
Abstract
Introduction
The weekend effect is a reported phenomenon whereby patients admitted at a weekend are found to have worse outcomes than those admitted during the week. The causes are not well understood, but may have implications for the planning of medical workforces throughout the developed world. Although the magnitude of the weekend effect is reduced whenknown confounding factors are adjusted for, there are likely to be substantial residual unmeasured confounding factors. It remains unclear how much effect exists in comparable patients. The aim of this study was to determine whether the presence of a weekend effect could be detected for the patients admitted with hip fracture to our unit and to quantify this effect if detected.
Methods
All hip fracture patients admitted to our unit over a five-year period were examined. All patients had their details entered onto the National Hip Fracture Database which was investigated to compare inpatient, 30-day, 120-day and 365-day mortality with specific reference to day of admission and operative treatment.
Results
Two thousand one hundred and thirty fractured neck of femur patients were admitted from 2011 to 2016. We found no difference in mortality in being admitted or treated at the weekend or weekday; however, patients operated upon on a Tuesday had a statistically significant higher risk of death (OR 2.813, 95% CI 1.336–5.992, p = 0.006). The reasons for this are unclear.
Conclusions
In our unit there is no evidence of a weekend effect for hip fractures.
Introduction
The ‘weekend effect’ is a phenomenon whereby patients admitted at a weekend are found to have worse outcomes than those admitted during the week. 1 The causes are not well understood, but may have implications for the planning of medical workforces throughout the developed world. The findings of many of these studies are likely to be confounded by the fact that a greater proportion of the patients admitted at weekends have higher predicted mortality than those admitted during the week. Although the magnitude of the weekend effect is reduced when known confounding factors are adjusted for, there are likely to be substantial residual unmeasured confounding factors. It remains unclear how much effect exists in patients who are comparable in terms of severity of admitting complaint and medical co-morbidities. The weekend effect has been described for all-cause medical admissions, but it has also been noted when specific diagnoses have been investigated.
Hip fracture is an ideal condition to assess for the presence of a weekend effect for a variety of reasons. First, patients are normally admitted shortly after sustaining their fracture and unlike other conditions previously studied there is unlikely to be a period of illness preceding admission. Patients with hip fractures have a relatively high mortality so a weekend effect may be easier to detect than in other patient groups. Treatment of hip fractures in the UK is now standardised under the Best Practice Tariff (BPT), 2 reducing management discrepancy between centres. Additionally data collected about patients presenting with hip fracture are particularly robust due to the practice of submitting to the National Hip Fracture Database (NHFD). Any such study in the UK may be of particular merit, due to the presence of the UK National Health Service, which reduces discrepancies in access to healthcare among patients.
The aim of this study was to determine whether the presence of a weekend effect could be detected for the patients admitted with hip fracture to our unit and to quantify this effect if detected.
Methods
Our unit is based in North London, UK with a high throughput, admitting around 450 patients with hip fractures per year, all of whom are admitted under joint care between an orthopaedic surgeon and a dedicated orthogeriatrician. There is a consultant-led trauma theatre seven days a week, allowing most patients to be operated on either the day of admission or the following day. All patients are treated in line with the targets set out by the BPT and have their details entered into the NHFD.
Data collection
Between 1 April 2011 and 1 January 2016, 2130 patients were admitted with a fractured neck of femur. Entries to the NHFD were retrospectively reviewed to collect data on date of admission, age of patient, gender, ASA, pre-morbid outdoor mobility, preoperative Abbreviated Mental Test Score (AMTS), fracture type, presence of pathological fracture, date of surgery, operation performed, death date (where applicable), discharge date, anaesthetic type and time from admission to geriatrician review. The weekend was defined as starting at 8:00 am on Saturday and ending at 8:00 am on Monday.
Statistics
To compare baseline characteristics between groups, the chi-square test was used to compare categorical data, independent samples t-test was used to compare continuous normal data and the Mann–Whitney U-test was used to compare non-parametric data.
To compare admission rates between different days, Poisson regression was used. To assess and adjust for the impact of patient factors on mortality and length of stay, logistic and linear regression methods were used respectively.
Missing data
Preoperative AMTS had approximately 17% missing data, but was found to have a significant impact on patient outcomes so multiple imputation was used to account for the missing values. Overall 25 patients (2%) did not undergo surgery so did not have an ASA score entered into the NHFD; these patients had high mortality as they were patients deemed too unwell to operate on and so it was decided to impute missing values of ASA, so as not to exclude these patients from analysis.
Results
Demographics
Demographics of weekday versus weekend admissions. Unless otherwise stated, the number in brackets represents a standardised rate of attendance based on the number of days of the week a group represents.
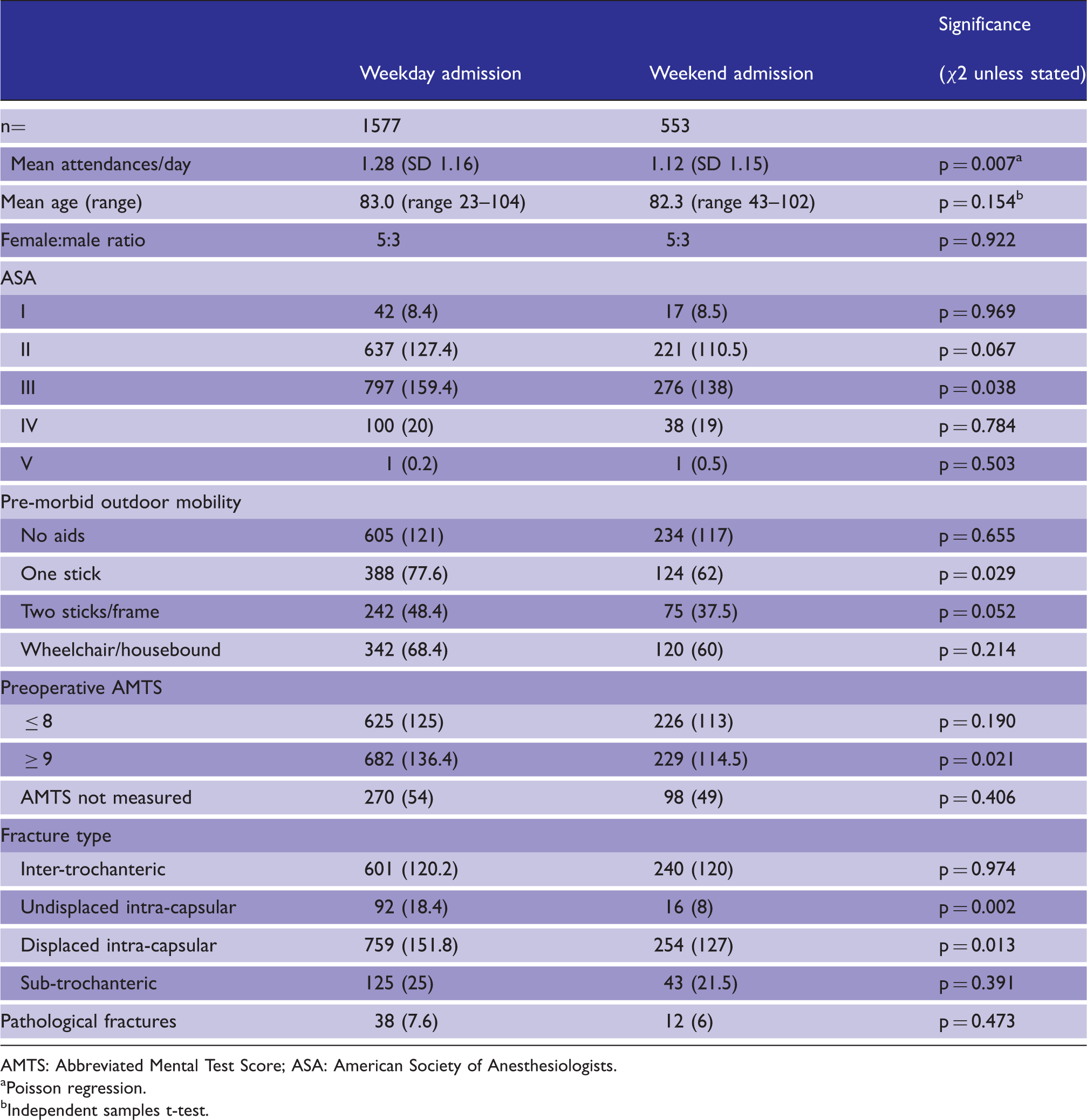
AMTS: Abbreviated Mental Test Score; ASA: American Society of Anesthesiologists.
Poisson regression.
Independent samples t-test.
Rates of attendance
There were significantly more admissions per day on weekdays than on weekend days, with a mean rate of admission of 1.12 per day on weekends (SD 1.15) and 1.28 on week days (SD 1.16, p = 0.007).
Treatment received
Care received: Weekday versus weekend admissions.
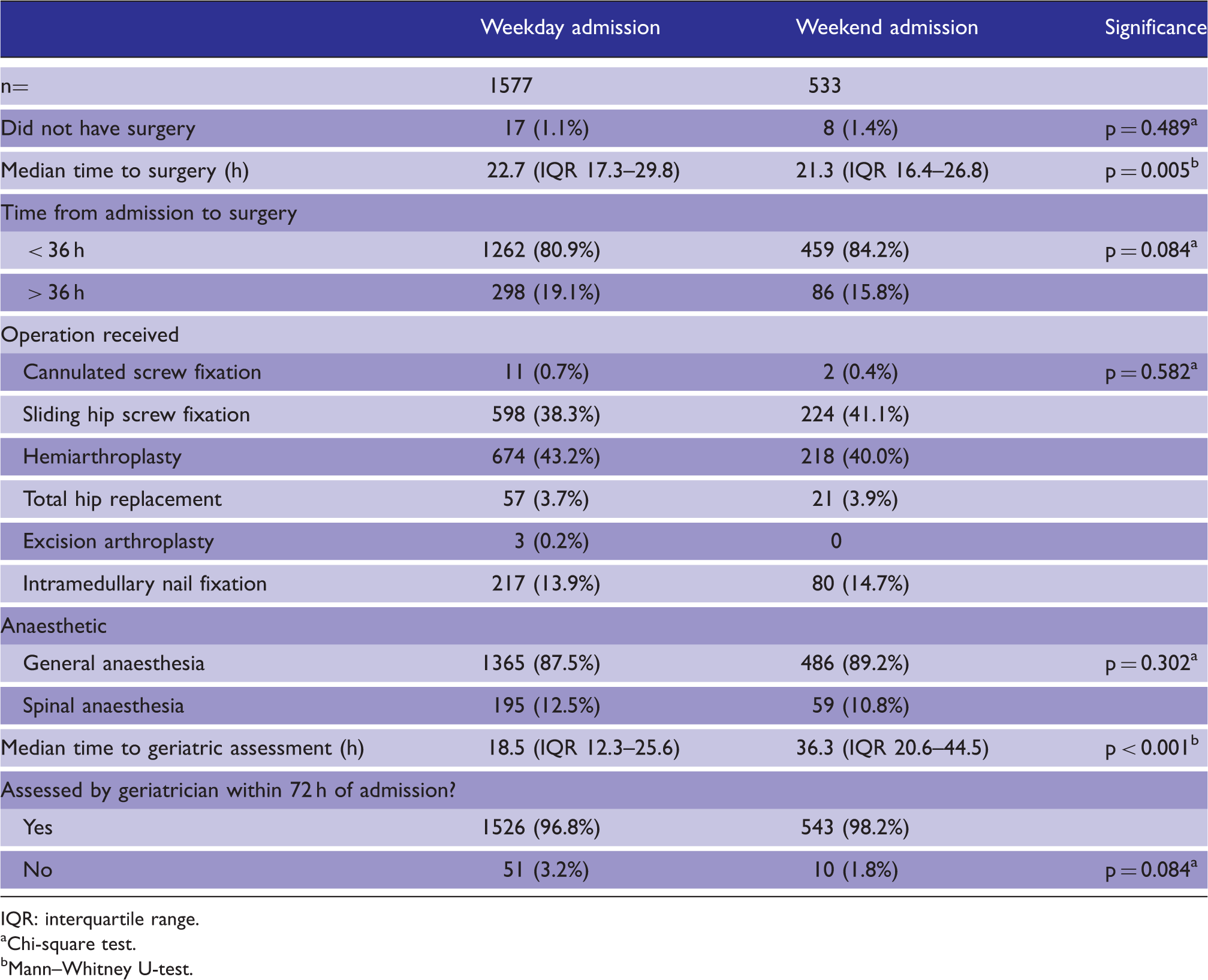
IQR: interquartile range.
Chi-square test.
Mann–Whitney U-test.
Patient outcomes
Outcomes of weekday versus weekend admissions.
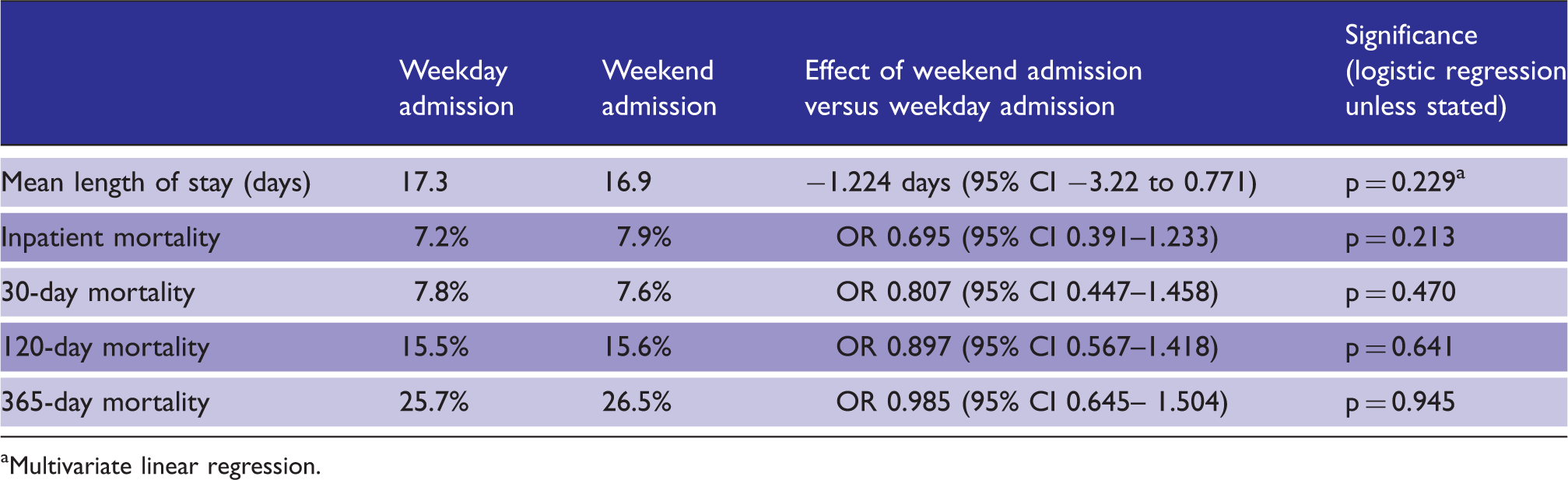
Multivariate linear regression.
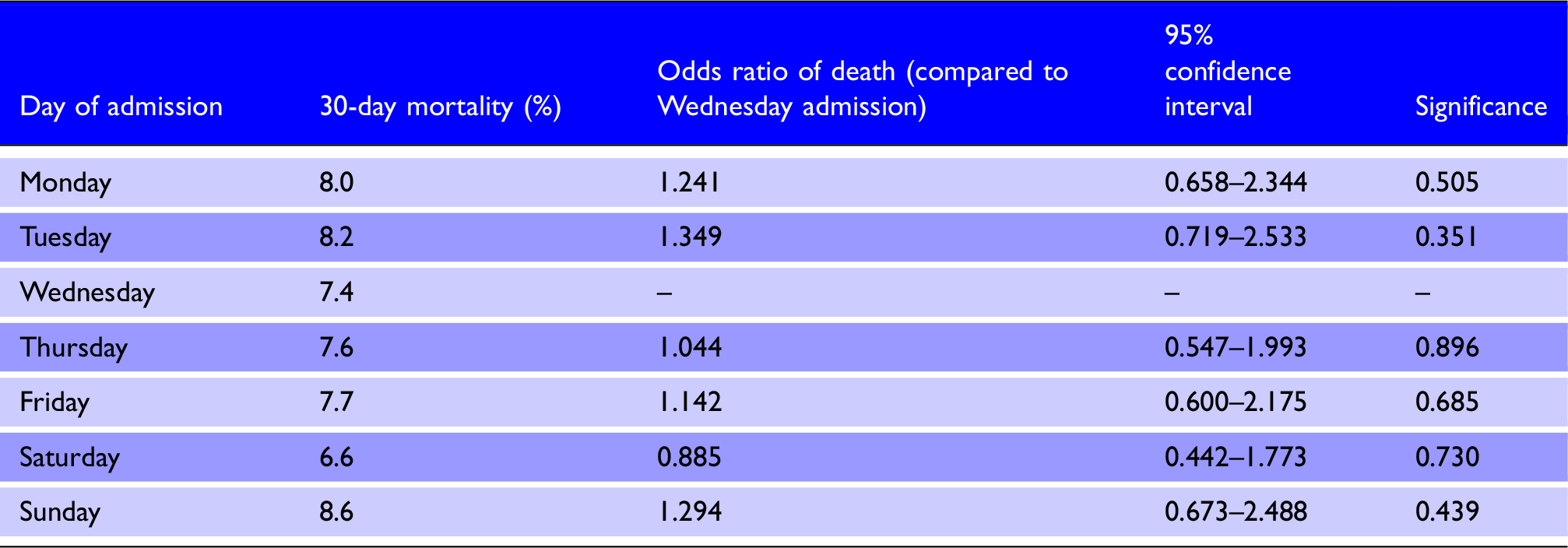
Effect of day of admission on 30-day mortality by logistic regression analysis.
Day of surgery
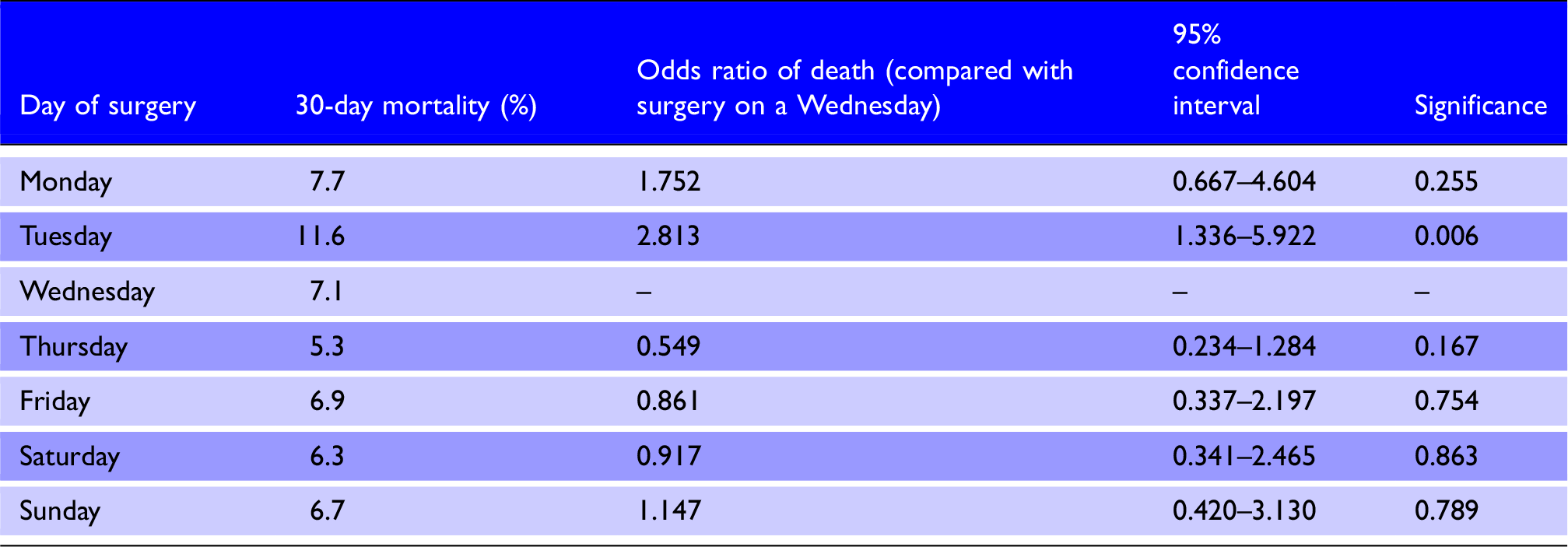
Effect of day of surgery on 30-day mortality by logistic regression analysis.
Day of death
Of the patients who died during their inpatient episode, there was no day of the week that they were statistically more or less likely to die on.
Discussion
These results show that weekend admission does not affect mortality for patients admitted with hip fracture and regardless of the day of admission, there was no significant difference in 30-day mortality between patients. In the crude comparison, Sunday was the day with the highest overall mortality rate but in the adjusted comparison the highest mortality rate was observed in patients admitted on a Tuesday; neither reached statistical significance.
Patients operated upon on a Tuesday had the highest mortality overall, which was the only comparison found to reach statistical significance, but it is difficult to determine the cause of this finding. It may be speculated that these patients are those admitted over the weekend who require preoperative investigations which may only be available during the week, implying a higher high anaesthetic risk. More likely is that, rather than being a true finding, the significance is a chance finding as a result of the multiple testing effect.
The characteristics of patients admitted at a weekend were similar to those admitted during the week with no significant differences between ages, gender, ASA, preoperative AMTS or the proportion of patients presenting with pathological fractures. Where they differed is that patients admitted on a weekday were significantly more likely to present with intracapsular fractures, baseline AMTS ≥ 9 or baseline mobility requiring the use of one stick when mobilising outdoors.
Surprisingly there were a significantly larger mean number of attendances per day on weekdays compared with weekends. Unfortunately our dataset only includes the date of admission and not the date of injury, as this information would help clarify the nature of the excess cohort of patients presenting on weekdays. These patients are either a group more at risk of sustaining a fracture on a weekday, or if fractures happen uniformly throughout the week, are patients who delay presentation to hospital until a weekday. The results show that there are significantly more attendances early in the working week compared with Sunday (the day with the lowest rate of attendance), but do not give weight to either hypothesis. Whichever is correct (or even if there is a combination of the two), this represents an as-yet uncharacterised social factor affecting the presenting patterns of patients.
The weekend effect has been documented to affect both all-cause hospital admissions1,3–5 and for individually studied conditions.6–11 There is a large international body of evidence demonstrating an absence of a weekend effect on mortality and length of stay, for patients admitted to hospital with hip fracture,12–21 but more recently, studies from hospitals in the UK have demonstrated varying results, with one showing a significantly higher mortality in patients admitted at a weekend, 17 and others demonstrating limited or no effect.18–20 In the first of these, 17 and in contrast to the other studies it is noted that patients presenting at a weekend had a significantly longer time from admission to surgery. Operative delay is well known to increase mortality in hip fracture patients 21 and may go some way to explaining their findings of 40% higher odds of death for patients admitted at a weekend and the absence of such a finding in this study and others. This delay to surgery is not present in our unit; patients admitted at a weekend actually had significantly less time from admission to surgery as we provide consultant-led trauma service at the weekends.
Patients presenting at a weekend have been previously found to differ in their demographics to those presenting during the week, with higher predicted mortality risk at admission. 3 Despite controlling for measured differences, greater rates of death within 30 days were still seen for those presenting at a weekend, in previous studies.
Early results from the High Intensity Specialist Acute Care Study 22 seem to suggest that patient’s presenting patterns are responsible for the weekend effect. Although the proportion of patients dying after weekend admission is higher, the absolute numbers of patients dying within 30 days of admission is similar for each day. It appears that sick patients may attend uniformly throughout the week, whereas less sick patients preferentially attend during the working week. It seems likely that the reported weekend effect was due to a combination of patient’s presenting patterns and cohorts of susceptible patients; where susceptible patients can be identified, deficiencies in hospital services may be rectified. 23
Despite the relatively high number of patients in this study, we are aware of its limitations, and the fact that the study is local to our unit. A relative risk increase of 15% over the baseline weekday 30-day mortality of 7.8% represents an absolute risk increase of only 1.17%. This translates into a number needed to harm of 85 weekend admissions to cause a single death within 30 days, which means that over the course of our four-year data series of 2130 patients, there would be only six excess deaths among the 553 patients admitted during the weekend.
A randomised controlled trial to detect a relative risk increase of 15% among two identical groups of patients with an enrolment ratio of 2.85 (the ratio of weekday attendances to weekend attendances) would require 22,619 trial subjects (16,744 weekday admission and 5875 weekend admissions) to detect an absolute risk increase of 1.17% (with 95% significance and 80% power). In order to generalise our findings such an RCT will play a pivotal role.
A further limitation of this study is that public holidays falling on a weekday were still counted as weekdays, despite having the same staffing levels as a weekend day. Due to the relative scarcity of public holidays throughout the calendar, this effect was likely to be negligible. A total of 2% of the patients included in the study did not have an ASA documented on the NHFD, as they were unfit for surgery, but were still included the dataset, due to their high mortality risk.
Conclusion
There was no association between weekend admission and treatment with worse outcomes for patients admitted to our unit with hip fracture. Patients admitted at a weekend had a shorter time to surgery and those who received their operation on a Tuesday had significantly worse 30-day mortality, the reasons for which are unclear. We found evidence of social factors affecting presenting patterns of patients with hip fracture, as there appeared to be a cohort of excess weekday attendances, which may represent a group of patients with unmet social needs.
Footnotes
Acknowledgements
Many thanks to Stella Legge, the trauma coordinator for our unit, who was invaluable during the collection of data.
Ethical approval
As the study was an observational study, examining the effect of weekend admissions on service provision, with no patient identifiable data, no ethics approval was needed.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Not applicable.
Trial registration
Not applicable.
Guarantor
AA.
Contributorship
The study was conceived by AA, MB and BF, the data were collected by MB, the data were analysed by MB and AL. The paper was written by MB and AA, AA was in charge of submission and paper revisions, one of the revisions was done by AL.
Provenance
Not commissioned, externally peer reviewed.