
Abstract
Previous research reported that healthcare professionals rate the physical work environment more negatively than other characteristics of the environment. This study investigated salient dimensions of employees’ perceptions of healthcare facilities and differences across demographic groups. A total of 496 healthcare professionals from eight acute care hospitals participated in this cross-sectional study. Employees’ perceptions of 27 different architectural and physical features in patient areas, work spaces, and staff areas were measured. Common factors were extracted through principal component analysis, levels of association between employees’ perceptions and each architectural and physical feature were determined through confirmatory factor analysis, and differences across demographic groups were defined through invariance analysis. Findings of this study highlight the importance of attention to caregiver needs for a safe and comfortable work environment via finishing materials, indoor air quality, and furniture design. In comparison, features that address the visual quality of the work environment, such as window views and artwork, were found to have smaller associations with positive evaluations by employees. However, in non-clinical staff areas, employees appreciate features improving the visual quality of their rest area. The study also found that younger employees and those newer to the facility would appreciate improvements in the architectural/physical features to a greater extent.
Keywords
Introduction
A satisfied and motivated staff is a necessary element of good healthcare delivery, and healthcare executives should regularly examine the factors that influence clinicians’ perceptions of quality and satisfaction to understand and plan for necessary changes. 1 One of the most extensive bodies of evidence and knowledge on the relationship between physical design of buildings and key patient and staff outcomes (injury, stress, work effectiveness, and satisfaction) exists in the healthcare design domain, which is commonly known as evidence-based design (EBD). Hamilton and Watkins 2 used principles of evidence-based medicine (EBM) and defined EBD as a process in which current best evidence from research and practice are used in informing critical design decisions. They noted that as medicine has increasingly moved towards EBM, healthcare design is increasingly moving towards approaches that link hospitals’ physical environments to healthcare outcome. As for staff outcomes, evaluation of the scientific research on evidence-based healthcare design conducted by Ulrich et al. 3 reported that well-designed physical settings play an important role in making hospitals a better workplace. Accordingly, as Mroczek et al. 4 suggested, it is important to understand how healthcare employees perceive different aspects of the hospital physical environment. The authors used previous studies to identify important dimensions involved in evaluating the facility physical environment by staff members and conducted a cross-sectional study to answer the following research questions:
Research Question 1: What is the relative importance of major environmental dimensions involved in evaluating facility physical environment by healthcare professionals?
Research Question 2: Is there any significant difference in employees’ perceptions of the physical work environment across different demographic groups?
As Gibson
5
noted, in addition to the object shapes and spatial relationships between them, perceiving meaning from the environment may depend on the individual’s intentions, experiences, social setting, and culture as well as the individual’s ability to perceive the information. Sallis et al.
6
also noted that individual factors should be considered as well to fully understand multiple levels of the environment’s influence on individuals. Because employees spend their working time at different locations, the authors decided to distinguish between three different types of spaces. These three spaces are defined as follows:
Patient areas, including spaces that are designed to be used by patients and families, such as inpatient rooms, patient rooms in critical access nursing units, critical care rooms, Labor, Delivery, Recovery, Postpartum (LDR/LDRP) rooms, and support areas for families and visitors Staff work spaces, including individual work spaces, shared work spaces (e.g. report rooms, nurse stations), patient treatment areas, examination rooms, operation rooms, therapy rooms, and other spaces where staff spend the majority of their working time performing their tasks. Staff areas, including spaces that are used solely by employees, such as staff lounge and caregiver sleeping areas.
Literature review
Summary of selected post-occupancy evaluation studies.

Among generic evaluation methods used in different types of buildings, the physical comfort subscale of work environment scale (WES) developed by Moos 12 has been used in numerous healthcare studies.20xref ref-type="bibr" rid="bibr21-1420326X13514868"/>xref ref-type="bibr" rid="bibr22-1420326X13514868"/>–23
Several measurement tools are also designed and used exclusively in healthcare environmental studies. Becker
24
posits that a healthcare workplace is an interdependent system comprising the environment, work processes, organizational culture, workforce demographics, and information technology. Berry and Parish
15
defined perception of hospital physical environment as quality of the physical environment as perceived by healthcare staff members. They maintained that four facets of the physical environment may influence employees’ perceptions, including the quality of patient care area, the quality of patient work spaces, safety (the degree of hazard for staff and patients related to facility design), and pleasantness (the ambience of the facility design due to specific design features). According to Harris et al.,
25
studies of environmental sources of satisfaction in healthcare facilities should distinguish between three relevant dimensions of the physical environment:
Architectural features, including relatively permanent characteristics such as the spatial layout of a hospital and room size Interior design features, including less permanent elements such as furnishings, colours, and artwork Ambient features, such as lighting, noise levels, odours, and temperature.
As Andrade et al. 1 noted, healthcare physical environments and their implications for users have been the major focus of environmental psychology. In a quasi-experimental study in a community mental health centre, Folkins et al. 26 found that the staff members who moved to new facilities reported a significantly higher satisfaction with the physical environment and higher overall job satisfaction. Similarly, in a before–after study of nurses in single-room maternity care versus traditional birth settings, Janssen et al. 19 found that nurses working in new units reported higher overall satisfaction with the work environment and higher job satisfaction.
In addition to job satisfaction, job-related stress and burnout have been the subject of many empirical studies. For example, Applebaum et al. 27 studied 116 full-time registered nurses in adult medical-surgical units and found significant relationships between perceived noise and stress and between stress and job satisfaction. In another study of nurses’ burnout, Alimoglu and Donmez 28 reported that nurses who were exposed to more than 3 h of daylight in a work shift reported higher job satisfaction and lower work-related stress. Dendaas 29 also studied work-related stress among 471 nurses in 39 medical-surgical units from 12 hospitals and found a moderate negative correlation (r = −0.55, p < 0.001) between physical environment attributes (e.g. room size, space around patient beds, individual storage space, and furnishings) and work-related stress.
Although several studies investigated the influence of facility design on healthcare professionals, the number of studies that performed an integrated analysis of comprehensive physical and architectural factors is very small. One example for such comprehensive investigations is the Monjur and Yisong’s 30 study of healthcare providers’ perceptions of design factors related to physical environments in two Chinese hospitals. They gathered perspectives of nurses, doctors, and administrative staff regarding 16 different physical features, including spatial characteristics (indoor plants, interior/exterior landscaping, furniture layout, exterior view from the space, presence of coordinated art objects, pleasant colour scheme, architectural design of the space, location and orientation of the space, spaciousness of working areas, and proximity to wards), environmental (adequate illumination, availability of daylight, thermal comfort, noise level, and air quality and freshness), and maintenance (provision for hand hygiene, cleanliness, and ease of maintenance). They found that cleanliness and ease of maintenance were considered very important, while the presence of coordinated art objects was considered the least important of the analysed design aspects. The respondents also rated air quality, noise level, and thermal comfort as the second, third, and fourth most important items.
The current study expands the findings of previous studies by exploring salient dimensions of caregiver perceptions of architectural and physical features of important environments within healthcare facilities (patient rooms, work spaces, and staff areas) and investigating differences in evaluation of employees across different demographic groups (age, number of years worked in the facility, work shift, and job title).
Methods
Study participants
Healthcare professionals who were employed full-time and involved in delivering care services that require direct interactions with patients were the subject population of this study. Participants were recruited from eight different short-term acute care hospitals run by three non-government and non-profit healthcare organizations in the United States. Regarding the size and age of facilities, facilities represent a wide range of spatial and physical conditions.
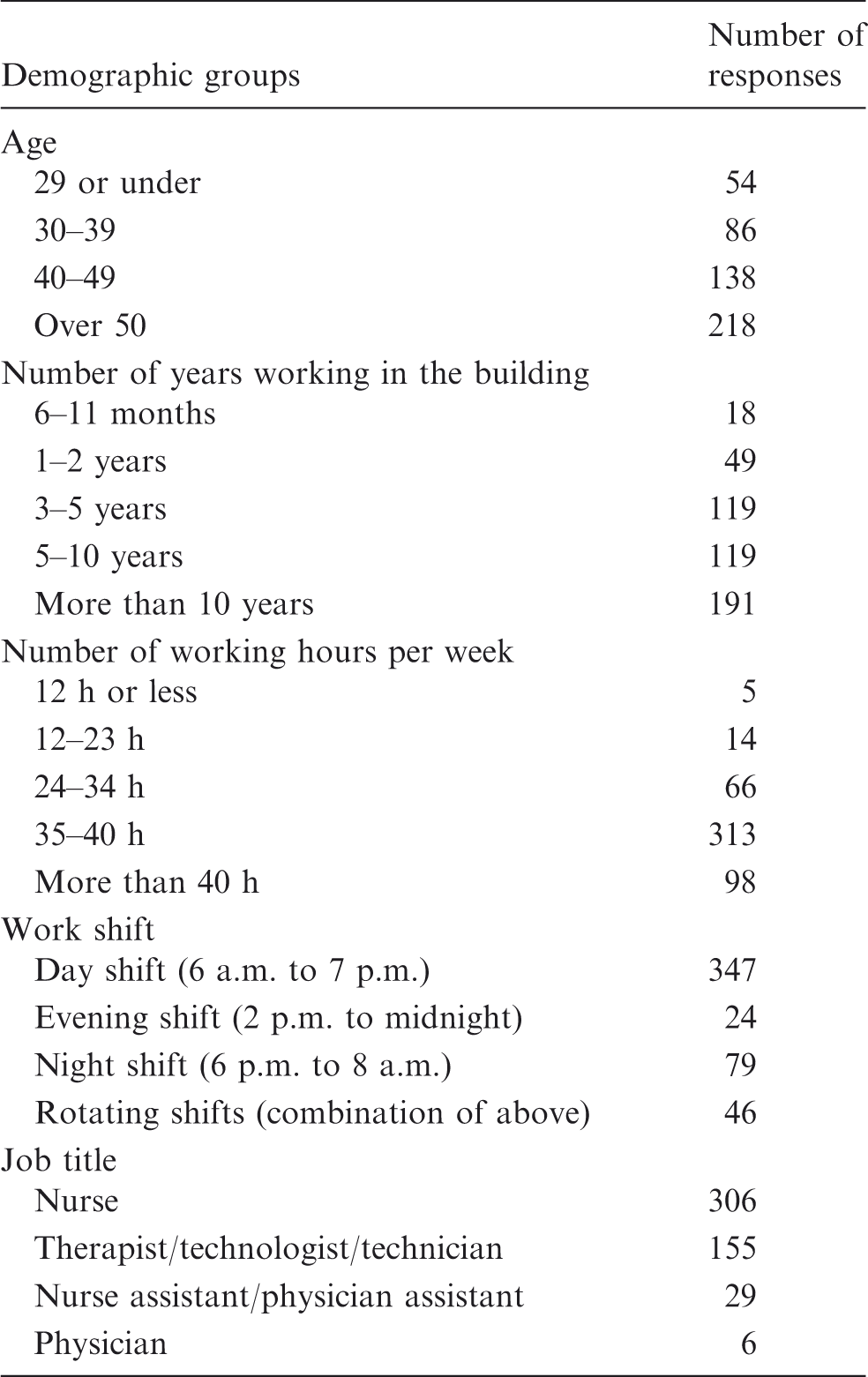
Demographic characteristics of survey participants.
Measurement
The authors used self-reported data of employees’ perceptions of their physical work environments in patient areas, staff work space, and staff areas. Measuring employees’ perceptions provides valuable information because they constitute the most frequent facility user group and are familiar with the relationship of the physical work environment with the requirements of their work. As stated previously, using judgmental measures, where respondents use survey questionnaires to rate various physical features, is a common approach for measuring individuals’ perceptions of their environment. This approach is advantageous for an employee-level analysis as some direct physical measures do not translate into employees’ perceptions of their environment. 31 Moreover, using judgmental measures is specifically helpful in measuring attributes of the physical environment that vary from person to person, 32 such as feelings of cleanliness and the amount of privacy afforded by the building.
The authors first developed a draft questionnaire by incorporating the findings from review of literature and industry guidelines, including U.S. Green Building Council’s (USGBC) Leadership in Engineering and Design (LEED) for Healthcare.
33
Two nurse researchers and two chief nursing officers from participating organizations as well as three staff registered nurses and two healthcare environmental researchers reviewed the draft for accuracy and content validity. Participants were asked to state any deficiencies of the content of the questionnaire and other potential sources of perceptions not covered. The questionnaire had two sections. The first section addressed background and demographic information, and the second section measured individuals’ evaluations of different architectural and physical features of the facility. Section two comprised eight sub-sections covering 27 different features and attributes of the work environment. Figure 1 shows the breakdown of architectural and physical features investigated. In summary, as Harris et al.
25
recommended, architectural features, interior design features, and ambient features were studied. Additionally, based on the comments provided by the review panel, the authors decided to provide definitions of important terms along with more information about environmental features (interior and exterior sources of noise, speech privacy, visual comfort of lights, and controllability of lighting) to ensure the consistency of respondents’ interpretations.
Breakdown of architectural and physical features included in the analysis. Twenty-seven different features (grey boxes) are measured in the second section of the survey.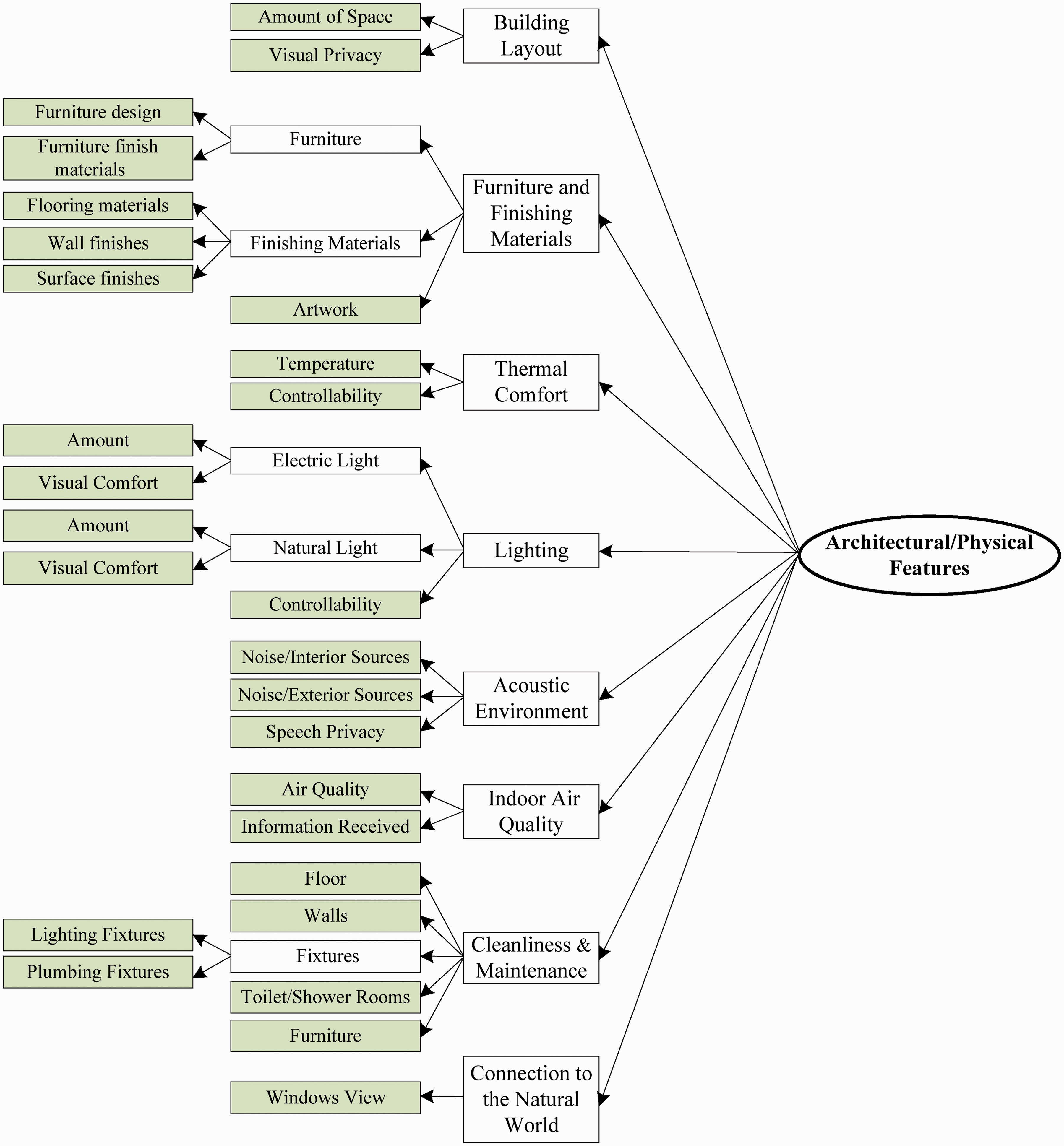
The authors administrated the survey in a web-based platform. To ensure the usability of the online survey instrument, two staff registered nurses, one nurse researcher, one graduate nursing student, and four graduate civil engineering students pilot-tested the online survey. Based on the comments provided by these individuals, minor adjustments were made to the wording of some of the questions. The final version of the online survey questionnaire is accessible using the following link: https://www.surveymonkey.com/s/96JYLBZ. The second section of the survey distinguished between three different types of spaces (patient areas, staff work space, and staff areas) and asked respondents to rate architectural and physical features of each space separately. Employees rated their satisfaction with each feature using a seven-point scale ranging from 1 to 7 (1 = Very dissatisfied; 2 = Mostly dissatisfied; 3 = Somewhat dissatisfied; 4 = Neither satisfied or dissatisfied; 5 = Somewhat satisfied; 6 = Mostly satisfied; and 7 = Very satisfied).
Analysis approach
The IBM® Statistical Package for the Social Sciences (SPSS®) and the Analysis of Moment Structures (AMOS®) version 21 were used for data analysis. The authors performed a separate analysis for patient areas, staff work space, and staff areas. To investigate the dimensionality of employees’ perceptions of their physical work environment, the authors performed principal component analysis (PCA) to determine the number of factors to be extracted. Confirmatory factor analysis (CFA) was then performed to establish the factor structure demonstrated by PCA results, evaluate the adequacy of model specification, and determine the level of association between each architectural feature and a higher order factor labelled as employees’ overall perceptions of their physical work environment. The results of CFA were used to prioritize architectural and physical features based on their association with the higher order factor. Finally, the authors then performed measurement model invariance analysis to identify differences across demographic groups. The authors followed the approach recommended by Chen et al. 34 and used the chi-square difference test 35 for evaluating a series of hierarchically nested models to test invariance across groups.
Results
Preliminary analysis
All variables had acceptable skewedness (lower than 2.0) and kurtosis (lower than 7.0) values for factor analysis with maximum-likelihood estimation. 36 Kaiser–Meyer–Olkin (KMO) 37 measures of sampling adequacy were higher than the minimum acceptable value (0.08) recommended by Kaiser. Bartlett’s tests of sphericity were also statistically significant in all three datasets at p < 0.000, indicating that the variables are not completely uncorrelated.
Principal component analysis
Summary of fit indices for CFA models.
CFA: confirmatory factor analysis.
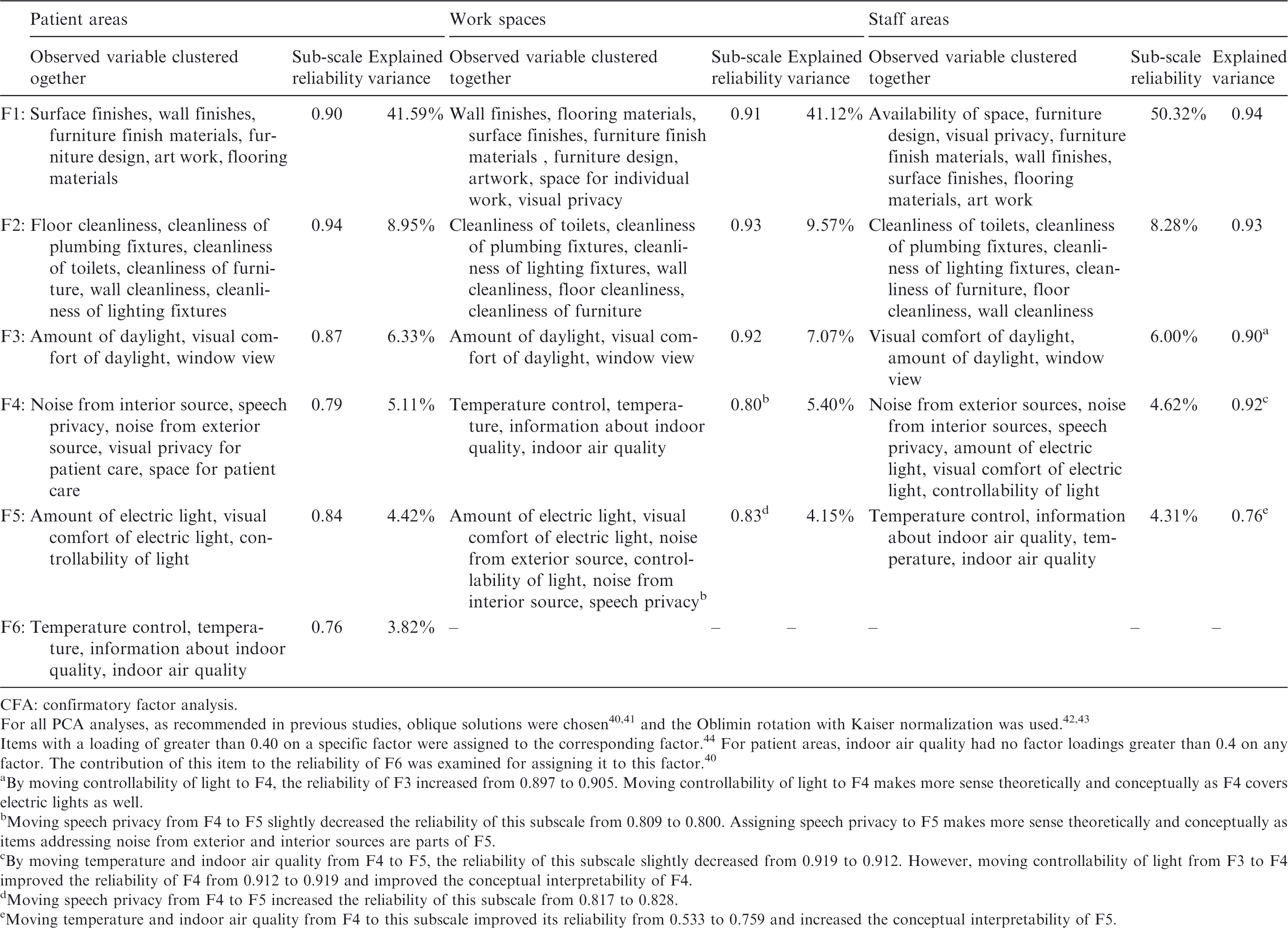
For all PCA analyses, as recommended in previous studies, oblique solutions were chosen40,41 and the Oblimin rotation with Kaiser normalization was used.42,43 Items with a loading of greater than 0.40 on a specific factor were assigned to the corresponding factor. 44 For patient areas, indoor air quality had no factor loadings greater than 0.4 on any factor. The contribution of this item to the reliability of F6 was examined for assigning it to this factor. 40 aBy moving controllability of light to F4, the reliability of F3 increased from 0.897 to 0.905. Moving controllability of light to F4 makes more sense theoretically and conceptually as F4 covers electric lights as well.
Moving speech privacy from F4 to F5 slightly decreased the reliability of this subscale from 0.809 to 0.800. Assigning speech privacy to F5 makes more sense theoretically and conceptually as items addressing noise from exterior and interior sources are parts of F5.
By moving temperature and indoor air quality from F4 to F5, the reliability of this subscale slightly decreased from 0.919 to 0.912. However, moving controllability of light from F3 to F4 improved the reliability of F4 from 0.912 to 0.919 and improved the conceptual interpretability of F4.
Moving speech privacy from F4 to F5 increased the reliability of this subscale from 0.817 to 0.828.
Moving temperature and indoor air quality from F4 to this subscale improved its reliability from 0.533 to 0.759 and increased the conceptual interpretability of F5.
All subscales exceeded the minimum level of internal reliability and after a few modifications for improving conceptual interpretations of subscales, structuring of variables in all three data sets resulted in simple and theoretically meaningful subdimensions.45,46 In summary, items measuring furniture and finishing materials clustered together in all three data sets and explained more than 50% of the variability in data, followed by items measuring cleanliness and maintenance. Daylight and window view items load on a common factor, and items related to the acoustic environment and space layout are part of the same factor as well. Moreover, in all three datasets, items measuring temperature and indoor air quality were clustered together. Because all subscales were interpretable and none of the items appear to be redundant, the authors decided to keep all 27 items (all observed variables) in the analysis.
Confirmatory factor analysis
Summary of fit indices for CFA models.
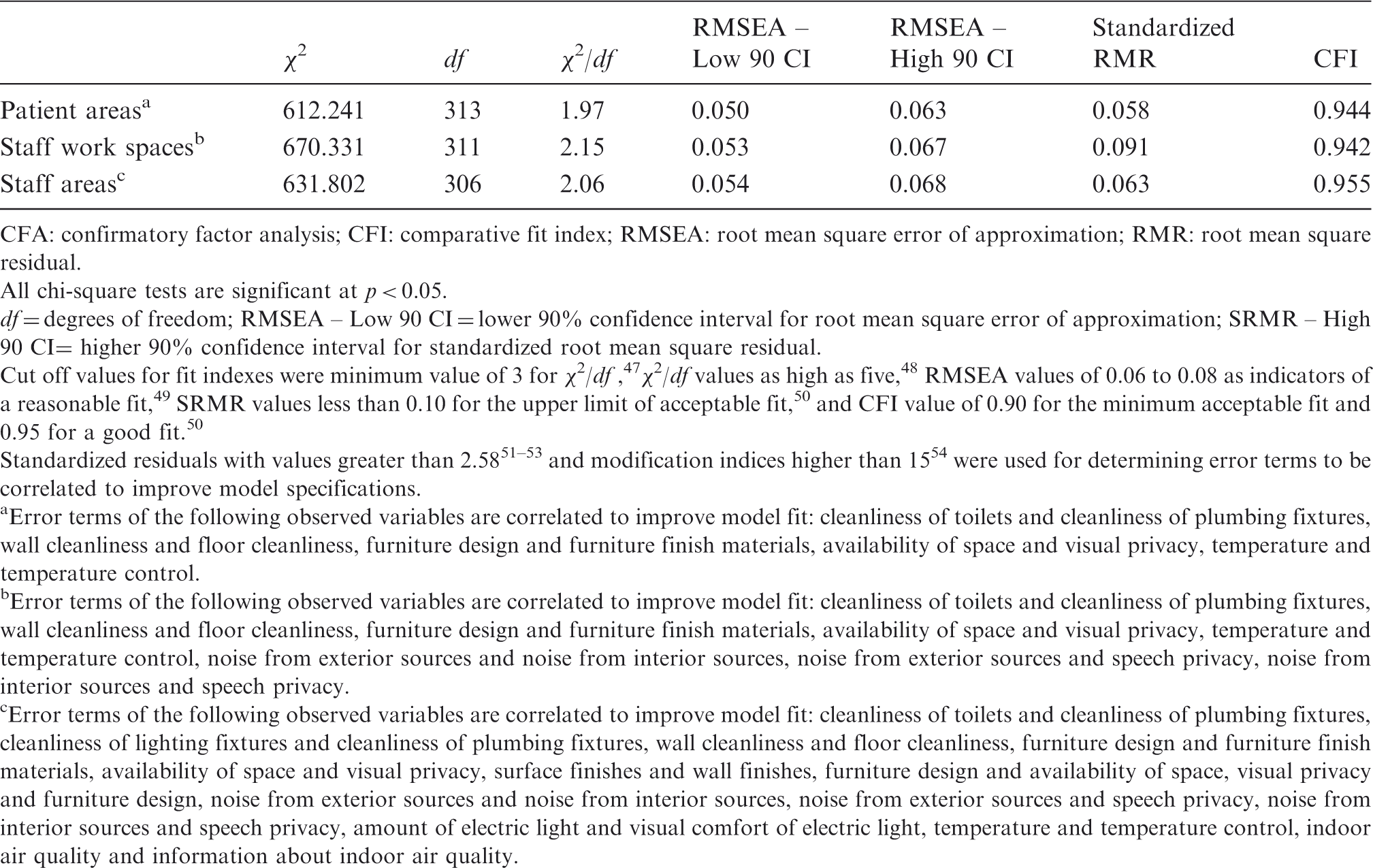
CFA: confirmatory factor analysis; CFI: comparative fit index; RMSEA: root mean square error of approximation; RMR: root mean square residual.
All chi-square tests are significant at p < 0.05.
df = degrees of freedom; RMSEA – Low 90 CI = lower 90% confidence interval for root mean square error of approximation; SRMR – High 90 CI= higher 90% confidence interval for standardized root mean square residual.
Cut off values for fit indexes were minimum value of 3 for χ2/df , 47 χ 2 /df values as high as five, 48 RMSEA values of 0.06 to 0.08 as indicators of a reasonable fit, 49 SRMR values less than 0.10 for the upper limit of acceptable fit, 50 and CFI value of 0.90 for the minimum acceptable fit and 0.95 for a good fit. 50
Standardized residuals with values greater than 2.5851–53 and modification indices higher than 1554 were used for determining error terms to be correlated to improve model specifications.
Error terms of the following observed variables are correlated to improve model fit: cleanliness of toilets and cleanliness of plumbing fixtures, wall cleanliness and floor cleanliness, furniture design and furniture finish materials, availability of space and visual privacy, temperature and temperature control.
Error terms of the following observed variables are correlated to improve model fit: cleanliness of toilets and cleanliness of plumbing fixtures, wall cleanliness and floor cleanliness, furniture design and furniture finish materials, availability of space and visual privacy, temperature and temperature control, noise from exterior sources and noise from interior sources, noise from exterior sources and speech privacy, noise from interior sources and speech privacy.
Error terms of the following observed variables are correlated to improve model fit: cleanliness of toilets and cleanliness of plumbing fixtures, cleanliness of lighting fixtures and cleanliness of plumbing fixtures, wall cleanliness and floor cleanliness, furniture design and furniture finish materials, availability of space and visual privacy, surface finishes and wall finishes, furniture design and availability of space, visual privacy and furniture design, noise from exterior sources and noise from interior sources, noise from exterior sources and speech privacy, noise from interior sources and speech privacy, amount of electric light and visual comfort of electric light, temperature and temperature control, indoor air quality and information about indoor air quality.
Invariance analysis and hypotheses testing
After confirming the factor structure, multiple-group CFA was applied to the best-fitting models to investigate the invariance of the measurement model across demographic variables. The authors assumed that factor structures are identical across groups. To test the other forms of invariance, 12 different models were analysed to examine the invariance of the measurement models in patient areas, work spaces, and staff areas. The hypotheses of these analyses are as follows:
Summary of chi-square difference test statistics for measurement model invariant analysis.
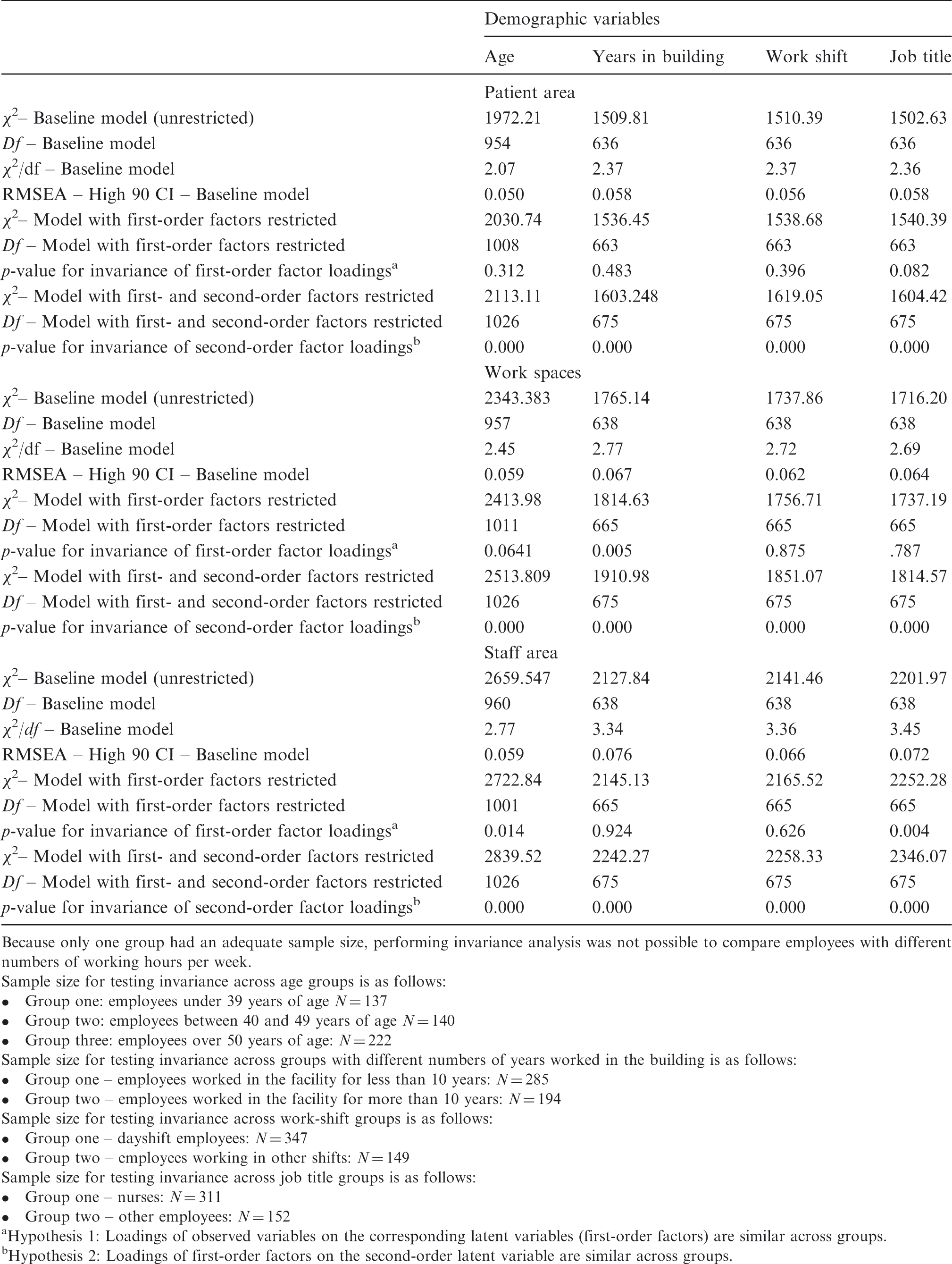
Because only one group had an adequate sample size, performing invariance analysis was not possible to compare employees with different numbers of working hours per week.
Sample size for testing invariance across age groups is as follows: • Group one: employees under 39 years of age N = 137 • Group two: employees between 40 and 49 years of age N = 140 • Group three: employees over 50 years of age: N = 222
Sample size for testing invariance across groups with different numbers of years worked in the building is as follows: • Group one – employees worked in the facility for less than 10 years: N = 285 • Group two – employees worked in the facility for more than 10 years: N = 194
Sample size for testing invariance across work-shift groups is as follows: • Group one – dayshift employees: N = 347 • Group two – employees working in other shifts: N = 149
Sample size for testing invariance across job title groups is as follows: • Group one – nurses: N = 311 • Group two – other employees: N = 152
Hypothesis 1: Loadings of observed variables on the corresponding latent variables (first-order factors) are similar across groups.
Hypothesis 2: Loadings of first-order factors on the second-order latent variable are similar across groups.
Age, number of years in building, work shift, and job title were selected for invariance analysis; p-values for the invariance of first-order factor loadings and second-order factor loadings are specified in Table 5, and p-values lower than 0.05 would indicate that study hypothesis is rejected. Overall, invariance analysis showed that employees’ perceptions of their physical work environment are different across demographic groups.
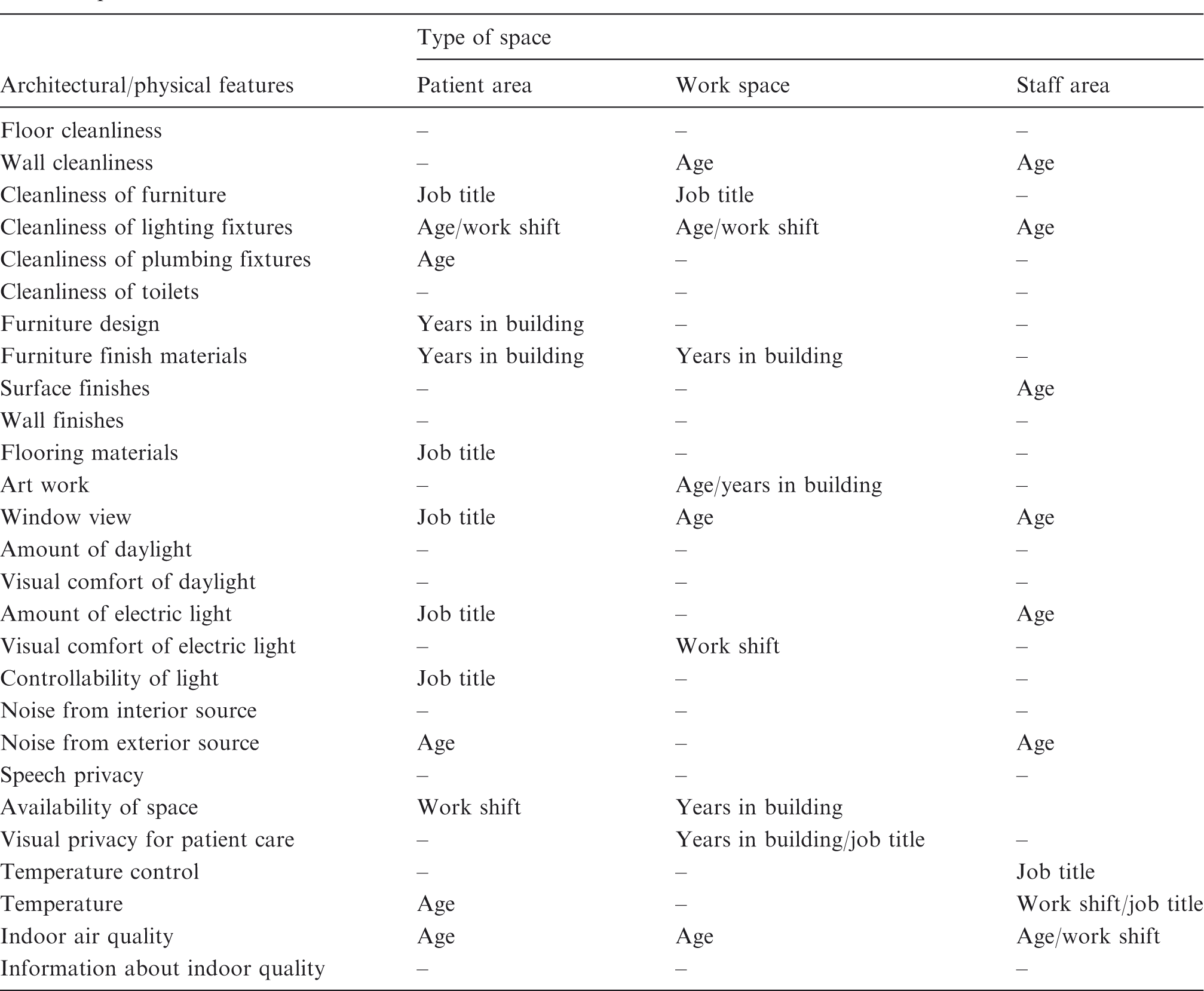
Pairwise parameter comparison across groups
Architectural/physical features contributing to differences in caregiver’s perception of the built environment in different spaces.
Discussion
In general, PCA and CFA results for the patient areas were more plausible than the results for work spaces and staff areas. This can be explained by the fact that, in comparison with other spaces, designers and facility owners likely pay more attention to well-designed patient and family areas. Additionally, employees may use this area more frequently, resulting in a clearer perception and evaluation of its features. As far as different demographic groups are considered, employees younger than 40 years and those who worked in the facility for less than 10 years are more perceptive of the physical work environment in patient areas, specifically artwork, furniture, and finish materials. As for work shift, the difference between estimated effect sizes is generally very small. However, the analysis showed that in staff areas and work spaces, dayshift employees care more about the acoustic environment, electric lighting, and space layout. Finally, differences of estimated effect sizes are very small across job titles. In general, with few exceptions, nurses care more about features of the patient areas, while non-nurse staff members care more about features of the staff areas.
Discussion regarding differences across spaces
A comparison of effect sizes associated with different features across spaces indicates that the function of an environment affects the dimensions along which employees evaluate it. For example, electric lighting (amount and visual quality of electric light) is a more salient feature of employees’ work spaces where they need task light for performing activities such as reading patents’ medical records or charting. Buchanan et al. 55 found that the rate of prescription-dispensing errors was associated with lower levels of illumination. Additionally, temperature (thermal comfort) is perceived as one of the most highly valued attributes of the environment in staff areas, while this is not the case in patient areas and work spaces. Lower level of association between thermal comfort and overall evaluation of the physical work environment in patient areas can be explained by the fact that caregivers are aware that the purpose of measuring and controlling temperature in patient rooms is providing a safe and comfortable environment for patients and families. Accordingly, staff members do not show their appreciation of it in patient areas. However, staff areas are solely used by caregivers and because of that thermal comfort is highly valued by employees.
Also, specifically in patient and staff areas, estimated effect sizes for temperature level are generally higher than effect sizes for temperature control. Visual comfort of electric light also has a greater effect size than controllability of lightings. As far as choice and control are considered, Shepley 56 noted that access to options and providing the ability to manipulate the physical environment regarding lighting, temperature, and acoustic environments are critical to stress reduction for employees. This study suggests that when environmental factors such as the amount of lighting and temperature are in the appropriate range, employees feel like the factors are under control and do not care much about personal control.
Discussion regarding similarities in different spaces
Despite variances in the importance of architectural/physical features in different types of spaces, certain patterns exist. The analysis found that items addressing indoor air quality and finishing materials (furniture, surfaces, and walls) emerged as highly associated with the evaluation of the physical work environment, regardless of the function of the environment and demographic characteristics of employees. Previous studies showed that furniture and finish materials contribute considerably to the design quality of the environment and to fostering a more home-like, less institutional feeling.3,57 Additionally, carpeting and rubber flooring that have softer properties can be used to mitigate some of the effects of long work hours and excessive workload, including fatigue. 58 Previous studies also provided evidence that the ergonomic design of work areas, including furniture, reduces staff back pain and work-related injuries. 59 The importance of indoor air quality as a concern for employees is also reported in previous studies. In an exploratory analysis of hospital design and staff perceptions, that air quality was mentioned by employees as one of the top three factors having a positive impact on the quality of their work life. 4 Moreover, in a study of healthcare providers’ perception of physical environment factors in two Chinese hospitals, Monjur and Yisong 30 found that in terms of mean response scores, air quality and freshness was ranked the second most important environmental factor.
The fact that indoor air quality and finishing materials have the highest relative importance among 27 features included in the analysis indicates that healthcare professionals are highly cognizant of health and safety-related risks at work, where they often use many highly toxic chemicals such as cleaners and disinfectants. According to the U.S. Bureau of Labor Statistics, the rate of occupational injuries and illnesses in hospitals is about 80% higher than the rate for all of the private industry. 60 Previous studies also reported that sick building syndrome (SBS) is generally high in hospitals buildings, and health-related complaints are higher in hospitals with SBS. 3 Note that the analysis also found that employees also highly value information they receive about the organizational efforts in reducing the quantity of indoor air contaminants, as evidenced by standardized effect sizes reported in Appendix 1.
As for noise levels, the current study found that in all three types of spaces, night and evening shift staffs are more sensitive to high noise levels. The night and evening shift staff may have higher sensitivity to noise, as previous studies 61 reported that hospitals are generally less noisy at night. Additionally, shift work may cause negative physical and psychological effects62–64 making night and evening shift staffs more susceptible to environmental stressors such as noise. The analysis also found that among the three types of spaces, the highest association between noise control and employees’ overall evaluations of the environment exists in staff areas. This indicates that quietness of staff areas is highly valued by employees. As pointed out in previous studies, this might indicate that employees recognize that noise in patient rooms and work areas (generated by alarms, paging systems, visitors, and staff conversations) is unavoidable and should not have a negative impact on their work.65,66 In comparison, in staff areas, employees expect lower levels of noise and value quietness to a greater extent. Another important finding with respect to perception of noise is that employees care more about control of interior noise than exterior noises. Joseph and Ulrich’s 61 literature review found that sounds contributing to the loud noise levels in hospitals come from interior sources such as mechanical equipment, staff, and visitors.
One of the important unexpected finding of this study is the low association of daylight and view items with employee’s perception of their work environment. The current study found that electric light has a higher association with employees’ perceptions across all demographic variables and in all three types of spaces. Although previous studies have found that daylight is not inherently better than artificial lighting for performance of most visual tasks. Previous studies also found that healthcare employees appear to feel better where natural daylight and views to nature are provided.3,67,68 The small effect sizes found for daylight and view probably should not be interpreted as if employees do not care about daylight and view in hospitals. Rather, it shows the higher ‘relative’ importance of other environmental features included in this study. In other words, the analysis suggests that employees give a higher priority to the design of furniture, indoor air quality, finishing materials, thermal comfort, and noise control, all of which are essential for safe and efficient delivery of care. Lower relative ranking of window view and daylight than other environmental and maintenance items is also reported by Monjur and Yisong. 30 They suggested that window view and daylight appear to be important in studies that look at individual aspects rather than the integrated whole.
Finally, the analysis found that compared with other spaces, artwork placed in staff areas is valued to a greater extent. According to Mroczek et al., 4 employees are not able to appreciate artwork in patient and family areas because of their work schedules. Interestingly enough, estimated effect size also indicated that compared with patient areas and work spaces, daylight and window view in staff areas are valued to a greater extent.
Practical implications
Attention to health and well-being of healthcare professionals become more important when we consider the fact that employees are the greatest cost in an organization. 69 According to the American Hospital Association, approximately 60 cents of every dollar spent is allocated for compensation of employees and other hospital workers. Human resource-related expenses are higher than other essential expenses, including medication, devices, and other supplies as well as improvements to treatment facilities, installation of or upgrades to health information technologies, utilities, and liability coverage. 70
Previous research on job satisfaction of healthcare professionals have reported that nurses and other employees rate the physical work environment more negatively than other characteristics of the environment.21,22,71 Findings of this study provide healthcare architects and facility owners with empirical evidence to inform design decisions by showing the most important factors that may improve employees’ satisfaction with architectural and physical features of their workplace. Informed decision making in the design phase is important because environment features are determined during early design stages, and subsequent modifications during facility operation are difficult to implement.
The most important finding of this study is that finishing materials play a critical role in improving staff satisfaction with the physical environment across all spaces. In addition to visual and physical properties of finishing materials, such as their pattern, colour, and texture, the correct selection of finishing materials has an influence on indoor air quality and caregiver safety. Analysis indicates the importance of providing comfortable furniture with ergonomic design in patient areas and staff work spaces. Ergonomic design includes features related to the adjustability of furniture, inclusion of armrests for support, locking casters, and contoured edges. 72 In addition to design features, this study also shows the importance of facility operation such as maintaining indoor air quality and thermal comfort. Findings also suggest that proper facility operation can compensate for functions facility design does not offer. For example, employees care less about personal control over room temperature or lighting devices when they are in the appropriate range. Finally, the analysis found that as far as employees are considered, improving visual quality by incorporating pieces of artwork and providing outside view and daylight is more effective in staff areas than in patient rooms and work spaces.
Appendix 1 shows the level of association between different architectural and physical features and employees’ evaluation of their physical work environment within each space. Cells with fully filled circles indicate that the corresponding architectural/physical feature has the highest ‘relative’ level of importance for the corresponding demographic group. In comparison, a white solid circle represents the lowest level of importance. Hospital designers and owners may use the information provided in Appendix 1 to determine the most effective improvements in the facility based on the demographic characteristics of their employees.
Study limitations and directions for future studies
Approaches such as analysis of variance commonly used for analysing the differences between group means do not account for underlying factor structures and the relationship between observed variables. Using second-order factor models added to the robustness of the analysis approach. However, certain limitations of this study need to be discussed. First of all, although CFA results indicated acceptable fit and satisfactory model specification in all three data sets, full psychometric evaluation of the measurement instrument was beyond the scope and purpose of this study. Instrument development is an iterative process requiring robust investigations to establish the reliability and validity of the instrument and provide evidence to support its psychometric integrity.
Additionally, because the number of variables incorporated in the measurement model is high, the sample size required for each categorical group was high. Although multiple sites participated in this study, the number of responses collected from certain demographic groups was not adequate to include them in the multigroup analysis, and several groups had to be combined to obtain adequate sample sizes. Furthermore, although the analysis did not find significant differences among nurses and employees, or in perceptions of employees working the day shift versus other shifts, there may be differences between subcategories. More specifically, the influence of work requirements in different medical departments should be taken into account before generalizing the findings of this study. For example, a greater need for cleanliness exists in departments such as surgery, emergency, and intensive care units where the risk of infection transfer from patients to employees might be higher. 30
With respect to differences found in different spaces, future studies should focus on understanding differences in activities and tasks performed in each space. Data could be collected mapping staff activities, recording location, activity, and time data to identify medical staff activity patterns and linking them with employees’ evaluations of architectural and physical features of each space. Future studies should also investigate those outcomes that are different than what was expected (such as window view and daylight) by follow-up detailed analysis of these specific factors via surveys or interviews.
Finally, besides employees’ evaluations, attitudinal outcomes, such as job satisfaction, organizational commitment, job-related well-being, and organizational commitment should be investigated in future studies.
Conclusion
This study highlights the importance of attention to caregiver needs for a safe and comfortable work environment. Among the 27 different environmental features investigated in this study, the analysis found that finishing materials and indoor air quality have the highest levels of association with employees’ overall satisfactions with their physical work environment, regardless of their individual characteristics. Additionally, employees highly valued furniture design and thermal comfort. In comparison, features that address the visual quality of the work environment, such as window view and pieces of artwork, were found to have smaller associations with employees’ evaluations. However, in non-clinical areas, where safety concerns are not as high as such concerns in patient areas and work spaces, staff appreciate features improving the visual quality of their rest area, such as daylight, window view, and the presence of artwork.
In general, this study found that the function of an environment affects the dimensions along which employees evaluate it. The study also found that demographic variables also influence employees’ evaluations of architectural and physical features. In general, employees younger than 40 years and those who had worked in the facility for less than 10 years will most appreciate the improvements in the architectural/physical features of patient rooms.
Footnotes
Acknowledgements
The authors would like to thank Professor Kirk Hamilton for his assistance in the recruitment of study participants. The authors would also like to express their deepest gratitude to the following individuals for their continual support during the course of this study: James Gaskin, Assistant Professor of Information Systems at Brigham Young University, Provo, Utah, Teri Weir, Charge Nurse Medical-Surgical floor at Texas Health Recourses; Kathleen Baldwin, Nurse Researcher at Texas Health Resources; Paula Spears, Vice President of Professional Practice, Research, and Magnet Program at Texas Health Resources; Ann Hendrich, Vice President of Clinical Excellence Operations at Ascension Health; Maria Strom, Chief Nursing Officer and Vice President of Patient Services & Operations at St. John Macomb-Oakland Hospital; and Maryann Barnes, Chief Nursing Officer and Vice President of Patient Care Services at St. John Hospital and Medical Center. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.