
Abstract
Objective:
As the representative body for orthodontic specialists, the British Orthodontic Society (BOS) provides advice and guidance to professionals and patients on a variety of topics. The BOS receive frequent queries from professionals and patients and, where appropriate, provide advice and guidance. By reflecting on the types of queries received, it is hoped that general guidance can be developed and ‘frequently asked questions’ information established to improve knowledge in these particular areas.
Design:
Retrospective assessment of queries raised to the BOS.
Setting:
BOS headquarters, London.
Methods:
All queries raised to the BOS by professionals and patients from January 2017 to October 2018 were collated and divided into those raised by dental professionals or by patients. Within each group, all queries were further subcategorised into different topic areas. For each of the main topics, guidance will be developed to improve clinician and patient knowledge in these areas.
Results:
In the time period assessed, 422 queries were received to the BOS, 51.8% (n = 229) were from patients and 48.2% (n = 213) from professionals. Commissioning was the most common topic queried by professionals (34.3%), which included NHS contracts and tendering. Queries regarding associate matters (9.4%), specific clinical queries (9.4%) and BOS issues (8.9%) were also common topics raised by professionals. The most common topic queried by patients was the eligibility for NHS treatment (29.3%), followed by specific clinical queries (22.3%) and seeking recommendations for clinicians (10.5%).
Conclusions:
Overall, a large number of queries were received by the BOS. While some queries required specific information from the BOS, the majority of queries could be addressed through already published information and guidance. This project identifies the more common queries and provides clear guidance on where to find the appropriate advice.
Keywords
Introduction
The British Orthodontic Society (BOS) is a registered charity (charity number 1073464) and is the national representative body for orthodontists and the practice of orthodontics in the UK. The mission statement of the BOS is to improve the quality of orthodontic care for patients by promoting the study and practice of orthodontics, maintaining and improving professional standards, and by encouraging research and education in orthodontics.
As part of its remit, the BOS answers queries from both patients and clinicians. The BOS is often asked to assist in resolving queries or complaints that may arise in relation to the specialty of orthodontics or to give advice on current practice or philosophy.
A query is regarded as a request for information, whereas a complaint is very different and is an expression of dissatisfaction with a service provided. Complaints can be raised in a number of ways and, whether justified or not, require a response. There is considerable guidance on best practice when handling complaints, including guidance available from NHS England and the BOS itself (British Orthodontic Society, 2016; NHS England, 2017). Complaints should be handled according to the principles outlined in these policies as well as in accordance to local hospital or practice policy.
The aim of this project was to collate recent queries raised to the BOS by both professionals and patients and to provide topic areas where queries were raised to generate ‘frequently asked questions’ for the benefit of patients and professionals. This is the first study of this nature for the BOS and there are currently no publications of similar topics for other societies.
Method
All queries raised to the BOS by professionals and patients from January 2017 to October 2018, inclusive, were collated and categorised according to if they were raised by a dental professional or a patient. All the queries were then assessed in detail by two assessors and further subcategorised into different topic areas depending on the nature of the query; a third assessor was consulted to mediate and achieve a consensus in cases of disagreement. The categories and subcategories used to collate the queries were not predetermined and were established according to the nature of the queries which were assessed.
Results
In total, 422 queries were received by the BOS between January 2017 and October 2018, inclusive. Of these, 51.8% (n = 229) were from patients and 48.2% (n = 213) were from professionals. Figure 1 shows the main categories of queries raised by professionals and Table 1 shows in more detail the number of professional queries raised in each category and the subcategories of these queries.
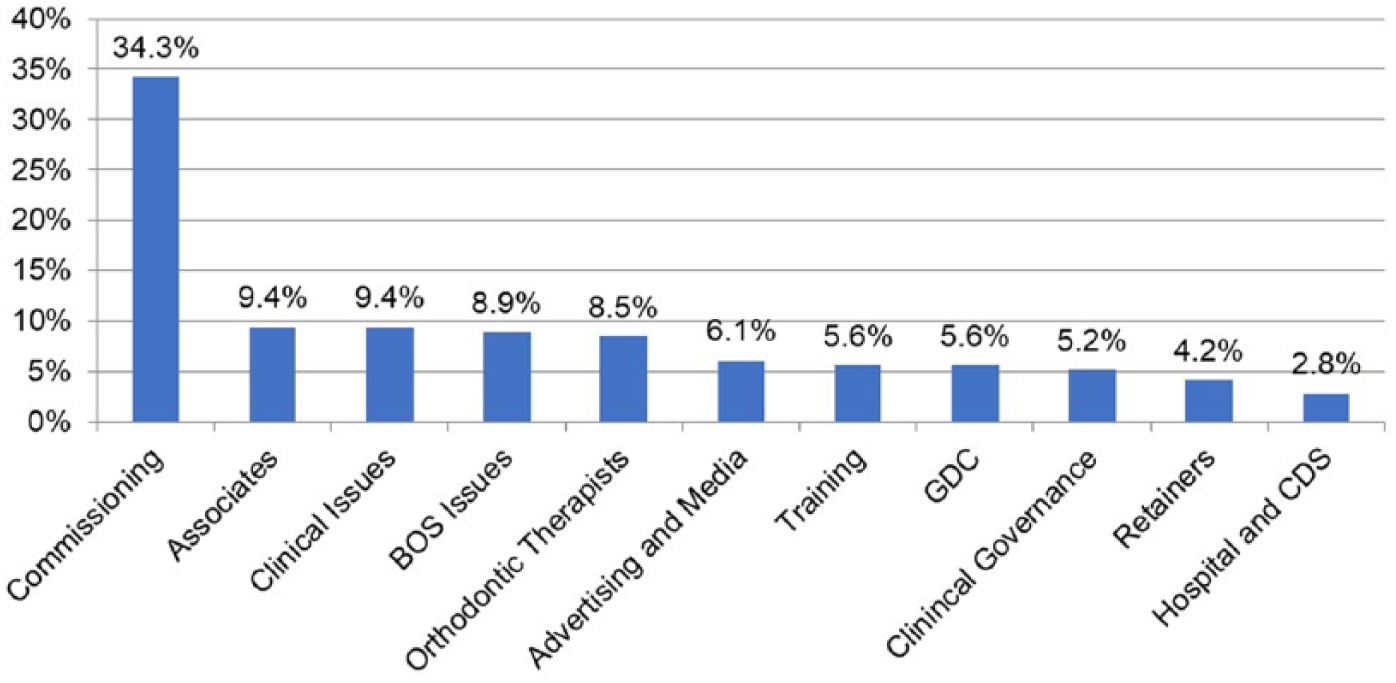
The main categories of professional queries.
Categories and subcategories of professional queries.
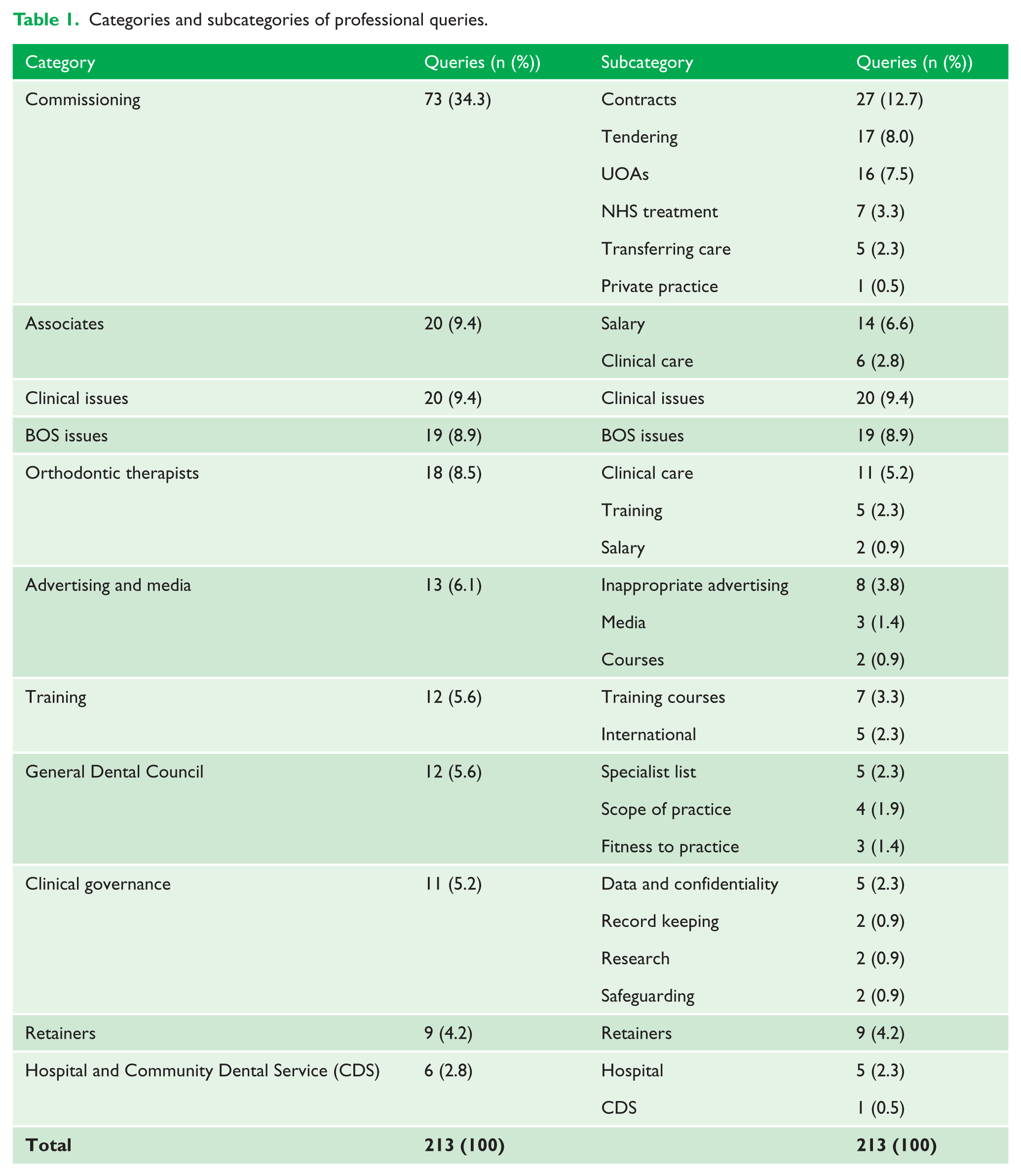
Figure 1 and Table 1 show that commissioning was the most common topic area queried by professionals (34.3%). This encompassed a variety of topics including contracts, tendering and units of orthodontic activity (UOAs). Queries regarding associates (9.4%), specific clinical queries (9.4%) and specific BOS issues (8.9%) were topics which were also queried relatively frequently
Figure 2 shows the main categories of queries raised by patients and Table 2 shows in more detail the number of patient queries raised in each category and the subcategories of these queries.
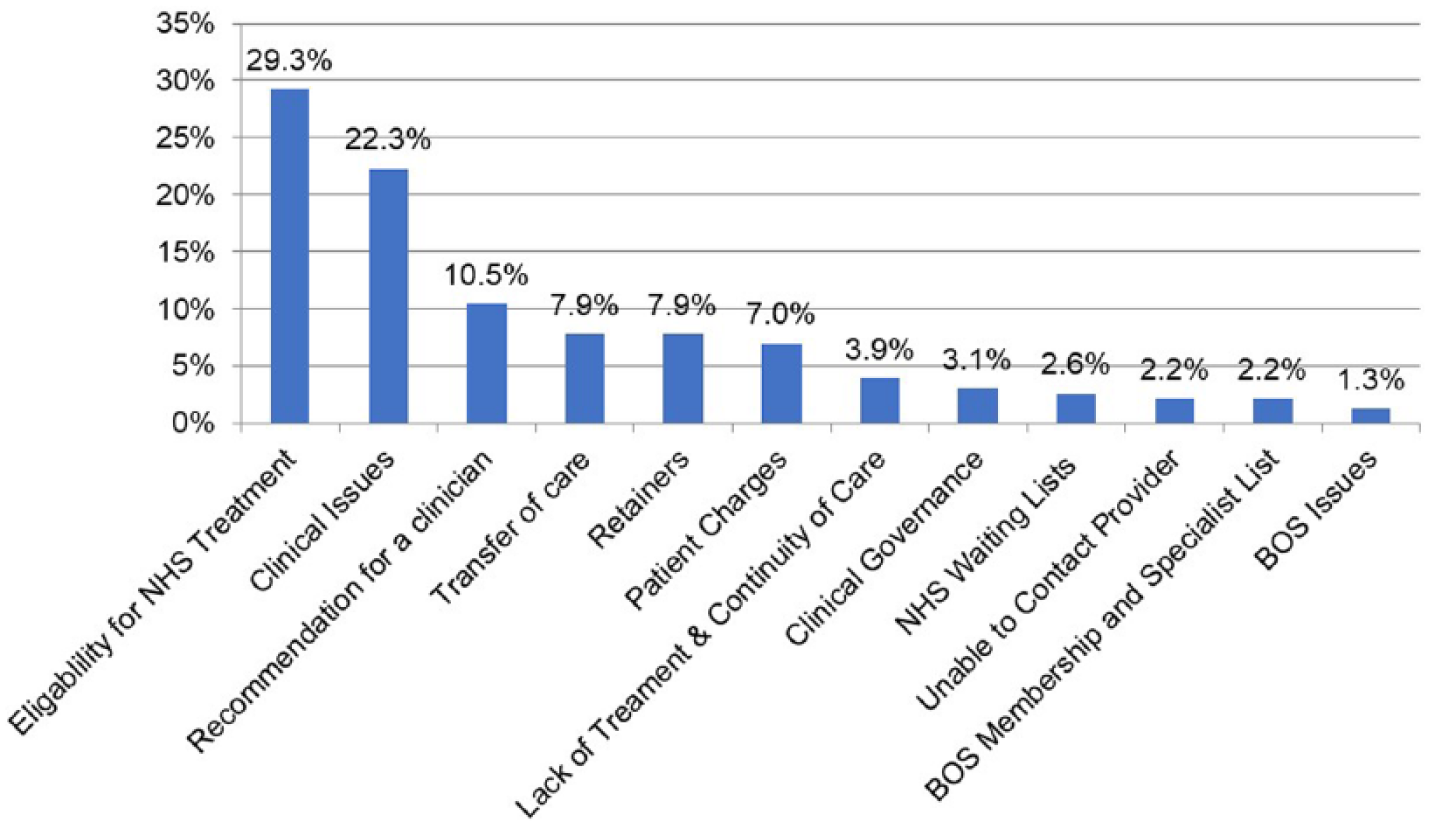
The main categories of patient queries.
Categories and subcategories of patient queries.
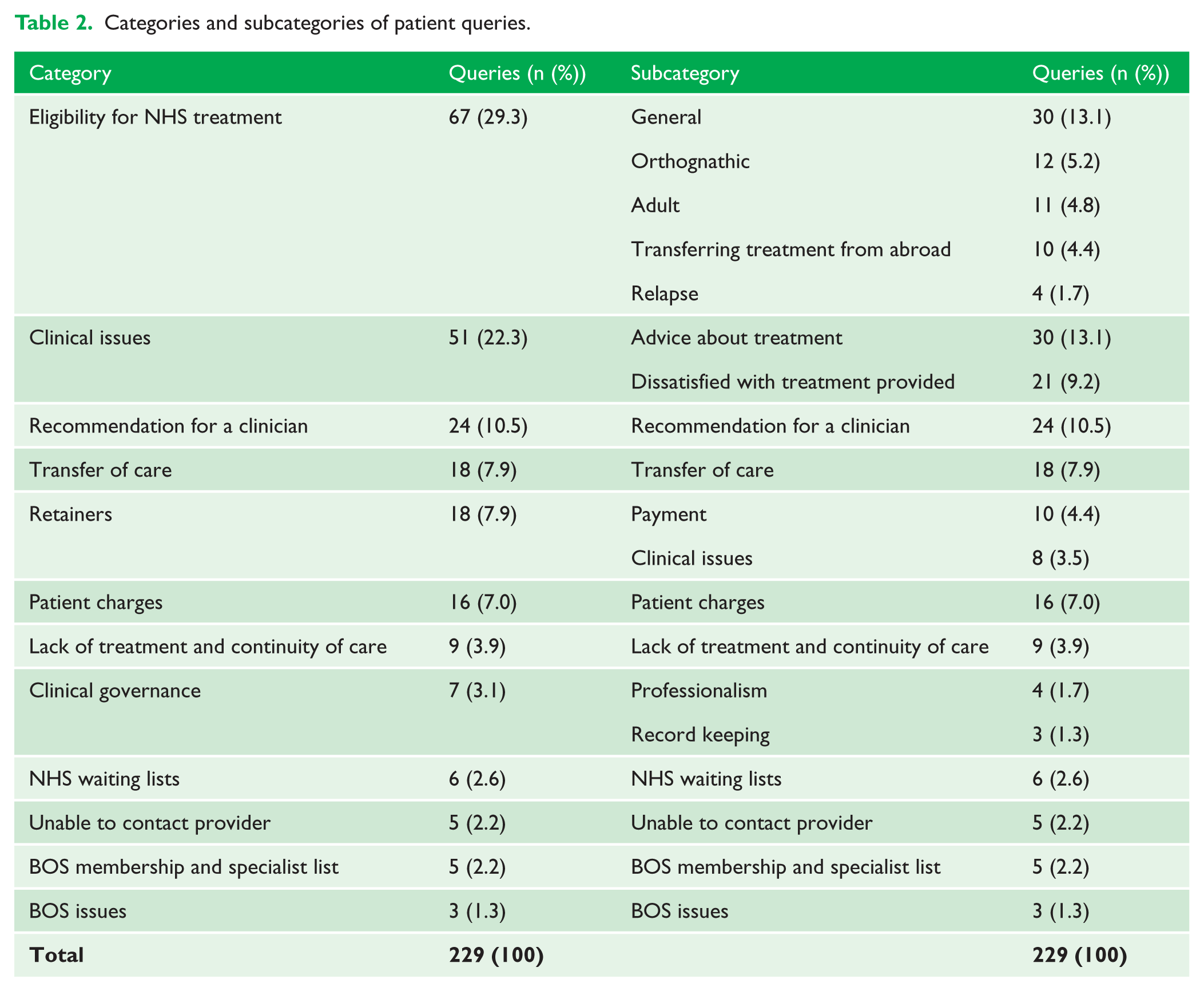
Figure 2 and Table 2 show that eligibility for NHS treatment (29.3%) and specific clinical issues (22.3%) were the most common topics where queries were raised from the patients. Within these topics, a high number of the queries focused on seeking advice about treatment (13.1%) or expressing dissatisfaction with treatment that had been provided (9.2%). There were also a number of queries regarding seeking recommendations for clinicians (10.5%), transferring care (7.9%) and questions about retainers (7.9%).
Discussion
Professional queries
One-third of the professional queries received were regarding commissioning. This included orthodontic contracts, UOAs, NHS treatment, private practice and the tendering process. UOAs represent the units of activity of NHS orthodontists. Orthodontists providing NHS services will hold a contract for a certain number of UOAs which reflects how much activity they can provide on the NHS as well as their payment per UOA. Therefore, the total number of UOAs included in a provider’s contract reflects their NHS payment. At present, the tendering of NHS contracts is a complex issue affecting many orthodontists working in primary care; therefore, the number of queries associated with this is understandable and reflects the current uncertainty surrounding this issue. The BOS has been helping its members by providing free legal support and through events such as running a ‘Tendering for your Orthodontic Contract’ meeting and lectures dedicated to NHS commissioning which were given at the 2018 British Orthodontic Conference.
A number of associate-related queries were received by the BOS both from associates and from their employers with managing patient transfers and associate salaries being the most common themes. Transferring care within the same practice was more commonly queried than transferring to different practices. The BOS has an advice sheet available on their website regarding transferring patient care during treatment which, although this focuses on patients moving practice, also includes a proforma which may be a useful template to use if patients are transferring to a different clinician within the same practice (British Orthodontic Society, Moving and Transferring During Treatment). The details of arranging inter-practice transfers are usually best discussed at a local level between the orthodontists involved in providing the patients care.
As with inter-practice patient transfers, it is usually most appropriate to discuss any queries regarding associate salary details at a local level. Especially when salary queries are regarding payment for transfer cases, these topics must be carefully negotiated and agreed before undertaking a patient’s treatment. The British Dental Association (BDA) is the professional association and trade union for dentists in the UK and, as such, it is a good source of information on many topics and issues affecting dentists and provides advice to its members on topics such as contracts and salaries (British Dental Association, Associates).
The queries regarding clinical issues were varied and were from both orthodontic specialists and general dental practitioners (GDP). Many queries concerned specific clinical situations where, in reality, advice can only be given following a full clinical examination of the patient. The BOS are therefore unable to advise on individual cases. Where appropriate, a second opinion from an orthodontic consultant at a local district general hospital or teaching hospital is often advised. If professionals are unsure where to refer for a second opinion the BOS can provide them with a list of local hospital orthodontic departments. Even with the use of Referral Management Systems (RMS), clinicians should still be able to refer patients appropriately for a second opinion.
Queries relating to orthodontic therapists primarily had a clinical focus such as their clinical remit and the level of supervision required. The BOS have published guidelines on the supervision of orthodontic therapists which includes guidance on the different roles and responsibilities of the different members of the clinical team (British Orthodontic Society, Supervision of Orthodontic Therapists, 2017). This guidance should be followed in conjunction with the General Dental Council (GDC) Scope of Practice (2017), which outlines the roles and competencies of different dental care professionals. It is important that clinicians adhere to such guidelines to prevent any clinical malpractice or clinicians treating patients outside of their competency.
Additionally, there were a number of queries regarding the training process for orthodontic therapists. For the majority of these queries, the relevant information is available on the BOS website (British Orthodontic Society, Becoming an Orthodontic Therapist). Not only is the role and training information outlined here, but links are also provided to more information about the different institutions offering training programmes.
The advertising and media queries were mainly highlighting behaviour or advertisements professionals considered inappropriate. The BOS have released statements regarding inappropriate advertisements (British Orthodontic Society, BOS Statements). For concerned professionals, contacting the BOS provides an opportunity to seek advice as these queries can be further investigated by the appropriate committees. This is a unique service that the BOS offers as such queries are outside of the remit of other organisations such as indemnity providers.
Training-related enquiries can be broadly separated into those from overseas clinicians and those from UK dentists enquiring about UK training courses. The BOS Training Grades Group (TGG) is a group within the BOS for specialty trainees and can also be joined by those who are interested in applying for orthodontic specialty training. This group runs an annual study day that focuses on applying for orthodontic specialty training in the UK and information on this topic can also be found via the BOS website (British Orthodontic Society, Orthodontic Specialty Training in the UK, 2013). The BOS also provide information about ‘dentists with a special interest’ in orthodontics. These are valuable sources of information for training-related queries and can be found in the careers section of the BOS website (British Orthodontic Society, Careers in Orthodontics).
GDC queries focused on verifying if orthodontists were on the GDC specialist list, as well as querying the scope of practice of clinicians and enquiries regarding GDC ‘fitness to practice’. Many of the answers to these GDC queries could be found through GDC publications and guidelines, for example the Scope of Practice guidelines (General Dental Council, Scope of Practice 2017). Additionally, individuals can use the search facility on the GDC website to see if clinicians are registered on a GDC specialist list (General Dental Council, Specialist Lists).
Clinical governance issues encompassed a range of topics including: record keeping; data protection; confidentiality; and safeguarding. These queries could generally be answered by the BOS advice sheets which are available free of charge to BOS members (British Orthodontic Society, Members Advice Sheets). These advice sheets are frequently reviewed and updated by the BOS to reflect current guidance and regulations, to ensure that members are provided with up-to-date, accurate information. Some of these areas also overlapped with GDC publications and guidelines and as such information can also be found on these topics via GDC publications and on their website.
Only a limited number of queries were received from professionals regarding retainers, which mainly focused on guidelines for retention consent, who is responsible for the cost of replacement retainers and whether GDPs are able to provide and charge patients for replacement retainers on the NHS. The BOS have recently developed the ‘Hold that Smile’ campaign, which is designed to give patients and professionals more information on retention (British Orthodontic Society, Orthodontic Retention for Patients). This, together with further information available on the BOS website, should help to address a large number of queries regarding retention (British Orthodontic Society, Retainers). It will be interesting to see the impact of the ‘Hold that Smile’ campaign in the future.
The main query regarding the Community Dental Service (CDS) was concerning CDS salaries for which the CDS pay scale can be found on the NHS employers’ website (NHS Employers, Pay and Conditions Circulars for Medical and Dental Staff). The CDS provides dental care for people who are unbale to access care from a dental practice or hospital setting. In addition, the CDS provide dental services in a variety of setting including health centres, clinics, mobile clinics and, where appropriate, home visits, to enable improved access to dental care for individuals. A range of queries were received regarding hospital dental services, including: whether there are any guidelines for running multidisciplinary clinics; and the role of clinical assistants. The BOS can give overall guidance in certain areas, for example, BOS documents on the role of an orthodontic consultant and the management of orthognathic patients (British Orthodontic Society, Consultant Orthodontist Group). In conjunction to these, there may also be Trust-specific guidelines which should also be consulted when addressing such queries.
The BOS received a number of queries on specific issues relating to the business of the society, such as questions regarding eligibility for BOS prizes, who can access the BOS Virtual Learning Environment, permission to use BOS images, and permission to translate and use BOS patient information leaflets internationally. The BOS also received requests for recommending and providing expert witnesses. All these queries required direct and specific information from the Society. Due to the varied nature of these specific enquiries, it is unlikely that generic guidance could be developed for this category.
Patient queries
The queries received from patients covered a wide variety of topics, the most common of which was the eligibility for NHS treatment. Commonly, queries resulted from patients feeling that they were eligible for NHS treatment despite being declined NHS treatment by a practice or hospital. There were also a number of queries where patients had undergone private treatment and now felt that this should have been provided by the NHS. Additionally, patients moving to the UK often wanted to know if their orthodontic treatment could be continued on the NHS in the UK. A number of queries were also received regarding relapse and whether this could be treated on the NHS.
Published guidance is available on the NHS and the BOS websites, detailing the severity of malocclusions that are eligible for NHS treatment (British Orthodontic Society, What is the IOTN?; NHS England, Orthodontics). At the present time, the BOS also have a dedicated section on their website regarding orthodontics and the NHS, which contains a wealth of valuable information on topics such as the Index of Orthodontic Treatment Need (IOTN), eligibility for NHS treatment and what to do if the NHS will not fund a patient’s treatment (British Orthodontic Society, Orthodontics and the NHS). Where individuals are unaware of this resource, the BOS plays an important role in directing people towards this information.
In some situations, it is essential that a full clinical examination is carried out to enable more specific advice to be given. In such cases, seeking a second opinion is often advisable. Patients can seek a second opinion either from a local orthodontic practice or request to be referred to the orthodontic department within their local district general hospital or their closest teaching hospital. If patients are finding it difficult to obtain a second opinion, they can ask the BOS for a list of local orthodontic specialists or hospital departments. If there is still disagreement regarding the eligibility for NHS treatment, patients can request for their case to be assessed by their NHS Local Area Team who will follow the Individual Funding Request Process (IFR) to review the eligibility of the case for NHS treatment (NHS England, 2014).
A number of queries were received regarding patient charges which mainly included: patients being charged for a second opinion; charges for broken appliances; and charges for restorative treatment after the completion of orthodontic treatment. The BOS provides information on its website whereby it is explained that if a patient is undergoing NHS-funded treatment, the appliances, adjustments and any repairs required during treatment are covered by the NHS; however, there may be charges for the replacement of removable appliances that are lost or broken beyond repair (British Orthodontic Society, What does orthodontic treatment cost?). Although the BOS can provide overall guidance on NHS regulations, a lot of the queries received by the BOS were very specific; therefore, more information would be required before providing detailed advice. In such instances, patients should discuss the matter with their treating clinician and aim to resolve the grievance locally, in the first instance. If there is an issue between the clinician and the patient, then patients are advised to use the local complaints procedure which all practices are obliged to have in place.
The length of NHS waiting lists received a number of queries, with patients being concerned about the length of the wait and the subsequent delay before starting treatment. Waiting list lengths will vary from practice to practice and between different trusts; therefore, this is usually a matter which is best investigated at a local level. Patients referred for hospital consultant-led treatment should have a maximum waiting time of 18 weeks from the hospital receiving their referral to commencing treatment (NHS England, Guide to NHS Waiting Times). With the introduction of the new NHS orthodontic contacts, this may affect waiting lists in the NHS; however, this will only become apparent over time. Once the new contracts are established, it will be interesting to assess if this has an effect on the number of queries that are raised to the BOS both by patients and by professionals.
Patients often expressed concerns about a perceived lack of treatment provided at their appointments or a long duration between appointments. In these clinical situations, it is impossible to give appropriate advice without knowing the whole story. Good communication with patients is paramount to ensure that patients are up-to-date with their treatment progress and are informed about what treatment has been carried out at each appointment. Clinicians should always explain the timeframe until the patients’ next appointment and the rationale for this. Good communication helps to prevent any misunderstandings between patients and the clinicians in these areas and ensures that continued informed consent is forthcoming.
A number of queries were raised where an orthodontist had left a practice or retired and no provision had been made for the continuation of patient care. Patients also expressed concerns where it was difficult or not possible to contact their care provider. In addition, a number of queries were received about transferring care, often in situations where patients had moved and wished to find an orthodontist closer to their new home. A small number of queries were received from patients moving abroad and wishing to know if their NHS treatment could be continued abroad. The BOS has advice available on their website regarding patients transferring care (British Orthodontic Society, Moving and Transferring During Treatment). Current guidance is that under the NHS there should not be any obstacles to changing orthodontists during NHS treatment. Orthodontists can also accept patients who have commenced treatment elsewhere, either in the UK or abroad, although they are not obliged to do so. Patients wishing to transfer care will require a comprehensive assessment by the orthodontist to whom they wish to be transferred so that their case can be fully assessed before any transfer being agreed. The transfer the patients who have commenced NHS treatment to a different NHS provider is likely to be more straightforward than patients transferring from abroad or those who have commenced non-NHS treatment. In situations where patients have commenced treatment abroad or have commenced non-NHS treatment or are undergoing treatment with appliances that are not available on the NHS, their care may not be eligible to be continued on the NHS and these cases will need to be carefully assess on an individual basis.
If clinicians require further advice on patients wishing to transfer care or accepting transfer patients, this can be sought from the NHS Local Area Team, Managed Clinical Network for Orthodontics or the Local Orthodontic/Dental Committee. Details of Local Area Teams and their contact information can be found on the NHS England website (NHS England, Authorities and Trusts). The BDA is also a good source of information and provides a list of all of the Local Dental Committees (British Dental Association, Local Dental Committee Contacts).
A high number of queries were received from patients about specific clinical issues which were most commonly regarding different treatment options, indications for specific appliances and if certain appliances were available in the UK. A number of patients also contacted the BOS to express dissatisfaction with the outcome of their treatment or feeling that their treatment was taking too long. For the vast majority of clinical queries, a full patient history and clinical examination is required to be able to advise patients appropriately; therefore, the society is usually only acting as a mediator to advise patients to discuss such matters with their clinician or to seek a second opinion where appropriate.
If patients are unhappy with treatment that has been provided, they can seek a second opinion either from a local orthodontic specialist or request to be referred to the orthodontic department within their local district general hospital or their closest teaching hospital. The GDC Standards for Dental Professionals (2013) state that dentists should refer patients for a second opinion if the patient requests this. Similar to other instances where patients express dissatisfaction, if there is an issue between the clinician and the patient then patients are advised to use the local complaints procedure.
Queries regarding retainers fell into two main categories: clinical queries or queries regarding payment for retainers. Payment queries were more common than clinical queries and usually focused on patients being dissatisfied with having to pay for replacement retainers. Queries regarding payment for replacement retainers should, in the first instance, be directed to the practice or hospital department which completed the orthodontic treatment and provided the initial retainers as it is not within the remit of the BOS to set charges or make policy regarding the use or replacement of retainers. If patients remain unsatisfied, they can then either request to be referred for a second opinion or they can follow the practice or hospital complaints procedure. Questions were also addressed to the BOS regarding retention regimes and the types of retainers provided. The BOS ‘Hold that Smile’ campaign is specifically designed to give patents more information about retention and will enable patients to be better informed about long-term retention (British Orthodontic Society, Orthodontic Retention).
Only a small number of queries were received regarding clinical governance topics and these could usually be address through BOS and GDC publications and guidance (GDC, Standards for the Dental Team, 2013; British Orthodontic Society, Orthodontic Records: Collection and Management, 2015). Finally, the BOS received a number of specific enquires, for example: requesting recommendations for clinicians; enquiring if clinicians were BOS members; enquiring if clinicians were registered on the GDC specialist list; and also requesting permission to use BOS information. Information regarding whether a clinician is a member of the BOS can be requested directly from the BOS. The BOS do not recommend individual clinicians; however, they can provide patients with a list of local orthodontic specialists or hospital departments which provide orthodontic treatment. The GDC hold the specialist lists for each dental specialty and members of the public can search these lists to see if clinicians are registered on a GDC specialist list (GDC, Specialist Lists). If individuals are unaware of this facility, the BOS can aid an enquiry by informing the individual about this service available on the GDC website.
Assessing the queries raised to the BOS by both patients and professional has been very valuable and it has allowed the number of queries raised to be quantified and common topic areas identified. This enables the BOS to identify areas where information and advice already exist as well as areas where resources can be further developed in the future. Continually assessing the queries raised to the BOS and how these change over time would be very useful and can be carried out regularly.
Conclusion
Overall, in the timeframe assessed, the BOS received a high number of queries from both patients and professionals. These queries were varied and covered a range of topics. The most common topics queried by professionals were commissioning, matters concerning associates and specific clinical issues, while the most common topics queried by patients were the eligibility for NHS treatment and specific clinical issues. While some queries required specific information from the BOS, the majority of the queries could be addressed through already published information and guidelines which are readily available to patients and the public. This paper documents the more common queries and provides guidance on where to find the appropriate advice for them.
Footnotes
Acknowledgements
The authors thank Ann Wright at the British Orthodontic Society for her assistance with data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.