
Abstract
Background
Alzheimer's disease (AD) is a prevalent neurodegenerative disorder among the elderly, influenced by both genetic and environmental factors. Organochlorine pesticides (OCPs) have recently been identified as potential environmental risk factors due to their bioaccumulation in adipose tissue and neurotoxic properties.
Objective
This systematic review aimed to examine the human evidence regarding exposure to OCPs and the risk of AD. The results of the meta-analysis showed that exposure to pesticides is significantly associated with an increased risk of AD.
Methods
A comprehensive search was performed across major scientific databases, including PubMed/MEDLINE, Scopus, Web of Science, the Cochrane Library, and Embase.
Results
Pooled estimates (random effects meta-analysis) of the four eligible studies showed a significant positive association between exposure to OCPs and the risk of AD (OR = 2.19; 95% CI: 1.40–3.42). These findings indicate that exposure to OCPs may significantly increase the risk of AD. The substantial heterogeneity among studies (I2 = 84.58%) may partly reflect differences in exposure assessment approaches, such as biomonitoring-based measurements compared with occupational or geographically inferred exposure assessments.
Conclusions
These findings highlight the importance of controlling occupational and environmental exposures to pesticides in preventing neurodegenerative outcomes. The findings suggest that chronic exposure to lipophilic pesticides, particularly persistent chlorinated compounds, may contribute to neurodegenerative processes implicated in the pathophysiology of AD. Therefore, more studies with similar designs and more precise exposure measurements are needed to confirm the results and reduce the heterogeneity.
Introduction
Alzheimer's disease (AD) is a major neurodegenerative illness affecting older adults, marked by specific neuropathological and biochemical features. Even with scientific progress, its exact cause is still unknown. Predictions show that the number of people with AD will triple in the next 40 years. The most common form, late-onset AD, usually appears after age 60 and involves memory and cognitive decline. 1 While some studies point to genetic factors linked to certain chromosomes, many cases happen without a clear genetic cause. This suggests that both genetic and environmental factors likely contribute to AD development.2,3 Pesticides are some of the most widely used and harmful pollutants in the environment. These chemicals help control pests in farming, with about 2.5 million tons used worldwide each year. However, only a small part of this amount actually reaches the pests, while over 99% ends up in the environment by accident. 4
Multiple studies have shown that chronic exposure to pesticides can lead to cognitive impairment, motor and sensory problems, poor memory and concentration, and an inability to process visual and spatial information. 5 Among these pesticides, organochlorine pesticides (OCPs) pose a major risk for neurological diseases due to their unique chemical properties. 6 They, including dichlorodiphenyltrichloroethane (DDT), hexachlorocyclohexane (HCH), dieldrin, and endosulfan, are chemically stable, lipophilic, and resistant to environmental degradation. 4
These substances can build up in the food chain and enter the human body through food and even drinking water. 6 Experimental studies have found that they interfere with nerve cell function. While several recent reviews have examined the link between pesticide exposure and neurodegenerative diseases such as AD, most have taken a broad view and have not distinguished among different types of pesticides.7,8 As a result, the available information on the specific role of OCPs, as one of the persistent, lipophilic, and potentially neurotoxic groups in the occurrence of AD, remains scattered, limited, and sometimes contradictory.
Given the unique biological and behavioral properties of this group of compounds, as well as the growing evidence of their neurotoxic effects, a rigorous and focused systematic review could provide a more comprehensive picture of the association between organochlorines and AD. Such a study could not only identify gaps in the scientific literature but also guide future research and health policy to reduce high-risk exposures.
Methods
Search strategy
In this study, we designed and conducted the search and literature collection in accordance with internationally accepted standards for systematic reviews. First, we searched reliable databases and found 114 articles. After screening titles and abstracts and carefully reviewing the full texts for quality and eligibility, only six studies were included in the final analysis.1,4,8–11 This systematic review was limited to original and research articles published in English. The information search strategy was also designed according to patterns found in previous similar reviews and aimed at increasing accuracy and comprehensiveness. 12
The search criteria included the following MeSH terms and their combinations: “organochlorines”[All Fields] OR “hydrocarbons, chlorinated” [MeSH Terms] OR (“hydrocarbons”[All Fields] AND “chlorinated”[All Fields]) OR “chlorinated hydrocarbons” [All Fields] OR “organochlorinated”[All Fields] OR “organochlorine”[All Fields]) AND (“pesticidal”[All Fields] OR “pesticide s”[All Fields] OR “pesticides”[Pharmacological Action] OR “pesticides”[Supplementary Concept] OR “pesticides” [All Fields] OR “pesticide”[All Fields] OR “pesticides”[MeSH Terms]) AND (“Alzheimer's disease”[MeSH Terms] OR (“Alzheimer”[All Fields] AND “disease”[All Fields]) OR “Alzheimer's disease”[All Fields])) AND ((fft[Filter]) AND (1990:2026[pdat]) AND (english[Filter]))
To increase the accuracy of identifying relevant studies, the references of the included articles were also manually reviewed to consider any potentially relevant studies that were not identified in the initial search. A full description of the search steps, study selection, and screening process, along with the reasons for excluding articles, is provided in the appendix to the PRISMA checklist and in the flow chart presented in Figure 1.
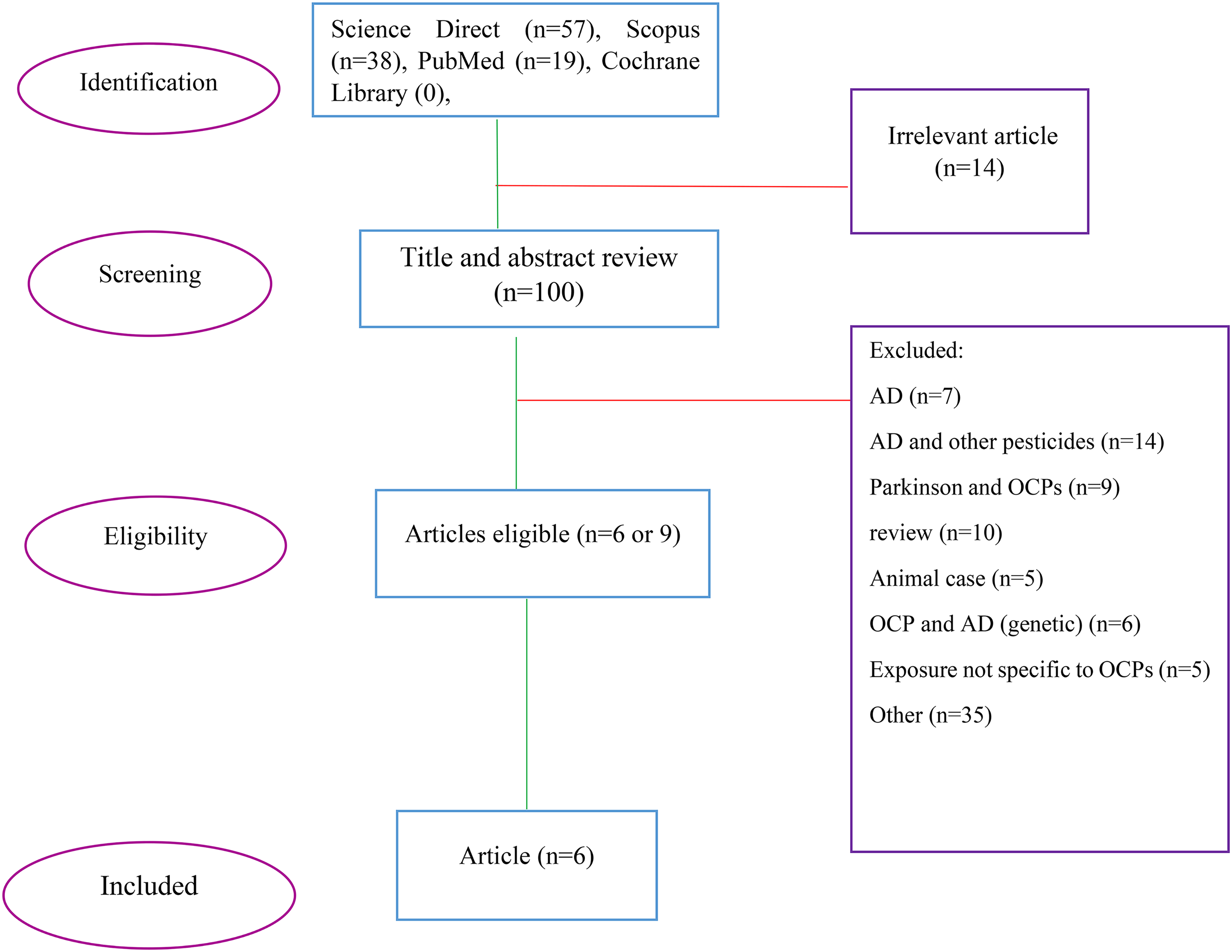
Flow diagram of studies search.
Study selection
This review included only original research. We excluded review articles, editorials, meta-analyses, and case reports. Studies that did not focus on the link between OCPs and AD, as well as those involving non-human subjects, dementia, or cognitive decline were left out. Also, studies assessing pesticides collectively with reporting OCPs specific estimates were excluded.
In the first stage, we retrieved the full texts of articles that passed the initial screening and carefully evaluated them. We then checked each article against the inclusion criteria. There were no age or ethnic restrictions on participants. In the end, eight articles met the criteria, but after a closer look, eleven were excluded for specific reasons.
Meta-analyses
Quantitative data pooling was performed using a random-effects model (DerSimonian–Laird method) to estimate adjusted odds ratios (ORs) and 95% confidence intervals (95% CIs) for the association between OCPs exposure and AD incidence. A total of six studies were identified after the final screening, of which four met the inclusion criteria for the meta-analysis and were included in the final quantitative analysis. Due to the limited number of studies included in the meta-analysis (n = 4), a formal assessment of publication bias using the Egger's test was not performed, as these methods are not reliable in the setting of small numbers of studies. The funnel plot is provided for completeness of the report only. Pooled estimates (random effects meta-analysis) of the four eligible studies showed a significant positive association between exposure to OCPs and the risk of AD (OR = 2.19; 95% CI: 1.40–3.42). These findings suggest that exposure to OCPs is associated with a more than two-fold increase in the risk of AD. In addition, the high heterogeneity (I2 = 84.58%) indicates significant differences between studies, which could be due to differences in exposure measurement methods.
Results
Study characteristics
We initially selected 114 articles for review. The studies included used valid epidemiological designs, such as cohort, case-control, and cross-sectional, to explore the link between exposure to chlorinated pesticides and AD. Eligible studies assessed this exposure directly or indirectly and reported AD related outcomes. After removing duplicates, six unique studies remained for further analysis: one cohort study, three case-control studies, and two cross-sectional studies. All studies provided valid biological and epidemiological data from 1980 to 2026 (January), with full texts available. Overall, these studies suggest a positive association between exposure to chlorinated pesticides and a higher risk of AD. Table 1 summarizes the characteristics of these studies.1,4,8–10,13
Summary of studies.
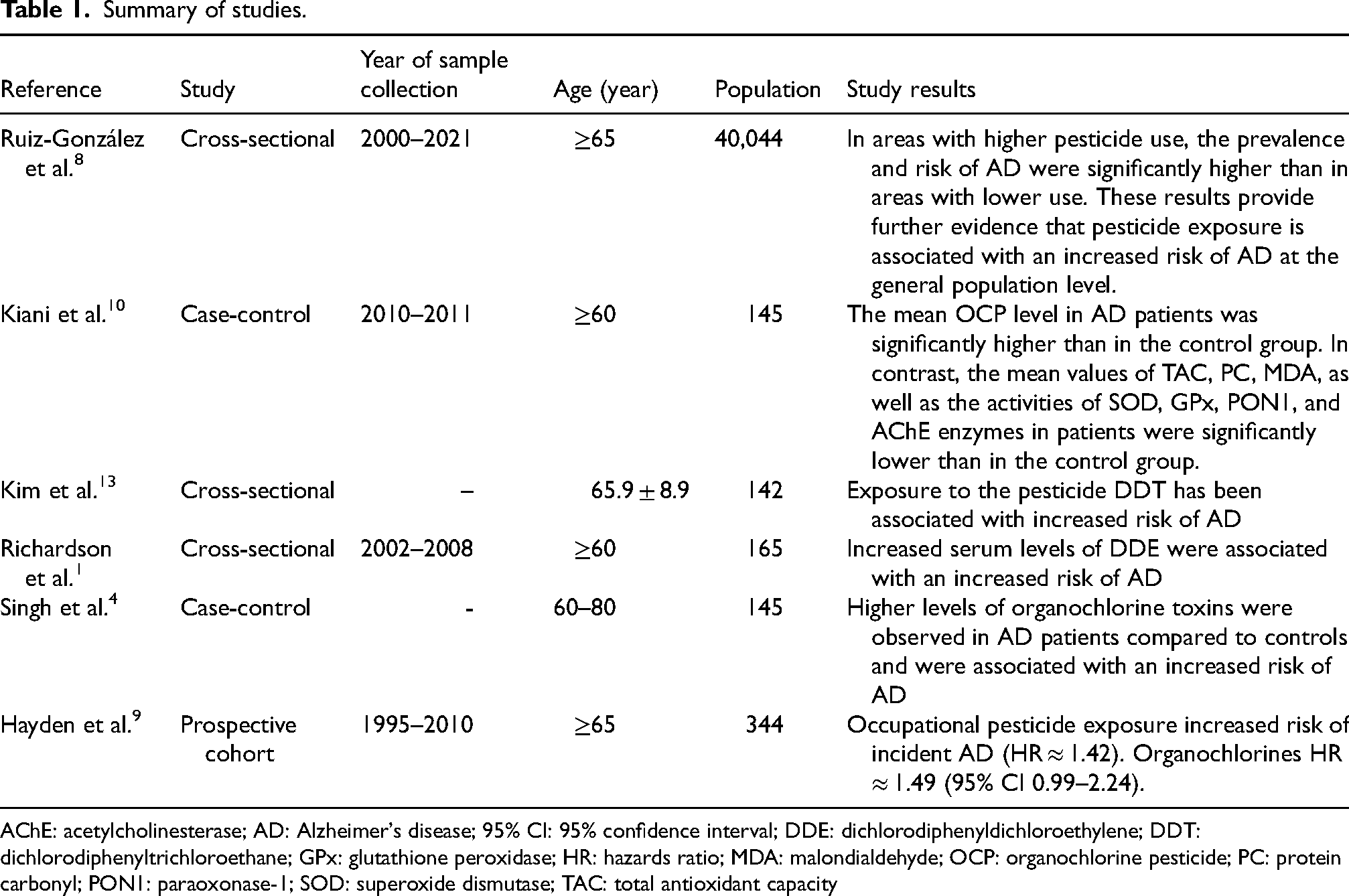
AChE: acetylcholinesterase; AD: Alzheimer's disease; 95% CI: 95% confidence interval; DDE: dichlorodiphenyldichloroethylene; DDT: dichlorodiphenyltrichloroethane; GPx: glutathione peroxidase; HR: hazards ratio; MDA: malondialdehyde; OCP: organochlorine pesticide; PC: protein carbonyl; PON1: paraoxonase-1; SOD: superoxide dismutase; TAC: total antioxidant capacity
OCP exposure and AD risk
Results of six human studies showed relatively consistent evidence for a link between OCP exposure and an increased risk of AD. Data from large populations, biomarker assays, and longitudinal follow-ups have all shown that residence in areas with high pesticide use, occupational exposure, and elevated serum concentrations of persistent compounds are all associated with an increased risk of the disease.
In one study, a large population of 591,735 people was monitored, during which 40,044 cases of AD were recorded. 8 The incidence of AD in areas with high pesticide use was almost twice that of areas with low use (3210 versus 1680 per 100,000 people). The mean age of AD patients in areas with high and low pesticide use was reported to be 81.03 ± 6.76 and 81.10 ± 6.29 years, respectively. The same pattern was observed in the control group: healthy individuals in areas with high and low pesticide use had mean ages of 81.45 and 81.63 years, respectively, which were not significantly different. 8
Examining the prevalence of F's per 100,000 population showed that the difference between areas with high pesticide use and areas with low use was statistically significant, with a crude OR of 2.09 (95% CI: 1.90–2.89); even after adjustment, the risk remained 64% higher (OR = 1.64; 95% CI: 1.41–1.89; p < 0.001) and the increase was more pronounced in women (OR = 2.27). This pattern was observed in both women and men, but the effect was more severe in women. 8 Evidence from biomarker-based studies further supports this pattern. In AD patients, β-HCH, dieldrin, and dichlorodiphenyldichloroethylene (DDE) levels were significantly higher, and each of these compounds independently increased the risk several-fold (β-HCH OR = 7.2; dieldrin OR = 6.0; DDE OR = 4.8; all p < 0.01).4,6,14
In a study of 165 people (79 healthy individuals and 86 AD patients), the chemical DDE was found in 70% of healthy individuals and 80% of AD patients. The mean serum DDE level was significantly higher in AD patients, about 3.8 times higher than in controls (2.64 versus 0.69 ng/mg cholesterol; p < 0.001). Genetic testing also showed that at least one APOE ε4 allele was present in 35% of healthy individuals and 65% of AD patients. 1 Further analysis showed that being in the highest quartile of DDE concentrations was associated with a more than fourfold increased risk of AD (OR = 4.18; 95% CI: 2.54–5.82; p < 0.001). Additionally, individuals in this quartile scored an average of 1.6 points lower on the Mini-Mental State Examiation (MMSE) test (p = 0.03). These findings suggest that both environmental factors (such as exposure to DDE) and genetic factors (such as the APOE ε4 allele) can independently and synergistically increase the risk of AD and cognitive decline. 1
A similar pattern was observed in the United States national data; in older adults aged 60–85 years, those in the fourth quartile of DDT concentrations were twice as likely to have cognitive decline (OR = 2.02; 95% CI: 1.48–2.74), and hexachlorobenzene (HCB) was associated with a similar risk (OR = 1.81; 95% CI: 1.34–2.45). Even at the 95th percentile of DDT, the risk of cognitive decline reached an OR of 6.5 (95% CI: 2.6–16.3). 13 These findings were consistent with the results of the Cache County Cohort, where 500 cases of dementia and 344 cases of AD were recorded in a 7-year follow-up of 3084 healthy individuals, and occupational exposure to pesticides increased the risk of dementia by 38% (HR = 1.38; 95% CI: 1.09–1.76) and the risk of AD by 42% (HR = 1.42; 95% CI: 1.06–1.91). In this population, organophosphates (HR = 1.53; 95% CI: 1.05–2.23) and organochlorines (HR = 1.49; 95% CI: 1.01–2.21) were both associated with an increased risk. 9
The results of the meta-analysis showed that there was considerable heterogeneity among studies (I2 = 93.7%), likely due to differences in the way exposure was assessed (occupational versus environmental), type of pesticide (chlorinated, phosphate), and outcome measurement method (clinical diagnosis of AD versus cognitive decline). However, the direction of the relationship was consistent across studies, with most reporting ORs greater than 1. The strongest correlations were observed in the studies by Singh et al. (2013) and Richardson et al. (2014), in which higher concentrations of DDE or β-HCH were significantly associated with increased odds of AD (see Figure 2).
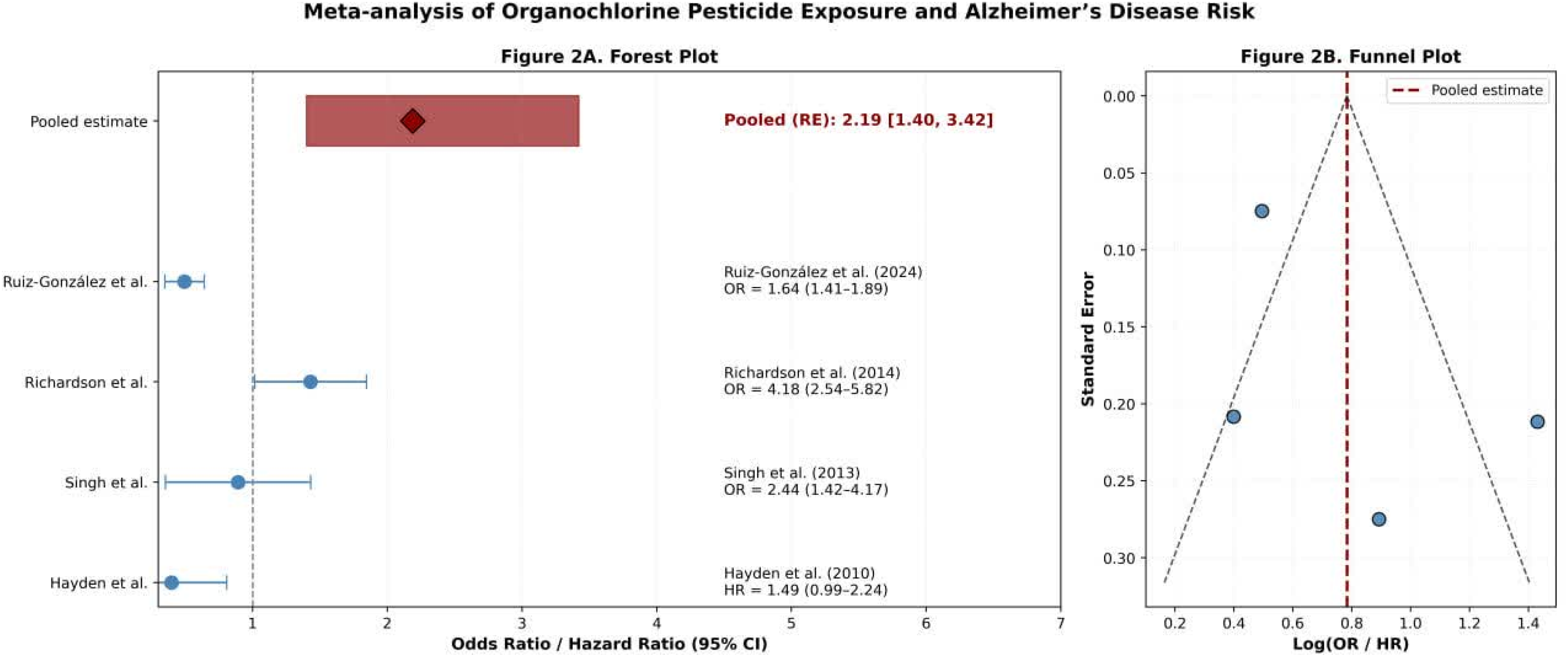
(A) Forest plot and (B) funnel plot of the random effect meta analaysis.
Overall, the findings suggest that chronic exposure to lipophilic pesticides, particularly persistent chlorinated compounds, may contribute to neurodegenerative processes implicated in AD pathophysiology; however, the high heterogeneity requires cautious interpretation.
Studied OCP
The present systematic review, based on six selected studies evaluating the association between exposure to OCPs and the incidence or progression of AD, indicates that a wide range of OCPs has been assessed across studies. The most common compounds included DDT and its metabolite (DDE), β-HCH, HCB, and, in some cases, polychlorinated biphenyls (PCBs). Three studies1,3,8,13 focused specifically on DDE as a stable indicator of DDT exposure, while three studies included PCBs in their analytical models in addition to organochlorines.9,13,15
Studies investigating this association are noteworthy for several reasons. First, some pesticides directly inhibit the enzyme acetylcholinesterase (AChE) or have similar effects.9,16,17 Scientific evidence suggests that long-term exposure to these compounds can have lasting, harmful effects on the central nervous system. Second, pesticide use has risen over the past half-century.9,16,17 According to official reports from the US Environmental Protection Agency, more than 18,000 pesticide-containing products are licensed for use, and about 2 billion pounds are used annually across a variety of areas, including agriculture, homes, schools, parks, and forests. Such statistics indicate that this issue could be a serious public health concern.9,16,17
Some studies have also examined compounds such as aldrin, dieldrin, chlordane, and endosulfan. Although these compounds are less abundant in human samples than DDE or β-HCH, they remain of public health concern due to their high adipose tissue binding and environmental persistence. The results of the studies are shown in Table 2.
General features of the main studies identified in this review.
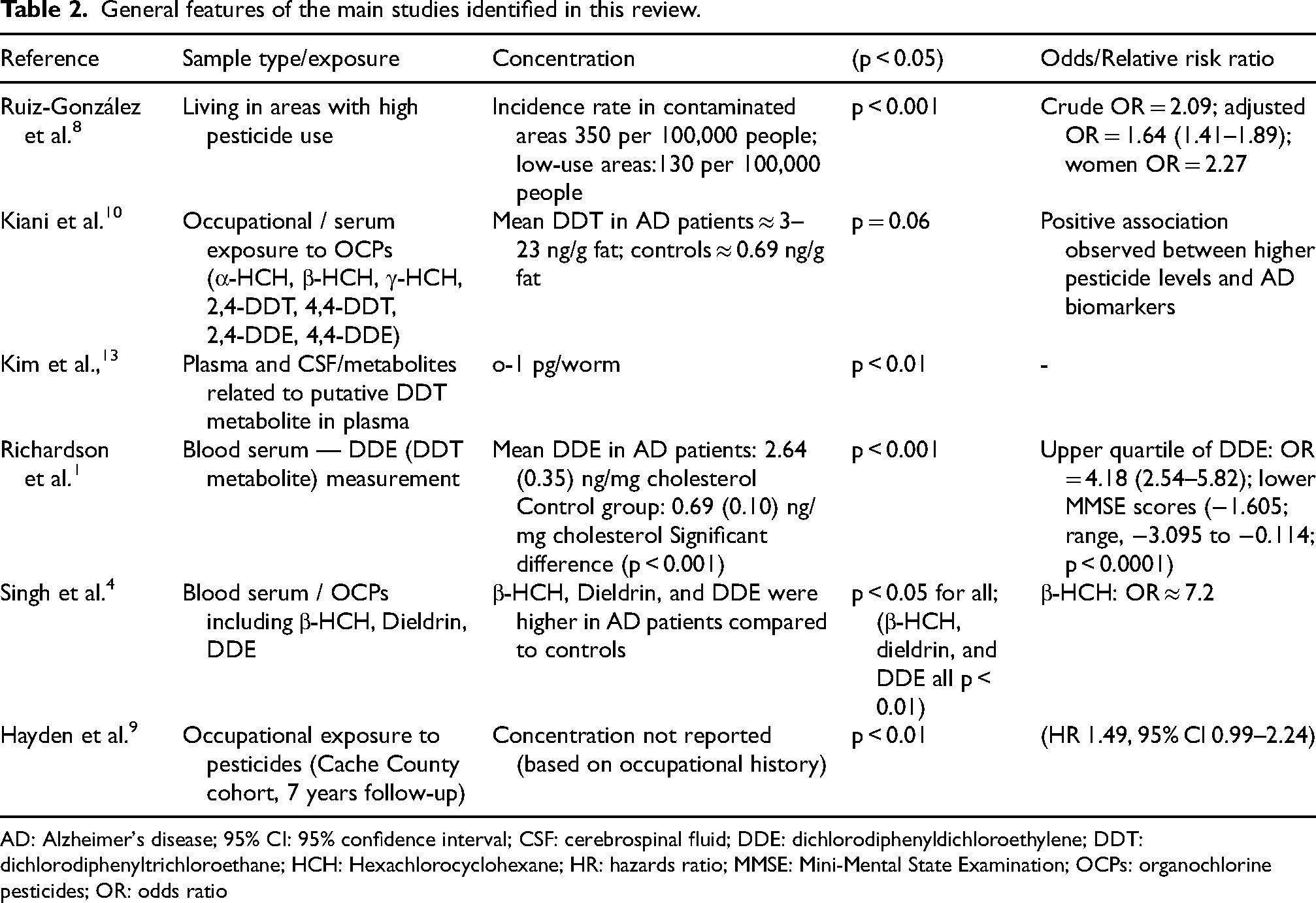
AD: Alzheimer's disease; 95% CI: 95% confidence interval; CSF: cerebrospinal fluid; DDE: dichlorodiphenyldichloroethylene; DDT: dichlorodiphenyltrichloroethane; HCH: Hexachlorocyclohexane; HR: hazards ratio; MMSE: Mini-Mental State Examination; OCPs: organochlorine pesticides; OR: odds ratio
Environmental and occupational exposure to OCPs and AD
Human studies have shown that environmental and occupational exposure to pesticides significantly increases the risk of AD and other cognitive disorders. A combined review of evidence from six human studies found that even relatively low levels of exposure to OCPs in environmental or occupational settings can have significant effects on cognitive health (see Table 3). In a cross-sectional study from Spain, which included the largest population studied (over 591,000 people), simply living in areas with higher pesticide use was associated with a twofold increased risk of AD compared with areas with lower use (OR = 2.09; 95% CI: 1.90–2.89), and this effect remained stable even after adjusting for confounders (OR = 1.64). This finding suggests that indirect and general (environmental) exposure can also significantly increase the risk of the disease. 8
Characteristics of key studies investigating OCP exposure and ad outcome.
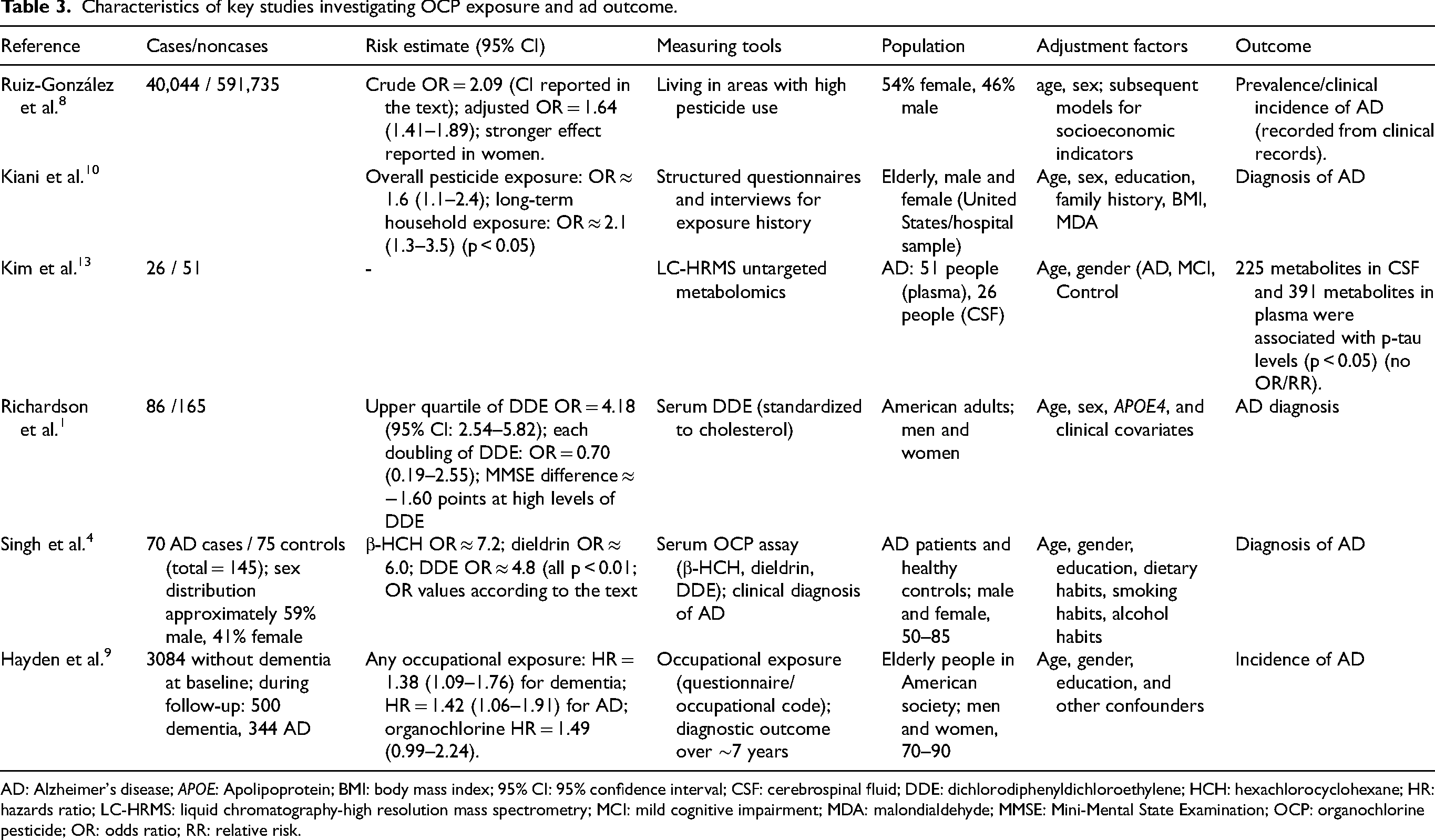
AD: Alzheimer's disease; APOE: Apolipoprotein; BMI: body mass index; 95% CI: 95% confidence interval; CSF: cerebrospinal fluid; DDE: dichlorodiphenyldichloroethylene; HCH: hexachlorocyclohexane; HR: hazards ratio; LC-HRMS: liquid chromatography-high resolution mass spectrometry; MCI: mild cognitive impairment; MDA: malondialdehyde; MMSE: Mini-Mental State Examination; OCP: organochlorine pesticide; OR: odds ratio; RR: relative risk.
In contrast, occupational exposures, which occur more directly and at higher doses, have shown a similar pattern but with greater intensity. The Cache County study found that people who worked in jobs involving direct pesticide use were 42% more likely to develop AD than those who did not (HR = 1.42). This effect was more pronounced among workers exposed to organophosphates and organochlorines (HR ≈ 1.5). 13 This emphasizes that the duration and frequency of exposure, as well as the chemical type of the toxin, are important in increasing the risk of the disease.
Biomarker measurements also reflect differences between general and occupational exposure. In studies conducted in India and the United States, AD patients had, on average, several times higher blood concentrations of β-HCH, DDE, and dieldrin than controls (β-HCH: 4.6 versus 1.3 µg/L; DDE: 5.2 versus 1.5 µg/L). These concentrations were generally due to long-term occupational exposures or to gradual accumulation from the consumption of contaminated food in high-consumption agricultural environments.1,10
On the other hand, an examination of NHANES data in the general United States population showed that even in older people without a specific occupational history, low but chronic blood levels of OCPs (DDE ≈ 3.5 ng/g lipid, DDT ≈ 1.2 ng/g lipid) were associated with a two- to six-fold increased risk of cognitive decline and AD.8,9 This suggests that pesticides can reach harmful levels due to their high environmental persistence and ability to accumulate in body fat.
Overall, the findings indicate that environmental exposure predominantly occurs through the consumption of contaminated food and water or via general environmental pollution, and is associated with an increased risk even at low exposure levels. In contrast, occupational exposure typically involves more direct and higher-dose contact, resulting in more pronounced effects on AD risk. Nevertheless, both exposure pathways may independently and synergistically contribute to an elevated risk of cognitive decline. 18
Various studies have reported an association between changes in sex hormone levels and an increased risk of cognitive decline in both sexes. For example, decreased estrogen levels in postmenopausal women are known to increase the risk of neurodegenerative diseases, including AD.8,19 Estrogen generally has protective effects on the brain, including enhancing neuronal survival, increasing synaptic plasticity, and reducing the accumulation of amyloid beta plaques.8,13 Accordingly, some evidence suggests that the use of estrogen replacement therapy in postmenopausal women may reduce the risk of dementia compared with those who do not receive this therapy. 19 In men, data also suggest that androgen deprivation therapies, particularly in patients with prostate cancer, may be associated with an increased risk of cognitive decline and dementia.8,13
This meta-analysis was based on only four studies, which significantly limited statistical power. In addition, the high heterogeneity (I2 = 84.58%) indicates significant differences between studies, which could be due to differences in exposure contexts, populations, and types of toxins; thus, the combined result should be interpreted with caution. However, most studies have adjusted for major confounders (age, sex, education, APOE status), residual confounding or unmeasured factors still exist. Ultimately, studies have used different exposure indices (biomarkers, occupational history, regional use). In general, this meta-analysis provides supporting evidence for a positive association between chronic exposure to organochlorine toxins and increased risk of AD. These findings seem biologically plausible given the lipophilic, stable, and neurotoxic nature of these compounds. However, due to the mentioned limitations, particularly the small number of studies and high heterogeneity, larger prospective cohort studies with standardized exposure assessments and accurate AD diagnosis are essential.
Discussion
The studies focused primarily on human populations, including middle-aged and older adults, as this age group is at the highest risk for neurodegenerative diseases, particularly AD and dementia. The age range of participants was typically 50 years of age and older, with some studies specifically targeting people aged 60 and older.1,4,8–10,13 The participants were recruited from various geographic locations, including the United States, Canada, India, and southern Spain. They represented both urban and rural populations in those areas. Some studies focused specifically on high-risk groups, such as farmers and workers with occupational exposure to pesticides, and people who have frequent and direct contact with toxic substances as part of their jobs.1,3,4,8–10,13,15
Data collection methods included standardized questionnaires to record environmental and occupational exposure history, interviews with participants, medical history review, and biological sampling of blood and urine to measure pesticide concentrations. These methods have enabled a more accurate assessment of exposure and its relationship to AD.1,4,8–10,13 In terms of cognitive health, participants at the beginning of the studies were often undiagnosed with neurodegenerative diseases (cohort studies) or were divided into patient and control groups (case-control studies). Cognitive function was assessed using internationally standardized tests, such as the MMSE, and the diagnosis of AD was established according to validated clinical diagnostic criteria.1,4,10,15,20
The diversity of the population and the assessment methods have enabled a more comprehensive examination of the relationship between OCP exposure and AD. This multifaceted approach helps better understand the role of environmental exposure in the development of cognitive disorders. It compensates for the limitations of individual studies by integrating data from other studies.
Pesticides are recognized as one of the main environmental factors that can increase the risk of neurodegenerative diseases. Although the results are not always completely consistent, there is evidence of neurological effects from chronic exposure to low levels of neurotoxic pesticides. These effects include problems with neurobehavioral functions, impaired sensation, movement, memory, attention, visuospatial processing, and pattern memory. 4
Scientific evidence indicates that OCPs can cause mitochondrial dysfunction and increase free radical production, leading to oxidative stress. Several studies have confirmed this mechanism and reported the neurotoxic effects of these compounds.3,4,14,21 Among OCPs, compounds such as HCH, DDT, dieldrin, and endosulfan are known to be highly persistent in the environment. 4 These substances can persist in nature for a long time due to their remarkable chemical stability, strong affinity for lipids, and very slow decomposition. These traits cause pesticides to build up in the food chain, reaching levels that can be found in food and even drinking water.4,21
Several studies have confirmed this mechanism and reported the neurotoxic effects of these compounds. Therefore, the combination of the high persistence of these pollutants in the environment and their capacity to cause neurological damage raises the possibility of a link between exposure to OCPs and an increased risk of AD.9,10,14
Although all these compounds belong to the OCP category, they differ in type, biological half-life, absorption routes, and possible mechanisms of action on the central nervous system, which could explain the heterogeneity of results across studies.1,3,4,8–10,13,15,20,22 The overlap in the types of compounds studied indicates that most research has focused on long-lasting toxins that tend to accumulate in organisms.1,8,13
The primary mechanism of action of most OCPs is the alteration of neuronal signal transmission, which can affect the transmission of messages along nerve fibres and at synapses, both between two nerves and between a nerve and a muscle fiber. Each class of pesticides disrupts this process in different ways, but the result is an abnormal transmission of nerve signals. OCPs primarily alter the ability of nerves to send messages by affecting the movement of ions across nerve cell membranes. 7 In addition, several studies have shown a significant association between pesticide exposure and an increased risk of AD.1,4,8–11
One of the most frequently studied organochlorine compounds is DDT and its stable metabolite para-para-dichlorodiphenyldichloroethylene (p,p'-DDE). These studies directly or indirectly measured the concentrations of these compounds in blood serum or adipose tissue.1,3,4,8,10,15 DDT was widely used as an agricultural insecticide and to control disease vectors (such as malaria mosquitoes) from the 1940s to the 1970s, and was banned or restricted in many countries after the 1970s. 23 However, its high stability means it remains present in the environment and the food chain. 24 Mechanistically, DDE, a stable metabolite of DDT, can accumulate in cell membranes, alter membrane permeability, and disrupt neuronal signalling by impairing sodium channel function.8,16,25
Epidemiological studies have shown that serum DDE levels were significantly higher in AD patients than in healthy individuals. 1 For example, a case-control study found that individuals with AD had higher serum DDE levels, and this association was stronger in individuals carrying the APOE4 allele. APOE4 is a known genetic factor for increasing the risk of AD, and exposure to DDE appears to exacerbate this risk. 1
There is also evidence that this compound may play a role in the pathogenesis of AD through oxidative stress and increased abnormal phosphorylation of tau protein. In the 2013–2014 NHANES study, serum DDE levels were significantly associated with an increased prevalence of AD in the elderly, even after adjusting for confounding factors such as age, sex, and education level.7,16
Studies have shown that HCB, a persistent and lipophilic organochlorine compound, has been measured in various countries, especially in Spain, Canada, and the United States.8,13,15 Due to its long half-life in the body, this substance can accumulate in adipose tissue, gradually enter the bloodstream, and have harmful effects on the nervous system over time. In a cross-sectional study in Spain, serum levels of HCB were reported as one of the key pollutants in AD patients 8 ; in a canadian study, higher levels were associated with a gradual decline in cognitive function and an increased incidence of AD during the follow-up period. 15 This evidence collectively suggests that HCB may play a role in the pathogenesis of AD through mechanisms such as mitochondrial dysfunction, stimulation of apoptosis pathways, and alterations in the regulation of genes associated with inflammation and neurodegeneration. 26
Hexachlorocyclohexane (HCH), in particular the β-HCH isomer, was measured in these studies.4,9 β-HCH is usually found at higher levels in human samples than other isomers due to its chemical stability and high tendency to bioaccumulate. 27 These compounds were mainly used as insecticides in agriculture and in household pest control. The neurotoxic mechanisms of HCH include disruption of dopamine metabolism, increased production of free radicals, and damage to the nerve cell mitochondria. 28 In a study of a population of North India, β-HCH was significantly higher in patients with AD than in the control group, and this result was maintained even after adjustment for demographic factors. This result strengthens the hypothesis of a gradual accumulation of HCH throughout life and its late effects on neurodegeneration. 4
OCPs are a large group of chlorinated hydrocarbon compounds with widespread applications in agriculture and public health programs, whose widespread use has had significant environmental consequences. The high persistence and relative non-degradability of these substances cause them to accumulate in the environment and gradually transfer through the food chain.3,4 As a result, humans, as the last link in this chain, bear the greatest burden of exposure and, due to the phenomenon of biomagnification, the amount absorbed into their bodies can be several times higher than the initial levels in the environment, which poses a potentially serious risk to public health.3,4
OCPs accumulate in adipose tissue and blood due to their high lipophilicity and persist in the environment due to their low rate of degradation. Epidemiological and experimental evidence suggest that these compounds may be associated with the development of neurodegenerative diseases.3,4,18 The proposed mechanisms focus primarily on oxidative stress: OCPs disrupt the balance between oxidizing agents and antioxidant systems, leading to lipid peroxidation and the production of active metabolites. This process, in turn, can cause oxidative damage to biomolecules and increase the levels of protein carbonyl (PC) compounds, resulting in disruption of normal protein metabolism. In this regard, exposure to OCPs may play a role in the development of cholinergic pathway disorders and increased free radical production in AD. However, there is still no definitive evidence in this regard.3,4,18
One of the hypotheses in the pathogenesis of AD emphasizes the role of oxidative stress in the initiation of neurodegenerative processes. The brain is particularly vulnerable to free radical damage due to its high levels of unsaturated fatty acids and limited antioxidant defense capacity. Under normal conditions, nerve signal transmission occurs by changing the neuronal membrane potential and moving ions through ion channels. Many pesticides disrupt this physiological cycle and interfere with nerve conduction. Chlorinated compounds, in particular, by altering the flow of ions in the axon, disrupt the balance of excitation and inhibition in neurons, ultimately leading to excessive excitation and uncontrolled discharge of nerve cells.3,4
Evidence suggests that oxidative damage plays an important role in the abnormal accumulation of amyloid beta and the destruction of neurofibrillary tangles in the brains of patients with AD. 10 Oxidative stress refers to the imbalance between the production of free radicals and the efficiency of antioxidant defense systems, and this process is directly involved in the development of age-related neurodegeneration and cognitive decline. 10
The findings indicate that PC and malondialdehyde (MDA) concentrations were significantly higher in healthy individuals than in AD patients. PCs are more stable than other indicators of oxidative stress and cause a wide range of secondary harmful effects; therefore, they are commonly used as an indicator to identify changes caused by oxidative stress. 10
According to Aksenov et al., oxidative stress-induced damage selectively affects a group of intracellular proteins, including important enzymes and structural proteins. These changes ultimately contribute to the destruction of neurofibrillary tangles in the brains of people with AD. 29 In contrast to the results of the present study, some previous studies have shown increased serum MDA levels in patients with AD. 30 This discrepancy in results is likely due to patients’ use of antioxidant supplements, which can lower MDA levels by reducing oxidative stress. However, larger and more comprehensive studies are necessary to clarify the role of all potential factors affecting MDA changes in patients with AD. 10
In the case-control study, serum levels of β-HCH, dieldrin, and p,p′-DDE were significantly higher in patients with AD than in the control group. Global surveys indicate that approximately 850,000 tons of technical HCH were used between 1945 and 2000, of which nearly 230,000 tons were released into the atmosphere. The structural features of this compound, especially in the β-HCH isomer, result in its high physical and metabolic stability.4,18,31
The different HCH isomers (α-HCH, β-HCH, and γ-HCH) enter the human body mainly through the consumption of drinking water or contaminated food. However, among them, β-HCH has the greatest ability to accumulate in tissues due to its slower excretion. Small amounts of β-HCH were also detected in the control group, although its average level was significantly lower than in AD patients. These findings suggest that, in addition to environmental exposure, other factors, such as genetic polymorphisms in enzymes involved in β-HCH metabolism, can increase levels of this compound and ultimately alter the risk of AD.3,4,18,31
The composition of DDT in its technical form mainly consists of p,p′-DDT (about 85%) and o,p′-DDT (about 15%), with other isomers present only in trace amounts. In the present study, it was found that the level of p,p′-DDE, as the main and stable metabolite of DDT, was significantly higher in AD patients than in the control group (p = 0.015). 4 The findings were consistent with those reported by Fleming et al., who detected DDT and its metabolites in brain tissue samples from AD patients more frequently than in those from Parkinson's disease patients or healthy subjects. However, the sample sizes in both studies were limited.4,32 Moreover, the results showed that dieldrin levels were significantly higher in AD patients than in the control group (p < 0.001).4,33 Dieldrin, the main metabolite of aldrin, readily accumulates in soil due to its chemical properties and is persistent in the environment because of its low rate of biodegradation. In living organisms, aldrin is converted to dieldrin mainly by monooxygenase enzymes, a process that is particularly active in the liver but also occurs in tissues such as the lung and skin.4,33
Since dieldrin is highly nonpolar and lipophilic, it is readily stored in animal fat, plant waxes, and other organic matter and accumulates in the food chain. This bioaccumulation can cause a gradual increase in dieldrin concentrations in living organisms, eventually reaching levels that exert significant toxic effects on predators higher up the food chain.3,4,33
The findings from logistic regression showed that each independent variable, including β-HCH, dieldrin, and p,p′-DDE, significantly contributed to the AD risk prediction model. The ORs for these compounds were 7.2, 6.0, and 4.8, respectively, indicating that for each unit increase in their levels, the likelihood of developing AD in the study population rises approximately 7-, 6-, and 5-fold, respectively. 4 However, in some patients with AD, these compounds were not detectable, highlighting the complexity of the disease's pathophysiology and the involvement of multiple factors in its development. Overall, these results, consistent with previous epidemiological studies, confirm the role of pesticide exposure as a risk factor for AD and specifically identify β-HCH, dieldrin, and p,p′-DDE as compounds associated with increased risk of the disease in the North Indian population.3,4
The findings showed that higher levels of OCPs were associated with increased reactive oxygen species (ROS), which ultimately led to oxidative stress. One important characteristic of aging is the weakening of the body's antioxidant defense system, such that reduced activity of endogenous antioxidant enzymes is accompanied by increased ROS production and oxidative stress in the brain. 4 This disruption in redox homeostasis plays a key role in the formation of amyloid plaques and the hyperphosphorylation of tau protein, ultimately leading to cognitive decline.4,34 In line with this, the results of the present study showed decreased activity of enzyme indicators of oxidative stress, including superoxide dismutase (SOD)3 and glutathione peroxidase (GPx)3, as well as decreased total antioxidant capacity (TAC), indicating a high severity of oxidative damage in AD patients. These results are consistent with the report by Padorario et al. They also reported decreased SOD and GPx activity in patients with cognitive impairment and AD, emphasizing the important role of oxidative damage in the development of this disease.3,4,30
Moreover, a study by Kharrazi et al. showed that decreased levels of TAS and decreased activities of catalase, GPx, and SOD enzymes are associated with an increased risk of AD in individuals carrying the APOE allele and may play a decisive role in the process of beta-amyloidosis formation, especially in individuals over 75 years of age.3,4,35
Paraoxonase-1 (PON1) is an HDL-bound esterase with known antioxidant and anti-inflammatory properties. The study found that PON1 activity was significantly lower in patients with AD than in healthy subjects. This finding is consistent with previous studies showing that both groups of pesticides, namely OCPs and organophosphate pesticides (OPPs), can inhibit PON1 activity.10,36,37 In this regard, Parag et al. examined PON1 activity in patients with AD and vascular dementia. They found that, although there was no significant difference between the two groups, PON1 activity was significantly lower than that of the control group.10,38 Also, Romani et al. have suggested that decreased PON1 arylesterase activity could be considered a specific feature of AD, which is inversely related to the severity of neurodegeneration in this disease and can therefore be considered a valuable prognostic indicator. This body of evidence suggests that PON1 dysfunction plays an important role in the pathogenesis of AD.10,39
On the other hand, the enzyme AChE, which is found in nervous tissues, muscles, plasma, and blood cells, exists mainly as a quaternary complex and plays a major role in rapidly degrading acetylcholine at cholinergic synapses. Reduced activity of this enzyme is associated, extracellularly, with amyloid protein deposition and the formation of neuritic plaques, and, intracellularly, with the development of neurofibrillary tangles.10,40 Also, AChE activity was significantly lower in AD patients than in healthy subjects. This could indicate the possible effect of OPPs on AChE inhibition.10,36,37 In line with these findings, Inestrosa et al. reported a 60% decrease in AChE activity in AD patients compared to controls, 41 indicating that AChE can be used as an indicator for monitoring the disease process and prognosis in AD. 10
However, it should be noted that almost all AD patients used AChE inhibitory drugs such as rivastigmine, donepezil, and galantamine. In contrast, such use was not observed in the control group. Therefore, it can be inferred that although OCPs inhibit AChE, the main reason for the decrease in AChE activity in the studied patients was the use of AChE-inhibitory drugs for the treatment of AD. 10 Another noteworthy point is that some reports have shown that AChE activity is increased in patients with vascular dementia and decreased in AD patients. Accordingly, measuring this enzyme's activity could be a useful tool for identifying and following patients in the early stages of cognitive impairment, before the onset of overt dementia, as decreased AChE levels are observed even in the early stages of AD.10,42
Pesticide sensitivity can be affected by gender differences; factors such as differences in body physiology, metabolic patterns, and hormonal status are among the main reasons for these differences. 43 Women, due to a higher percentage of adipose tissue than men, tend to metabolize and excrete pesticides more slowly, which can lead to long-term accumulation of chemicals in the body and thus an increased risk of adverse health outcomes.8,44 The exact mechanisms by which pesticides affect hormones are not yet fully clarified. However, evidence suggests that these compounds can interfere with the endocrine system, including by altering the synthesis, secretion, metabolism, or transport of sex hormones such as estrogens and androgens.8,43 In addition, some pesticides can activate or inhibit hormone receptors and even affect gene expression through epigenetic pathways, such as DNA methylation and histone modifications. 45
Various studies have reported an association between changes in sex hormone levels and an increased risk of cognitive decline in both sexes. For example, decreased estrogen levels in postmenopausal women are known to increase the risk of neurodegenerative diseases, including AD.8,19 Estrogen generally has protective effects on the brain, including enhancing neuronal survival, increasing synaptic plasticity, and reducing the accumulation of amyloid-β plaques.8,13 Accordingly, some evidence suggests that the use of estrogen replacement therapy in postmenopausal women may reduce the risk of dementia compared with those who do not receive this therapy. 19 In men, data also suggest that androgen deprivation therapies, particularly in patients with prostate cancer, may be associated with an increased risk of cognitive decline and dementia.8,13
Conclusion
The findings of this systematic review suggest that there was considerable heterogeneity among studies (I2 = 84.58%), likely due to differences in the way exposure was assessed (occupational versus environmental), type of pesticide (OCPs and OPPs), and outcome measurement method (clinical diagnosis of AD versus cognitive decline). The strongest associations were observed in the studies by Singh et al. (2013) and Richardson et al. (2014), where higher concentrations of DDE or β-HCH were significantly associated with increased odds of AD. Exposure to OCPs may be associated with an increased risk of AD. Epidemiological evidence and biomarker-based studies suggest that compounds such as DDE, β-HCH, and dieldrin accumulate to a greater extent in AD patients and are associated with an increased risk of the disease. Possible biological mechanisms include oxidative stress, disruption of defense enzyme activity, and direct effects on neurotransmission. However, due to limitations such as study design variability, small sample sizes in some studies, and the possibility of publication bias, the results should be interpreted with caution.
Footnotes
Acknowledgements
The Research Department has provided at the Shoushtar Faculty of Medical Sciences.
Ethical considerations
Project number: IR.SHOUSHTAR.REC.1405.008
Consent to participate
Because this study was a systematic review and meta-analysis based on previously published studies, informed consent to participate was not required.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Research Department at Shoushtar Faculty of Medical Sciences financially supported this research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data generated or analyzed during this study are included in this published article.