
Abstract
Social integration has a significant influence on physical and mental health. Older adults experience an increased risk of social isolation as their social networks contract. The purpose of this study is to examine associations between dementia special care unit residents’ overall well-being and cognition with structural aspects of their coresident relationships.
Design and Methods
Measures of social network structure were calculated from self-reported social contact data within three cohorts of residents in one dementia special care unit. Pearson correlations were used to describe associations between overall quality of life and cognition, with network characteristics indicative of social integration.
Results
Approximately half the ties sent or received were reciprocated and positive associations were found between social integration and quality of life. However, inconsistent associations were found between social integration and cognitive function. Friendship ties were more frequent between people of adjacent cognitive status categories. In addition, comparing across personal networks, residents tended to be tied to residents of higher quality of life status (43.3%, n = 13 personal networks) as opposed to lower (30%, n = 9 networks) or same (26.7%, n = 8 networks). There is a strong positive correlation between quality of life and respondent’s betweenness centrality, suggesting that individuals with high quality of life tend to be important intermediaries between others in the community.
Implications
Among the “oldest old,” quality of life and cognitive function are unevenly distributed, yet these health indicators tend to cluster in social networks. This reinforces that while quality of life may be highly individual, it is in part linked to relationships with others.
Keywords
Introduction
Maintaining social ties in the face of chronic illness or disability is challenging. Studies have shown a decline in the amount of social connectedness among older adults due to factors such as retirement, death of same aged peers, and functional health declines (Cornwell & Waite, 2009). Indeed, examination of the “oldest old” in American society reveals individuals with smaller social networks and less closeness with others (Cornwell, Laumann, & Schumm, 2008). Social integration and social support can directly impact our physical and mental health (Berkman, Glass, Brissette, & Seeman, 2000; Satariano, 2006; Smith & Christakis, 2008). For example, stress pathways can be affected by social relationships. A recent longitudinal network study of hypertension among older adults showed that increased social connections prospectively reduced the risk of hypertension, and perceptions of social support lowered systolic blood pressure (Yang, Boen, & Mullan, 2015). In addition, a meta-analysis found that greater social integration increased the likelihood of survival among older adults by 91% (Holt-Lunstad, Smith, & Layton, 2010). This equals a mortality risk associated with social isolation that is greater than that of such well-known lifestyle factors as smoking, obesity, and lack of physical exercise. However, the role of social integration as a risk factor for poor health among older adults has not received as much attention as these more widely publicized lifestyle behaviors.
With advancing age comes greater risk of developing cognitive impairment, and currently one in nine older Americans has Alzheimer’s Disease with 36 million people worldwide living with dementia (Alzheimer’s Association, 2014; World Alzheimer Report, 2014). Due to the progressive nature of the disease, informal or formal care is often needed (Nordberg, von Strauss, Kåreholt, Johansson, & Wimo, 2005) often precipitating a move to residential care (Mitchell & Kemp, 2000). Twenty percent of United States nursing homes report having a dementia special care unit (D-SCU) (Wimo & Prince, 2010). D-SCUs have developed to address the unique care needs of individuals with cognitive impairment and provide a separate secured physical space for residents. These units typically offer specialized programming and activities for residents to enhance social integration. In addition, D-SCUs have lower staff-to-resident ratios and a general orientation toward reducing the environmental and functional stressors residents’ experience leading to enhanced resident’s perception of their quality of life (QOL) (Gruneir, Lapane, Miller, & Mor, 2008; Holmes et al., 1990).
QOL is a broad multidimensional construct that can be affected by not only resident level characteristics, such as cognitive status, but by facility level characteristics (Abrahamson et al., 2013). Previous studies report that cognitively impaired nursing home residents are reliable informants of their QOL (Brod, Steward, Sands, & Walton, 1999; Kane et al., 2003; Logsdon, Gibbons, McCurry, & Teri, 2002; Maslow & Heck, 2005; Moszley et al., 1999). In fact, the voice of the older adult receiving long-term services and supports is considered crucial to the larger conceptual framework of health-related QOL (Zubritsky, Abbott, Hirschman, Bowles, & Naylor, 2012). Therefore, in order to develop interventions that can improve the social connections for this highly vulnerable and fast-growing population, adults’ perceptions of their QOL should be contextualized with reliable and valid measures of their social interactions. Doing so can provide a way to assess how relationships shape the health and QOL of residents in special care units.
Relationship measurement becomes especially complex with older adults in residential care because of the unique characteristics of their environment, which includes other residents and formal care workers. Social network analysis (SNA) has emerged as a powerful approach to measuring social integration. SNA makes use of data that are collected among connected individuals and is able to address the relationship between social integration and health by considering where individuals are situated in their social network. A whole-network approach to enumeration uses relational data to identify all ties containing specified relations in a defined population (Wasserman & Faust, 1994). While the transition to residential care makes it more difficult to maintain existing community ties, the special care setting presents opportunities to form new social ties as other residents and formal care providers become central to daily life. In general, measures of social network characteristics (e.g. network size, quality, centrality, and isolation) have been linked to a variety of mental and physical health outcomes across the life course, including mortality risk, happiness, obesity, and loneliness (Cacioppo, Fowler, & Christakis, 2009; Christakis & Fowler, 2007; Fowler & Christakis, 2008; Holt-Lunstad et al., 2010; Pantell et al., 2013). However, there is relatively little network research to scrutinize relationships of the “oldest old” in institutionalized settings, and so our knowledge of the structure of social connections for cognitively impaired older adults residing in settings such as the D-SCU is limited.
An ethnography of individuals with dementia residing in long-term care found that they created “nested social groups,” small clusters of friendships within their larger social environment (Doyle, de Mederios, & Saunders, 2012). In addition, the authors found that the physical environment could impede or enhance resident movement and potential socialization opportunities and that staff decisions used to maximize task efficiency created impediments to socialization between residents. Additional studies underscore how the design of the physical environment and opportunities to engage with other D-SCU residents facilitated social interactions (Diaz Moore, 1999). Fewer agitated behaviors were observed among cognitively impaired residents who had more frequent social visits by individuals living outside of the D-SCU (Cohen-Mansfield & Marx, 1992; Kutner, Brown, Stavisky, Clark, & Green, 2000). Despite this growing body of literature on social interactions, research measuring the social network characteristics of elderly individuals in residential care environments remains limited. While whole-network studies are often conducted among individuals in closed network populations such as students at schools (Lewis, Kaufman, Gonzales, Wimmer, & Christakis, 2008; Pachucki, Ozer, Barrat, & Cattuto, 2015), this approach has not yet been pursued in depth in the dementia special care environment.
The goals for the present study are to examine associations between elderly residents’ overall well-being and cognition with aspects of their coresident relationships, and to report on the viability of using network enumeration as a useful way to document the social environment of institutionalized older adults. Using the whole-network approach allows us to identify opportunities and constraints based upon a resident’s location within the D-SCU. This location is hypothesized to be predictive of resident outcomes (Borgatti, Everett, & Johnson, 2013) such as QOL, depression, or behavior. In tandem, scrutinizing residents’ personal networks within the bounded social group and comparing them to one another can provide complementary insights into individuals’ varying social contexts. The aims of this study are as follows: (1) to describe the stability of friendship networks among residents of the D-SCU to inform larger and more representative studies; (2) to describe D-SCU residents’ network characteristics; (3) to explore preliminary associations between network characteristics, cognitive function, and QOL. We ask two key questions: (a) Does cognitive function cluster in social networks? (b) Is greater social integration associated with higher reported QOL? We hypothesized that both cognitive function and QOL would cluster in one’s community.
Methods
Setting
This study was conducted in a D-SCU of a 501(c)(3) not-for-profit long-term care (LTC) organization providing a continuum of aging services in the Eastern United States. The data for this study were collected as a component of a parent study designed to develop methodological approaches to capturing social network data among older adults living in assisted living and D-SCUs (Abbott, Bettger, Hampton, & Kohler, 2012, 2013). This specialty unit was selected by the researchers to test the feasibility of measuring social networks among individuals with cognitive impairment. The original goal of the study was to be able to conduct longitudinal analysis across three years. However, due to resident mortality and relocation we ended up with only three individuals who were present across all three time points. We therefore felt it was more appropriate to use a cross-sectional approach and to refer to each wave as a Cohort (wave 1 = Cohort A and so on). We discuss this further in the statistical analysis section of the paper. Family members of 8% of residents in Cohort A, 20% in Cohort B, and 15% in Cohort C declined their relative’s participation in the study. The University of Pennsylvania Office of Regulatory Affairs reviewed and approved this study, and the administration of the LTC organization was intimately involved with each step of planning and implementation.
Sample recruitment
There were no age, physical, or mental health exclusion criteria, and all residents in the D-SCU were English speakers. The social worker in D-SCU assessed the cognitive status of all eligible residents three weeks prior to data collection via the Mini Mental State Examination (MMSE). The MMSE was used to obtain an estimate of cognitive function (Crum, Anthony, Bassett, & Folstein, 1993). This instrument asks questions related to time orientation, place orientation, attention, recall, language, repetition, and registration and is known to be associated with age-related cognitive impairments such as dementia. The continuous MMSE scale ranges from 0 to 30. A member of the LTC organization contacted legally authorized representatives (LAR) of individuals with MMSE scores of 22 or lower to explain the study and request consent for the resident to participate in the study. Upon receiving LAR consent we approached each resident for their assent. Residents with MMSE scores of 23 or higher who were interested completed informed consent documents without their LAR being contacted. Additional recruitment details are described in detail elsewhere (Abbott et al., 2012, 2013).
Data collection
Data collection about resident social interactions was collected via face-to-face interviews with participating residents in March 2011, March 2012, and March 2013. Between the last two observations the D-SCU added four rooms to the unit, increasing the number of residents from 12 to 16. Organization support was crucial to the success of this study and amounted to approximately 20 h of support from D-SCU staff. Staff assisted by obtaining informed consent, MMSE scores, and taking photos. Study funds were provided to the D-SCU for its participation. The interview guide was developed using previously tested items and approaches used by the investigative team (Abbott, Stoller, & Rose, 2007; Hampton, 2011; Abbott, Prvu Bettger, Hanlon & Hirschman, 2012; Hampton & Wellman, 2003; Helleringer, Kohler, Chimbiri, Chatonda, Mkandawire, 2009). Residents in the D-SCU completed one 30 min interview that addressed demographics, QOL, health status, and friendship networks.
Measures
Our primary outcome measures are cognitive function (MMSE) and a QOL measure. To ascertain network clustering of cognitive function, continuous MMSE scores were classified into a categorical variable according to common boundaries into high function/cognitively capable (MMSE: 23–30), mild impairment (19–22), moderate impairment (10–18), and severe impairment (0–9) (Mungas, 1991). The QOL measure was derived from a Likert-scale question asking residents (“How would you rate your quality of life overall?”) with response options ranging from Poor/Bad (1) to Excellent (5), with “don’t know/refused/doesn’t understand” listed as missing (Stewart & Ware, 1992).
The social network component of the interview asked residents to look at pictures of other residents and to answer five questions regarding who they spent time with, listened to problems, helped with something, who helped them, and who listened to them. Nominations were limited to five people to prevent respondent fatigue. Photographs were used to aid with the data collection process due to difficulties with recall among individuals with cognitive impairment.
This information on social relationships allows us to describe aspects of the social structure of one D-SCU community with snapshots taken during three consecutive years. A first set of network covariates is concerned with residents’ personal network size. Indegree refers to the number of friendship ties a resident (e.g. ego) receives from others in the community (e.g. alters), while outdegree refers to the number of ties a resident sends to others. Personal network size (unique persons within the set of receiving and sending ties) is an attribute typically used to proxy the availability of social support. Last, for each resident we counted how many social ties were reciprocated in their personal network; a mutually recognized relationship can be more meaningful than a relationship perceived by only one person.
Another set of network covariates concerns measures of residents’ relative centrality within the structure of the group (Borgatti et al., 2013). We include two different measures of centrality reflective of our hypotheses. First, we are interested in betweenness centrality, which is the extent to which an individual mediates other connected individuals. A resident with high betweenness centrality is positioned between many other residents and because of her structural location has the potential to control what flows through the network. Closeness centrality tells us how close an individual is to all others in their network. This is of interest in terms of social integration as individuals with high closeness centrality would be seen as being well integrated.
A measure of whole-network density allows us to characterize the integration of the entire network (in this case the residents of the D-SCU) and compare it across the three cohorts. Data on social relationships were then matched to information on each resident’s health attributes. By assessing the mean MMSE or QOL across the uniquely connected alters of each resident, we produced two measures of average peer MMSE and average peer QOL. Together, these network measures provide insight into different levels of social integration and help us to describe characteristics of relationships in each of the three D-SCU cohorts.
Statistical analyses
The first set of analyses measure associations between resident cognition and different aspects of self-reported friendships using Pearson correlations. The second set of analyses calculates associations between self-reported overall QOL and friendship ties. We note that due to high replacement each period owing to both mortality, and moving from the D-SCU to the traditional nursing home, we conservatively decided to consider these cohorts as discrete (i.e. cross-sectional) with a small amount of continuity rather than as a longitudinal study. For instance, while the first two periods have 10-person cohorts, only 60% (n = 6) of T1 individuals are present at T2, with four individuals joining and four leaving. From T2 (n = 10) to T3 (n = 17), only 35% (n = 6) of T2 individuals are present at T3, with 11 new persons joining and six leaving. Only three individuals are present at all three periods. From this point forward, we therefore describe residents as belonging to Cohort A (T1), B (T2), or C (T3).
Results
Descriptive statistics
Cohort description.
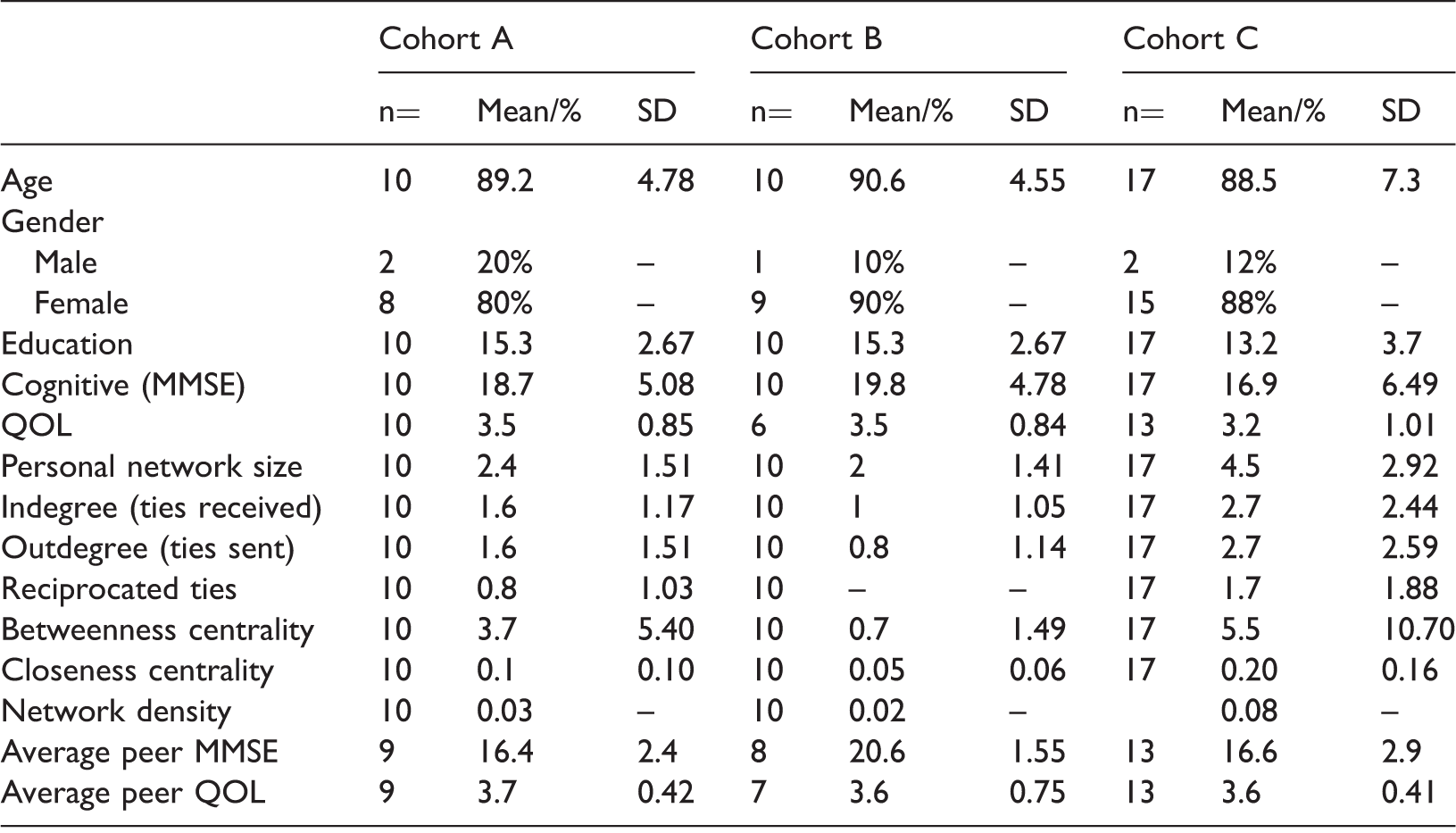
MMSE: Mini Mental State Examination; QOL: quality of life.
We choose to focus on a small number of basic aspects of residents’ networks: network size (number of socially connected residents), frequencies of nominations to others, nominations from others, reciprocated nominations, two measures of centrality (betweenness and closeness), and density. Average personal network size is smallest in Cohort B (µ = 2 unique ties to others) and highest in Cohort C (µ = 4.5 ties). This roughly comports with connectedness of slightly younger (i.e. 75–85 y.o.), albeit noninstitutionalized adults in a nationally representative American sample (Cornwell, Laumann, Schumm, & Graber, 2009). Approximately half the ties sent or received are reciprocated. On average, individuals’ MMSE is higher than peers in Cohorts A and C and lower than peers in Cohort B. Individuals’ QOL tends to be lower than connected peers across all three cohorts.
These statistics are usefully complemented with network graphs that visualize friendship ties between all residents across the three cohorts. In Figure 1, node size indicates QOL, and node color indicates cognitive impairment status (high, mild impairment, moderate, severe). There is an observable amount of clustering by cognitive function in Cohorts A and B. In Cohort A, moderately impaired individuals tend to affiliate the most, while in Cohort B affiliation is more frequent between mildly impaired individuals. Of the several socially isolated individuals observed across the three cohorts, there is no discernible pattern in terms of their cognitive impairment. However, isolated individuals have a tendency toward lower than average or missing QOL.
Friendship ties and cognitive function (Cohort A, B, C). Note: Black (cognitively capable), Dark gray (mild), Light gray (moderate), White (severe). Node size is proportional to overall quality of life. QOL missing in Cohort B (V4, V5, V8, V9, V11), Cohort C (V8, V11, V12, V22).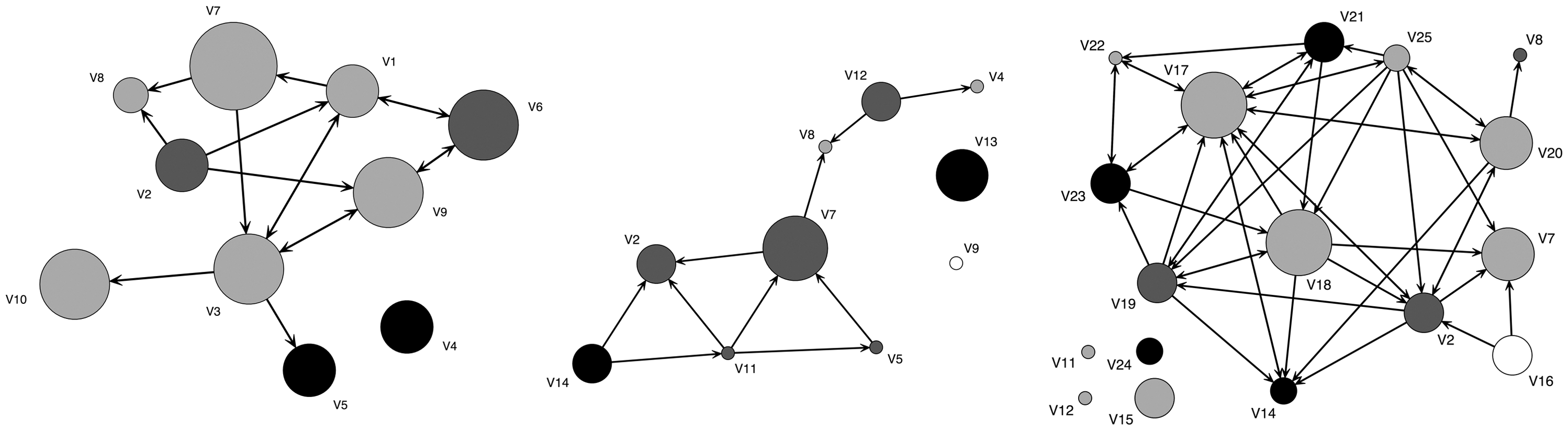
Cognitive function
Correlations between cognitive function and network attributes.
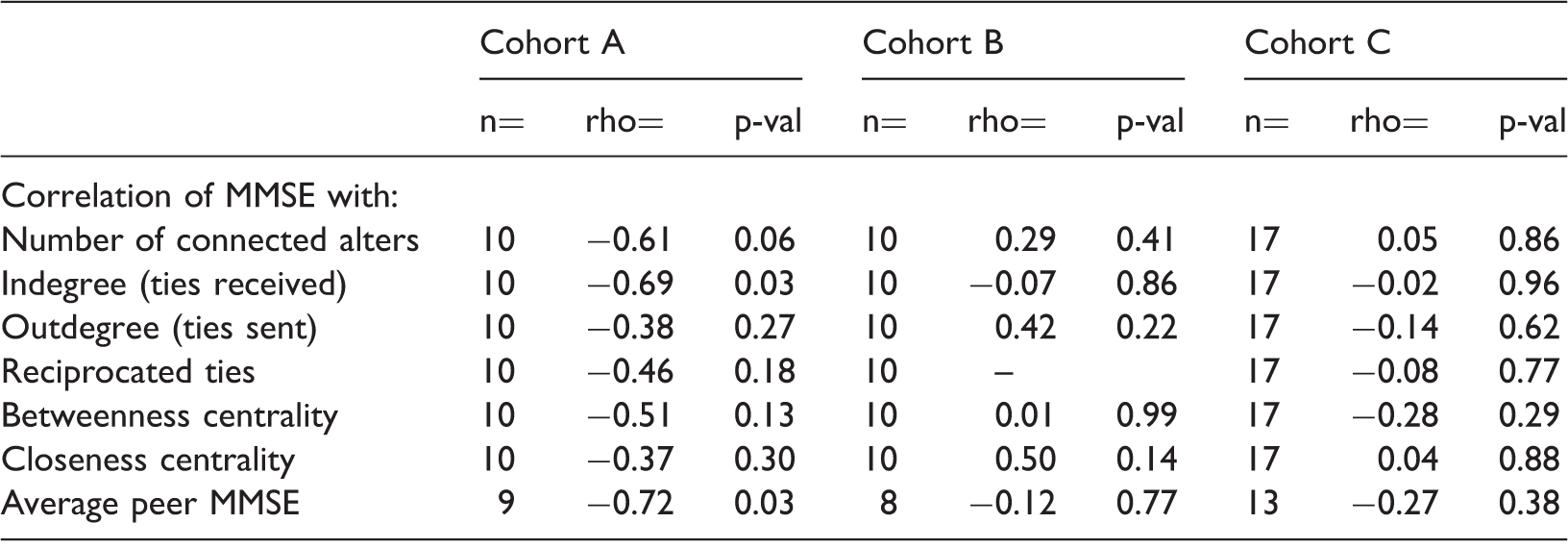
MMSE: Mini Mental State Examination.
Note: No reciprocated ties in Cohort B.
Inspection of personal networks is also revealing (see Figure 2). In Cohort A there were nine residents with at least one alter; in Cohort B there were eight; in Cohort C there were 13 residents. Visual inspection of the personal networks in Figure 2 reveals a great deal of variation in terms of network size, as well as the extent to which a resident’s alters are connected to one another. Comparing across personal networks, residents tended to be tied to residents of higher QOL status (43.3%, n = 13 personal networks) as opposed to lower (30%, n = 9 networks) or same (26.7%, n = 8 networks). Ties are more frequent between people of adjacent cognitive status categories. For instance, there are relatively numerous ties between people of moderate impairment and mild impairment, and between no impairment and mild impairment. In contrast, there are no ties between highly impaired and unimpaired residents.
Egocentric networks, quality of life, and cognitive function of D-SCU residents. Note: Black (unimpaired cognitive function), Dark gray (mild), Light gray (moderate), White (severe). Node size is proportional to overall quality of life. Some QOL missing (e.g. id #2, Cohort B, V11).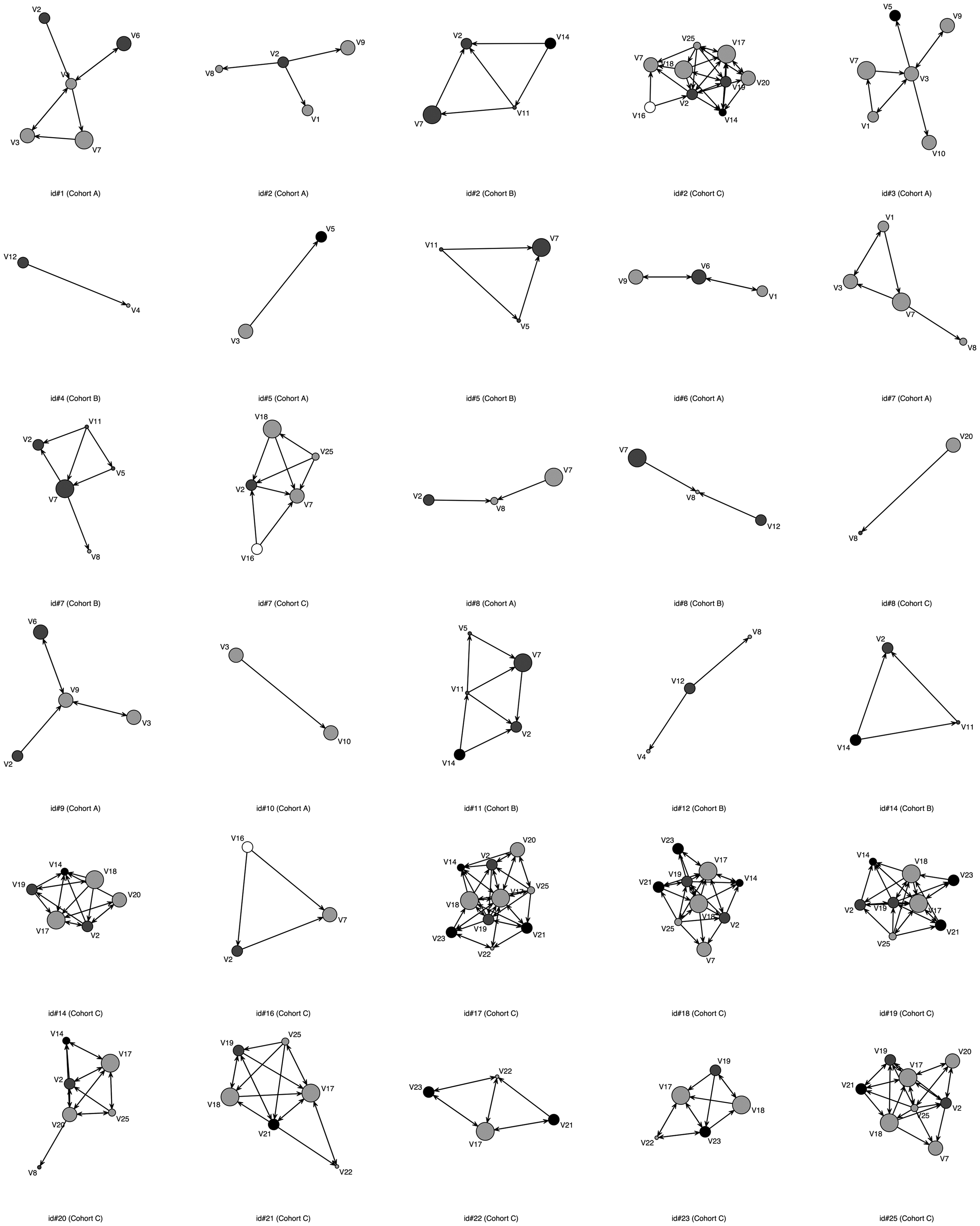
QOL
Correlations between quality of life and network attributes.
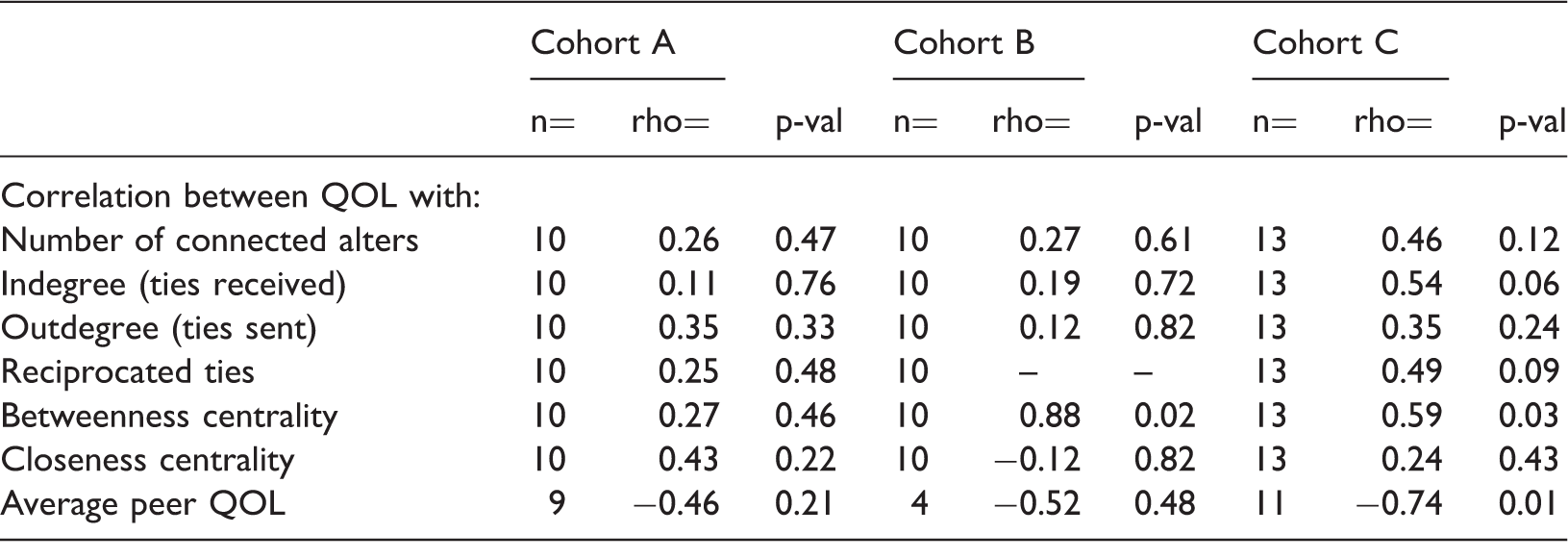
QOL: quality of life.
Note: No reciprocated ties in Cohort B.
Discussion
Overall, this study illustrates the feasibility and utility of examining social structural correlates of cognitive function in a network setting. Using a whole-network approach to enumerate ties within a community offers a hyper-dyadic view of the patterns of relationships not observable to any one resident herself. Comparison across personal networks illustrates the value of examining each individual’s relationship context and may help staff to identify appropriate targets for reinforcement of social support. With the exception of Cohort B, the overall pattern observed across cohorts was a trend toward higher functioning and lower functioning individuals having smaller networks and being relatively peripheral in the D-SCU network. This is consistent with a situation wherein high-functioning individuals may not feel comfortable socializing—or may be unable to socialize with—lower functioning coresidents. It bears recalling the unstable and transient nature of a D-SCU environment. No doubt residents are aware of people entering, and then temporarily or permanently leaving their environment. Some individuals may feel resentful of being residents in this setting, and others may behave in a manner that disrupts pro-social interaction or be unable to initiate a conversation. These dynamics and others may contribute to a lack of interest/ability for socialization and raises questions about the benefits of segregating individuals by cognitive status.
While friendships made in residential care are qualitatively different than friendships made in younger years (Sefcik & Abbott, 2014) they remain important to resident health and QOL. Studies involving relationships in residential care are crucial to understanding the impact of segregating individuals with cognitive impairment from cognitively capable individuals. Special care units are being developed and marketed without the evidence to support claims of better care, outcomes, or social integration (Gruneir et al., 2008; Phillips et al., 1997). One study found that segregating cognitively impaired residents with no additional programming led to poor outcomes for individuals with dementia (Van Haitsma, Lawton, & Kleban, 2000) One could argue that all nursing home residents could benefit from lower staff-to-resident ratios, tailored programming, and smaller units.
The finding that residents largely appear to have higher MMSE than their peers suggests that they may be limited in their ability to interact with individuals with similar functional status, which may lead to boredom contributing to behavioral and psychological symptoms of dementia (BPSD). Over the course of the illness, BPSD can affect 90% of all persons with dementia and is associated with poor outcomes and increased health care costs (Cerejeira, Lagarto, & Mukaetova-Ladinska, 2012). Given the emerging research on neuroplasticity and cognitive reserve, persons with dementia are able to learn new things (Vance & Crowe, 2006). Therefore, active steps should be taken to avoid speeding up cognitive decline through segregation.
We found inconsistent results related to QOL and relationship attributes. While this requires further study, these findings suggest that QOL may be linked to relationships with others. During two of the three years of D-SCU observation, a key measure of social integration—betweenness centrality—was associated with increased QOL. This may indicate that individuals with high QOL serve a function as intermediaries, or brokers, between other D-SCU residents. It is conceivable that interventions could be designed to target these individuals to assist in improving the social connectedness of D-SCU communities. Egocentric analysis of friendship networks revealed a lack of ties between unimpaired residents and those with high levels of cognitive impairment. This suggests that interventions that seek to improve connectivity of residents may be most successful in encouraging relationships between those of similar or neighboring cognitive status.
This study lays the groundwork for improving the measurement and, therefore, the understanding of social networks among older adults who live in D-SCU and traditional nursing homes. Studies comparing resident outcomes between traditional nursing homes and D-SCU do not exist due to the difficulties of randomizing individuals to residential care settings. Network approaches equipped to examine bidirectional associations of health in the relational social environment may provide a useful way to compare settings.
Limitations and next steps
While the small size of this study is a limitation, most D-SCUs are of similar sizes. Thus, future directions include replicating this study at different facilities and scaling up the sample size by including multiple providers. While the majority of long-term care residents nationwide are female, it would be important to explore how the dynamics might be different among a cohort with different gender, racial, and ethnic compositions. In addition, our reliance on self-report from individuals with MMSE scores below 17 is not necessarily as problematic as we anticipated. While we typically would question the reliability of a resident with moderate-to-severe dementia, we had a resident with an MMSE of 11 who had both of her nominations reciprocated. We recommend that future studies combine third-party observations of social interactions among residents and compare findings with residents’ self-reported relationships in order to validate how perceived friendships of D-SCU residents overlap with who residents actually affiliate with.
Current shifts in the long-term care industry make longitudinal studies challenging. Between years two and three of data collection the facility expanded by four rooms. However, the increase in new residents occurred five months prior to the final wave of data collection and our results show they were able to nominate and be nominated by friends in this short time period. As is common in many social network studies, we limited the number of friendship nominations to five (Marin & Hampton, 2007). While this procedure may limit the scope of an individual’s social network, it decreases respondent burden. With respondent burden in mind, we chose to use a limited QOL measure that we acknowledge is not a robust indicator. Future studies can include QOL measures specifically developed for people with dementia (Logsdon et al., 2002).
Over the three years of the study, family members of 17% of residents declined to allow their relative to participate. This is a low refusal rate and is reflective of the partnerships developed among the researchers, staff, residents, and family members. Each year the first author would present preliminary findings to the executive committee, the direct care staff, and families. These dissemination efforts assisted in building trusting relationships that continue to develop into new projects and are recommended for future studies. Refusals lead to limitations in what can be inferred from partial, as opposed to complete, whole network data, and additional work remains to understand the ramifications of selection bias (Borgatti, Carley, & Krackhardt, 2006; Kossinets, 2006). While partial data can be obtained if individuals who decline are nominated by others, there are a host of ethical and privacy considerations to such proxy inclusion (Breiger, 2005).
This study describes friendship relations between residents, and we are not able to comment on the meanings or content of ties, information that could enhance our understanding of the cultural context of networks considerably (Pachucki & Breiger, 2010). Additional relationship information between staff and residents, and between visitors and residents would enrich the network perspective offered here. As a cross-sectional study, these data do not allow us to make inferences about whether network structure is responsible for shaping health status or the reverse. People may select friends with similar health attributes to begin with, which can generate within-network associations, and a person might reasonably be influenced by the behaviors of the people she is surrounded by. A major recommendation for future research is to perform assessments either quarterly or biannually in order to account for health and network instability among this population.
Conclusions
This study shows the feasibility of incorporating network measures into larger longitudinal studies by providing guidance for examining social relationships, social integration, QOL, and health in residential long-term care. Ultimately, we believe that a focus on individuals’ relationships allows us to better identify residents for network-informed dyadic or small-group health intervention. This study joins others in showing that health and well-being is unevenly distributed in social networks. Understanding residents’ relational social contexts gives practitioners a lever to improve health in a manner that goes beyond simply assessing the patient as an individual.
Footnotes
Acknowledgements
The authors wish to thank the older adults who participated in this study as well as the employees from the facility who provided guidance throughout the study period.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Francis E. Parker Foundation and the University of Pennsylvania School Of Nursing.