
Abstract
For people living with dementia and their care partners, a decline in the ability to effectively communicate can cause significant distress. However, in recent decades, the arts have emerged as an effective care modality in fostering communication and expression for those with declining verbal skills and memory loss. Opening Minds through Art (OMA) is a national initiative that empowers people living with dementia by facilitating creative expression and social engagement through art-making in partnership with trained college student volunteers. Research has demonstrated that participation in the program benefits quality of life for those living with dementia and also improves student attitudes toward dementia. To date, however, no research has involved primary care partners. We implemented an OMA program at three residential care homes in State College, Pennsylvania, with residents cocreating artwork alongside primary care partners (i.e., a family member or primary medical personnel) over the course of four art-making sessions. We evaluated the effects of participation on quality of life and care partner burnout through pre–post use of “emotional thermometers” (measuring levels of distress, anxiety, depression, anger, and perceived quality of life), the National Institute of Health NIH emotional support scale, and the NIH caregiver assessment (care partner burnout). For people living with dementia, participation significantly increased perceived quality of life while decreasing distress, anxiety, depression, and anger (p < .01; n = 12) after each class; however, the intervention did not significantly impact perceived emotional support. For care partners, participation significantly lowered post-intervention measures of burnout and self-rated stress (p < .01; n = 9). This preliminary study suggests that a structured art-based activity appears to positively impact acute mood for patients and, importantly, decrease care partner burnout. Future research can bring more robust methods to bear in determining how to use OMA and other arts interventions to optimize social support for people living with dementia and their care partners.
Keywords
Introduction
According to the World Health Organization, an estimated 47 million people worldwide are currently living with dementia, a collective term for a number of progressive brain syndromes that impact memory, thinking, behavior, and emotion, gradually making daily activities a challenge for those affected (WHO, 2018). As dementia progresses, a person’s ability to effectively engage with their environment can become increasingly difficult. Later stages of illness are characterized by a lack of ability to communicate through logical verbal channels (Lokon et al., 2016). Despite this loss of capacity, a need to communicate and express oneself remains present in those affected—a dynamic that can cause significant frustration for both patients and their care partners (Takai et al., 2009). For this reason, as well as the reality that pharmaceutical approaches have failed to modify disease progression or effectively treat symptoms, interventions aimed at improving quality of life for persons with dementia and their care partners are greatly needed (de Medeiros & Basting, 2014).
In recent decades, there has been emerging evidence that non-pharmacologic approaches, and specifically arts-based therapies, are particularly impactful for people living with dementia (Cohen, 2006; Fox et al., 2014; Kinney & Rentz, 2005; Rentz, 2002; Rusted et al., 2006; Windle et al., 2014; Zelig et al., 2014). Thus far, research examining the impact of arts-based approaches has shown that their main value is providing a means of nonverbal communication (Beard, 2012; Odell-Miller et al., 2006) while promoting psychological well-being and affirming individuals’ sense of self-worth through imaginative, failure-free activities (Basting, 2020; Chancellor et al., 2014; Deshmukh et al., 2018; Windle et al., 2014). Due to these established psychosocial benefits, there has been a push to create standardized, reproducible interventions aimed at improving quality of life for elders living in residential care settings by training volunteers to programmatically assist patients in artistic creation.
One such standardized intervention to emerge in recent years, Opening Minds through Art (OMA), founded by Dr Elizabeth Lokon in 2007, certifies college student volunteers with training in the basics of dementia and person-centered communication skills and then pairs them with people living with dementia to facilitate creation of expressive artwork across multiple 60-min sessions (college students assist in manual dexterity tasks and give active encouragement). Prior research on OMA has shown that the program momentarily increases patient engagement, social interest, and pleasure (Sauer et al., 2016). Additionally, studies have demonstrated that participation in OMA can improve volunteer understanding and attitudes toward people living with dementia (Lokon et al., 2012, 2018).
To date, no research on the OMA program has involved familial or institutional care partners. This is particularly of interest as studies have demonstrated that creative programs can offer care partners an opportunity to participate in a meaningful interaction outside of regular caring routines, leading to improved care partner–patient interactions (Broome et al., 2017; Duignan et al., 2009; George & Houser, 2014), the positive effects of which have been shown to persist even beyond the creative session itself (Hsu et al., 2015).
Beyond relational dynamics, there is a need for interventions to focus on the health of care partners themselves. Caregiving specifically for persons with dementia is a risk factor for psychological stress and physical ill-health (Gilhooly et al., 2016), with more than 80% of dementia care partners frequently experiencing high levels of stress, and almost half reporting depression (Etters et al., 2008). Approximately half of dementia care partners report frank symptoms of burnout, which corresponds to lower quality of life (Takai et al., 2009). Burnout is experienced for both formal care partners (i.e., nursing staff) and informal care partners (i.e., family members, friends, or neighbors) (Alves et al., 2019).
Several arts-based interventions involving people living with dementia and their primary care partners (informal and formal) have been evaluated. Studies show that an hour to two hour-long sessions of either art-making or art viewing decrease career stress (Hazzan et al., 2016), increase patient engagement (Hazzan et al., 2016), and increase patient well-being (Camic et al., 2014). Interventions focusing on different modes of creative expression, such as collaborative singing, have been shown to decrease care partner distress and depressive symptoms (PHQ-9) (Walters, 2019).
Given the potential for arts-based interventions to uniquely contribute to care partner well-being, this study aimed to integrate primary care partners into the OMA process—filling the role normally played by college student volunteers—and examine how participation would affect both people living with dementia and the care partners themselves. We hypothesized that providing a creative shared OMA activity outside of the normal caregiving routine would positively impact both cohorts of participants. Moreover, we hypothesized that individual classes would positively impact mood and perceived quality of life, as well as perceived amount of social support for people living with dementia. With respect to care partners, we hypothesized that the series of classes would decrease care partner burnout.
Methods
Study design
Persons living with dementia and their primary care partners were recruited to participate in four weekly OMA art classes that were an hour-long. The class was organized by one of us (KL), who had been formally trained to facilitate OMA sessions, with input from Elizabeth Lokon, creator of the national OMA initiative. Each class was designed to be feasible for participants with limited dexterity and artistic ability and included a different mode of artistic creation (i.e., printing, painting, drawing, and mask-making). Sessions began with an introduction to the materials, demonstration of a sample art project, and a read-through of written directions. All participants were then given a large-print copy of the written directions and their own art materials.
Care partners and persons with dementia cocreated a single piece of artwork, with the former encouraged to assist by promoting decision-making and autonomy for the latter (e.g., care partners would pick two colors of paint and ask their partner to decide which one to use), and by aiding in painting-related motions requiring manual dexterity that persons living with dementia may not possess. Care partners were instructed to let the patient lead the project to whatever degree the patient felt comfortable doing so, resulting in the intervention taking a partially idiosyncratic form for each care partner–patient dyad. At the end of each class, all participants were encouraged to share their artwork with peers by holding up the painting for the class to see and stating an imaginative title of the work. Participants were not required to share their work if they preferred not to.
Three residential care facilities collaborated on the initiative, and each class contained three to six people living with dementia who were either paired one-to-one with a family member or two-to-one with a primary care partners from the nursing home (i.e., nursing staff). Half of the participants (n = 6) were paired with a family member, while the other half (n = 6) were partnered with institutional caregiving personnel (when family members could not join the intervention, participants were placed with nurses who were their daily primary care partners). Participants stayed with the same partner (primary informal or formal care partners) for all four classes.
People living with dementia and their care partners participated in classes with the same group of participants for each of the four weekly classes. All participants joined all four classes. Penn State College of Medicine’s Institutional Review Board approved all aspects of the study.
Participants and recruitment
Potential participants were identified by working with care coordinators at three residential care communities in State College, Pennsylvania. All participants were diagnosed with mild to moderate dementia as measured through the St. Louis University MentalStatus Examination (SLUMS) dementia scale. The criterion for inclusion of care partners was direct family relation to the resident or nursing staff member at the residential care facility who regularly cared for the individual. Eligible residents for whom informed consent was not provided were excluded, as well as residents and care partners who could not speak English. Residents lacking a diagnosis of mild to moderate dementia were excluded.
Those interested were invited to an in-person meeting to explain the study and review the consent process. Individuals scoring below a 14 on the SLUMS scale (Cruz-Oliver et al., 2012) were invited to an additional face-to-face consent meeting, and those with a score higher than 14 were given the option of consenting via phone or mail. Consent was also obtained for care partners. To avoid coercion throughout the course of the project, the decisions of each resident and care partners to assent to attending (or not attending) a given art session were respected.
Measures
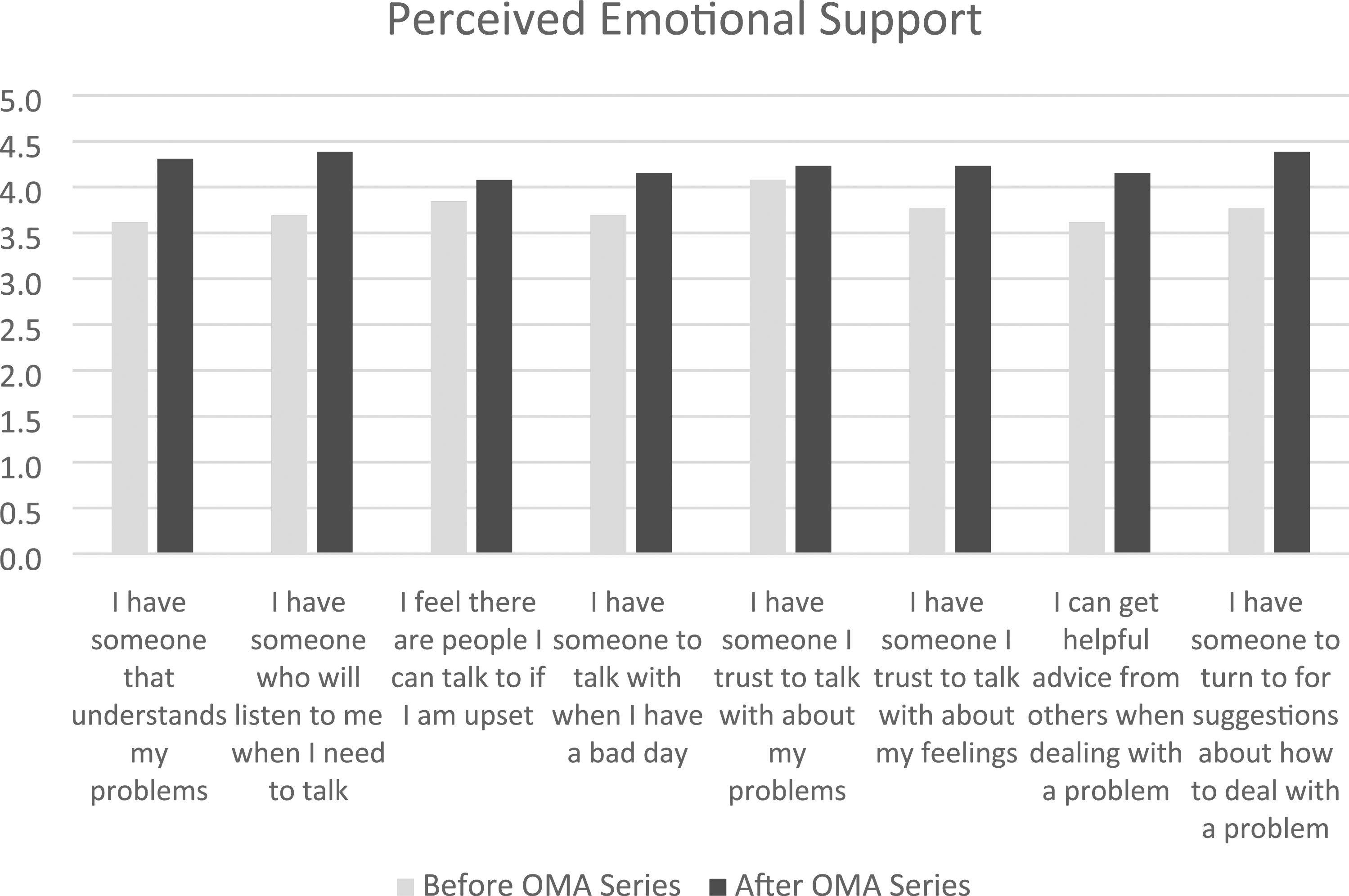
Study design consisted of pre- and post-intervention questionnaires to evaluate the aforementioned hypotheses for care partners and people living with dementia. Prior to the first OMA class, persons with dementia were given the National Institute of Health(NIH) emotional support survey, a previously assessed and validated NIH questionnaire consisting of individual responses to statements such as “I have someone who understands my problems,” with responses ranging from numerical ratings of 1 to 5, representing frequency with 1 = never, 2 = rarely, 3 = sometimes, 4 = usually, and 5 = always (Cyranowski et al., 2013). A listing of each question in the survey can be seen in Figure 1. Care partners were given the AMA caregiver burnout questionnaire, a previously validated questionnaire created by the American Medical Association, in which individuals rank “yes or no” to describe feelings of burnout within the past week for 16 questions, as well as ranking their current stress and physical health on scales of 1–10 (Epstein-Lubow et al., 2010). If there are 10 or more “yes” responses, or ratings of 6 or higher for the ranked stress level or physical health rating, this indicates a high degree of distress. These scales were readministered at the end of the last OMA session. The impact of individual art classes on participants with dementia was measured through the use of “emotional thermometers,” a visual system to describe acute levels of distress, anxiety, depression, anger, and perceived quality of life, administered before and after individual classes. Emotional thermometers consisted of rating perceptions of the aforementioned emotions on scales of 0–10 (with 0 representing the least degree of agreement with the emotion being rated). This tool has been previously published and assessed in peer-reviewed publications (Heuer & Willer, 2020.; Vigliotti et al., 2019). Average changes in perceived emotional support (N = 12). The National Institutes of Health emotional support survey was administered before and after the art class series. The survey consisted of questions listed in column 1. Individuals responded to statements such as “I have someone who understands my problems,” by ranking the degree to which they agree with the statement with numerical ratings of 1–5, representing frequency with 1 = never, 2 = rarely, 3 = sometimes, 4 = usually, and 5 = always. Responses were averaged and charted as bar graphs.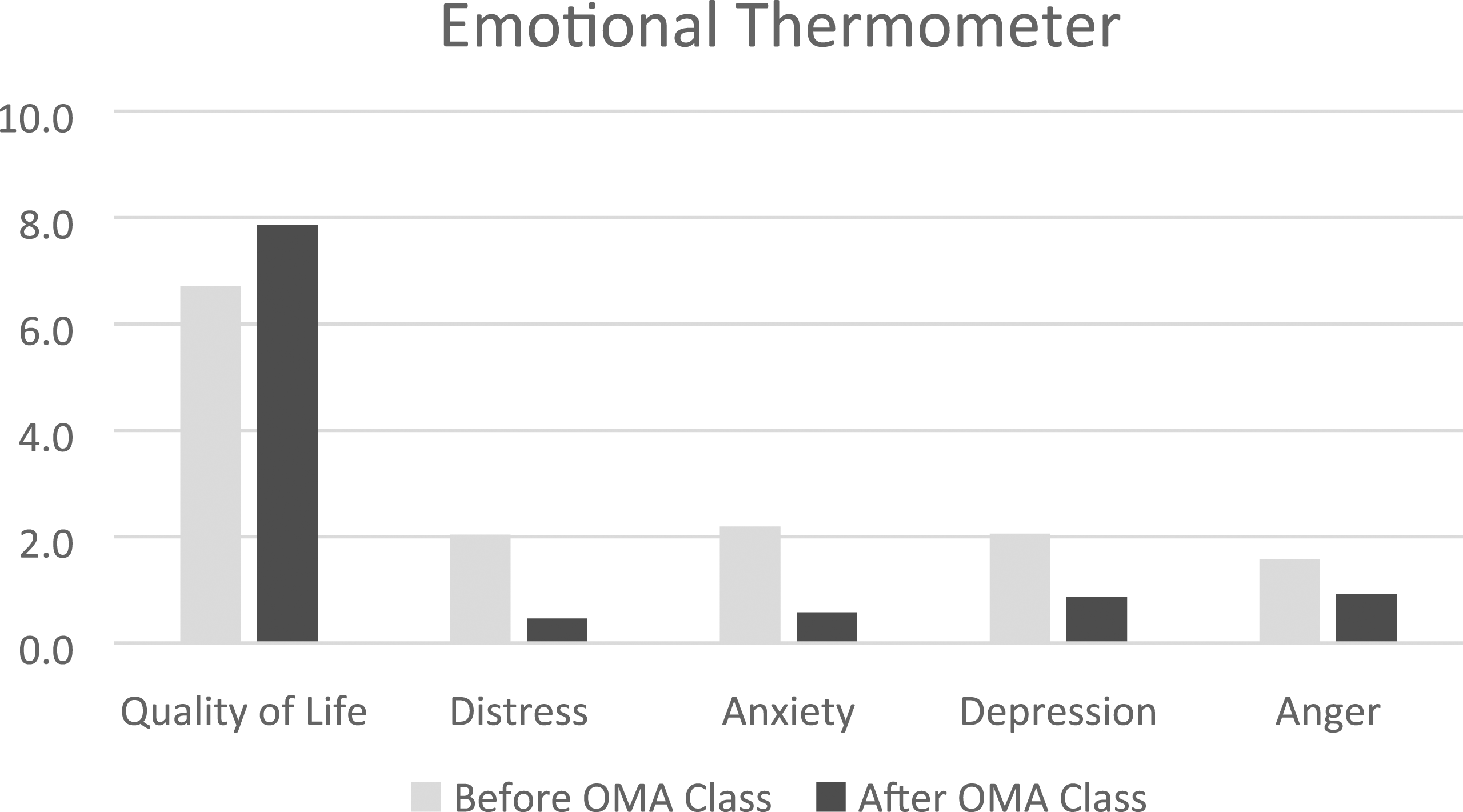
Statistical analysis
Averages of emotional thermometer ratings before and after individual art classes (N = 12). Individuals provided self-perceived ratings of quality of life, distress, anxiety, depression, and anger on scales from 0 to 10, with 10 indicating the highest expression of emotion or best quality of life. Scales were administered before and after each art class. All ratings were averaged together with significance determined through paired t-tests.
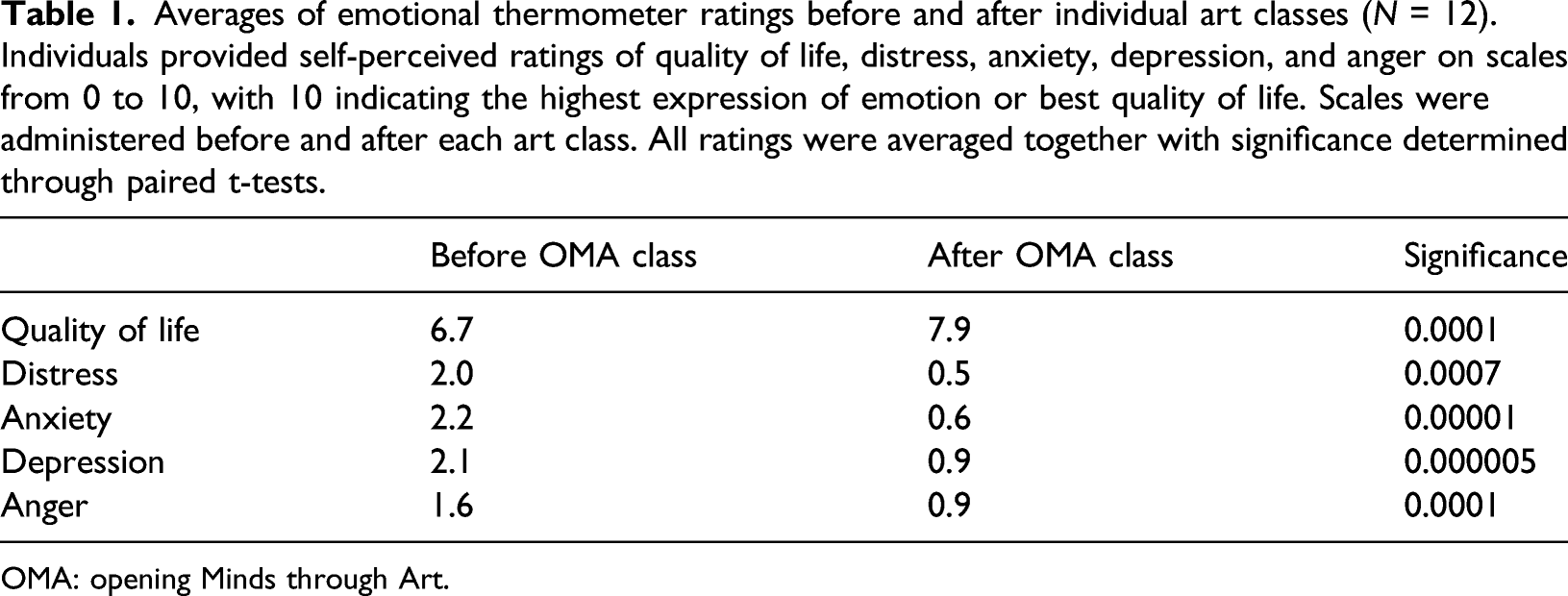
OMA: opening Minds through Art.
Average changes for the NIH emotional support survey (N = 12). NIH social support survey was administered before and after the art class series. The survey consisted of questions listed in column 1. Individuals responded to statements such as “I have someone who understands my problems,” by ranking the degree to which they agree with the statement with numerical ratings of 1–5, representing frequency with 1 = never, 2 = rarely, 3 = sometimes, 4 = usually, and 5 = always. Surveys were administered before and after the series of classes. Responses were averaged, with significance determined through paired t-tests.
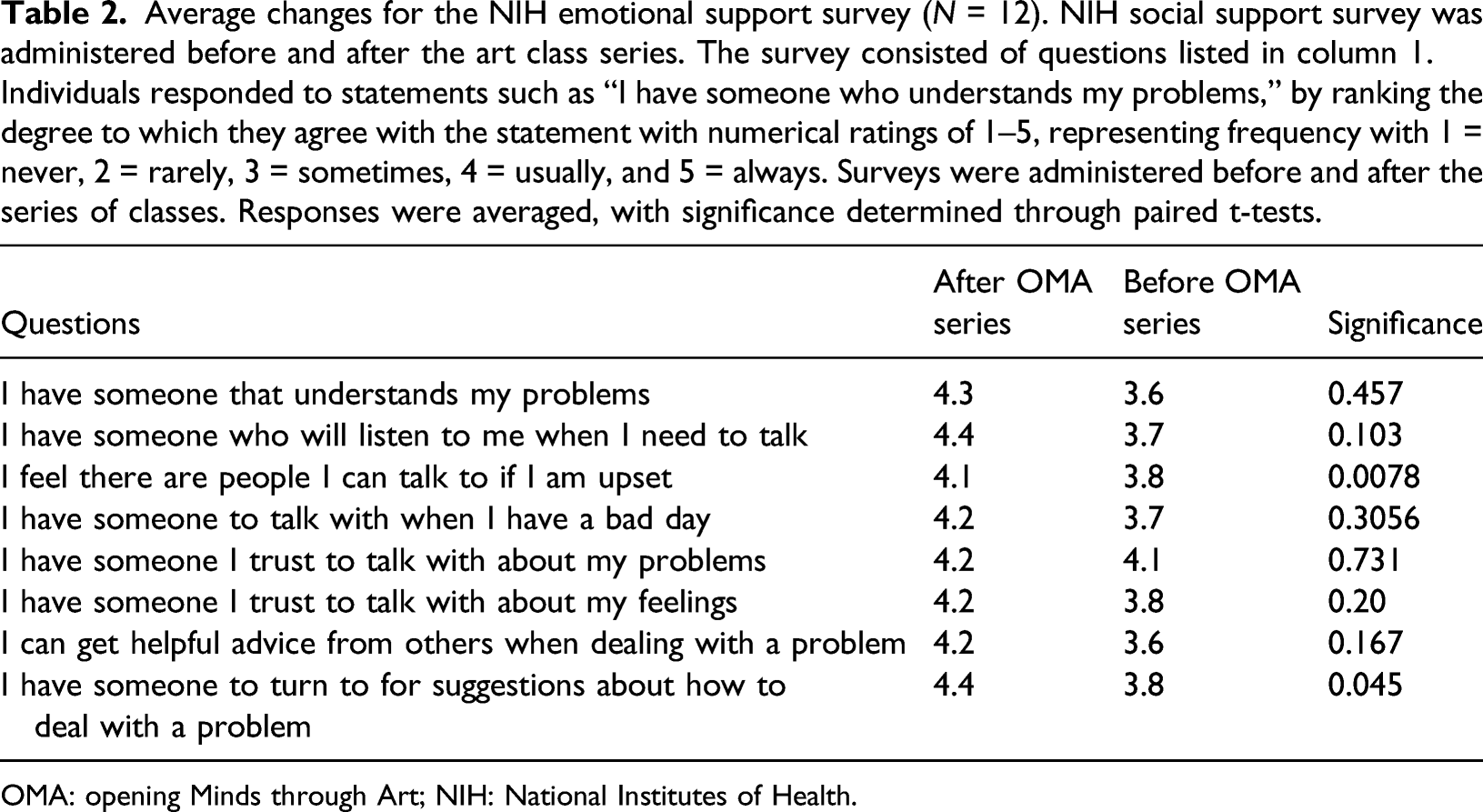
OMA: opening Minds through Art; NIH: National Institutes of Health.
Average scores on AMA caregiver burnout surveys and self-rated stress level (N = 9). Care partners were given the American Medical Association caregiver burnout survey in which individuals rank “yes or no” to describe feelings of burnout within the past week for 16 questions, as well as ranking their current stress and physical health on scales of 1–10. Ten or more “yes” responses, or ratings of 6 or higher for the ranked stress level or physical health rating, indicates a high degree of distress. Scales were administered before and after the series of classes. The total score (number of “yes” responses) as well as the self-rated stress level were averaged. Significance was determined through paired t-tests.
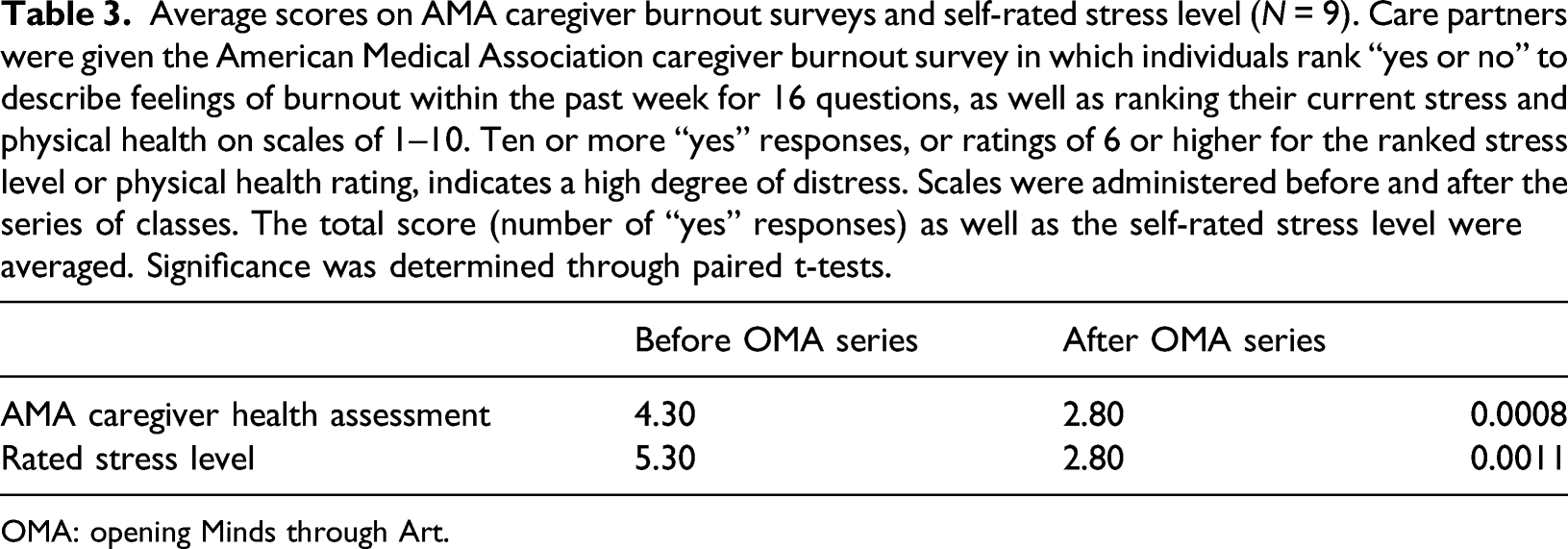
OMA: opening Minds through Art.
AMA caregiver burnout survey (N = 9). Care partners were given the American Medical Association caregiver burnout survey in which individuals rank “yes or no” to describe feelings of burnout within the past week for 16 questions, as well as ranking their current stress and physical health on scales of 1–10. Ten or more “yes” responses, or ratings of 6 or higher for the ranked stress level or physical health rating, indicates a high degree of distress. Scales were administered before and after the series of classes. The total score (number of “yes” responses) as well as the self-rated stress level were averaged and represented above in a bar graph.
Results
With respect to the acute emotional state of those living with dementia, individual OMA sessions impacted measures of distress, anxiety, depression, and anger, all of which were significantly lowered (p < .01; n = 12). Differences in self-rated emotional state and quality of life can be numerically observed in Table 1 and visualized in Figure 3. Visual representation of emotional thermometer averages (N = 12). Individuals provided self-perceived ratings of quality of life, distress, anxiety, depression, and anger on scales from 0 to 10 with 10 indicating the highest expression of emotion or best quality of life. Scales were administered before and after each art class. Ratings were averaged and presented in bar graphs above.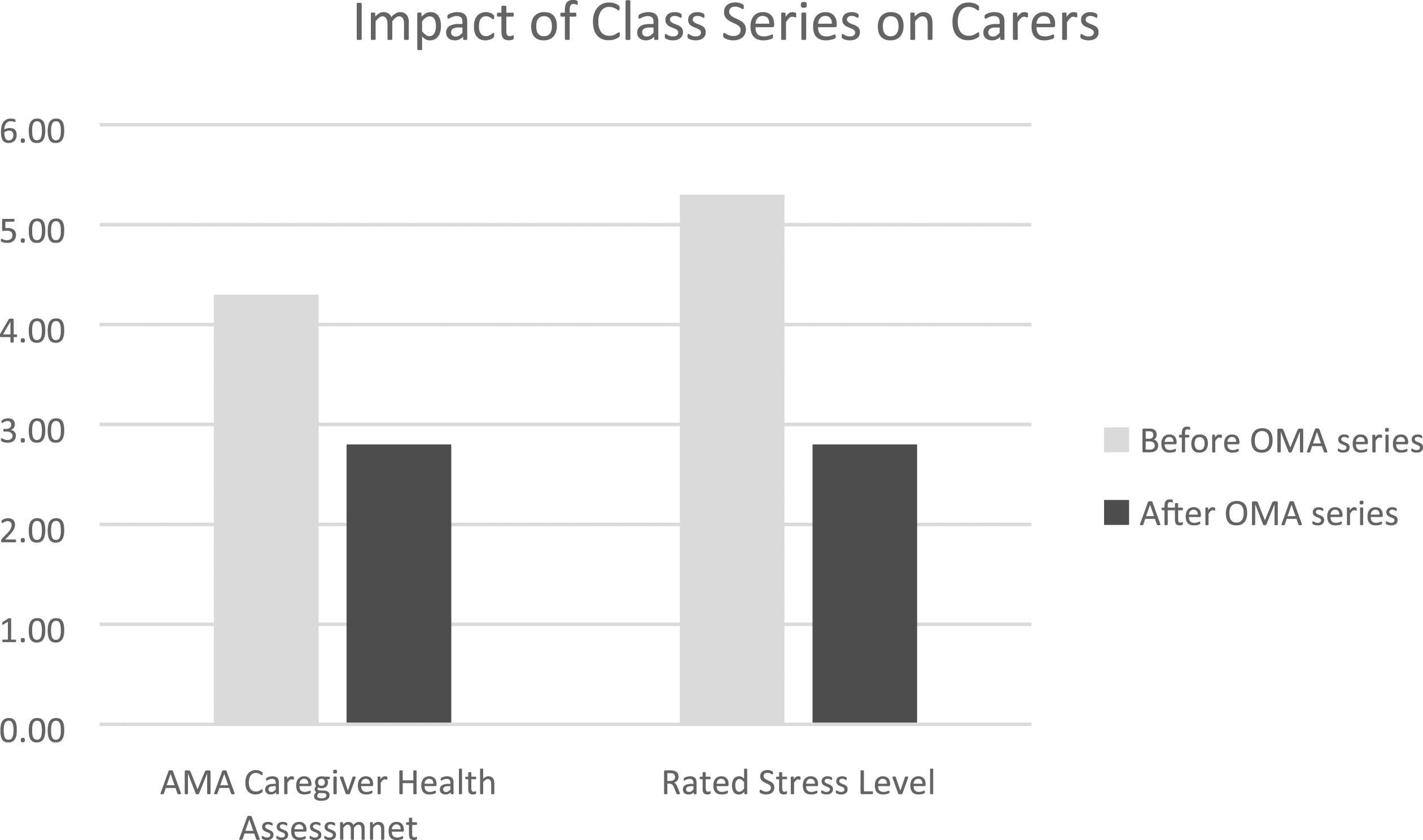
With regard to perceived emotional support, the overall series of classes had an observable impact on individuals with dementia (as visualized in Figure 1); however, changes were not all significant. The perception of the ability to “get helpful advice from others when dealing with a problem” significantly increased after the series of classes (p < .01; n = 12). Changes per each question in the NIH emotional support survey can be seen in Table 2.
For care partners, self-reporting on the AMA caregiver burnout questionnaire showed significant decreases in perceived burnout (p < .001, n = 9) after participation in the intervention. Additionally, perceived stress on a scale from 1 to 10 showed significant decreases after the series of four classes (p < .01; p = 9). A graphic representation and a table of average scores with significance can be seen in Figure 2 and Table 3, respectively.
Discussion
This is the first known study to evaluate participation of primary care partners (i.e., family members and members of institutional care teams) in the OMA initiative. We found that the impact of individual classes on improving acute emotional state for people living with dementia was significant, including measures of distress, anxiety, depression, anger, and perceived quality of life. The series of classes impacted perceived emotional support for people living with dementia, with a significant difference in the perception of the ability to “get helpful advice from others when dealing with a problem.” This confirms prior findings that involvement in creative expression programs can have a significant impact on the well-being of people living with dementia. With respect to care partner burnout and perceived stress, we also found that the OMA intervention led to significant improvements. Such findings suggest that providing a shared arts-based activity outside of typical caregiving routines can positively impact care partners—a particularly notable result given the relatively little attention this demographic has received in the literature on burnout in general, and more specifically with regard to creative programming. It also suggests that primary care partners can effectively fill the role previously carried out by college students in the OMA process.
Our results are congruent with prior arts-based interventions for people living with dementia and their primary care partners (informal and formal). It suggests that arts-based therapies that provide platforms for both verbal and nonverbal communication while promoting psychological well-being through imaginative, failure-free activities are particularly powerful in changing the dynamic of care partner relationships. In creating a milieu within residential care settings in which those living with dementia can be supported in their remaining strengths and capacities, there are opportunities to engender reciprocal benefits for care partners and residents.
We believe that implementing OMA more broadly with care partner involvement is feasible. OMA has an effective means of training individuals on how to conduct classes and grants access to instructions for many different art projects. From an institutional perspective, OMA sessions are relatively time-efficient, as each art-making session in our study was only one-hour long, with measurable benefits noticeable after a series of just four classes. Our preliminary results suggest that effective dyads can be composed of either formal or informal care partners, allowing for flexibility in implementation. One limitation to implementing this program elsewhere may be the number of primary care partners needed to join the program. Our model paired persons living with dementia with primary care partners in either a one-to-one or two-to-one ratio.
This study had several key limitations. Primarily, the relatively small sample size (9 care partners and 12 persons living with dementia) limits the generalizability of these preliminary results. Additionally, that half of participants were paired one-on-one with a care partner while the other half were joined by both care partners and a member of the nursing staff complicated the dynamics of the intervention (as mentioned, this was done in the spirit of allowing more social support for study participants who wished to engage in OMA sessions). However, this inbuilt flexibility in study design arguably makes the intervention more replicable in other care settings where staff will be present and family participation will not always logistically possible. Third, this study took place across three separate residential care homes, which limits the standardization of study context, although uniform methods were used in each setting. We believe this mitigates the potential confounder of the results being influenced by the nursing facility itself; however, we did not analyze the impact of the different nursing homes separately due to the small sample sizes. Finally, we measured care partner burnout and perceived social support by people living with dementia before and after the series of four art classes. Results may have been different had we evaluated before and after each class.
Conclusion
In recent years, non-pharmacological, arts-based activities for persons with dementia have been shown to promote psychosocial well-being, affirm a sense of self-worth, and increase overall quality of life. Opening Minds through Art is one such intervention, and this study established that care partner involvement in the OMA program is feasible. While our results should be interpreted with caution due to the small participant numbers, the preliminary data indicate that care partner involvement in the OMA program may positively affect emotional state for people living with dementia and may decrease care partner burnout.
Future research should aim to undertake studies involving greater numbers of participants. It would be especially valuable to implement study designs that compare the efficacy of different arts-based interventions and forms of expression (e.g., song, dance, and painting) on persons with dementia and their care partners and that compare such approaches with pharmacologic or other nonarts interventions. With respect to OMA, future research could look more granularly at pre–post measures for each session as opposed to the overall scope as the findings may differ.
Given the difficulty of measuring the effects of a complex human activity such as artistic expression, it may be beneficial for future researchers to use qualitative and mixed-methods approaches in evaluating the effects of such interventions. There may also be opportunities for more biometric analyses (e.g., cortisol markers for pre–post stress). Ultimately, this preliminary work suggests that visual arts–based interventions like OMA can have a positive impact on both people living with dementia and their primary care partners.
Footnotes
Acknowledgements
We would like to thank the Caputo family and Penn State College of Medicine for supporting this work. We would also like to acknowledge the care coordinators of Foxdale, Centre Crest, and Harmony retirement communities for their involvement and collaboration with this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received the Caputo Alzheimer Grant from Penn State University College of Medicine. Art supplies and training through Opening Minds through Art were paid for with this funding. Participants did not receive monetary compensation for participation in the study.
Ethical Approval
This work was approved by Penn State College of Medicine’s Institutional Review Board.