 3), with the magnitude of difference ranging from moderate to large (Table 4; Figure 3). In non-carriers, a significant reduction in anxiety was observed from pre- to post-disclosure (time 2) only, with the magnitude of difference considered very large (Table 4; Figure 3).
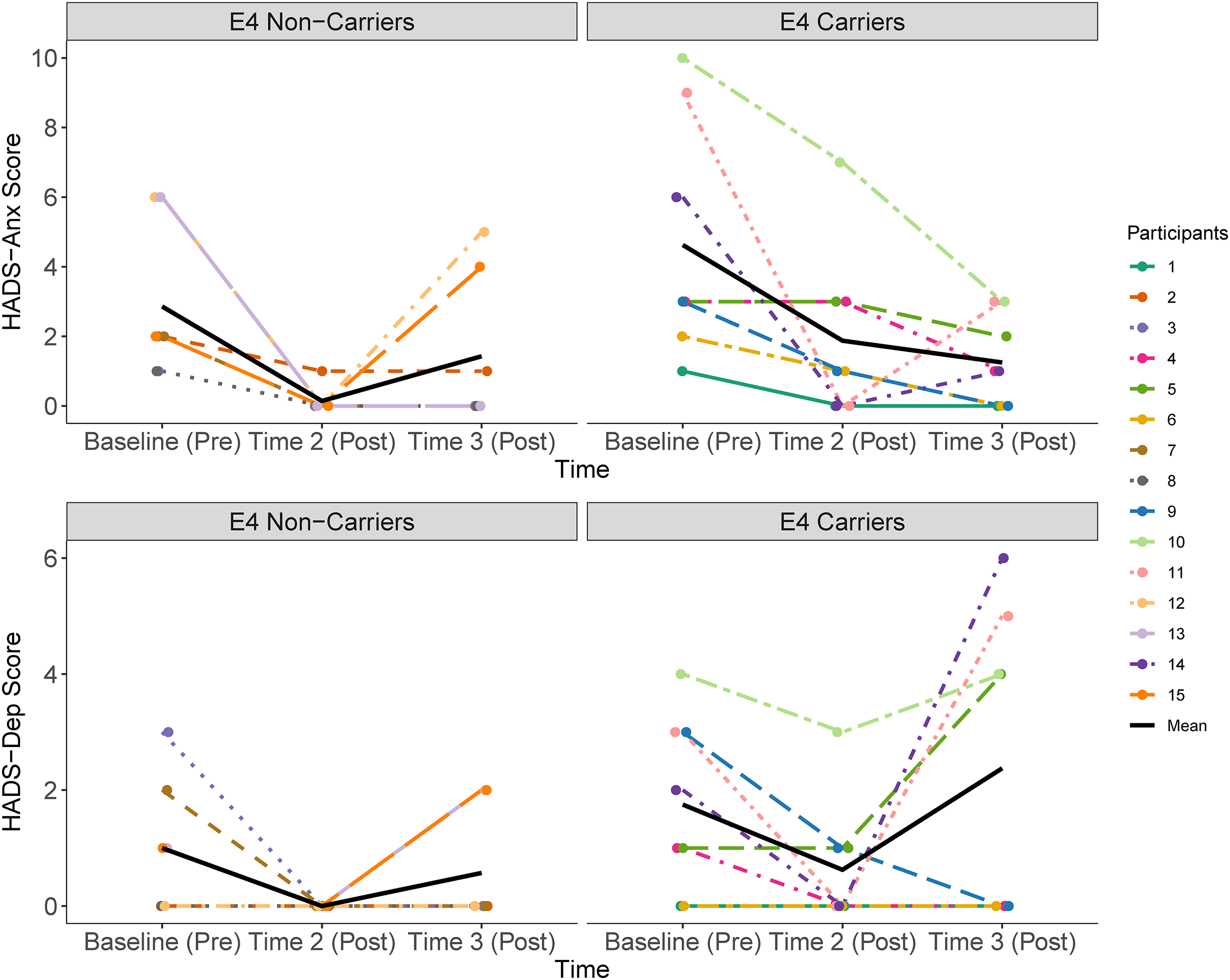
Spaghetti plot demonstrating HADS anxiety and depression scores and pre-post differences within each APOE genotype group and for each participant.
Summary of results from the paired samples t-tests assessing pre- and post- disclosure differences in mean anxiety and depression scores within APOE genotype groups.
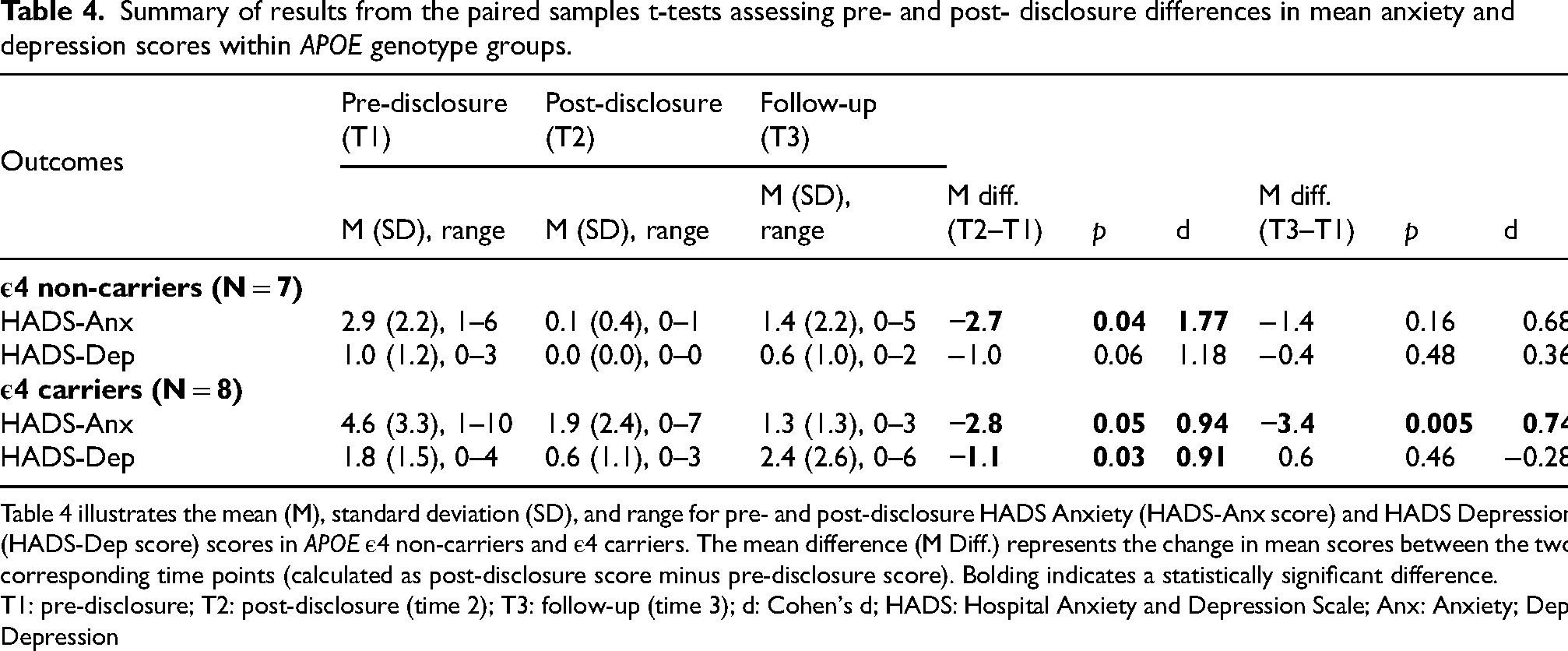
Table 4 illustrates the mean (M), standard deviation (SD), and range for pre- and post-disclosure HADS Anxiety (HADS-Anx score) and HADS Depression (HADS-Dep score) scores in APOE ε4 non-carriers and ε4 carriers. The mean difference (M Diff.) represents the change in mean scores between the two corresponding time points (calculated as post-disclosure score minus pre-disclosure score). Bolding indicates a statistically significant difference.
T1: pre-disclosure; T2: post-disclosure (time 2); T3: follow-up (time 3); d: Cohen's d; HADS: Hospital Anxiety and Depression Scale; Anx: Anxiety; Dep: Depression
A significant reduction in depression scores was observed in ε4 carriers from pre- to post-disclosure (time 2) only, with the magnitude of difference considered large (Table 4; Figure 3). In non-carriers, no significant differences in depression scores were observed from pre- to post-disclosure (time 2), or from pre-disclosure to follow-up (time 3), although the magnitude of differences were considered very large and moderate, respectively (Table 4; Figure 3).
Between-group post-disclosure differences
Event- and test-related distress
Groups did not differ significantly on the IES post-disclosure (time 2) (Table 5). However, compared to non-carriers, ε4 carriers scored significantly higher on the IGT-AD negative subscale at follow-up (time 3) (Table 5), although scores in ε4 carriers remained below clinical-thresholds for test-related distress.
Summary of results from the ANOVAs assessing group differences in the Impact of Events scale and Impact of Genetic Testing for Alzheimer's Disease scale between ε4 non-carriers and heterozygotes/homozygotes post-disclosure.
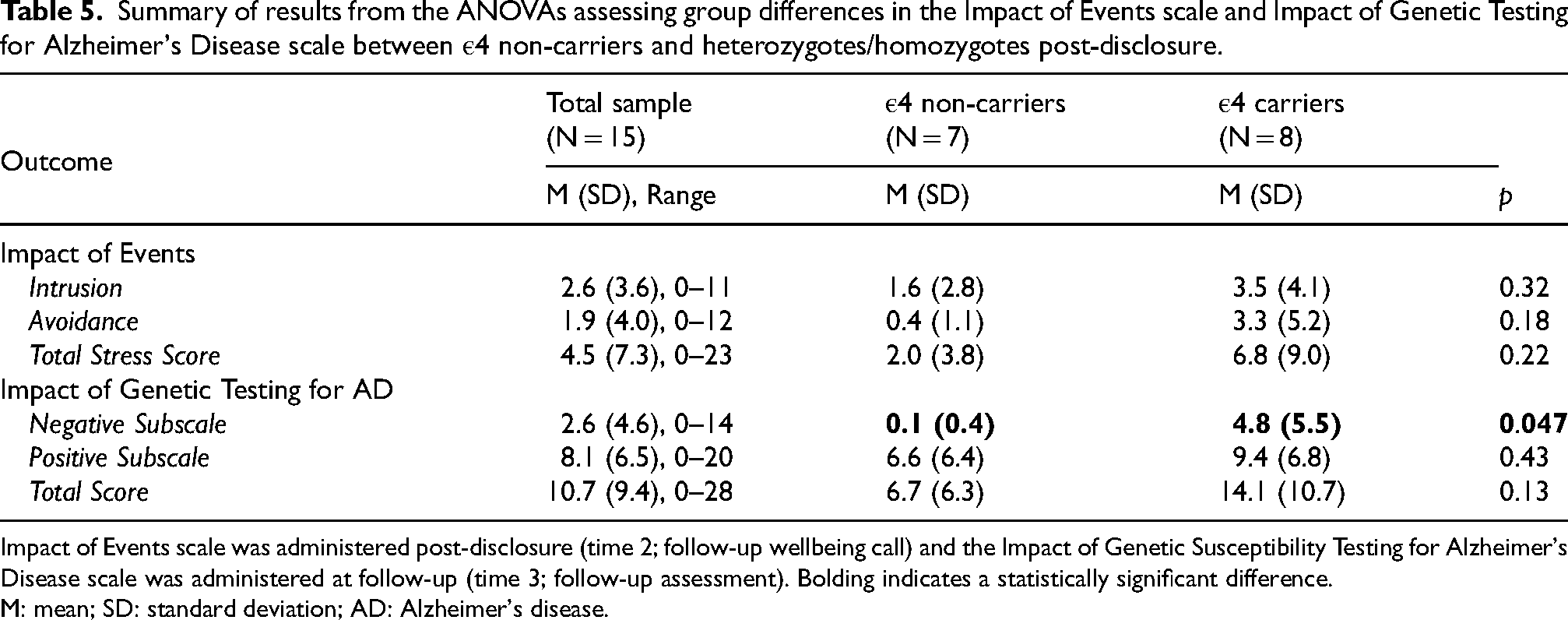
Impact of Events scale was administered post-disclosure (time 2; follow-up wellbeing call) and the Impact of Genetic Susceptibility Testing for Alzheimer's Disease scale was administered at follow-up (time 3; follow-up assessment). Bolding indicates a statistically significant difference.
M: mean; SD: standard deviation; AD: Alzheimer's disease.
Discussion
Preliminary outcomes indicate that researcher-delivered, videoconferencing-based APOE disclosure is likely feasible, acceptable, and well tolerated in CU Australian adults with dementia family history. The primary hypothesis, that anxiety and depressive symptomatology would be higher following APOE disclosure compared to pre-disclosure in ε4 carriers, but not non-carriers, was not supported. Instead, ε4 carriers demonstrated reduced anxiety and depressive symptomatology shortly after disclosure, whereas non-carriers experienced anxiety reductions only. Results are consistent with studies in CU ε4 carriers and non-carriers showing that depression and anxiety scores generally decrease15,39 or remain stable post-disclosure.13,40 If scores increase, increases are typically small and below clinical thresholds. Increases also occurred only in ε4 carriers. 13 The second hypothesis, that levels of event- and test-related distress would differ between groups post-disclosure, was supported partially. ε4 carriers and non-carriers showed equivalent event-related distress and positive test-related impacts post-disclosure. However, compared to non-carriers, ε4 carriers reported greater negative test-related impacts, including feeling worried, consistent with previous research,16,18,41,42 although scores were clinically trivial. In addition, no adverse events were reported. Together, pilot results suggest that APOE disclosure delivered by a researcher with expertise in APOE via videoconferencing is psychologically safe, with minimal negative short-term mood impacts. These findings provide a strong foundation for further understanding the use of this approach in adults at risk of, or living with, AD.
Feasibility and acceptability of researcher-delivered APOE disclosure via videoconferencing
Anti-Aβ therapies have increased demand for APOE testing and disclosure globally. 12 Similarly, demand has increased in Australia with the approval of donanemab and lecanemab by the Therapeutic Goods Administration for use only in ε4 heterozygotes and non-carriers. 43 Previous ε4 disclosure methods mostly utilize conventional in-person approaches including education and pre-/post-disclosure sessions with a genetic counselor or medical specialist. As such, feasibility and acceptability may be partially modality- and clinician-specific and this study examined feasibility and acceptability of remote pre-disclosure education, pre-/post-disclosure counseling, follow-up, and assessment with a trained researcher. The current pilot results provide important early data suggesting that researcher-delivered APOE disclosure via Zoom is feasible and acceptable, although future studies including larger samples and longer follow-ups are essential. Nevertheless, participants demonstrated high engagement with remote screening, education, disclosure, follow-up and assessment, with few withdrawals, no adverse events, and complete retention. In addition, participants demonstrated high APOE knowledge after education (M accuracy=91.8%), suggesting that content was appropriate. Lastly, there were no recorded recruitment or technological challenges, with participants demonstrating high interest in APOE disclosure and accessing scheduled sessions as planned. Our findings are consistent with, and extend, recent European-based research which found equivalent psychological and behavioral impacts of telehealth versus in-clinic APOE disclosure in Greek adults classified as CU or who had MCI. 24 These insights are important, as access to genetic counseling services in Australia is limited and standard approaches have restricted scalability. This limitation is worsened by the fact that 28% of the Australian population resides rurally or remotely, 44 as well as estimates which suggest that only 346 full-time genetic counsellors are available across Australasia, with most offices located in metropolitan centers. 27 For regional and rural populations, this increases health inequities and travel burdens. 27 Thus, the requirement for APOE testing and disclosure to determine anti-Aβ treatment eligibility may be inaccessible for many, and will place additional demand on an already over-extended workforce. Current findings support future exploration of a potential solution where content experts can deliver APOE results using standardized, evidence-based methods, accompanied by movement of APOE educational and disclosure systems online. Compared to telephone-based methods, telemedicine incorporating video, audio and screen-sharing functions may more closely resemble in-person administration, enabling attendance of a support person(s) and real-time review of study information. This study provides strong foundational data supporting the feasibility and acceptability of remote APOE disclosure, and future studies should continue to build on this evidence base to capture nuanced implications.
Effects on mood
In this study, non-carriers self-reported reduced anxiety symptomatology 1-day post-disclosure, while ε4 carriers reported reduced anxiety and depressive symptomatology. Longer-term symptom reductions from pre-disclosure to 2-weeks post-disclosure persisted only for anxiety in ε4 carriers. Importantly, neither group reported suicidal ideation or behavior. Perhaps the most consistent prior finding, also observed here, is reduced anxiety among non-carriers. 17 Other psychological impacts vary across studies and genotypes, with differences evident in the direction and magnitude of mood changes, possibly reflecting methodological (e.g., follow-up length, outcomes) and analytic differences between studies (e.g., between versus within-subjects analyses, comparisons conducted at disclosure versus non-disclosure level). Thus, that ε4 carriers demonstrated reduced anxiety and depressive symptomatology after disclosure is both contrary to, and consistent with, previous research. However, the nature of relationships observed in this pilot evaluation point positively towards methodological tolerability, with results generally reflecting observations described previously. For example, secondary analyses from REVEAL I showed no differences in changes in time-averaged anxiety and depressive scores between ε4 carriers and controls. 16 Another study reported decreased depressive symptoms in some, but not all participants, from baseline to 12-months. 39 In REVEAL II, most anxiety and depression scores fell below cutoffs across disclosure protocols and participants, with only 9% scoring above the depression cutoff after 12-months. 39 In REVEAL III, which utilized in-person and telephone disclosure, anxiety and depression scores remained below cutoffs in ε4 carriers who underwent telephone disclosure. 23 Finally, in a sample of Greek adults with a family history of AD classified as CU or with MCI, depression and anxiety scores did not increase significantly following telehealth-based disclosure. 24 While mixed findings challenge generalizability across studies, our pilot results are broadly consistent with this literature, suggesting that ε4 disclosure is well tolerated across cohorts and countries, even when conducted remotely, with little possibility for observing clinically significant distress in the short-term. Nonetheless, it will be important to remain alert to potential adverse responses in larger studies.
Effects on test- and event-related distress
There were no significant differences between ε4 carriers and non-carriers on the IES or IGT-AD positive subscale measured 1-day and 2-weeks post-disclosure, respectively. However, IGT-AD negative subscale scores, which captures adverse genetic disclosure impacts (e.g., regret, sadness), were significantly higher in ε4 carriers compared to non-carriers, although not clinically concerning (M = 4.8 out of a possible 60). Nevertheless, that IES scores did not significantly differ between groups 1-day post-disclosure contrasts with results that ε4 carriers experience higher test-related distress compared to non-carriers at 3-days, 13 6-weeks and 6-months, but not 12-months, 16 post-disclosure, although most timepoints are longer than those here. Consistent with our findings, studies report higher IGT-AD scores, including negative subscale scores, among ε4 carriers compared to non-carriers measured at 3-days, 6-weeks, 6-months, and 12-months post-disclosure.13,23,24,45 Our findings also support REVEAL III conclusions about carefully approaching remote disclosure of ε4, after observations of consistently higher IGT-AD scores among ε4 carriers who underwent telephone compared to in-person disclosure. 23 Although generalizations are limited by the small sample size and potential for Type I error, consistencies between our findings and prior literature supports the validity of our approach. As ε4 disclosure carries risk for unintended distress, it was important to comprehensively probe the potential of this methodology to cause harm and include a detailed array of outcomes. Pilot data could therefore contribute to meta-analyses of disclosure outcomes.
Limitations and future directions
Study limitations must be considered when interpreting results. First, this was a small pilot feasibility study, and as such, the sample size was constrained by the scope of available staffing and funding and intentionally conservative methodological choices, including piloting in a small sample before considering implementation in a larger future study, and findings must therefore be considered preliminary. However, these findings provide valuable initial insights into the feasibility and impacts of APOE disclosure in an at-risk population. Second, as this was the first known APOE disclosure study in Australia, we conservatively approached eligibility screening and excluded participants with HADS-Depression/Anxiety scores >11 or with history of suicidal ideation or behavior, based on reports that pre-disclosure anxiety and depression strongly predict post-disclosure outcomes. 23 Additionally, participants were recruited from two existing AD risk studies and have dementia family history, which may confer greater baseline APOE knowledge and higher interest in, and willingness to undergo, APOE disclosure compared to the general Australian population. This might enhance participants’ ability to cope with learning genetic information and to understand risk estimates. Furthermore, mean years of education among the sample was 16.9 years, equating to a tertiary level of education, which limits the generalizability of findings to populations with lower educational attainment, for whom genetic risk information may be interpreted or responded to differently. Additionally, we included only two short-term follow-up assessments and utilized mostly a within-subjects design and analyses due to sample size constraints. Future studies should assess post-disclosure outcomes within diverse samples over longer durations and between-groups, as psychological responses are likely dynamic. Notably, while qualitative data on consumer preferences for APOE disclosure were collected as part of a prior survey and informed the DISCLOSE-APOE protocol, these data form part of a broader mixed-methods research program and will be reported in a subsequent manuscript, which will further contextualize the quantitative findings presented here. Finally, future studies should examine predictors of participation and tolerability, identify implementation barriers and enablers, and evaluate the integration of APOE disclosure protocols into healthcare systems to support clinical decision making.
Conclusions
Pilot data suggest that researcher-delivered, videoconferencing-based APOE disclosure in CU Australian adults is likely feasible, acceptable, and psychologically safe, with no clinically-significant short-term adverse effects observed. Preliminary findings will guide development and implementation of culturally-appropriate and scalable APOE disclosure protocols in research and clinical settings to facilitate anti-Aβ therapy delivery in Australia.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261459068 - Supplemental material for Pilot feasibility, acceptability, and tolerability of researcher-delivered apolipoprotein E (APOE) disclosure via videoconferencing in Australian adults at-risk of dementia
Supplemental material, sj-docx-1-alz-10.1177_13872877261459068 for Pilot feasibility, acceptability, and tolerability of researcher-delivered apolipoprotein E (APOE) disclosure via videoconferencing in Australian adults at-risk of dementia by Emily Rosenich, Simran Chauhan, Ruby Haeusler, Mirette Keriakes, Hannah Cummins, Hannah Olver, Lisa Bransby, Paul Maruff and Yen Ying Lim in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors wish to acknowledge and thank all participants and their study partners involved in this study for their time, dedication, and commitment to advancing Alzheimer's disease research.
Ethical considerations
This study was approved by the Monash University Human Research Ethics Committee (approval number: 40227) and was conducted in line with the ethical principles set out in the Declaration of Helsinki.
Consent to participate
All participants provided written informed consent prior to any study procedures.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: E Rosenich is supported by an Alzheimer's Association Research Fellowship (grant number 23AARF-1025519) and a Monash University School of Psychological Sciences Strategic Project Grant. YY Lim is supported by a National Health and Medical Research Council Investigator Grant (grant number GNT2009550). The funders had no role in the study design, collection, analysis or interpretation of data, in the writing of the report, and in the decision to submit the article for publication.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: E Rosenich is an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review. YY Lim is an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review. S Chauhan, M Keriakes, R Haeusler, H Cummins, H Olver, L Bransby, and P Maruff declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available on reasonable request from the corresponding author and due to ethical restrictions, will only be shared after an approved data sharing agreement is in place.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.