
Abstract
Aims: The aim of this study was to describe emergency admissions in Greenland’s healthcare system, and the extent to which admissions were associated with alcohol abuse or violence. Furthermore, we aimed to test whether data on emergencies in Greenland could be registered in a reliable way by simple means. Methods: Registration of all emergencies presented in 15 out of 17 of Greenland’s health districts in the period 21 May to 7 June 2010. Results: In the 17-day registration period, 2403 emergencies were registered. In 10% of cases the patients were clinically alcohol intoxicated. When reason for presentation were mental or social problems, attempted suicide, accidents, or violence, 24, 50, 15, and 59% respectively were intoxicated. Alcohol intoxication was statistically significantly more often associated with advanced treatment (e.g. evacuation, hospitalisation, or follow up by doctor or nurse).
Introduction
For centuries, it has been well known that excessive alcohol consumption has a negative influence on health and increases the risk of premature death. Scientific evidence pinpoints that excessive alcohol consumption especially among men is a considerable risk factor and reason for high burden of illness and puts considerable strain on the healthcare system. Each year in Denmark, alcohol is the reason for at least 3000 deaths, 28,000 admissions to hospital, 10,000 emergency department visits and 72,000 outpatient treatments [1]. The World Health Organization has published guidelines and documentation on how to counteract effects of alcohol [2]. It is underlined here that data sources on specific relation to injuries are largely lacking [3] and the association between alcohol use and injuries is very prominent [4].
Since 1987, sales of pure alcohol in Denmark per person over 14 years old measured in average numbers of litres have been rather stable, at 10–12 litres. Within the last 10 years, a slightly decreasing consumption has been observed. In Greenland, importation of pure alcohol has until recently been very high. In the years 1987–94, a steep decrease in alcohol importation was observed and since then alcohol importation has further decreased to a level comparable to the Danish consumption (Figure 1). Comparable to Greenland with respect to location north of the polar circle, size, and population, the Northwest Territories and Nunavut region of Canada have considerably lower sales and presumably consumption, as alcohol in some areas is restricted.
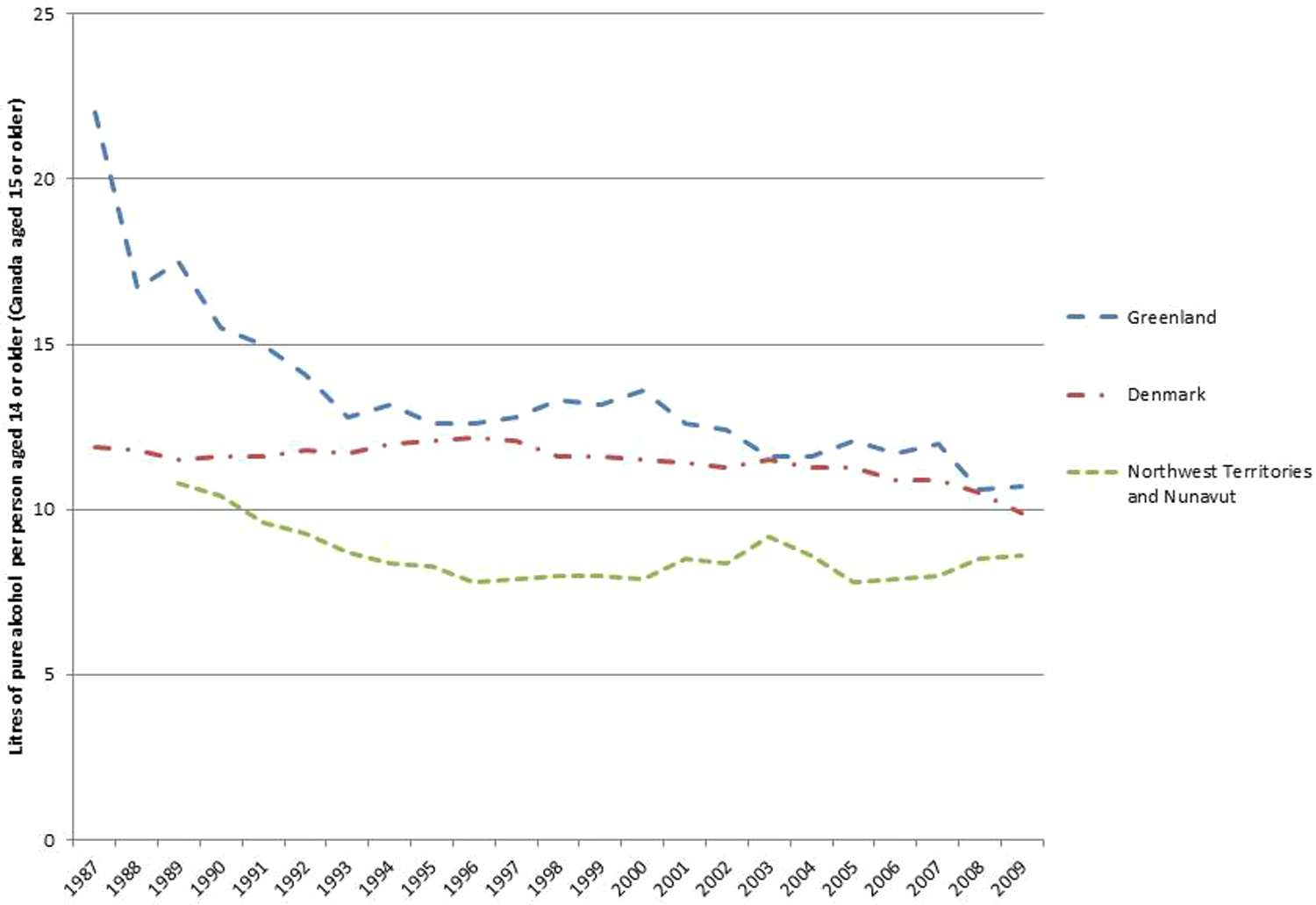
Sales of pure alcohol in Denmark and Northwest Territories and Nunavit region in Canada. Import of pure alcohol in Greenland per person aged 14 years (15 years in Canada) and above (average numbers of litres). From Statistics Denmark, Statistics Canada, and Statistics Greenland.
Accidents are common reasons for loss of life in Greenland and most likely also sick days and other suffering. Strain on the healthcare system due to of accidents is excessive, especially out of hours. Alcohol intoxication is often a contributing factor. In a study of deaths attributable to accidents in the years 1968–85, alcohol was a contributing factor in minimum 25% of cases [5]. However, alcohol intoxication is seldom noted as a cause of death in the certificate of death unless the deceased is a known alcoholic. Most often, deaths are caused by drowning, but deaths due to fire, exposure, falls, and accidental shooting are also observed in high numbers.
In a study from 1983 on emergencies admitted to the healthcare system in Greenland [6], violence accounted for 36% of admissions, alcohol-related accidents 21%, and other accidents 43%. The violent offenders were most often male, while male and female were evenly distributed among victims. Both offenders and victims were often under the influence of alcohol (80%).
In 1993–94, a nationwide health survey was conducted in Greenland. According to this survey, 48% of males and 47% among females had been exposed to violence or serious threats. Some 30% of males and 27% of females had been exposed to excessive violence such as kicking, fist fighting, pushing, strangulation, and attacks with knives or firearms. Violence victims were predominantly found among young adults less than 24 years of age. Women were most often (58% of cases) exposed to domestic violence, while male victims most often (62% of cases) did not know the offender [7].
Healthcare resources are scarce in Greenland as in many other countries. It is believed that healthcare expenditures due to alcohol intoxication and violence are huge. However, no recent studies on strains on the healthcare system due to alcohol abuse or violence are available.
The purpose of this study was to describe emergencies admitted to the healthcare system and to which extent admissions were associated with alcohol abuse or violence. Furthermore, it was tested to which extent data on emergencies in Greenland could be registered in a reliable way by simple means.
Methods
Greenland is an autonomous country within the Kingdom of Denmark. The population is 56,000. The 17 towns with approximately 47,000 inhabitants each have a hospital. About 9000 live in villages or other small settlements. Nuuk, the capital, has about 15,000 inhabitants [8]. There are no roads outside the towns, transport between towns is by sea or air, and by snowmobiles and dog sledges in the winter in areas north of the polar circle. Distances are vast: for example, the distance from the northernmost to the southernmost point is 2670 km.
The 17 towns varying in size from 500 inhabitants to 15,000 each have a hospital or rather a healthcare centre with one or more physicians, nurses, and other healthcare personnel appropriate for the population. Each healthcare centre is responsible for primary healthcare. In addition the healthcare centres have facilities for surgery and a number of inpatient beds. Queen Ingrid’s Hospital located in Nuuk is the national hospital, which has numerous specialist physicians affiliated.
Some 15 out of 17 healthcare centres participated in the study. Tasiilaq Healthcare Centre, serving 1893 inhabitants, did not want to participate because of lack of resources. Despite reminders, Paamiut Healthcare Centre serving 1679 inhabitants did not return any registration forms for unknown reasons.
Emergencies presenting from 08:00 on 21 May until 08:00 hours on 7 June 2010 were registered by the doctor, nurse, or certificated healthcare worker receiving the patient. Emergencies were defined as presentations due to of injury, illness, or disease developed or worsened within the last 24 hours. The registrations were made on a simple registration chart used in the Audit Project Odense quality improvement concept [9]. For each patient the data registered included date of birth, gender, reason for presentation, if the patient appeared clinically intoxicated, kind of treatment given, and any advanced treatment given. Possible alcohol intoxication was registered as perceived by the attending healthcare personnel and registered as heavily intoxicated, intoxicated to some extent, or not intoxicated. If uncertain whether the patient was intoxicated or not, this should be indicated. If reason for presentation was accidents or violence, additional registration forms were filled in to register site of damage, possible loss of consciousness, and diagnosis. In case of violence, number of offenders, the victim’s knowledge of or acquaintance with the offender, and any weapons used, were also registered.
Registration forms were distributed to the districts by the Ministry of Health. EpiData [10] software was used for data entry and data documentation. Data were analysed using STATA ver. 10 [11].
Results
In the 17-day registration period, 2403 emergencies were registered. The number of emergencies per 1000 inhabitants differed, from 6 in Kangaasiaq (631 inhabitants) to 190 in Narsaq (1627 inhabitants). In Nuuk, 49 emergencies per 1000 inhabitants were registered. Women accounted for 1279 emergencies, men 1081, and for 43 gender was not registered. Relatively more women were seen due to somatic disease (χ2=4.4, p=0.04). More men were seen when reason for presentation was accident (χ2=33.8, p<0.001; Table I).
Registered emergencies
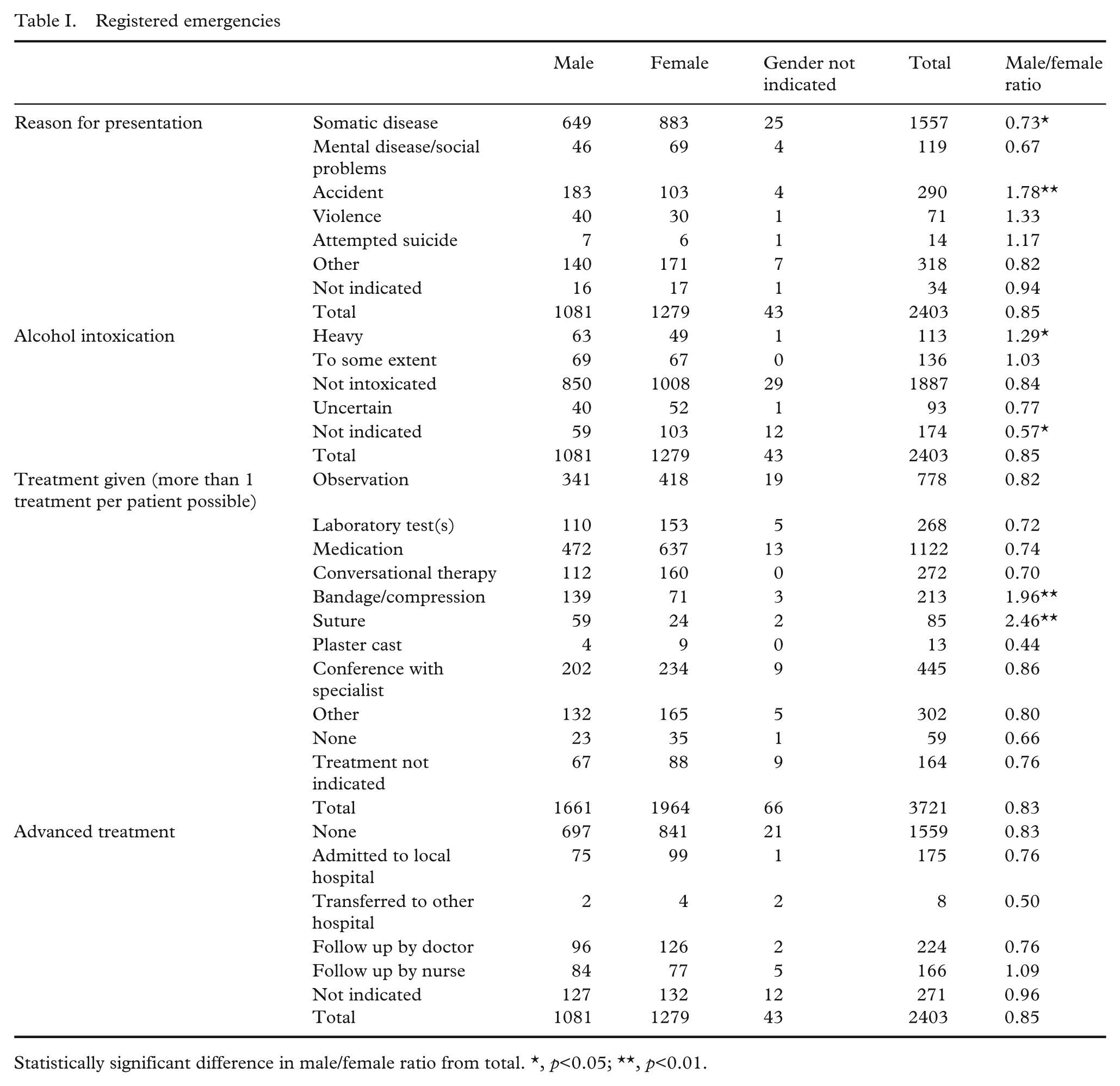
Statistically significant difference in male/female ratio from total. *, p<0.05; **, p<0.01.
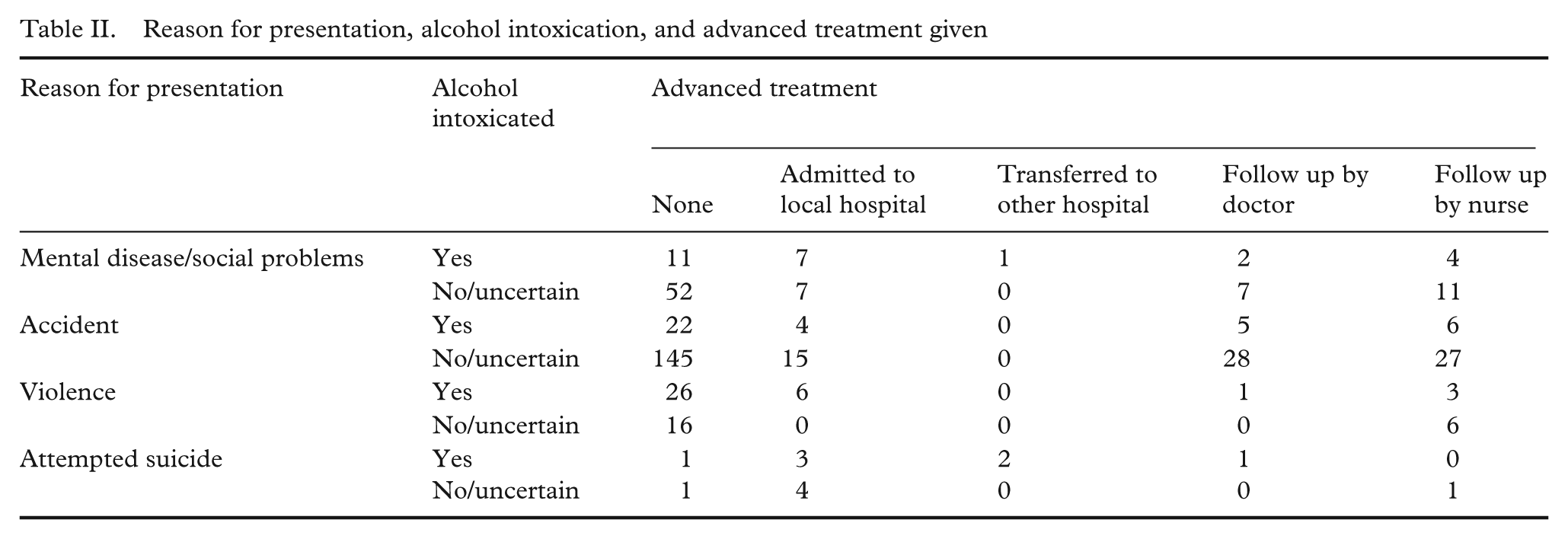
In 10% of presentations, the patients were clinically alcohol intoxicated. When reason for presentation was mental or social problems, attempted suicide, accidents, or violence, 24, 50, 15, and 59% respectively were intoxicated. Alcohol intoxication was statistically significantly more often associated with advanced treatment, e.g. evacuation, hospitalisation, or follow up by doctor or nurse (χ2=12.2, p=0.002; Table II).
Reason for presentation, alcohol intoxication, and advanced treatment given
Treatments such as observation, laboratory tests, conversational therapy, bandage, suture, plaster cast, consultation with specialist, and other treatments were registered after each presentation if any given. In 223 presentations, no treatments were given or at least not registered (Table I). One, two, three, and four of the above-mentioned treatments were given on 1311, 525, 239, and 105 presentations, respectively.
Around half the presentations (52%) took place out of hours (Table III). In 1501 cases, the treatment provider was not a doctor (nurse 920, healthcare worker 482, other 99). Among these presentations, 403 were, however, conferred with a doctor.
Registered emergencies during the day and night. A total of 272 patients with the following reasons for presentation and alcohol intoxication and/or advanced treatment given were not registered.
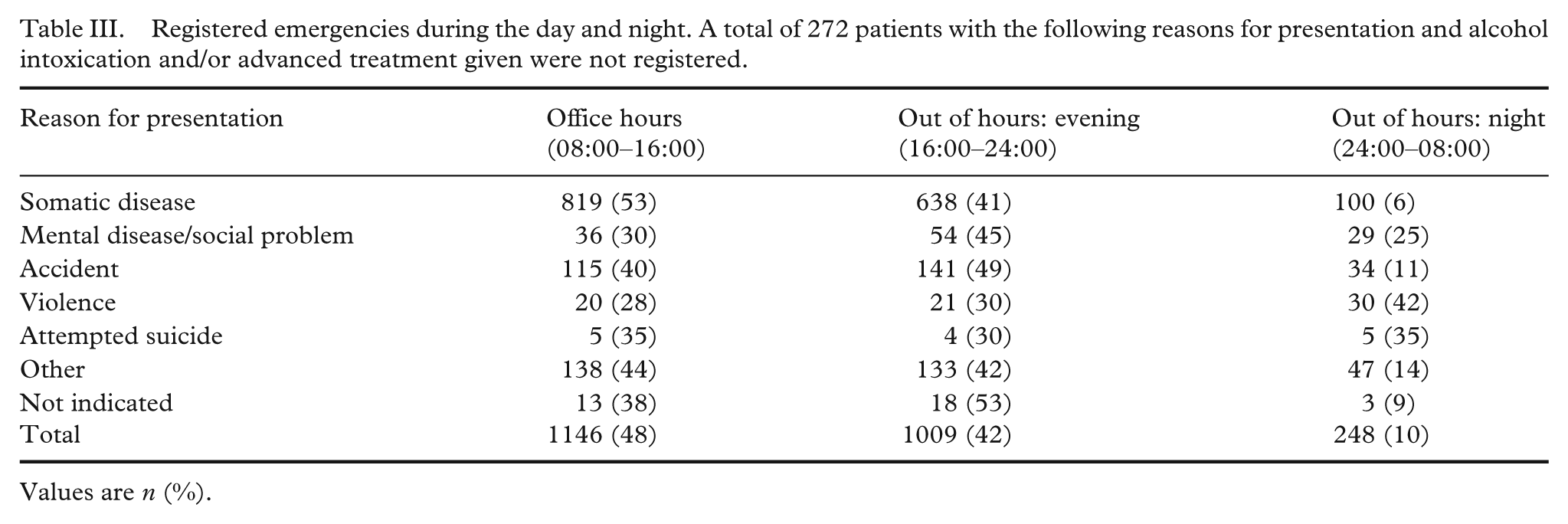
Values are n (%).
A total of 14 suicide attempts (7 males, 6 females, 1 not stated) were registered. None of these had a fatal outcome. In the registration period that included a payday, three Fridays, and two weekends, 290 accidents and 71 cases of violence were registered in the healthcare system. The additional charts were filled in for 201 and 66 patients respectively. Among the treated victims of accidents or violence, 16 and 62%, respectively, were to some degree clinically alcohol intoxicated. Among accidents, 14% were possible accidents at work. Reported accidents involved blunt trauma (46%), cuts (18%), and too excessive load on body or body parts (13%). Reported violence involved blunt trauma (77%) or cuts (8%). No reported incident of violence involved the use of firearms. In 59% of registrations concerning violence, the offender was known to the victim. More than one-third of cases were categorised as domestic violence.
Discussion
The main finding was that at least 10% of emergencies registered were clinically alcohol intoxicated when seen in the healthcare system. Not surprising, figures on alcohol intoxication were even higher when reason for presentation was mental disease or social problems, accidents, violence, or attempted suicide. The second main finding was that it is possible to gather data on emergencies treated in Greenland’s healthcare system in a reliable way by simple means.
The Audit Project Odense method is a quality development concept for general practice, which has existed since 1989. It has proven effective in registering patient encounters in Danish general practice [9]. Most recently the method has been used for describing variations in the treatment of acute otitis media [12] and treatment of hypertension in general practice [13]. Lately it has also been used for registering treatment of respiratory tract infections [14] and nurses’ tasks and perceived competency in the health districts in Greenland [15].
With the actual study design, it was, however, not possible to ensure that all presentations were registered. We do find it likely that the registration is close to complete considering the large number of presentations. Unfortunately, we did not use unique person identification on the registration forms. For this reason, repeated contacts to the healthcare system by the same person could not be identified in this study.
In relation to alcohol, the current study is in accordance with the findings in a recent Australian study on alcohol-related presentations to emergency departments in rural Australia where 9% of presentations were identified as alcohol related [16]. In a review of a number of studies of emergency departments, it was found that victims of violence more often were under the influence of alcohol than other patients presenting at emergency departments [17]. Male victims of violence were more often alcohol intoxicated than females. We found the same pattern although gender differences were not statistically significant, most likely because of small figures.
Compared to a countrywide study from 1983 where injuries were registered [6], alcohol related acute contacts to the healthcare system in Greenland seem to have diminished from 21 to 10%. However, registration methods differ, and the two registrations may therefore not be directly comparable, but it seems plausible that the burden of alcohol in the healthcare system in Greenland is diminishing although still heavy.
It is well known that assessment of clinical alcohol intoxication is difficult even for well-trained personnel. In an international study on the validity of clinical assessment of alcohol intoxication compared with estimated blood alcohol concentration using a breathalyser among patients presenting in emergency departments, clinical assessment was moderately concordant with estimated blood alcohol concentration. Overall, 93.4% of patients with blood alcohol concentration under 0.06 were assessed as not intoxicated, whereas 84.6% of those with blood alcohol concentration over or equal to 0.06 were assessed as clinically intoxicated [18]. It may therefore be a weakness of this study that alcohol intoxication was not assessed in an objective way. In a relatively high proportion of presentations (11%), the attending doctor, nurse, or certified healthcare worker refrained from assessing whether the presenting patient was intoxicated or not. This may be due to cautiousness in clinical assessment. Therefore, we find it likely that the estimated proportion of alcohol-intoxicated patients in this study is a minimum figure. We did consider using a breathalyser, but did not implement it for practical and ethical reasons.
We have not established any certain causal relation between alcohol intoxication and acute presentation in the healthcare system. However, one may speculate that a number of presentations could have been avoided or consequences might have been less severe if alcohol had not been involved.
We did find relation between alcohol intoxication and very cost-intensive advanced treatment such as admission to hospital and transfer to other hospital. Especially the latter is very cost-intensive as this most often involve the use of airplane or helicopter evacuation due to the special infrastructure in Greenland.
Conclusions
This study confirms that violence- and alcohol-related emergencies put a considerable strain on the healthcare system. Due to the short observation period, we have not described the actual extent of the problem in detail nor was it possible to estimate whether this problem is more pronounced in Greenland than in other countries, for example Denmark.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None.