
Abstract
Background
Living arrangements play an important role in determining the quality of life (QoL) of people with dementia. Although informal care (home-based) is favored, the transition to formal (institutional) care often becomes necessary, especially in the later stages of dementia. Nevertheless, there is currently no definitive evidence showing that informal or formal care provides a higher QoL for those with dementia.
Objective
To compare the QoL of people with dementia in the nursing home and home care, and identify factors that differentiate their QoL.
Design and methods
This was a cross-sectional survey. A total of 49 people with dementia ≥60 years old were recruited from government nursing homes and hospitals (home care). Consenting participants were assessed on cognitive severity, QoL, activities of daily living (ADLs), depression, and social isolation/connectedness by the Short Mini Mental State Examination (SMMSE), the WHO-8 (the EUROHIS-QOL), Short Assessment of Quality of Life (AQoL-8), Barthel Index (BI), Cornell Scale for Depression (CSDD), and Friendship Scale (FS).
Results
There were significant differences in QoL, HRQoLs, ADLs, and social connectedness among people with dementia in home care (n = 19) and those in nursing homes (n = 30) (p < 0.01). No significant differences were found by socio-demographic factors, cognitive severity, or depression between the study cohorts.
Conclusions
Older adults with dementia who were living at home experienced higher QoL, ADLs, and social connectedness compared with those living in institutional care. Support should be provided enabling home care and empowering caregivers to provide better care for people with dementia.
Introduction
As the population ages, increasing numbers of older adults afflicted with dementia raise various social and economic concerns for both families and the government, particularly regarding care management (Access Economics, 2006; Chan, 2005). According to the Alzheimer Disease International report, the prevalence of dementia in Malaysia in 2005 was 0.063% and the annual incidence rate 0.020% (Access Economics, 2006). This figure is projected to increase to 0.126% and 0.454% in 2020 and 2050, respectively (Access Economics, 2006), which ranked it among the top 10 leading disabling conditions in older adults for low- and middle-income countries (WHO, 2008).
Alarmed by this rapid and projected future growth, attention has been given to the care management of people with dementia, especially in relation to their quality of life (QoL) (Aminzadeh, Dalziel, Molnar, & Garcia, 2009; te Boekhorst, Depla, de Lange, Pot, & Eefsting, 2009). Although a range of services are available—from assisted living facilities, nursing homes, residential care, day care centre, and home care—the literature suggests that the elderly and their caregivers are in favor of staying at home (Iwarsson et al., 2007).
Consistent with the Malaysian culture, care for older adults has been viewed as a religious obligation and the responsibility of the children (MacKenzie, 2006). In Malaysian society, the family has been universally regarded as the main supporter, carer, and home provider for the elderly and particularly those who are unable to look after themselves (Alavi, Sail, Idris, Samah, & Omar, 2011; Aziz & Yusooff, 2012). Therefore, placing relatives with dementia to residential or nursing home care is perceived as abandonment and against these cultural obligations (Bowes & Wilkinson, 2003; MacKenzie, 2006). Care in the community as opposed to institutional care has been a norm in this region.
However, transfer to nursing home and/or residential care becomes unavoidable, especially during the later stage of the illness when caregivers are no longer able to cope with the condition of the dementia patient (Moyle, McAllister, Venturato, & Adams, 2007; Rigaud et al., 2003). In the nursing home, a wide range of facilities and professional care can be provided for the benefit of patients. Nevertheless, there are negative sentiments attached to nursing homes. In a study of public perceptions of nursing homes’ quality it was reported that 52% of respondents assessed their quality as fair or poor (Hogan & Mickus, 2002).
Several studies have reported negative consequences following institutionalization, including depression, increased sense of loneliness, alienation, and a decrease in functional competence (Ball et al., 2000; Scocco, Rapattoni, & Fantoni, 2006), although other studies have reported that QoL may remain the same or even improve depending upon the type of care institution (Gonzalez-Salvador et al., 2000; Missotten et al., 2009; Zimmerman et al., 2005). Therefore, it remains unclear which of the living arrangement options is more beneficial for patients with mild dementia. The aim of this study was to directly compare the experience of self-reported QoL of those with mild dementia who were living at home with those living in institutional care.
Method
Design
This was a cross-sectional study involving people with dementia in home and nursing care. As participants could not be randomly assigned, a quasi-experimental study design was used. Participants were sampled from two different settings: nursing homes (people with dementia residing in government nursing homes) and community home care (people with dementia who live with a carer and get services from the memory clinic in a government hospital). Government nursing homes in Malaysia were built based on a mixture of a home-like environment and hospital model. They provide care, shelter, medical treatment, counseling, rehabilitation, physiotherapy services, prayer facilities, and recreation services to older people to ensure their well-being and QoL. Domestic tasks such as cooking and cleaning are also provided by the nursing home staff.
Participants
Patients aged 60–89 years old who attended a memory clinic or resided in the nursing homes were invited to participate in the study. They were subsequently assessed by the investigator for DSM-IV dementia diagnosis (APA, 2000) and Short Mini Mental State Examination (SMMSE) score. Participants who met the diagnosis criteria, who scored below 11 on the SMMSE, and who provided written informed signed consent were recruited into the study. Those who were unable to communicate in or understand Malay or English were excluded.
Materials
Procedure and measures
Prior to commencing the study, ethics approval was gained conforming to the Helsinki Declaration (World Medical Association, 2004), particularly with regard to informed consent, from The Human Research Ethics Committee of The University of Melbourne, Victoria, Australia, The Social Welfare Department of Malaysia, and The Ministry of Health of Malaysia.
All data were collected through face-to-face interviews, which enabled factors such as timing, language used, fatigue, and sensitivity of the participants to be taken into consideration. Participants were provided with a consent form and participant information sheet which contained a brief description of the study, the objectives of the study, issues of confidentiality, rights to withdraw from the study, and risks and benefits in participating in the study. Consented participants were interviewed in a quiet environment to avoid distractions.
Given the potential issues with participant fatigue, short outcome measures were selected. The questionnaire included socio-demographic information, the Short Mini Mental State Examination (SMMSE) (Braekhus, Laake, & Engedal, 1992), the Cornell Scale for Depression in Dementia (CSDD) (Alexopoulos, Abrams, Young, & Shamoian, 1988), the Barthel Index (BI) (Mahoney & Barthel, 1965), the EUROHIS-QOL (WHO-8) (Power, 2003), the Assessment of Quality of Life (AQoL-8) (Hawthorne, 2009) and the Friendship Scale (FS) (Hawthorne, 2006). Questionnaires were translated into Malay using forward and backward translation with reconciliation by the Malaysian National Institution for Translation. It took an average of 40 min to conduct each interview. Respondents were offered a break during the procedure.
Assessment of cognitive severity
The SMMSE (Braekhus et al., 1992) is a brief cognitive screening tool derived from the original Mental State Examination (Folstein, Folstein, & McHugh, 1975). It consists of 12 items namely, year, month, date, day of the week, country, postal code of address, spell backwards, recall object, repeat sentence, three stage command, write a sentence, and copy design. Each of these items was scored binomially which gave a total score of 12. Giving a sensitivity of 98% and specificity of 91%, a cutoff score of 10 was used to differentiate those with cognitive impairment (Braekhus et al., 1992). The SMMSE was reported to have high validity against the full MMSE with r = 0.95. The Cronbach’s α for SMMSE was 0.71 in this study.
Assessment of QoL
The definition of QoL used in the study was based on the World Health Organization’s definition of QoL; viz., that this involved the individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns. It covers a broad range of concept that affects the person’s physical health, psychological state, level of independence, social relationships, and their relationship to salient features of their environment (WHOQoL Group, 1993). Importantly, this was consistent with Ettema et al.’s (2005) review which reported that the concept of QoL in dementia was defined as the multidimensional evaluation of the person–environment system of the individual in terms of adaptation to the perceived consequences of their dementia. Following review of available measures, the WHO-8 was selected because it assessed the four key areas implicit in these definitions: psychological, physical, social, and environment.
The WHO-8 is a short QoL measure that was derived from the original WHOQOL-100 and the WHOQOL-BREF (Power, 2003; Schmidt, Muhlan, & Power, 2006). It consists of eight items which are representative of two items from each of the psychological, physical, social, and environmental domains of the WHOQOL-BREF (Power, 2003). Each item is rated using a five-point response format from ‘0 = not at all/very poor’ to ‘5 = completely/very good’. Higher overall scores indicate better QoL (Power, 2003). The scale demonstrates good convergent validity with the Mental Health Index (MHI5), general health variable, and social support (OSLO measure) with r = 0.49, 0.53, and 0.36, respectively (Schmidt et al., 2006). The Cronbach’s α values for internal consistency in three centers (UK, Germany, France) was 0.80 (Power, 2003). In this study, the Cronbach’s α was 0.84.
The AQoL-8 (Hawthorne, 2009) is a short HRQoL measure that was derived from the original AQoL. It consists of eight items which are representative of two items from each independent living, social relationship, physical senses, and psychological well-being domains of the AQoL. Each item is rated on four levels of responses from normal health state to a very poor health state. Total scores are presented as utility score on a life–death scale which ranged from −0.04 (worse than death), 0.00 (death) to 1.00 (best HRQoL) (Hawthorne, 2009). The item coefficient scalability of the AQoL-8 was reported to range from 0.22 to 0.44 with Mokken reliability = 0.80. For criterion validity, the AQoL-8 demonstrates good correlation with the original AQoL (r = 0.94–0.95). The Cronbach’s α value for internal consistency in this study was 0.75.
Assessment of depression
The CSDD (Alexopoulos et al., 1988) is an assessment specifically designed to screen depression in a demented elderly population (Alexopoulos et al., 1988; Debruyne et al., 2009). It consists of 19 items concerning physical well-being, sleep, appetite, and other vegetative symptoms (Alexopoulos et al., 1988; Korner et al., 2006). Each of the items are rated as a = unable to evaluate, 0 (absent), 1 (mild or moderate), and 2 (severe). The scores of the individual items are summed and a cutoff of 8 indicates mild depression and 12 for major depression (Alexopoulos et al., 1988). The CSDD demonstrates high correlation with the GDS-30, the HDRS, and the CGI with r = 0.82, 0.91, and 0.82, respectively (Korner et al., 2006). It also has good reliability, with a Cronbach’s α value of 0.73 (in this study).
Assessment of activity of daily living
The Barthel Index (BI, Mahoney & Barthel, 1965) consists of 10 items; feeding, moving from wheelchair to bed and return, getting on and off toilet, bathing self, walking on level surface, ascending and descending stairs, dressing, and controlling bowels and bladder (Mahoney & Barthel, 1965). Each item is scored on a three-point scale, with 0 = totally dependent, 1 = some help needed, and 2 = totally independent (Cohen & Marino, 2000). Items are weighted and summed to give a score range from 0 to 100, with higher scores indicating total independence (Giles, Hawthorne, & Crotty, 2009). In relation to the validity and reliability of the BI, inter-rater reliability was shown to be acceptably correlated with kappa coefficient for each item ranging from 0.27 to 0.68 (Richards et al., 2000). The Cronbach’s α value for internal consistency in this study was 0.83.
Assessment of social isolation
The FS (Hawthorne, 2006) is an instrument which assesses aspects of both perceived social isolation and loneliness. It consists of six items with three of the items covering the feelings of loneliness and the other three items probing the importance of actual social contacts. Responses are categorized into five levels of perceived social isolation (almost always/most of the time/about half the time/occasionally/not at all). A total score is derived from the summation of item responses (items 1, 3, and 6 are reversed prior to scoring). A score of ‘0’ indicates complete social isolation and a score of ‘24’ indicates high social connectedness (Hawthorne, 2006). With regard to concurrent validity, the FS revealed significant correlation with the mental health scores (r = 0.37, p < 0.01) and physical health scores (r = −0.12, p < 0.01) from the SF-12 (Hawthorne, 2006). The FS demonstrated good reliability with Cronbach’s α = 0.80 (in this study).
Data analysis
The data were analyzed with the Statistical Package for the Social Sciences Version 16 (SPSS, 2008). Before analyses, data were screened for missing values and data entry errors. Descriptive statistics and categorical variables are presented as counts, proportions, or percentages. Categorical data were analyzed using χ2 (Chi-square); where distributional assumptions were violated, the Fisher’s exact test was used. The relationship between QoL and other variables were analyzed using non-parametric correlations, and multivariate analysis was used to determine factors that differentiated QoL between the two settings.
Scale score data was assessed and where the data were non-normally distributed, the data were transformed prior to analysis. Analysis of variance (ANOVA) was used to examine known groups and differences are described as Cohen’s effect size (d), where d = 0.20 represents a small effect, d = 0.50 a moderate effect, and d = 0.80 a large effect (Cohen, 1988).
Results
A total of 31 people with dementia from nursing homes and 82 from home care were invited to participate in the study. Of them, 62 agreed to participate but only 49 met the study entry criteria and completed the questionnaire, a participation rate of 44%. Thirty participants were from nursing homes and 19 from home care.
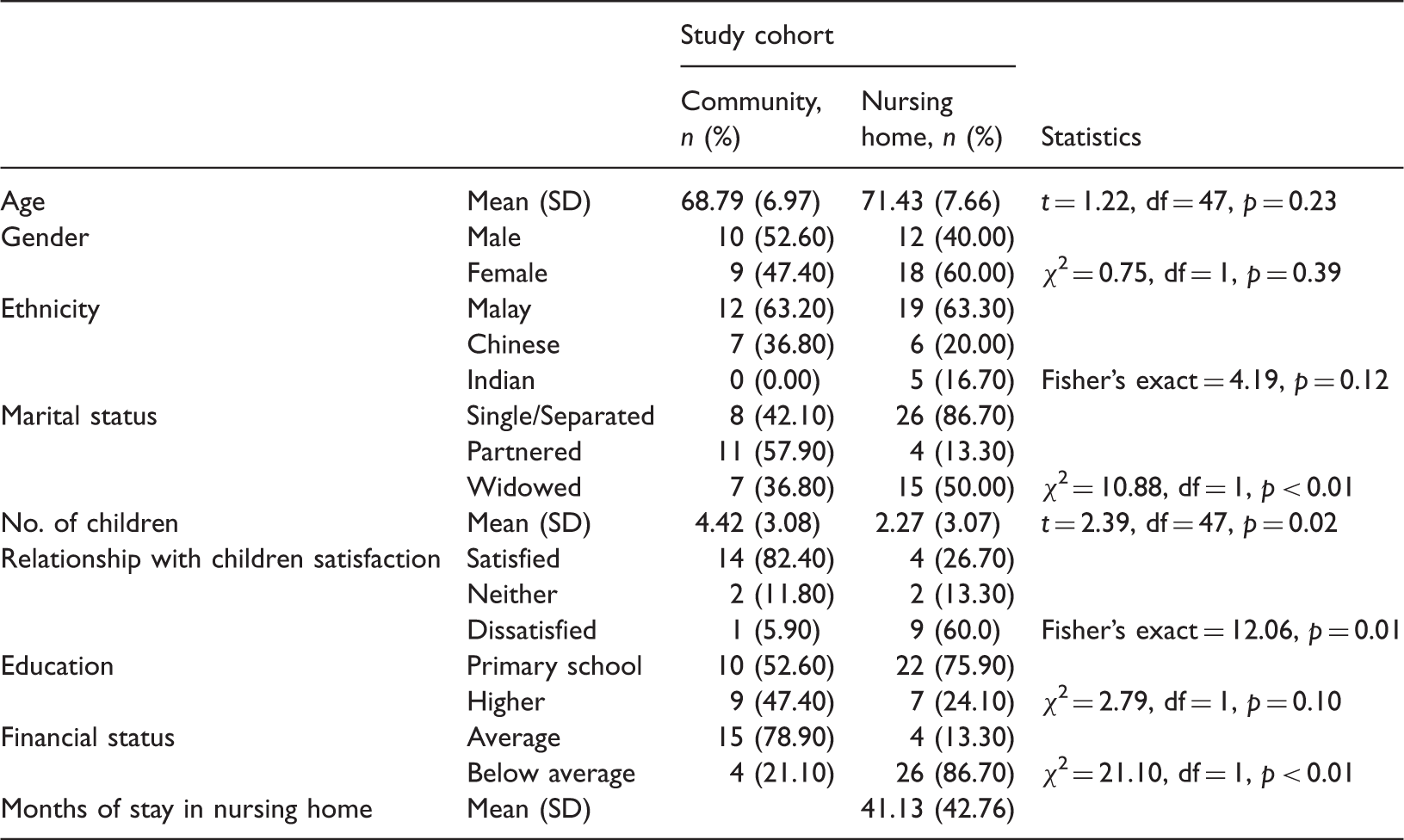
Demographic profiles of people with dementia in home care and nursing homes.
Health status of participants by study cohort.
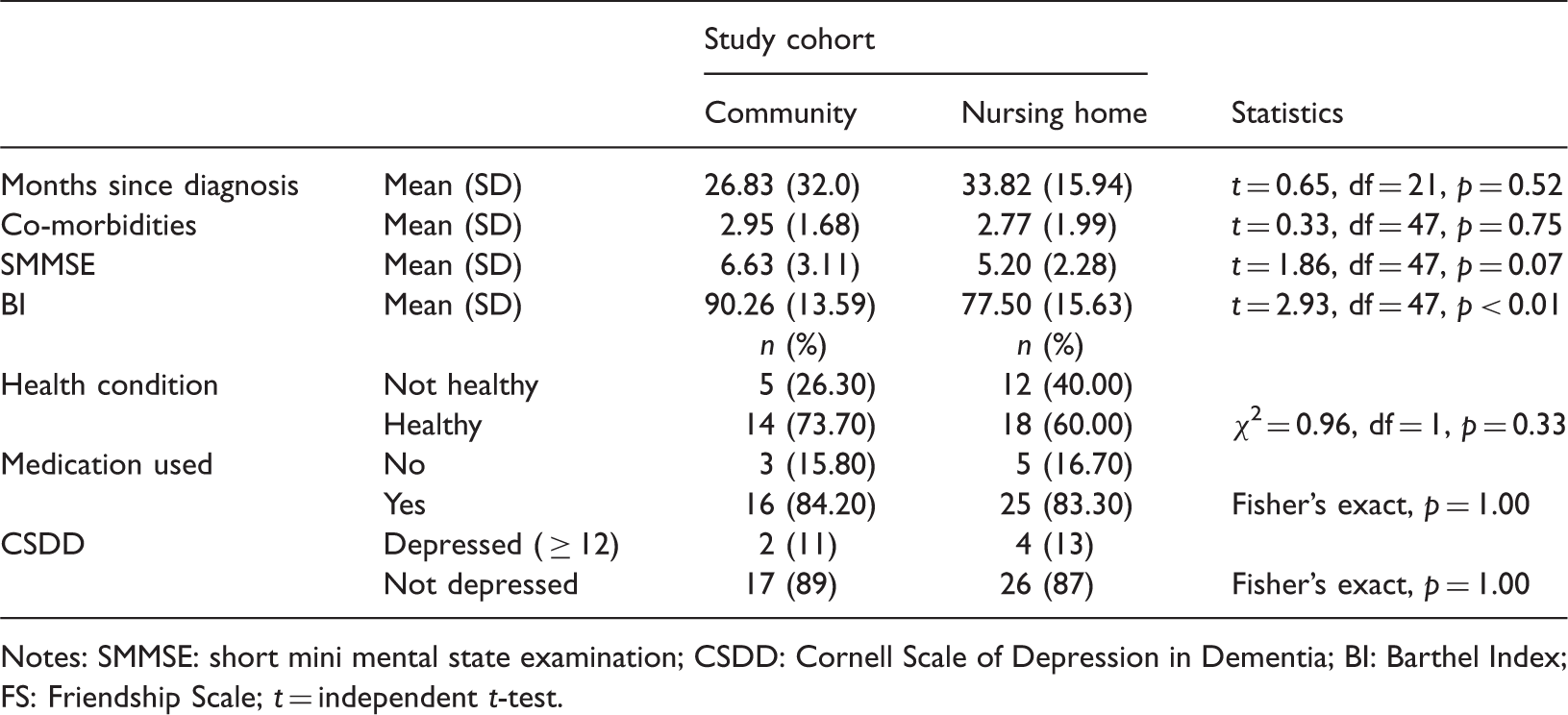
Notes: SMMSE: short mini mental state examination; CSDD: Cornell Scale of Depression in Dementia; BI: Barthel Index; FS: Friendship Scale; t = independent t-test.
Comparing the QoL of people with dementia in the nursing homes and home care, there was a statistically significant difference on both QoL indicators, the WHO-8 and AQoL-8, and for social isolation (the FS). The Spearman correlations between these three outcomes were rsAQoL-8/WHO-8 = 0.42, rsAQoL-8/FS = 0.61, and rsWHO-8/FS = 0.43 (all p < 0.01), suggesting that they were all moderately related to each other (the common variance was between 18 and 37%).
Quality of life by study cohort.
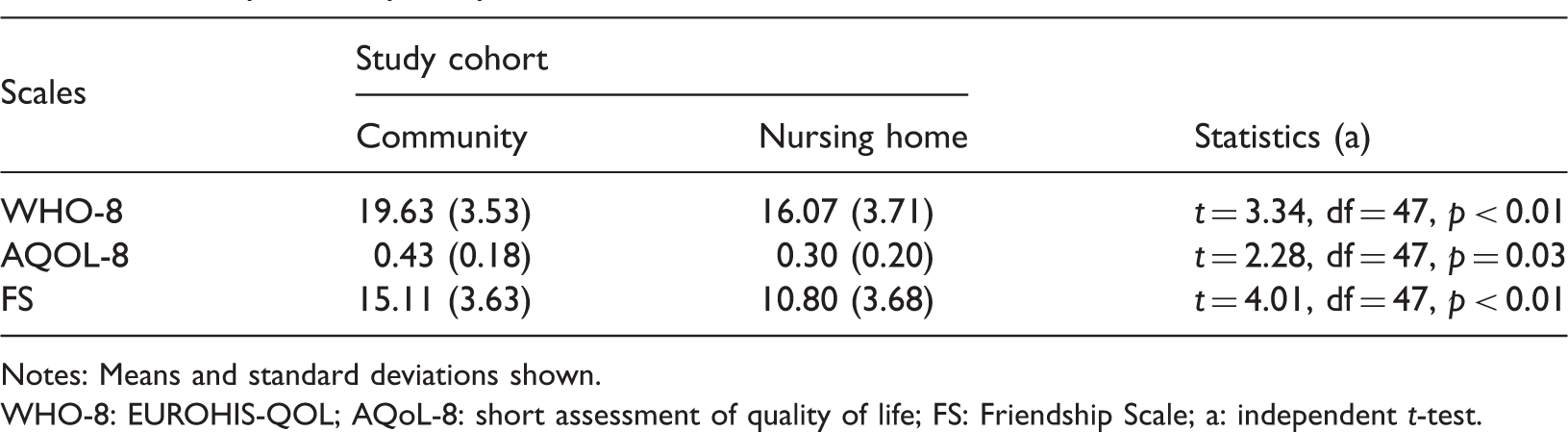
Notes: Means and standard deviations shown.
WHO-8: EUROHIS-QOL; AQoL-8: short assessment of quality of life; FS: Friendship Scale; a: independent t-test.
Discussion
This study compared the QoL of people with mild dementia living in the nursing home with those living in home care, and reported variables associated with overall QoL. Findings demonstrate that people with mild dementia living at home were mostly married, had children, had more satisfactory relationship with their children, and had enough money for their own expenses. However, the key findings for this study were that people with mild dementia living at home were more socially connected, had better physical functions, experienced higher HRQoL, and had better overall QoL.
The findings from this study stand in marked contrast with those previously published. The effect sizes for the two of the three study outcomes measures were large, whilst on the third measure, the AQoL-8, the difference between home and institutional care was double the published minimum important difference for the full AQoL (Hawthorne & Osborne, 2005). Collectively, these three findings favor those living at home suggesting that those living at home enjoyed a higher QoL than those in institutional care. Elsewhere, there are few studies which have directly compared QoL in dementia by home versus institutional care. The findings from these studies are mixed with some studies reporting that the place of residence plays considerable part in QoL (Missotten et al., 2009; te Boekhorst et al., 2009), whereas other studies have reported no significant difference in QoL between people with dementia in institutional care (te Boekhorst et al., 2009).
Precisely why we should have observed such large differences whereas other studies did not is not entirely clear, given that on all (but one) of the health status measures there was no statistically significant difference between the two study cohorts. For example, although other research have suggested that cognitive impairment or depression are predictors of nursing home admission (Kim, Shin, Jeong, Gormley, & Yoon, 2002; Yaffe et al., 2002), we did not find statistically significant differences for cognitive impairment or depression between nursing home and community residents. Differences in age group and measurement scale used in our study might explain the disagreement in our findings (Kim et al., 2002). Although Hamilton Depression Scale has been widely used in reseach, they were not specifically designed for older adults and those with cognitive limitations (Hamilton, 1960).
The finding concerning cognitive impairment is consistent with at least one other study (Kim et al., 2002). This progression argument, however, has important implications for this study’s findings; viz., it might be expected that participants living at home would report better QoL because they were younger (Yaffe et al., 2002) and in the earlier stages of dementia when compared with those living in institutions (Bond & Clark, 2002), although this is not fully supported by the literature (Missotten et al., 2009).
That those living at home had greater autonomy with ADLs was consistent with this expectation, although this may also be due to living in a familiar home and social surroundings (Iwarsson et al., 2007). This finding, however, was consistent with the literature on the characteristics of people with dementia in the institutions; namely, that those who are more dependent in ADLs or with greater physical losses are more likely to be institutionalized (Kim et al., 2002; Luppa et al., 2010; Yaffe et al., 2002), though being physically dependent does not necessarily predict institutionalization among older adults with dementia (Bond & Clark, 2002; Kim et al., 2002). Nonetheless, this result imposed important implication on this study, as it may suggest that people with dementia living at home would report better QoL and social connectedness as they can maintain their independence and social contacts with family members and neighbors.
As the correlations showed, there was an important association between living in a nursing home, social isolation and QoL. Although this has not been widely studied in dementia, there is at least one other report that older people who are lonely are more likely to be admitted to a nursing home, especially those with a high level of loneliness (Russell, Cutrona, de la Mora, & Wallace, 1997). It is also consistent with studies reporting that older people living in nursing homes are more lonely compared to those living in the community (Hawthorne, 2006; Holmen, Ericsson, & Winblad, 2000). This might be due to significant difference in marital status between older adults with dementia in the nursing home and home care. As suggested by other studies, absence of a partner creates insecurity and isolation to the other (Beal, 2006; Glaser, Tomassini, Racioppi, & Stuchbury, 2006; Thomopoulou, Thomopoulou, & Koutsouki, 2010).
There were a number of possible limitations to this study which must be acknowledged. The study was carried out in a naturalistic setting and the findings are subject to the associated limitations. Given the small sample size, the generalizability of findings to the general population is uncertain. The results need to be replicated with a larger sample before fully accepting the study findings. In addition, factors that influence the QoL and loneliness in older adults with mild dementia need to be identified. Similarly, information on type of dementia may be useful in providing better understanding on the QoL of older adults with mild dementia.
In conclusion, the findings indicated that older adults with mild dementia experience a higher QoL and greater social connection living in the community than in the nursing home. These findings may suggest health care plans promoting community care for people with dementia supported by initiatives to reduce the burden of the caregivers. Additionally, suitable rehabilitation programmes could be introduced for older adults in institutions in enhancing their physical, mental, and social well-being.
Ethical approval
Study procedures were approved by the University of Melbourne Human Ethics Committee and the Ministry of Health Research and Ethics Committee of Malaysia.
Footnotes
Acknowledgements
This study was funded by a grant from the Research Management Institute of Universiti Teknologi MARA, Malaysia, and was supported by The University of Melbourne. The Ministry of Higher Education of Malaysia sponsored this study. We thank the anonymous reviewers for their contributions to improving the manuscript.