
Abstract
Objective:
To explore the relationship between malocclusion, orthodontic treatment and peer relationships in adolescents.
Design:
A cross-sectional qualitative study.
Setting:
Three secondary schools in the South-East of the U.K.
Participants:
A total of 14 schoolchildren aged 14–16 years (mean age = 15.7 years; age range = 14.4–16.5 years).
Methods:
In-depth one-to-one semi-structured interviews carried out online. All interviews were transcribed verbatim and analysed thematically according to Braun and Clarke’s model of thematic analysis.
Results:
The central finding of this research was that adolescents are self-conscious of their dental appearance, it impacts on social interactions, and peers and friends are both a source of pressure and support regarding dental appearance and treatment. Two main themes were identified: (1) malocclusion and peer relationships; and (2) social expectations and experience of orthodontic treatment. Participants reported being self-consciousness of their teeth before treatment, and this increased with age. They feared being judged based on their dental appearance, undertaking behaviour to hide their teeth in social situations, in photographs or online. All participants reported either being teased personally about their teeth or witnessing this happening to someone else although they mostly did not see this as bullying. This had a negative impact on self-confidence. No one reported being teased after starting orthodontic treatment. Orthodontic treatment was seen as desirable and normal within this age group, with an expectation it would improve self-confidence, particularly in social settings. Friends and peers were a source of support during treatment.
Conclusion:
Young people are self-conscious of their dental appearance, which impacts their peer relationships and can make them a target for teasing and bullying. Orthodontic treatment is considered normal, with peers and friends providing support.
Plain language summary
Having a malocclusion in the form of crooked or sticking-out teeth is very common, meaning a lot of children and adolescents wear braces. This is during a period when they are moving away from the control of their parents or guardians and their psychosocial development is more influenced by their peers. Peer relationships are very important for healthy development, with poor relationships or being a victim bullying being linked to loneliness, depression, poor academic achievement and poorer quality of life in the long term. In this study, we interviewed 14 young people aged 14–16 years about their social experiences of having crooked or sticking-out teeth and subsequently braces to treat them. From the interviews, it was found that being very self-conscious and embarrassed socially about their teeth was very common, resulting in trying to avoid smiling and hiding their teeth in photographs. As this study was carried out during the COVID-19 pandemic, a couple of the participants reported that wearing face masks made them feel more confident. They also felt they were being judged by their peers about the appearance of their teeth, even if nothing explicit was said. They in turn were aware they judged other people. All the young people had either experienced being teased or having mean comments made about their teeth or witnessed it happening to someone else. Although most tried to shrug this off, it was apparent that some of the young people found this very hurtful both in the short and long term. Most were having brace treatment or waiting for it to start. This was seen as positive thing and a normal part of growing up. None of them reported being teased for wearing braces and their friends were very supportive and helpful during treatment.
Introduction
Peer relationships are interpersonal relationships established and developed as a result of social interactions among peers or individuals with similar levels of psychological development (La Greca and Harrison, 2005). They are shaped by numerous factors, both individual and environmental, and are crucial for healthy social and psychological development (Mitic et al., 2021). Poor peer relationships in adolescence are associated with higher levels of social anxiety, loneliness, depression, poor academic achievement and poorer quality of life (Kochel et al., 2017; Ranøyen et al., 2019; Schwartz-Mette et al., 2020; Woodward and Ferguson, 2000).
Malocclusion has been shown to impact peer relationships. Patients with an aesthetically handicapping malocclusion report higher levels of loneliness, particularly girls (DiBiase et al., 2025). Teenagers fear being judged by their peers, are aware of other people’s teeth and often judge themselves negatively against others (Taghavi Bayat et al., 2013; Trulsson et al., 2002). This can affect their behaviour, for example by trying to avoid showing their teeth when smiling and in photographs (Josefsson et al., 2010; Prado et al., 2022). Although most young people seek orthodontic treatment primarily to improve their dental aesthetics, there is also an expectation that having straight teeth and a nice smile will improve peer relationships, self-esteem and dental health (Geoghegan et al., 2019; Josefsson et al., 2010; Prabakaran et al., 2012; Prado et al., 2022; Shah et al., 2019; Trulsson et al., 2002).
Ontologically, the majority of research in orthodontics has focussed on treatment mechanics and morphological outcomes. Although these are useful in measuring the success of treatment from a clinician’s perspective, they often mean very little to the patient. Epistemologically, therefore, in the past two decades, there has been a move to more patient-centred research. Following a neo-positivist approach, this has primarily been through questionnaire-based quantitative research using oral health-related quality of life (OHRQoL). This research has shown that although there is a relationship between malocclusion and OHRQoL, OHRQoL is also affected by other factors including age, gender, socioeconomic status, self-esteem and peer relationships (Agou et al., 2008; Alrashed and Alqerban, 2021; Benson et al., 2015; DiBiase et al., 2025: Dimberg et al., 2015; Goranson et al., 2023).
To date, however, despite anecdotal reports from patients, there is little quantitative evidence of any long-term dental health or psychological benefits of orthodontic treatment (Kenealy et al., 2007; Macey et al., 2020). This may be because we are focussing on the wrong outcome measures rather than what our patients want or expect from treatment. As most of our patients seek orthodontic treatment primarily to improve their dental and smile aesthetics, which play an important role in social interactions (Kettle and Warren, 2024), we propose that the main impact of malocclusion, and therefore the principal benefit of orthodontic treatment, is social, improving an individual’s confidence in group situations and their perception of their peer relationships.
Epistemologically, it is difficult to quantify and measure patients’ experiences and expectations as every one of our patients is unique and does not necessarily regress to the mean of quantitative data. Therefore, we have less of an understanding about the individual experience of having a malocclusion and undergoing orthodontic treatment and the impact these have on peer relationships. This is an area where qualitative research can play an important role. It can provide an in-depth understanding of an individual’s experiences, especially in a complex area such as orthodontic treatment, which occurs over an extended period and usually during adolescence, a time of physical, emotional and social change. It can give contextual insight allowing understanding of expectations and behaviour while putting the participant at the centre of the research. In orthodontics much of the qualitative research to date has focussed on individual motivation, expectations and experience of treatment (Abed Al Jawad et al., 2012; Almeida et al., 2018; AlQuraini et al., 2019; Kettle et al., 2020; Mohammed et al., 2022, 2024). Less is known about the social aspects of malocclusion and treatment, particularly in how this is influenced by, and influences, peer relationships. Approaching this from the ontological position that the main impacts of malocclusion, and therefore the principal benefits of orthodontic treatment, are social, the aim of this study was to explore the relationship between malocclusion, orthodontic treatment and peer relationships. More specifically, the research examined whether malocclusion affects social interactions and may make an individual a target of bullying or victimisation, as well as the motivations for and expectations of orthodontic treatment in relation to peer relationships and the perceived social benefits of treatment.
Methods
This was a cross-sectional qualitative study, involving participants originally recruited to a study investigating the relationship between bullying, peer relationships and malocclusion in schoolchildren aged 10–14 years in the South-East of the U.K.( DiBiase et al., 2024). Ethical approval was obtained from the London-Surrey Research Ethics Committee (no. 17/LO/0791). Further ethical approval was sought from the same committee to allow follow-up of the original sample group. This was granted on 2 May 2020, coinciding with school closure due to the COVID-19 pandemic. As this had a significant impact on potential recruitment to this study, a further amendment and ethical approval were sought to undertake consent, data collection and interviews online, which was granted on 8 July 2021.
Participants
Participants were recruited from the original sample group of 698 adolescents recruited from 16 schools in the South-East of the U.K. The schools were contacted initially to see if they were willing to participate in this follow-up study (Figure 1). Of the original 16 schools, six initially agreed to participate, but only three ultimately took part. A letter of invitation was sent out via the school to all the parents or guardians of all students who had participated in the original study. This included information for both the student and the parent/guardian, followed by a second letter 4 weeks later. The letters included the research team’s contact details and a form for parents/guardians to express interest in participation. When a potential participant contacted the research team, they were contacted directly and screened for interview eligibility based on the following criteria:
- Had undergone/were currently undergoing orthodontic treatment
- Awaiting orthodontic treatment
- Wanted orthodontic treatment but unable to access it
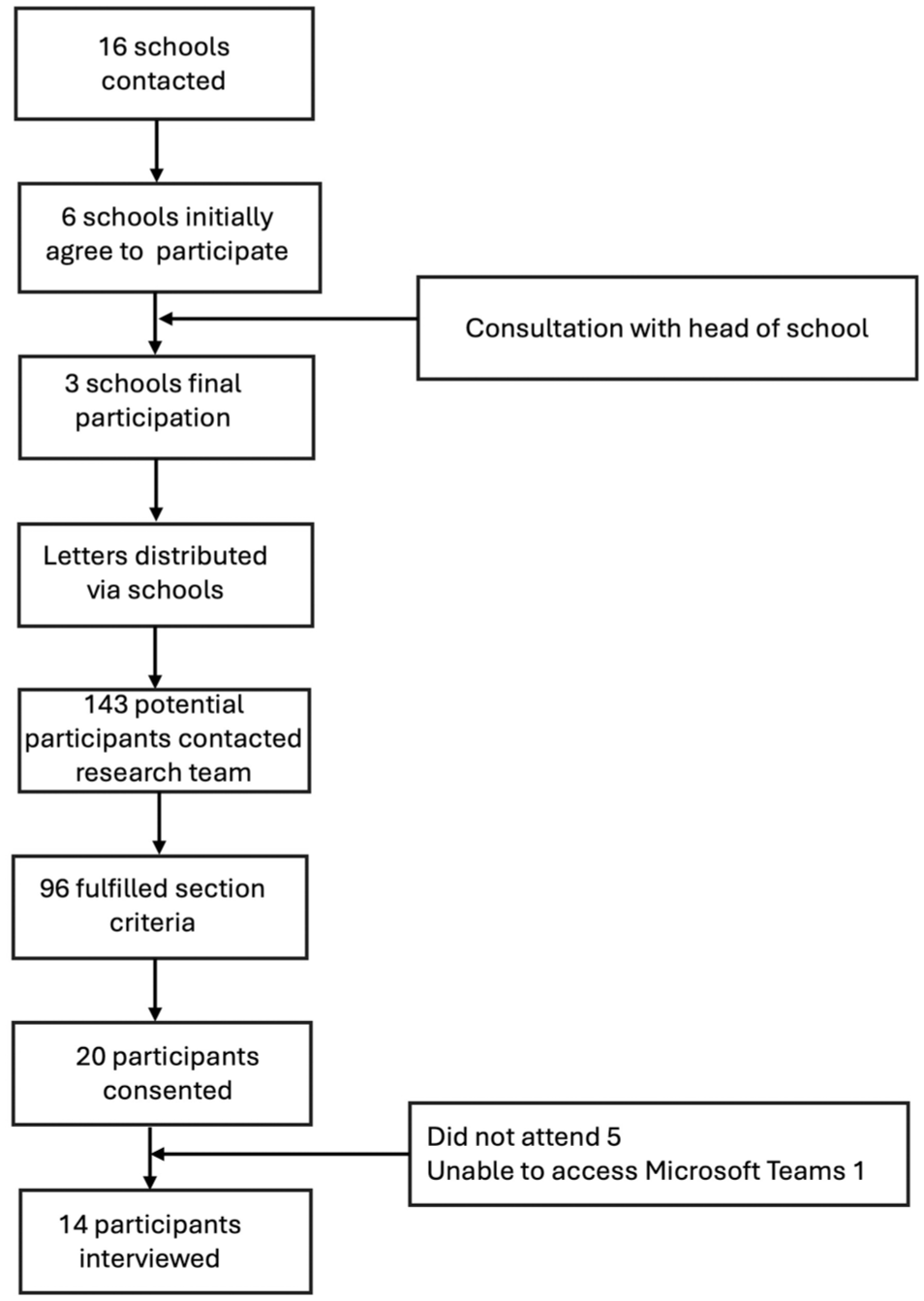
Flow chart showing participant recruitment and drop-out.
The participants selected for interview were contacted directly by the research team, provided consent and a mutual time was set up for interview.
Interviews
One-to-one interviews were conducted online using Microsoft Teams 1.3.00.13565 (Microsoft Corp., Redmond, WA, USA). The interviews were semi-structured and the participants were encouraged to talk about anything they felt was significant regarding their experiences of malocclusion and orthodontic treatment but focussing on the impact on, and influence of, peer relationships. Interviews were based on a topic guide, which included a list of relevant questions, prompts and probes for follow-up questions to encourage participants to elaborate on their thoughts, experiences and perceptions. Questions in the topic guide were developed by the research team based on previous research findings. The interviews took place between August 2021 and February 2022 and were carried out by a psychology research assistant with training in interview techniques related to qualitative research (Qualitative Research Methods in Health, University College London 2022) (SA). A psychology research assistant was selected to undertake the interviews due to similarity with the participants in terms of age and recent experience of orthodontic treatment but with limited technical understanding of orthodontics to try and reduce bias and bringing personal assumptions to the interview. Pilot interviews were carried out online with first year university students supervised by a senior psychology researcher with extensive experience of qualitative research methodology (LC) before commencing the study to allow the interviewer to gain experience. The participants were informed at the start of the interview of the purpose and nature of the interview and that the interviewer had herself undergone a course of orthodontic treatment in adolescence. They were advised they could have someone with them when they were being interviewed although all opted to be alone. With consent of the participants, the interviews were recorded and transcribed verbatim by two research assistants (SA, VA) and cross-checked for accuracy. The transcripts were saved and coding conducted in Nvivo 14 (Lumivero, Denver, CO, USA).
Analysis of the interviews
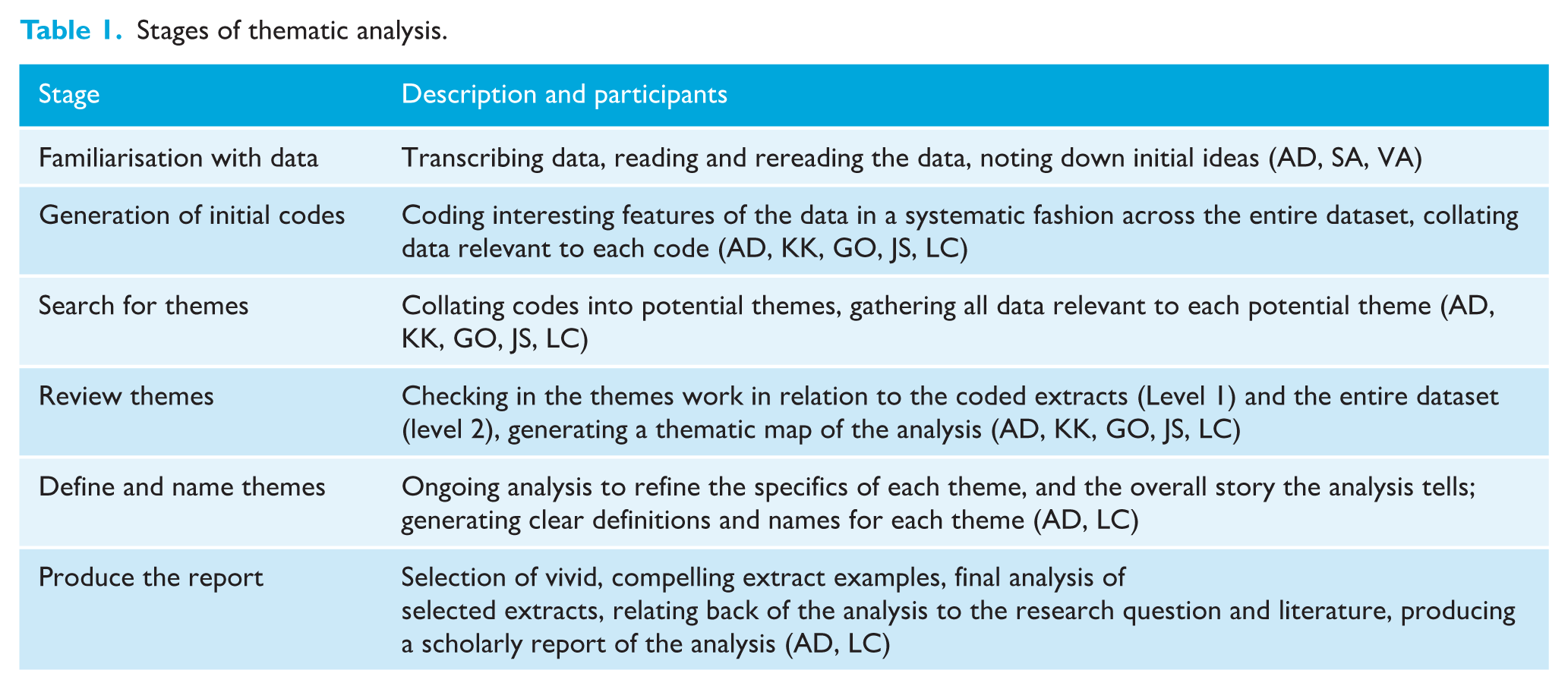
Transcripts were coded using thematic analysis. Analysis was conducted using the six-phase analytic process set out by Braun and Clark (2006) (Table 1). Although we applied a reflexive approach accounting for the epistemological/ontological beliefs and expectations of the researchers, in light of research questions we set ourselves and the intended audience, the analysis was primarily theoretical or deductive in nature (Braun and Clarke, 2019a). This was undertaken at a semantic level, focussing on the interpretation of the explicit meaning expressed in the data. This means that although we hope to have addressed the research questions we set ourselves, the dataset undoubtedly contains additional themes or underlying ideas that have not been explored. We adopted an essentialist/realist approach to the analysis, focussing on individual responses and themes. Values and beliefs relating to malocclusion and orthodontic treatment are also socially and culturally constructed and have only been partially explored in this study.
Stages of thematic analysis.
Analysis
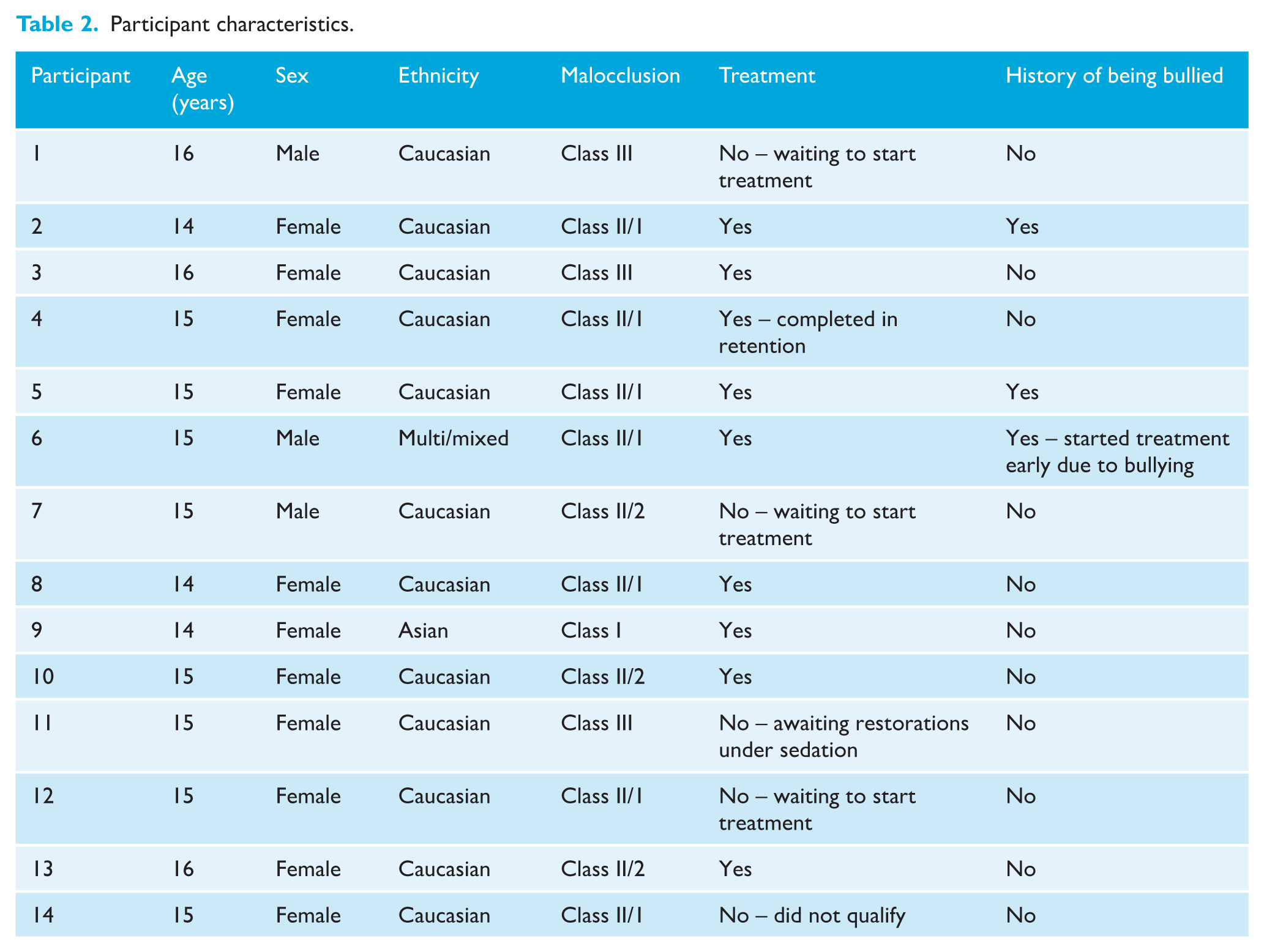
A total of 143 individuals contacted the research team, of whom 20 provided consent and 14 ultimately participating in interviews (Figure 1). The mean age was 15.7 years (range = 14.4–16.5 years) and the majority of the participants were female (n = 11/14) and currently undergoing orthodontic treatment (n = 10/14) (Table 2). Of the four participants not undergoing treatment, P1 and P7 were currently waiting to start treatment, P11 reported high levels of anxiety and was awaiting restorative work under sedation before orthodontic treatment, while P14 wanted treatment but did not qualify for NHS treatment. Each interview lasted approximately 45 min.
Participant characteristics.
Two inter-related themes were generated that create a narrative about the intricate relationship between malocclusion, orthodontic treatment and peer relationships.
Theme 1: Malocclusion and peer relationships
The participants all reported how having a malocclusion and subsequent orthodontic treatment impacted on their peer relationships in both positive and negative ways. An overriding subtheme of this that developed from the data concerned young people being self-conscious and feeling judged by their peers based on their dental appearance, which they felt affected their self-esteem and confidence. They reported it affected their behaviour, and they tried to avoid showing their teeth in social interactions. Young people also felt pressured by their peers, both implicitly and explicitly, to seek orthodontic treatment.
Participants reported not liking their teeth before orthodontic treatment and being very self-conscious or embarrassed about their dental appearance, especially in social situations, with several participants reporting they felt people were staring at their teeth: ‘I don’t like pictures of me when I smile or just like whenever I look in the mirror or like brushing my teeth.’ (P12) ‘I don’t really like people looking at my mouth when I smile kind of thing.’ (P10) ‘People would look at my teeth quite a lot. That’s why I don’t smile because I know, they noticed that.’ (P7)
Participants reported this led to a lack of confidence in social situations and social anxiety, especially when meeting new people, even if nothing was said: ‘Well, I definitely felt more shy because I didn’t want anyone to look at me. I wasn’t really confident into going up to people.’ (P8) ‘I worry what other people think about my teeth especially if I'm with someone that I don’t know. I really like worry what they might think.’ (P14)
Participants reported becoming more self-conscious of dental appearance with age, with a corresponding greater impact on social confidence: ‘Well, I mean, I didn’t like them, and stuff like in primary school though, I like, I don’t really care. And then in like secondary school, I think I started to care more about what I looked like and stuff and then like I didn’t like my teeth.’ (P2)
As well as being self-conscious about their teeth, participants reported that they felt they were being judged on their dental appearance, even if not overtly, and they worried about what other people thought of them. They were at the same time aware that appearance-based judgement was a universal behaviour and they in turn judge people in the same way: ‘I guess that you’re scared other people will judge you for that [appearance of teeth], because you’re kind of judging other people.’ (P13) ‘I really try to not judge people on how they look. And yeah, you can try as hard as you want, but it always happens.’ (P3) ‘I just always thought that people would like, treat me differently. But I know that was in my head, so I kind of just let it go.’ (P7)
This included broader moral and socioeconomic judgements, with having good teeth and a nice smile being associated with being a good person and affluence, and having malocclusion and a poor smile associated with being a bad person and poverty: ‘In some people’s minds subconsciously, they would perceive you as a better person. Depending on your teeth, because if you had really awful teeth, I think it would change their view on you.’ (P4) ‘Some people, like, couldn’t afford to have braces and stuff. So, then you might think, oh, they’re poor or something by having like wonky teeth. If you have really straight white teeth, like ones that almost look like composite bonding and stuff like that, then you definitely would look like you’re rich.’ (P13)
Participants reported they felt under pressure socially from peers to have orthodontic treatment: ‘You have that extra added pressure of people saying things like “Oh their teeth are wonky” or making jokes and things like that so it’s preventable by getting braces.’ (P5) ‘It’s mainly just people around me being just like, oh, you’re gonna need braces. Or else people want like you to have stuff like that. So, it’s kind of like subliminal messaging that has gotten me to the point I’m at [deciding to have orthodontic treatment].’ (P1) ‘Once, I wanted to start crying because the boys are like, “you should get braces treatment”, before I got braces.’ (P2)
Participants, however, did not feel judged by friends, who they felt were more accepting: ‘With my friends, I like to think at least that they get along with me well because of how I act, how I am, not just how I look.’ (P1)
Participants reported actively trying hide their teeth in social situations and online, avoiding smiling and showing their teeth, for example in photographs.
‘I, like, take a selfie on my phone and so you can only see the top half of my face, it’s just like my eyes and forehead.’ (P3) ‘Well, I didn’t smile ever like in pictures or anything. Even when I talk to people I would never smile.’ (P7)
This all highlights the increased level of self-consciousness and embarrassment this age group feels about their dental appearance and how this increases from childhood to adolescence. This included affecting behaviour in social interactions with participants actively trying to hide their teeth most notably avoiding smiling, which supports previous research (Josefsson et al., 2010; Mohammed et al., 2023; Prado et al., 2022; Taghavi Bayat et al., 2013; Trulsson, 2002). The influence of peers as a motivating factor to seek orthodontic treatment has also previously been highlighted (Longstaff et al., 2021; Prado et al., 2022). An interesting finding of the current study was participants reporting not feeling judged solely on their appearance by their friends but on their character and behaviour. Friendship in childhood and adolescence has previously been shown to be important for healthy psychological development (Waldrip et al., 2008).
The current research was conducted in the aftermath of the COVID-19 pandemic, with so much of young people’s social and academic world moving online. Although advertising, television and social media have previously been shown to influence young people’s desire for orthodontic treatment (Josefsson et al., 2010: Longstaff et al., 2021; Taghavi Bayat et al., 2013), the current study revealed a number of perceptions and experiences specific to that point in time, particularly behavioural. Most preferred not to have the camera on during online lessons and discussed the use of lighting and filters to enhance their appearance. A number of participants reported they found face masks and online lessons, in which they could turn their cameras off, provided a means of escape from the self-consciousness they would normally experience, related to their teeth, and provided some relief from the fear of negative responses from peers they would normally experience.
‘I have the mask on all the time. That brings a little comfort to me, like when I’m at school. So, I very much appreciated masks because it kind of made me look like it made me feel like I was less like a bunny.’ (P12)
The impact of the pandemic on this generation’s mental health, which may have heightened negative concerns about appearance particularly in girls, has previously been reported; however, it remains to be seen if the effects are long term (Choukas-Bradley et al., 2022; Holt-White et al., 2022).
In relation to orthodontic patients, previous research has investigated issues that the pandemic had relating to treatment progression and psychosocial effects but not in relation to potential perceived positive benefits such as mask wearing (Wafaie et al., 2022).
One of the main issues that was discussed was the prevalence of bullying and teasing directly related to dental appearance, which in part reflects the nature of the interview and research aims of the study. All participants reported being either being victims or witnessing bullying or teasing related to dental appearance. This was primarily non-physical in nature, mostly making mean comments behind someone’s back or online usually as a comment on photographs that the participant had posted on social media sites: ‘From a young age, I was suffering a bit of bullying in school because of my teeth. At the time I don’t think it really bothered me that much at the time. I suppose it only really bothered me when people started saying things.’ (P8) ‘There was some girl who said some really nasty stuff about my teeth, and I think that like definitely made it worse. What she said wasn’t very nice, but it wasn’t to me. It was behind my back to quite a few other people. I obviously felt more insecure about how they looked.’ (P14) ‘I’ve had it before like a photo of me being sent to a group chat, people have been talking about me and not in the most like particularly nice way.’ (P5)
An association between bullying and certain traits of malocclusion has previously been found, with the incidence varying greatly dependent on the definition of bullying used, the sample group and the geographic location (DiBiase et al., 2024; Seehra et al., 2011; Tristao et al., 2020). Although not all participants reported being bullied or teased personally about their teeth, without exception all had observed it happening to other people and were aware of the impact this could have on the victim: ‘Well, there was this one person, and her teeth were very well all over the place. And she would get called things like a rabbit and stuff.’ (P8) ‘Even if she wasn't insecure about her teeth someone making a comment like that, you know, that would affect me.’ (P5) ‘Like, this girl had her front teeth, were more like what do you call it like, you know, like, forward, yeah. So, they would like call bunny teeth and stuff.’ (P9)
Although most of the participants claimed, or were not aware of, being affected by insults or comments made about their dental appearance, some did talk about how this impacted them in the longer term. One participant observed that their experience had stayed with them, suggesting it had impacted them in a way they were not able to fully process or articulate: ‘I think they got to me like because as much as I can try the right things like that not to get to me, it’s hard to stop them completely, so they definitely like got me a little bit.’ (P3) ‘No, not really [when asked if a comment made about their teeth bothered them] but I just think it’s kind of weird that I’ve held that one comment in my head for like 6 years.’ (P12)
There is a wealth of research showing the long-term negative effects of bullying, including depression, anxiety, relationship problems and social isolation, poor physical health and life outcomes (Arseneault et al., 2010; Copeland et al., 2013; Gladstone et al., 2006). A number of participants were sanguine about comments based on dental appearance. They did not interpret them to be malicious, seeing them as not meant to cause insult or believed these comments to be an attempt at humour, particularly if it was made by someone they liked, or this was acceptable behaviour within their friendship group: ‘The most creative insult I think I ever got was someone called me a vending machine. They were like, they were like: are you a vending machine? Can I put some coins? I was like “OK”?’ (P3) ‘Like I do remember though, like one of my friends and somebody said like it was her best friend though, but he was like “Oh gappy” or something. And then she was just like “Oh stop”. Like it wasn't like deep. Like, it’s not like she was getting upset, like it was just like funny thing because they were her friends.’ (P12)
None of the participants reported being bullied once they started orthodontic treatment. Although this may be in part indicative of other factors, such as the age of the participants and the school environment, it also would imply the implementation of orthodontic treatment in itself has a positive impact on children and adolescents who are experiencing bullying due to their dental appearance (Seehra et al., 2013; Shah et al., 2019).
Theme 2: Social expectations and experience of treatment
The majority of participants were undergoing or waiting to start treatment, and they discussed how this had impacted on peer relationships, as well as how their friendships were a source of support for them during treatment. Orthodontic treatment was universally seen as ‘normal’ and acceptable by the participants and a part of growing up, accompanied by an expectation that treatment should ideally be carried out in childhood or adolescence when a lot of their peers were undergoing the same experience, normalising it and making it socially acceptable: ‘I didn’t think of them as cool, I just kind of thought of them like a normal thing you would get when your teenager is like. You get the braces, and you get them off when you’re an adult.’ (P3) ‘Loads of people have braces, I think, and stuff. You’ll get them at different times. A lot of people got them on in like year 7 and year 8. But it’s not like nobody really cares if you have braces.’ (P13)
It was considered unusual and less socially acceptable to have orthodontic treatment as an adult: ‘I think, but I think if anyone’s got them at any age, it’s fine. But it’s just a bit more odd, but sort of, oh, you’ve got braces at 25, that’s a bit different. Because you know, you’re at work at that age. Not many people do have them at that age. You’re not really with a community that are going through the same thing as you. So yeah, I think it’s a bit different.’ (P7)
The acceptance and desirability of treatment in adolescent patients and their parents/guardians have previously been reported (Geoghegan et al., 2019; Longstaff et al., 2021). Despite this, several participants currently in fixed appliance treatment highlighted the problems they had eating socially, as food got stuck in their appliance and they were not able to clean their teeth. One participant actively avoided eating at school because of this: ‘Sometimes I didn’t eat at school. I don’t have lunch at school. Because if it’s something, if I see my teeth because on the toilets, there are no mirrors so I can’t see my teeth, if they’re dirty. So, I prefer just to not eat.’ (P2) ‘To do like with smiling and stuff, especially like it’s quite difficult to clean the braces right. Especially if you’re in school and like you have lunch.’ (P3)
Participants reported discussing their treatment with friends who had also gone through the same experience. Orthodontic treatment was therefore creating connections and binding young people in a new way: friends were viewed as a source of support and information without judgement, which has previously been reported (Longstaff et al., 2021; McNair et al., 2006): ‘Yes, I had a small friendship group. And well, they all had some sort of treatment to their teeth as well. All of my friends. And they didn’t really judge me because, they knew how it was.’ (P8) ‘Like, I suppose it’s probably just nice to talk to people who have like, gone through and experienced the same thing that you have. And it’s just nice to know that there are people like that.’ (P6)
Overwhelmingly, there was a belief among participants that treatment would improve social and emotional well-being and self-confidence in social situations, allowing them to smile without embarrassment and worrying about being judged: ‘But I know that once it’s over, I know I will be way more confident.’ (P8) ‘I think I’ll be able to like, smile and laugh [after orthodontic treatment]. Not covering my mouth and like worrying what other people would think of me, even when I’m eating and stuff.’ (P14) ‘I think I’ll stop hearing comments, like negative comments or have more positive comments. Yeah, I think I will feel more confident.’ (P2)
This finding again supports previous research that a major incentive to pursue treatment is social, with an expectation that it will reduce social anxiety and improve peer relationships (AlQuraini et al., 2019; McNair et al., 2006; Mohammed et al., 2022; Twigge et al., 2016).
Discussion
The results of this study show that dental appearance causes a high degree of self-consciousness that increases from childhood to adolescence, with a belief that it results in being judged by peers, with most participants reporting undertaking behaviour to try and hide their teeth in social situations or photographs. All participants reported being teased or having nasty comments made about their teeth or witnessing it happening to others. Although many stated that this did not upset them, several reported that they were still affected by the comments, even though they may not have been able to articulate the specific impact this had. There was also a tendency not to see this behaviour as malicious, especially if it came from someone whom they considered a friend. Orthodontic treatment was seen as desirable and normal at this age, with an expectation it would improve confidence in social situations. Peers and friendship groups were a source of support and information during treatment.
This study shows that dental appearance matters socially to young people and it can affect their peer relationships. This reinforces the importance of our teeth and smile in social interactions and the impact that malocclusion can have. Similarly, it would imply that ultimately the main benefits of orthodontic treatment are social, which is an important finding as poor relationships are related to negative psychosocial outcomes (Deater-Deckard, 2001; Kochel et al., 2017; Pickering et al., 2020; Ranøyen et al., 2019; Schwartz-Mette et al., 2020; Woodward and Ferguson, 2000).
A concerning finding in this study is that all participants had either experienced or witnessed what would be considered bullying in relation to dental appearance, which shows how prevalent it is. This is consistent with previous research showing a relationship between certain traits of malocclusion and being a victim of bullying (Seehra et al., 2011; Tristao et al., 2020). However, most of the young people in this study did not see it as bullying but rather as normal behaviour in this age group, often trying to make light of it, saying it had little impact on them or that it was meant in humour. This strategy arguably allows young people to maintain face within their peer group and friendships with those making comments. Despite trying to minimise the impact of such comments, several participants reported being affected in the longer term, still thinking about what had been said: clearly these instances were memorable, as participants recalled them easily, and in detail, despite the incidents in some cases happening a number of years ago.
In this study, orthodontic treatment was universally seen as normal or indeed desirable, a belief that is driven both by the judgements of individuals with untreated malocclusion and the prevalence of orthodontic treatment in this age group. During treatment, participants found friends supportive. This consisted of feeling they were part of a community with everyone having treatment at the same time, they were able to be themselves among friends without fear of judgement and talking with friends about treatment. Overall, the experience of this group socially in relation to orthodontic treatment was very positive. However, issues were raised on eating at school with fixed appliances, with one participant reporting not eating at school due to the fear of bits of food getting caught in her appliance and not being able to clean it properly. With the huge increase in eating disorders reported in this age group over the past decade, this is a concern (Pastore et al., 2023). Therefore, schools should be encouraged to provide adequate facilities for young people undergoing orthodontic treatment, particularly fixed appliances, to be able to clean their teeth and appliances after eating.
The age of orthodontic treatment was also an important issue: treatment was seen as normal in adolescence but not in adulthood. Teenagers have a strong desire for social proof, to be like everyone else, leading them to seek treatment at the same time as their peers (Trulsson et al., 2002). It is seen as a rite of passage from childhood and adolescence into adulthood (Longstaff et al., 2021). Access to treatment also reflected an underlying social judgement on a person’s financial status, despite the majority of individuals in this study receiving their treatment on the NHS, meaning there was no direct personal cost. The one participant who did not receive NHS treatment because her malocclusion fell below the acceptance criteria remained unhappy with the appearance of her teeth. Meanwhile, a participant who was undergoing treatment specifically supported the provision of orthodontic treatment by the NHS because of its positive psychosocial benefits and felt it should be eligible to more people. However, this is not reflected in the current funding model in the UK, which is defined on morphological features of the malocclusion not its psychosocial impact.
Limitations
The COVID-19 pandemic had a significant impact on the design of and recruitment to this study. This reflected in the number of schools that were ultimately recruited from, the sample used and the nature of the interviews. Although online interviews are more convenient than being face-to-face in terms of scheduling, they may arguably have affected the development of a rapport between the interviewer and participants and the ability to pick up and react to non-verbal cues (Lobe et al., 2022). However, online interviews (as opposed to face-to-face) with young people may be less detrimental to interview quality and rapport than one may expect. It does not appear to affect conversational involvement or impact on the quality of the data that can be generated (Anthony et al., 2025). The social restrictions caused by the pandemic may have affected the participants’ perceptions and experiences, which are reflected to some extent in the findings of this study. This may affect the generalisability of the results. However, as the findings are supported by previous research, we consider them applicable to adolescents in the UK and other similar countries. We also believe that this study makes an important contribution to understanding young people’s experiences during this unique period in time.
In qualitative research, sample size is highly debated. The concept of data saturation has previously been used to provide a cutoff point at which no further recruitment is considered necessary. However, the appropriateness this practice has been questioned in terms of what it actually means, whether it is ever possible to determine that it has been achieved, and its neo-positivist epistemological approach, which is inconsistent with the principles of reflexive thematic analysis (Braun and Clarke, 2019b). The original plan was to recruit 20 participants, but ultimately only 14 were interviewed, primarily because of non-attendance. However, we feel that the depth and nature of the interviews provided sufficient information power within the dataset to address the research questions.
Qualitative research methodology is incredibly varied and diverse (Holloway and Todres, 2003). In a speciality like orthodontics, which is patient-driven, with individuals actively seeking treatment to address specific concerns, qualitative research can add depth to our understanding. Through its theoretical freedom, thematic analysis provides a flexible and useful research tool, which can potentially provide a rich and detailed, yet complex account of data. Although not associated with a particular epistemological position, such as analyses like grounded theory, the use of thematic analysis is still tied to the theoretical framework that prompted the research question, both from the perspective of the team carrying out the research and the broader society in which it occurs. It is important to acknowledge that this will undoubtedly influence the direction and content of the interviews.
A common finding in this study was the experience of or witnessing of teasing or name calling in relation to dental appearance. This study represents a follow-up study to a quantitative study looking specifically at the relationship between malocclusion and bullying. The initial aim was to follow up the participants who reported being bullied in the original study, thereby providing longitudinal data to investigate whether orthodontic treatment had a positive impact of their experiences (DiBiase et al., 2024). This was not possible because of the high level of attrition, primarily resulting from the COVID-19 pandemic and the limited number of schools ultimately involved in the study. However, despite the majority of the sample having not previously been identified as being bullied, it was concerning how commonly participants reported experiencing or witnessing teasing or name calling related to dental appearance before treatment, suggesting that this behaviour is widespread. Although none of the participants reported experiencing or witnessing bullying of themselves or their peers during treatment, we cannot conclude whether the provision of orthodontic treatment itself reduced levels of bullying.
The sample consisted of mostly adolescent girls. Gender differences have previously been reported in relation to OHRQoL, with girls and women having a stronger relationship between OHRQoL and malocclusion (Rantavuori et al., 2023; Twigge et al., 2016). With a sample mainly consisting of female adolescents, this may have led to a greater emphasis on the psychosocial impact of a malocclusion than we would find if our sample included more boys. Future research should look more closely at the nature of the relationship between peer relations, malocclusion and orthodontic treatment in male adolescents.
Conclusions
Adolescents have a high level of self-consciousness about their dental appearance, which is reflected in behavioural strategies they will undertake to try and hide their teeth in social situations, online and in photographs. They judge others and fear being judged themselves based on dental appearance. Most have experienced or witnessed teasing or having negative comments made about them regarding their teeth and this has a long-term psychological impact. Orthodontic treatment was perceived as desirable, even in cases of mild malocclusion, with the expectation that, in addition to improving dental aesthetics, it would enhance social confidence. Their friends and peers were described as a source of support during treatment, and no participants reported being bullied or teased for wearing braces.
Footnotes
Acknowledgements
We would like to thank the schools and their students and teachers who participated in this study. We would also like to thank Kirsty Kemp, Gabrielle Oblea, Jamie Scott and Vinnie Akombo from the University of Kent for their help with transcription and coding.
Ethical considerations
Ethical approval was obtained on 21 July 2017 from the London-Surrey Research Ethics Committee (no. 17/LO/0791). Further approval for an amendment to the study protocol was obtained on 1 May 2020 from the London-Surrey Research Ethics Committee.
Author contributions
ADB: conceptualisation, methodology, data curation, formal analysis, writing – original draft, review and editing, project administration, funding acquisition. SA: investigation, data curation. LC: conceptualisation, methodology, formal analysis, writing –review and editing, supervision, project administration, funding acquisition.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the British Orthodontic Society Foundation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The original data used in this study is stored at the University of Kent and is available from the corresponding author (DiBiase AT) upon reasonable request.