
Abstract
Background:
This cohort study evaluates the American Society of Anesthesiologists (ASA) Physical Status Classification as a predictor for long-term survival after major abdominal cancer surgery and reassesses its conventional use for perioperative risk assessment.
Method:
Using data from the Norwegian Registry for Gastrointestinal Surgery (NORGAST), we identified patients who underwent formal resection for colorectal cancer, as well as patients undergoing surgery for pancreatic or liver malignancies, between January 2016 and December 2023. Log-rank analyses were used to assess survival differences according to ASA class.
Results:
This study analyzed 20,784 patients undergoing surgery for colorectal cancer and 4792 patients undergoing surgery for pancreatic or liver malignancy. After excluding patients who died within 90 days postoperatively, 20,244 colorectal and 4702 pancreatic/liver patients remained for survival analysis. ASA class was associated with postoperative morbidity, mortality, and length of stay after colorectal cancer surgery; however, a very large number of patients was required to demonstrate a modest percentage-point differences. In both log-rank and multivariable analyses, ASA class was strongly associated with long-term survival after colorectal cancer surgery (p < 0.001) and after resection for pancreatic and liver malignancies (p < 0.001). This association persisted across age-matched cohorts, and ASA class outperformed age in multivariable survival analysis.
Conclusion:
Although the ASA classification demonstrates clear relevance in predicting long-term survival after major abdominal cancer surgery, its clinical utility for perioperative risk assessment appears limited. Despite criticisms regarding subjectivity and moderate inter-rater reliability, ASA classification determined by experienced professionals may capture patient factors beyond documented comorbidities, potentially reflecting underlying disease severity or patient resilience.
Introduction
The American Society of Anesthesiologists (ASA) Physical Status Classification System has been in use for over 60 years and was developed to communicate patient’s comorbidity burden before anesthesia rather than to predict surgical risk.1,2 Despite well-recognized limitations—including subjectivity and moderate inter-rater variability—it remains widely used and has repeatedly shown prognostic relevance in perioperative settings.3–12
The ASA classification has been associated with long-term outcomes, including overall survival following surgery.13,14 This association is conceptually plausible, as patients with more severe systemic disease may have reduced physiological reserves or limited access to adjuvant therapy. However, the published literature remains inconsistent.15–17 Differences in cancer types, stage distributions, comorbidity profiles, and other variations between cohorts likely contribute to contradictory findings. Whether ASA classification provides meaningful prognostic information beyond traditional risk factors, particularly in settings where cancer recurrence is the dominant cause of mortality, remains unclear.
The primary aim of this study was to evaluate the association between the ASA classification and long-term overall survival after major abdominal cancer surgery from Norwegian Registry for Gastrointestinal Surgery (NORGAST). As a secondary aim, we assessed the relationship between ASA class and postoperative complications to clarify its clinical value for perioperative risk stratification.
In addition to colorectal cancer (CRC) surgery, we decided to further explore whether ASA remains prognostic in settings where cancer-specific mortality predominates, by examining patients undergoing surgery for pancreatic or liver malignancies. These complementary cohorts provide an opportunity to evaluate the relevance of ASA classification across distinct oncologic contexts.
Methods
Patients and management
This study was approved by the regional ethics committee (protocol number 2024/761406) and prepared according to the STROBE guidelines. 18
NORGAST is a nationwide, prospective registry established in 2014, with an 87.8% coverage rate across Norwegian hospitals performing major gastrointestinal, hepatobiliary, or pancreatic resections. Coverage refers to the proportion of registered procedures relative to those reported for reimbursement. With a limited set of digital variables, 19 NORGAST enables efficient data entry and broad clinical adoption. NORGAST was queried to identify patients undergoing formal resection for CRC, as well as patients undergoing surgery for pancreatic or liver malignancies, from January 2016 until December 2023.
The following de-identified variables were extracted: diagnosis (ICD-10), age, body mass index (BMI), comorbidities (heart disease, lung disease, diabetes) ASA classification (ASA 1–5; ASA-E was not used), WHO/ECOG performance status, preoperative albumin and C-reactive protein, Modified Glasgow Prognostic Score, 20 tumor location, neoadjuvant therapies, type of resection, elective versus acute surgery, open versus laparoscopic access, relaparotomies, other interventions, single organ failure, multiorgan failure, 90-day mortality, Accordion grade of postoperative complications, 21 length of stay, discharge destination, readmissions, and last follow-up date or date of death.
In Norway, more than half of all liver resections are performed for colorectal metastases; thus, some patients are represented in both the CRC cohort and the liver malignancy cohort. This overlap was not considered a major limitation because no statistical comparisons between the two cohorts were performed. The hepatopancreatic cohort was included as a proof-of-concept group to evaluate whether the prognostic value of ASA extends to malignancies associated with high cancer-specific mortality. Survival analyses were conducted from the date of surgery, with separate starting points for primary colorectal procedures and liver resections.
ASA class was assigned bedside by the responsible anesthesiologist on the day of surgery and recorded in the electronic patient record. NORGAST is updated weekly with 30-day postoperative data. Mortality information is retrieved from the national population registry and continuously updated to allow calculation of 90-day mortality and overall survival. Postoperative complications occurring within 30 days are recorded and graded according to the Accordion classification, 21 and these data were used to assess the association between ASA class and postoperative morbidity in the CRC cohort.
Management and surgical treatment followed national guidelines at 33 hospitals treating colon cancer, 23 treating rectal cancer, and 5 treating hepatobiliary cancer. 22
Statistical analysis
Normality of continuous variables was assessed using the Kolmogorov–Smirnov test. Normally distributed variables are presented as mean with standard deviation (SD) and compared using independent t-tests or one-way analysis of variance (ANOVA). Non-normally distributed variables are presented as median with range and compared using Mann–Whitney U test or Kruskal–Wallis test. Categorical variables were compared using Pearson’s chi-square test. A p-value <0.05 was considered statistically significant.
Survival differences across ASA classes were assessed using Kaplan–Meier curves with log-rank tests. For improved graphical clarity, patients at risk were reported in the overall survival plots, and censored cases were marked with a “+” in the age-matched analyses. Patients who died within 90 days of surgery were excluded from survival analyses to reduce the influence of postoperative mortality, which is more common in higher ASA classes and could otherwise obscure patterns of long-term, non-surgical mortality.
Multivariable survival analyses were performed using Cox regression. All covariates were entered simultaneously using the enter method to estimate adjusted hazard ratios. Due to large sample size, variables were selected based on clinical relevance (covariates depicted in Table 3) rather than significance in univariable testing, to avoid potential biases associated with data-driven variable selection.
For age-matched survival analyses, patients were grouped into age was grouped into conventional 10-year categories (<50, 50–59, 60–69, 70–79, 80–89, and ⩾90 years). This approach was chosen for clinical interpretability and adequate subgroup size. No data-driven cutoffs were explored.
Missing data were minimal for all variables. For most variables, complete data were available, and for those with missing values, the proportion was very low and considered negligible. Therefore, no imputation was performed. Analyses were conducted using available data for each variable (available case analysis), and patients were not excluded from the overall dataset due to missing values in individual variables. SPSS v.23.0 (SPSS Inc., IBM, Chicago, IL, USA) was used to perform the statistical analyses.
Results
ASA classification and long-term survival after CRC surgery
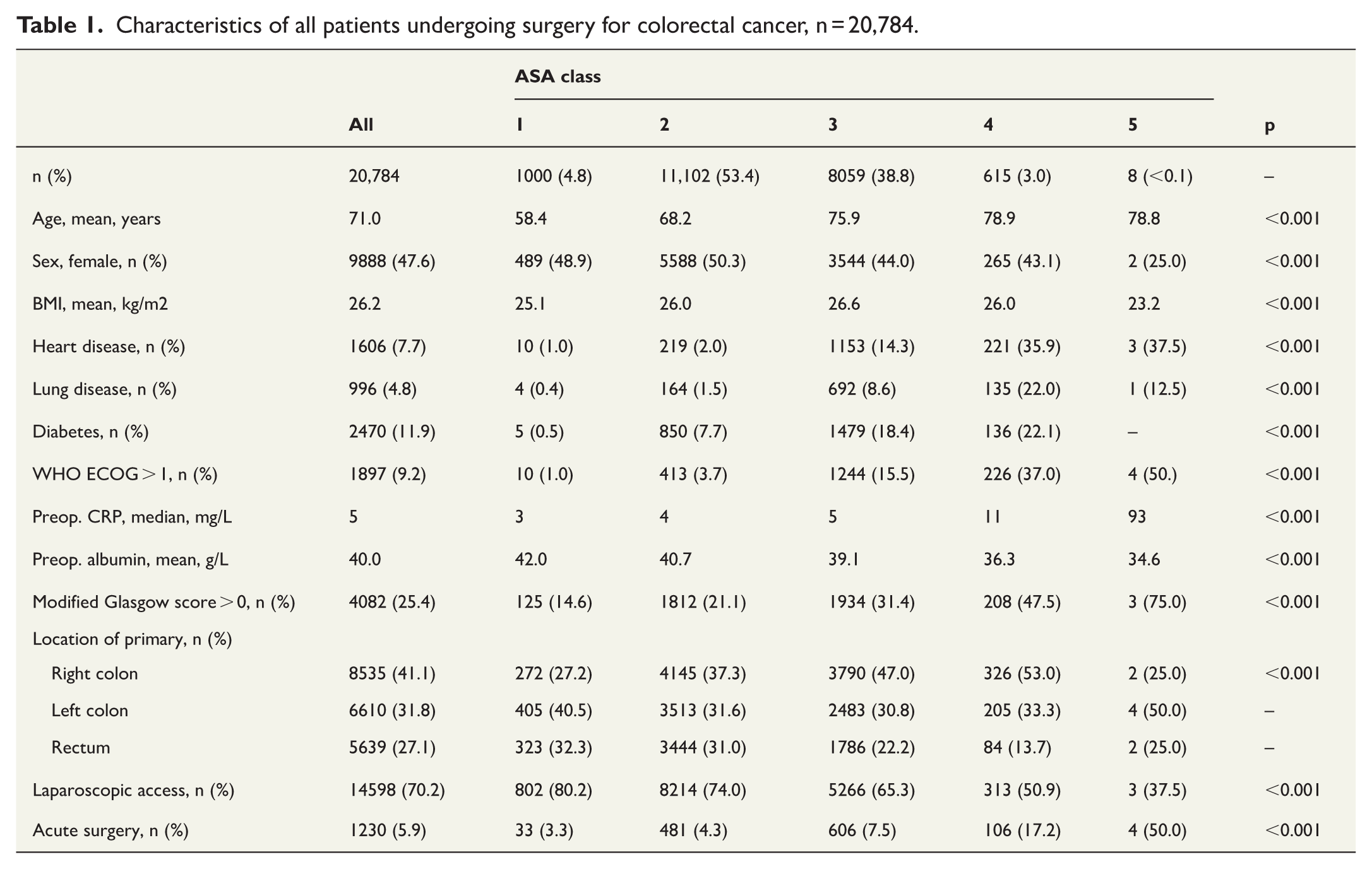
Between January 2016 and December 2023, 20,784 patients underwent surgery for CRC (Fig. 1). All patients had a minimum follow-up of 90 days, and the median follow-up was 45.8 months. ASA class distribution was ASA 1, 1000 (4.8%) patients; ASA 2, 11,102 (53.4%); ASA 3, 8059 (38.8%); ASA 4, 615 (3.0%); and ASA 5, 8 (<0.1%). The mean age at surgery was 71.0 years, increasing progressively with higher ASA class (ASA 1: 58.4 years; in, ASA 2: 68.2 years; ASA 3: 75.9 years; ASA 4: 78.9 years; ASA 5: 78.8 years). Baseline characteristics and postoperative adverse events are presented in Table 1 and Table 2, respectively.
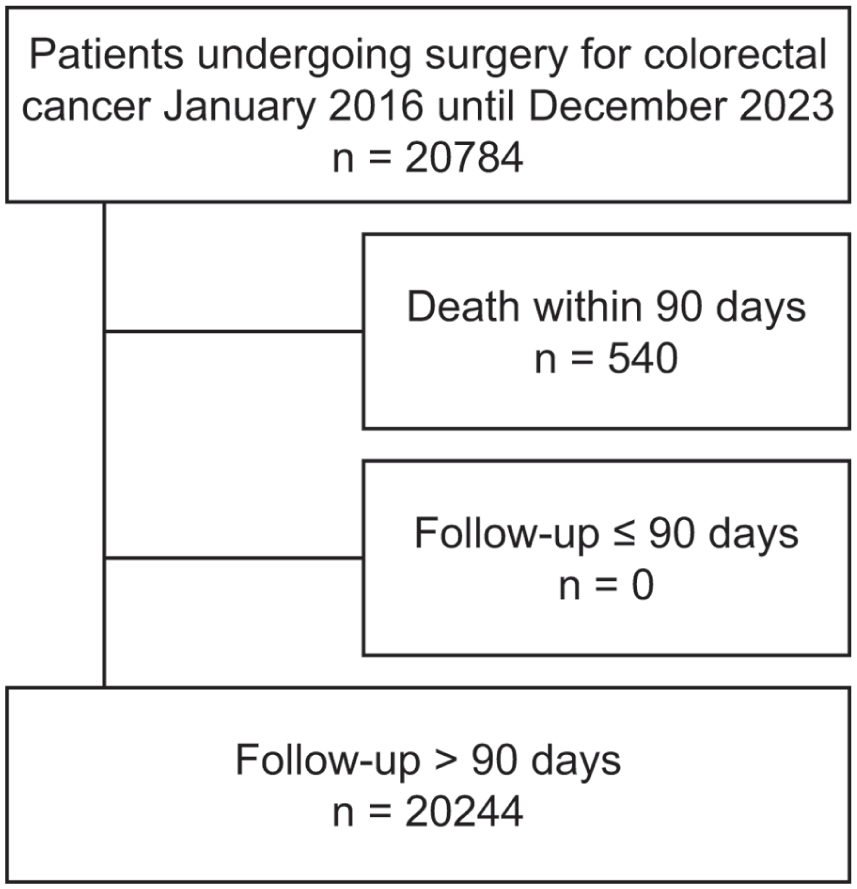
Flowchart of patients undergoing surgery for colorectal cancer and included in the survival analysis.
Characteristics of all patients undergoing surgery for colorectal cancer, n = 20,784.
Postoperative adverse events in all patients undergoing surgery for colorectal cancer, n = 20,784.
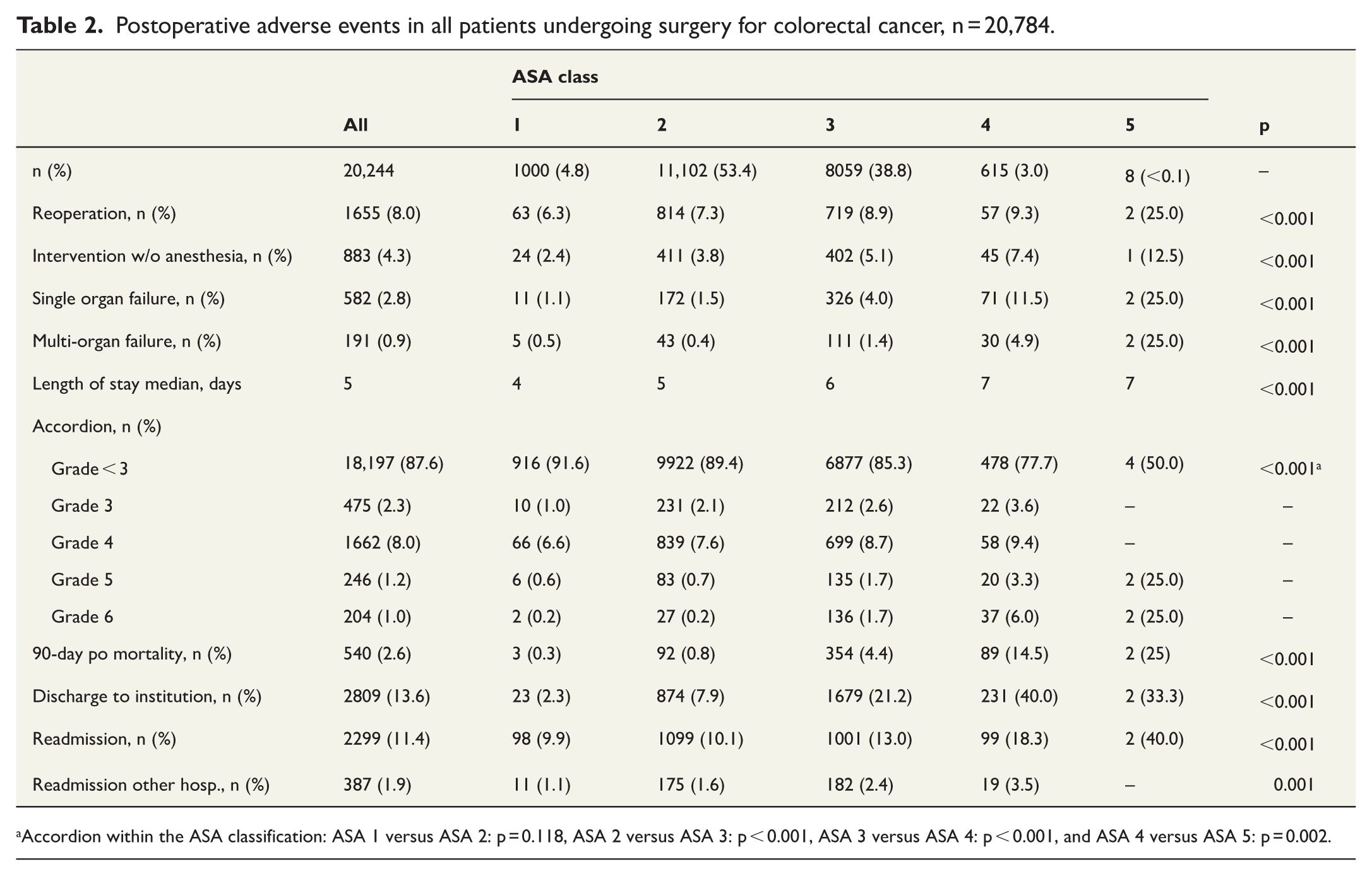
Accordion within the ASA classification: ASA 1 versus ASA 2: p = 0.118, ASA 2 versus ASA 3: p < 0.001, ASA 3 versus ASA 4: p < 0.001, and ASA 4 versus ASA 5: p = 0.002.
To minimize the effect of postoperative mortality, patients who died within 90 days of surgery were excluded from survival analyses, leaving 20,244 patients for evaluation (Fig. 1).
Kaplan–Meier analysis demonstrated significant differences in overall survival between ASA classes (Fig. 2). Survival curves were clearly separated for all adjacent ASA classes, except between ASA 4 and ASA 5, likely reflecting the very small number of patients classified as ASA 5.
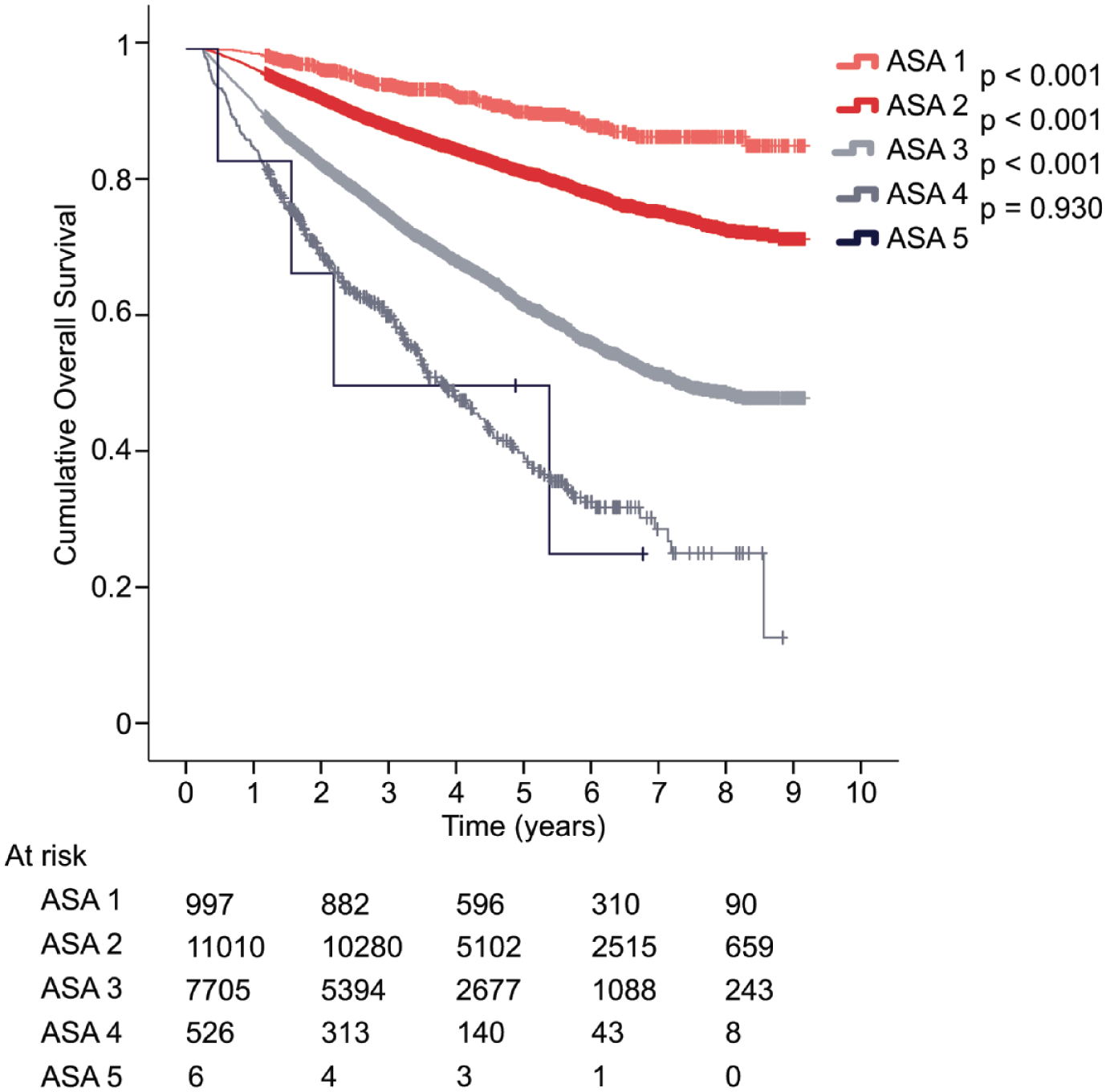
Cumulative overall survival among patients undergoing surgery for colorectal cancer (n = 20,244), stratified by ASA class.
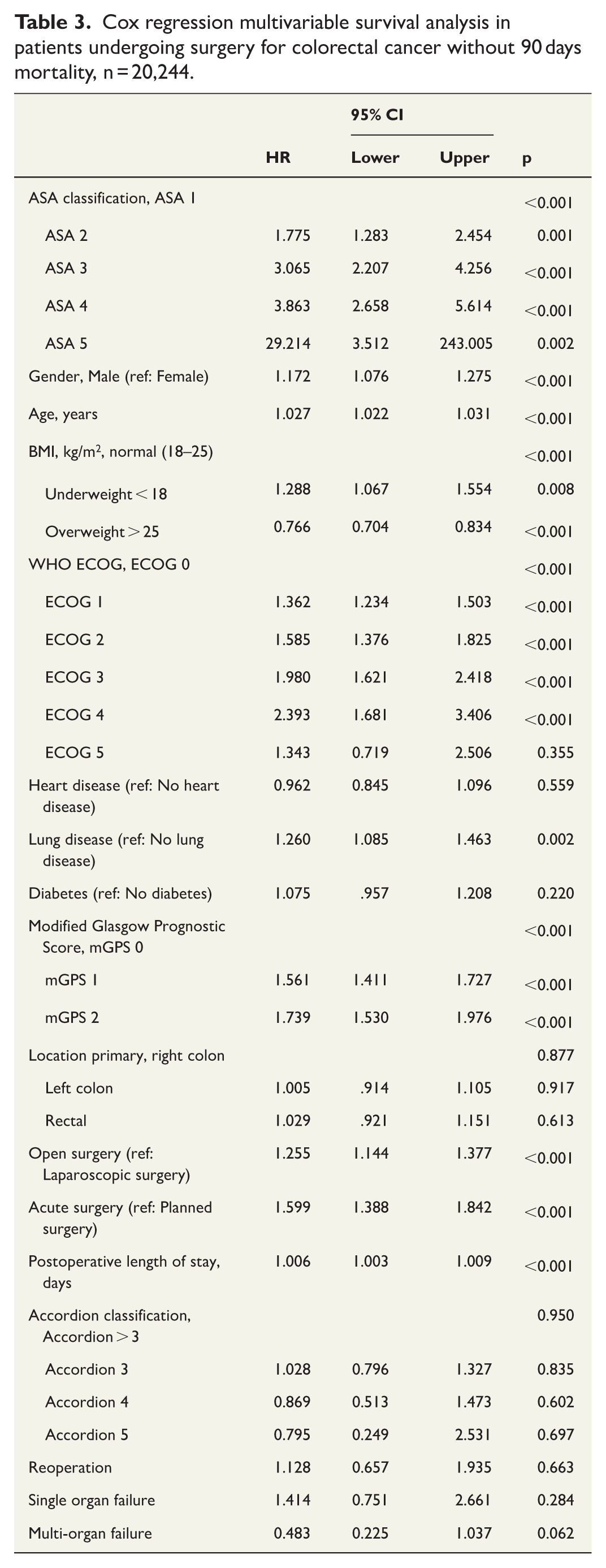
Because age differed substantially across ASA classes, survival analyses were repeated within 10-year age strata. Within each age group, ASA class remained significantly associated with overall survival (p < 0.004 for all age strata; Supplemental Fig. 1). Furthermore, in multivariable Cox regression model, ASA class remained independently associated with survival (p < 0.001, Table 3).
Cox regression multivariable survival analysis in patients undergoing surgery for colorectal cancer without 90 days mortality, n = 20,244.
ASA 2 and ASA 3 patients constituted the majority of the cohort and accounted for most survival events. Among these patients, the risk of death during the first, second, and third postoperative years was 2.9%, 4.4%, and 4.2%, respectively, for ASA 2, compared with 8.0%, 9.1%, and 7.6% for ASA three patients (p < 0.001). The mean age at surgery in the survival cohort was 70.8 years. For comparison, the 1-year mortality in the general Norwegian population aged 70–72 years was 1.22%, 1.45%, and 1.54%, respectively (Statistics Norway, 2023). 23
ASA classification and long-term survival after surgery for pancreatic or liver malignancies
During the study period, 6061 patients underwent pancreatic or liver resection. After exclusion of patients operated on for benign disease (n = 1269) and those who died within 90 days after surgery (n = 90), 4702 patients were included in survival analyses. The 3-year and 5-year overall survival rates were 63.7% and 49.0%, respectively.
ASA class distribution was ASA 1, 54 (1.1%) patients; ASA 2, 2333 (49.6%); ASA 3, 2258 (48.0%); and ASA 4, 57 (1.2%). There were no ASA 5 patients. ASA classification was significantly associated with long-term survival (Fig. 3A).
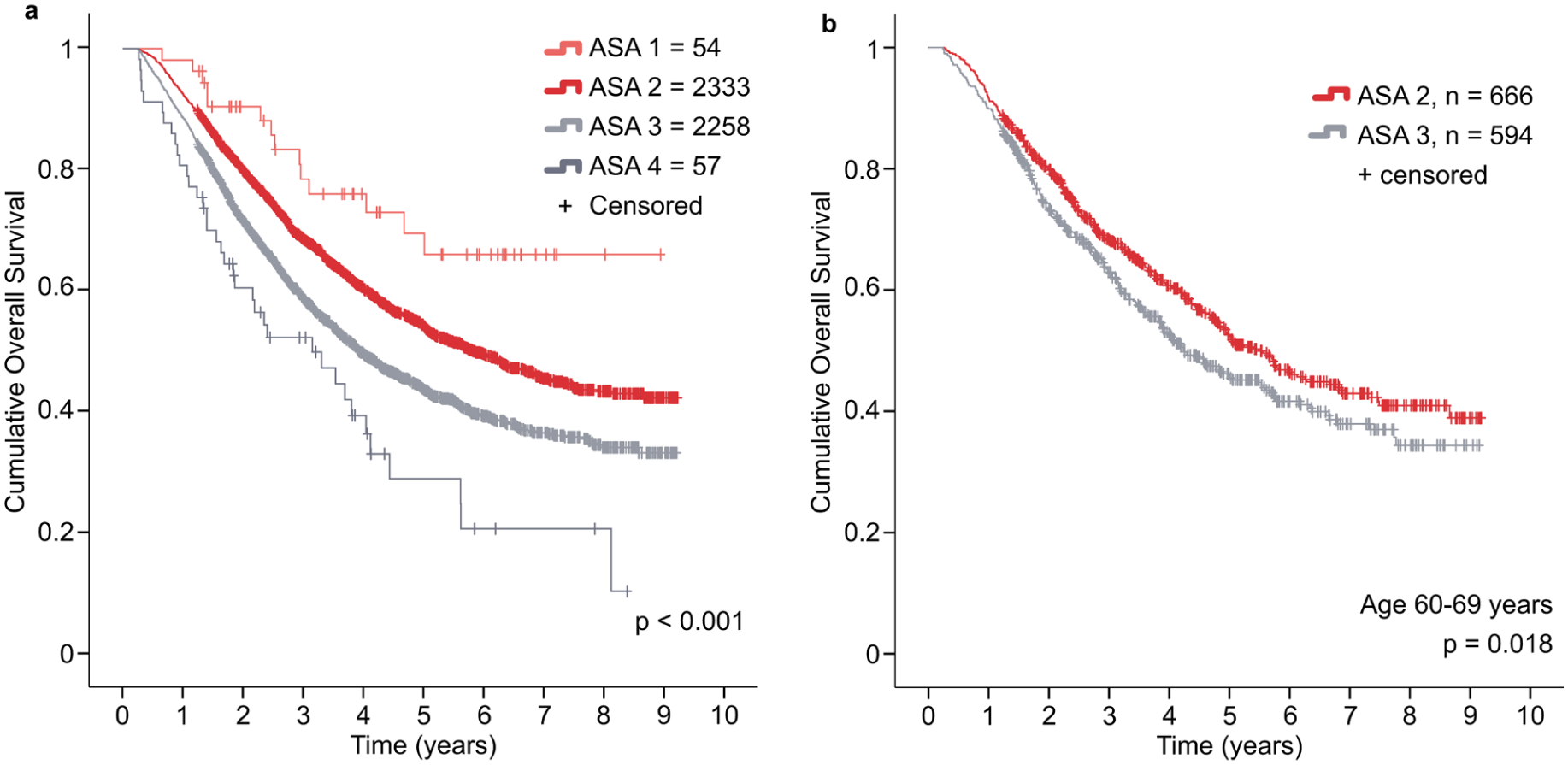
(A) Cumulative overall survival among patients undergoing surgery for pancreatic or liver malignancies (n = 4702), stratified by ASA class. Kaplan–Meier curves with log-rank tests are shown; censored observations are indicated by plus signs (+). (B) Overall survival in the same cohort restricted to patients aged 60–69 years.
Most patients were classified as ASA 2 or ASA 3. Mean age was 63.7 years in ASA 2 and 69.3 years in ASA 3. To address age imbalance, a subgroup of patients aged 60–69 years (n = 1283) was analyzed. Within this age-restricted cohort, ASA 2 patients demonstrated superior survival compared with ASA 3 (Fig. 3B, p = 0.048), with divergence becoming more apparent beyond two postoperative years.
In multivariable Cox regression analysis including ASA class (2 vs 3), age and sex, ASA 3 (vs ASA 2; hazard ratio (HR): 1.254, 95% confidence interval (CI): 1.149–1.369, p < 0.001) and increasing age (HR: 1.017, 95% CI: 1.013–1.022, p < 0.001) remained independently associated with reduced survival. Sex was not associated with outcome (HR: 0.986, 95% CI: 0.904–1.075, p = 0.742).
ASA classification and perioperative risk in after CRC surgery
Postoperative complications increased with higher ASA class. According to the Accordion grading system, 18,196 patients experienced complications graded <3, while grades 3, 4, 5, and 6 were observed in 475, 1662, 246, and 204 patients, respectively.
Among ASA 2 patients, Accordion grades 3–6 occurred in 2.1%, 7.6%, 0.7%, and 0.2%, respectively, compared with 2.6%, 8.7%, 1.7%, and 1.7%, among ASA 3 patients. The corresponding absolute percentage-point differences between ASA 2 and ASA 3 were +0.5, +1.1, +1.0, and +1.5 pp, respectively (p < 0.001).
Overall, 1655 patients underwent reoperation following CRC surgery. Reoperation rates increased with ASA class: 6.3% (ASA 1), 7.3% (ASA 2), 8.9% (ASA 3), 9.3% (ASA 4), and 25.0% (ASA 5) (p < 0.001). There was a small (+1.6 pp) but significant discrimination between ASA 2 and ASA 3, p < 0.001, but not between ASA 1 and ASA 2 (p = 0.228) nor between ASA 3 and ASA 4 (p = 0.772).
Postoperative interventions not requiring general anesthesia occurred in 2.4% (ASA 1), 3.8% (ASA 2), 5.1% (ASA 3), 7.4% (ASA 4), and 12.5% (ASA 5) of patients (p < 0.001). Given that most patients were classified ASA 2 or ASA 3, and that the absolute difference was modest (+1.6 pp), ASA class demonstrated limited clinical utility for predicting minor postoperative interventions.
Length of stay increased with ASA class. Median postoperative length of stay was 4, 5, 6, 7 and 7 days for ASA 1 through ASA 5, respectively (p < 0.001).
Discussion
In this large national cohort study, we show an association between preoperatively assigned ASA classification and long-term overall survival after major abdominal cancer surgery. This association persisted after exclusion of 90-day postoperative mortality, across age-matched subgroups, and in multivariable survival analyses, indicating that the observed survival differences cannot be explained solely by perioperative deaths or pre-existing comorbidities. Importantly, this finding was present not only in CRC patients, but also in patients undergoing surgery for pancreatic and liver malignancies—settings in which cancer-specific mortality is expected to dominate long-term outcomes.
The ASA classification system was originally developed to assess perioperative risk associated with anesthesia but has been criticized for its lack of scientific precision for this purpose. 6
ASA is often used in conjunction with other factors, such as the type of surgery or frailty, to jointly estimate perioperative risk. In this study, ASA class was statistically significantly associated with postoperative adverse events. However, the absolute differences between adjacent subgroups were modest. In contrast to its limited discriminatory ability for perioperative morbidity, the association between ASA class and long-term survival was robust and consistent following major abdominal cancer surgery, despite previous studies showing inconsistent ASA class assignment among anesthesiologists.6,24 This finding persisted across different malignancies, adding weight to its relevance.
Cancer is frequently associated with fatigue and reduced overall physical condition and may also exacerbate the symptom burden of pre-existing chronic diseases such as heart disease, lung disease, liver disease, or diabetes. The association between ASA class and survival could, in theory, reflect more advanced cancer at the time of surgery among patients with higher ASA class. However, most patients were classified as ASA 2 or ASA 3, categories in which it is less likely that cancer severity alone determines the ASA assignment. Furthermore, an interesting observation was the difference in primary tumor location, with ASA 3 patients more often presenting with right-sided colon cancer, which is known to be associated with reduced survival. 25
Cancer is, in practice, a chronic and ultimately life-threatening disease. However, since all patients in this study had cancer, this alone does not explain the overall survival (OS) differences between ASA classes. One speculative hypothesis is that anesthesiologists, perhaps unintentionally, may be using the ASA classification to reflect underlying cancer burden rather than comorbidity alone—and that they may be doing so with a degree of accuracy comparable to established oncologic stratification tools.
In patients undergoing major surgery such as a pancreatoduodenectomy, the presence of comorbidity threatening survival within the next year would typically preclude surgery. Moreover, modern preoperative imaging makes it unlikely that patients with extensive undiagnosed lung metastases or undetected carcinomatosis proceed to resection. Thus, an association between underreported cancer stage at the time of surgery and ASA class is unlikely to fully explain this observation.
A study from Memorial Sloan Kettering Cancer Center found no association between ASA classification and 6-month postoperative mortality in oncogeriatric patients. 15 However, that study evaluated a smaller cohort of 980 patients, and more than 85% of the patients were classified as ASA 3, limiting discrimination between groups. In contrast, our study followed a substantially larger cohort for a median of nearly 4 years, with a more balanced distribution between ASA 2 and ASA 3 patients, allowing clearer separation of survival curves.
Similarly, a single-center Italian study found no association between ASA classification and overall survival in 473 patients undergoing surgery for gastric cancer. 16 In contrast, this study demonstrates a consistent association between ASA class and long-term survival in both CRC patients and patients undergoing resection for pancreatic or liver malignancies. These divergent findings may reflect diagnose-specific differences or limited statistical power in smaller cohorts. Supporting the relevance of ASA classification in CRC, another study reported an association between ASA class and postoperative survival in 385 rectal cancer patients. 17
The ASA class is assigned by the attending anesthesiologist immediately prior to surgery and is documented in the electronic patient record. As such, it represents a rapid bedside clinical assessment without reliance on objective or standardized measurements. 6 Despite concerns regarding subjectivity and inter-rater variability, most patients were classified as ASA 2 or ASA 3, and notably, survival curves for these two groups diverged early and remained separated throughout follow-up. This finding is particularly striking given the expected overlap and potential misclassification between adjacent ASA categories.
Age increased progressively with higher ASA class among patients undergoing CRC resection, confirming age as an important determinant of long-term survival. However, when survival analyses were repeated within 10-year age strata, ASA class remained significantly associated with survival, with ASA 3 patients consistently demonstrating worse outcomes than ASA 2 patients. In multivariable analysis, both age and ASA class were independently associated with overall survival, with ASA class emerging as the stronger predictor.
Although the NORGAST registry provides a large, high-quality dataset, several limitations must be acknowledged. Most importantly, cancer-specific survival data were unavailable. In CRC patients, where a substantial proportion of patients achieve long-term survival, pre-existing comorbidities are likely to play an increasingly important role in determining prognosis as time from surgery increases. Conversely, in patients with pancreatic or liver malignancies, where recurrence rates are high and cancer-specific mortality predominates, the relative impact of comorbid disease on long-term survival may be less pronounced, as most patients ultimately die from their cancer rather than from competing causes.
Another limitation is the lack of detailed pathological and oncological data. In CRC, it would have been informative to evaluate ASA classification alongside established prognostic factors such as tumor stage, margin status, disease burden, and systemic therapy. Pre-existing comorbidities may limit eligibility for adjuvant therapy and thereby indirectly influence long-term survival. An association between higher ASA class and more advanced or aggressive tumor biology has previously been proposed, 26 although this relationship has not been consistently demonstrated across cancer types and remains debated. 27 The absence of such variables precluded their inclusion in multivariable analyses together with ASA classification.
This limitation is likely even more relevant in the hepatopancreatic cohort, which comprises a heterogeneous mix of histological subtypes. While most pancreatic resections were performed for pancreatic ductal adenocarcinoma, distal cholangiocarcinoma, duodenal cancer, or ampullary cancer, liver resections were primarily undertaken for colorectal liver metastases, hepatocellular carcinoma, or cholangiocarcinoma. Comparison with national survival data for pancreatic cancer in Norway—where reported 3- and 5-year after resection are 36.4% and 21.5%, respectively—suggests that the NORGAST cohort also includes patients with more indolent malignancies, such as neuroendocrine tumors, as well as patients operated on for lesions later confirmed to be premalignant. 28
Based on this large national dataset, it appears that the ASA classification has received some undeserved criticism with respect to its scientific value in perioperative risk assessment. Although ASA class was significantly associated with postoperative adverse events, very large sample sizes were required to detect relatively small absolute differences between adjacent categories, limiting its clinical usefulness in this context. Thus, the key issue may not be scientific precision but clinical relevance, and the role of ASA classification in perioperative risk stratification warrants discussion in patients undergoing surgery for colorectal, pancreatic, or liver malignancies. 29
In contrast, the ASA classification demonstrated both scientific precision and clinical relevance in predicting long-term survival after surgery after major abdominal cancer surgery. Survival discrimination between ASA classes was distinct, consistent across age groups, preserved after exclusion of postoperative mortality, and evident even in settings where non-cancer-related mortality is minimal. These findings suggest that ASA classification captures prognostically important patient characteristics beyond documented comorbidity alone and that its association with long-term survival is likely multifactorial. Future studies incorporating cause-specific mortality data will be essential to further clarify the mechanisms underlying this association.
Supplemental Material
sj-eps-1-sjs-10.1177_14574969261463220 – Supplemental material for Revisiting the ASA physical status classification: Differential associations with long-term survival in abdominal cancer surgery
Supplemental material, sj-eps-1-sjs-10.1177_14574969261463220 for Revisiting the ASA physical status classification: Differential associations with long-term survival in abdominal cancer surgery by Lars A. B. Grønvold, Linn S. Nymo, Dyre Kleive, Kjerstin Havnes, Stig Norderval, Kristoffer Lassen and Kristoffer W. Brudvik in Scandinavian Journal of Surgery
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Clinical trial registration
N/A
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.