
Abstract
Advance care planning is a crucial element of high-quality, person-centred end-of-life care for people with dementia; however, levels have remained persistently low. Recent debates have emphasised informal conversations within families. Understanding factors associated with advance care planning and informal conversations may help target support more effectively. Data were collected in face-to-face interviews with 420 dyads of people with dementia and their carers, within 18 months of diagnosis, as part of the observational DETERMIND cohort study. Cross-sectional multivariable logistic regression analyses of observational data were used to examine factors associated with five types of future care planning. Nearly a quarter (22.1%) had undertaken no future care planning at all, not even informally with their carer. Less than half (44.9%) reported having an informal conversation with their carer, with only 16.9% saying that they had ‘definitely’ had such a conversation and the remaining 28% saying they had done so only ‘to some degree.’ Lasting powers of attorney (LPA) for health and welfare (64.7%) were common but frequently not underpinned by informal discussions. Conversations with a GP (14.1%), advance statements (9.1%) and advance decisions (10%) appeared to occur late, when people were older, had more severe dementia symptoms and lower quality of life, and carers were experiencing greater burden. People with dementia with better-resourced carers were more likely to engage in future care planning, suggesting inequalities in access. This included carer use of support and information services, associated with conversations with a GP or other professional and LPAs for health and welfare, and higher carer educational attainment, associated with having informal conversations. Lower dementia severity was also associated with informal conversations, suggesting a more active role for people with mild dementia. Our findings suggest a need for more relational approaches, including support for informal conversations, high-quality carer support, timely and consistent professional involvement and additional support for those without close carers.
Background
Advance care planning is defined by the European Association for Palliative Care (EAPC) as a process that enables ‘individuals to define goals and preferences for future medical treatment and care, to discuss these goals and preferences with family and healthcare providers, and to record and review these preferences, if appropriate’ (Rietjens et al., 2017). It is recognised as a crucial element of high-quality, person-centred end-of-life care (National Institute for Health and Care Excellence, 2019), and has been associated in research with a range of positive outcomes, including greater alignment of care with individual preferences, lower levels of hospitalisation in the last three months of life, and improved bereavement outcomes for carers (Brinkman-Stoppelenburg et al., 2014; Dixon et al., 2018; McMahan et al., 2021; Wendrich-van Dael et al., 2020). Advance care planning is especially important for people with dementia since capacity to communicate and participate in decision-making declines as the cognitive impairment implicit in the condition progresses (National Institute for Health and Care Excellence, 2018; Van den Block, 2019; van der Steen et al., 2014a).
Despite reported benefits, levels of advance care planning among people with dementia have remained persistently low (Gotanda et al., 2022; Lewis et al., 2015). This is despite an emphasis in policy on early or ‘timely’ diagnosis to support better care planning (Hampel et al., 2022). Identified barriers for general populations include diagnostic uncertainty, discomfort discussing end of life, time pressures within services, and uncertainty about when and how advance care planning conversations should be initiated (Blackwood et al., 2019; Lund et al., 2015). People with dementia face additional challenges. They often have a limited understanding of their condition due to lack of insight (Sleeman & Sampson, 2022; van der Steen et al., 2013), avoidance (Ashworth, 2020). Professionals may avoid discussion of dementia as a progressive, terminal condition and/or lack the tools or confidence to facilitate advance care planning in this population (Moore et al., 2019; Tilburgs et al., 2018). Unwarranted assumptions about capacity can also lead to people with dementia being inappropriately excluded from discussions (Tilburgs et al., 2018). Carers can, as a result, be left making decisions on behalf of the person with dementia while feeling insufficiently prepared or supported (Sellars et al., 2019). Calls for a more relational approach have emphasised ongoing, informal conversations within families and preparing carers for later ‘in-the-moment’ decision-making (Malhotra, 2023; Van den Block, 2019; van der Steen et al., 2024).
Given this context, it is important to understand factors that are associated with formal advance care planning and informal family conversations, especially in the first year or two following diagnosis diagnosis when people with dementia are most able to contribute meaningfully. This may help policymakers and clinicians target their efforts more effectively. The existing literature here is limited. Most relevant studies focus on general populations of older people, not people with dementia, and are predominantly from the United States (US) (Lai et al., 2019). To our knowledge, there are no existing studies, particularly using large quantitative samples, that focus on individuals recently diagnosed with dementia including factors relating to the person with dementia and their carer. Studies into factors associated with informal conversations about future care are also rare (Van den Block, 2019). This study addresses these gaps by aiming to identify factors associated with different ways of planning for future care, including advance care planning and informal family conversations, in a large UK cohort of people recently diagnosed with dementia and their family carers. 1
Methods
Sample and Data Collection
This paper reports cross-sectional analyses of data from the DETERMinants of quality of life, care and costs, and consequences of INequalities in people with Dementia and their carers (DETERMIND) study. DETERMIND is a mixed-methods, longitudinal, observational cohort study that recruited a new cohort of people with dementia (target n = 900) and their family carers from memory assessment services in three areas of England: South East, South London and North East. Recruitment took place between August 2019 and March 2023, with a pause in recruitment between March 2020 and February 2021 due to the COVID-19 pandemic.
Eligible participants were people with dementia within six months of diagnosis; there were no other exclusion criteria. Clinicians within participating services made initial approaches to eligible participants to find out whether they would be willing to be contacted by a DETERMIND researcher. Those who agreed were provided with study information and researchers followed up one to two weeks later to answer any questions and confirm willingness to take part. Where a family carer was available and willing to participate, they were also recruited.
Survey data were collected at baseline and annually for up to three years. Data analysed in this paper were drawn from baseline and the one-year follow-up interview to cover a follow up period of 18 months post-diagnosis. At each wave, people with dementia and carers completed a series of questionnaires administered by researchers face-to-face in participants’ homes (or by telephone or video-conferencing when pandemic restrictions prevented home visits). These lasted approximately 120 minutes. Interviews were conducted flexibly where needed, for example across multiple visits or with two researchers interviewing the person with dementia and carer simultaneously. All participants with dementia provided informed consent or were consented via a consultee, with proxy data collected where appropriate.
Further information about sampling, recruitment and data collection are provided in Farina et al. (2020). Ethics approval was granted by the Health Research Authority Brighton and Sussex Research Ethics Committee (REC 19/LO/0528; IRAS 261263).
Measures
Questions concerning five future care planning activities were included in the DETERMIND questionnaires (see Figure 1). These were chosen to reflect a broad conceptualisation of future care planning, encompassing both formal advance care planning processes (advance statements, advance decisions, and lasting power of attorney for health and welfare), as well as discussions about future care with a GP or other professional and informal conversations with a carer. Future care planning questions in DETERMIND questionnaires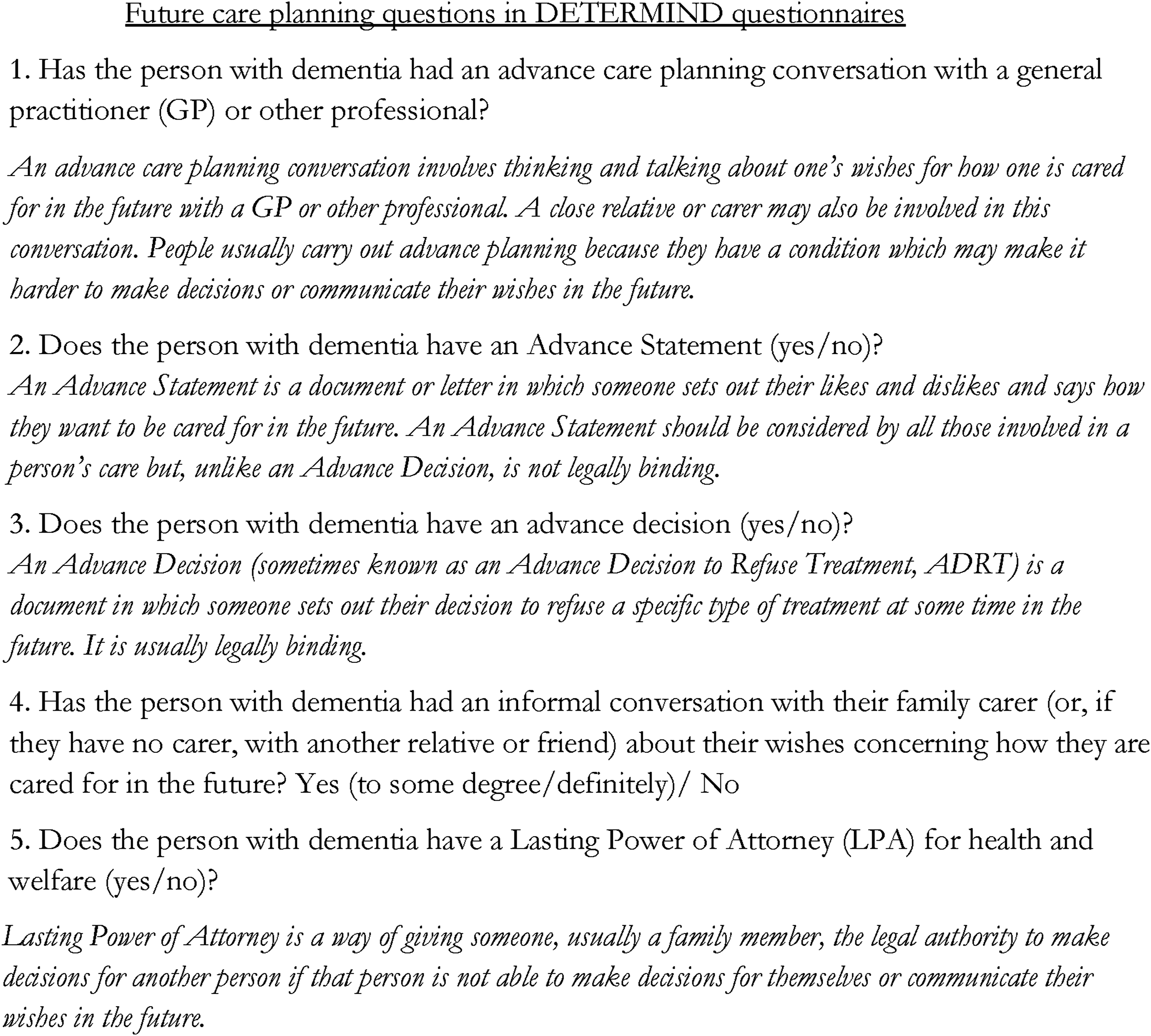
The selection and structuring of these different future care planning outcomes were informed by existing conceptual and empirical literature that characterises advance care planning as a process rather than a single event, as involving both documentation and ongoing conversations over time, and as occurring across clinical and family contexts (Rietjens et al., 2017; van der Steen et al., 2024). Particular attention was given to relational perspectives emphasizing the role of family discussion and shared decision-making in dementia care (Phenwan et al., 2025; Van den Block, 2019).
As no suitable existing survey items were identified, these measures were developed specifically for DETERMIND. Their development was informed by the literature and consensus among the study’s co-authors, alongside consultation with an experts-by-experience group comprising five family carers and two people with dementia, supported by the study’s Research Involvement Manager, herself a carer of her husband with dementia.
People with dementia and carers were asked these questions at baseline baseline (within 6 months of diagnosis) and approximately one year later (within 18 months of diagnosis). Data from these two time points were included but analyses were cross-sectional rather than longitudinal. Outcomes were defined cumulatively, with data from both waves used to identify whether future care planning activities had occurred within the follow-up period, up to 18 months following diagnosis.
Five binary outcome measures were available for analysis. A positive response (e.g. having an advance statement) was recorded if the person with dementia or their carer reported such at either of the two time points.
DETERMIND included a wide range of potential factors to examine for their association with different approaches to planning for future care. Selection was informed by the literature (e.g. Lai et al., 2019; Lovell & Yates, 2014; van der Steen et al., 2014b), discussion amongst the DETERMIND study team comprised of clinical and non-clinical dementia researchers, and consensus among the study’s authors. As with the outcome measures, it was also informed by consultation with an experts-by-experience group. Factors were grouped into the following categories. Indicators for each factor were derived from baseline data unless otherwise indicated.
Demographic Factors
We included measures of sex and age for both the person with dementia and their carer, and whether or not at least one member of the dyad belonged to a non-White minority ethnic group (y/n). We also included the memory assessment service area (South East England; Newcastle and the North East; and South London).
Education Level/Socio-Economic Status
We included the highest educational qualification for the person with dementia and their carer, and socio-economic status using the Index of Multiple Deprivation (IMD) for England based on the person with dementia’s postcode (scores between 1 to 10).
Relationships
We included the relationship of the carer to the person with dementia (spouse, son/daughter, other). We measured the quality of the relationship between the person with dementia and their carer, viewed from both the person with dementia’s and carer’s perspective, using a question taken from the 5-item Positive Affect Index: “Taking everything into consideration, how close do you feel in your relationship with (person with dementia/carer)?” (Bengston & Schrader, 1982). Response options range from 1-not close at all, to 6-extremely close. We also included the six-item Lubben Social Network Scale (Lubben et al., 2006), with scores ranging from 0 to 30, where higher scores reflect more social engagement.
Health Status
We used the Standardised Mini Mental Scale Examination (sMMSE), administered in person by an interviewer (Molloy & Standish, 1997) to measure cognitive impairment with the total score ranging from 0 to 30 and distinguishing between mild (20–30), moderate (10–19) and severe (0–9) cognitive impairment. We used the Clinical Dementia Rating Scale (CDR) (Morris, 1993) to ascertain severity of dementia, this was completed by researchers after interviewing the person with dementia and discussion with their carer, with scores of 0 (no dementia), 0.5 (minimal), 1 (mild), 2 (moderate) and 3 (severe). We also included the Charlson Comorbidity Index (CCI), which predicts the ten-year mortality for those with a range of comorbid conditions (Charlson et al., 1987). This was completed by both the carer and the person with dementia.
Support and Information
We derived an index that combined responses to three questions about whether information was provided at diagnosis about, respectively, what dementia is, disease progression and advance care planning. A value of 1 indicated that information on at least one of these topics was provided. We also included a measure of whether the carer had used any of the following support and information services: self-help groups, education groups, expert relative groups, advice lines, online support, Alzheimer’s Café, and/or an Admiral Nurse. . This was asked at both baseline and again a year later in order to identify use across the follow up period, up to 18 months post-diagnosis.
Quality of Life and Burden
For the person with dementia this was measured using the self-report DEMQOL (Smith et al., 2007) and proxy-report DEMQOL-Proxy (Smith et al., 2007). For the carer we used C-DEMQOL (Brown et al., 2019). Carer burden was measured using the Zarit Carer Burden Inventory (short form) (ZCBI) (Zarit et al., 1980) with a score range of 0 to 88, with higher scores reflecting greater burden.
Optimism, Activation and Coping
We included the Revised Life Orientation Test (LOT-R) to measure optimism completed by the person with dementia and the carer (Scheier et al., 1994). Total scores for this five-item measure range from 0 to 20, with higher scores representing greater optimism. We also used the Brief COPE, both for the person with dementia and their carer (Carver, 1997). This was used to identify coping styles; problem-focused coping (scoring 0–32), emotion-focussed coping (scoring 0–48) and avoidant coping (scoring 0–32).
Statistical Analysis
All analysis was performed using Stata Version 18.5 (StataCorp, 2023). The demographic characteristics of the sample and descriptive statistics for the five outcomes of interest - conversations with a GP or other professional, advance statements, advance decisions, informal conversations with a carer and lasting power of attorney for health and welfare - were summarised. Subsequent statistical analysis was exploratory in nature. Selection of variables potentially associated with the different future care planning outcomes was iterative. Initial selection was theoretically driven, with bivariate analysis conducted as a screen to assess the association between each future care planning outcome variable and potentially related factors. If the factor indicator was continuous (e.g. age), t-tests were performed; if categorical (e.g., relationship of carer to person with dementia), chi-squared tests were performed. The high number of corrections might suggest using a Bonferroni correction (Dunn, 1961), however, given the exploratory nature of the analysis, we used a p-value of 0.05 to indicate statistical significance. We then estimated multivariable models for each of the future care planning outcomes using logistic regression. Each model started with factors found statistically significant in bivariate analysis. Where two or more of explanatory variables were found to be highly correlated, the one with the stronger bivariate association with the outcome was retained. A backward elimination process was followed to remove factors no longer statistically significant in the presence of the other factors. The final model for each outcome variable included only factors remaining statistically significant. Results are presented as odds ratios. Unless otherwise stated, the direction of the association remained the same across the bivariate and multivariable models in relation to the outcome variable.
The goodness of fit of each final model was assessed using the Pearson’s chi-square goodness of fit test (Pearson, 1992). This test evaluates the differences between the counts of observed and expected outcomes, using cells defined by the covariate patterns. The null hypothesis is that the differences between the observed and expected counts are similarly distributed. The overall rate at which the model correctly predicts the observed binary outcome is presented for each model (using the Stata ‘estat classification’ postestimation command with the observed probability of a positive outcome specified)) (StataCorp, 2023). We were guided by the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for reporting of cross-sectional, observational studies (von Elm et al., 2007).
Results
Sample
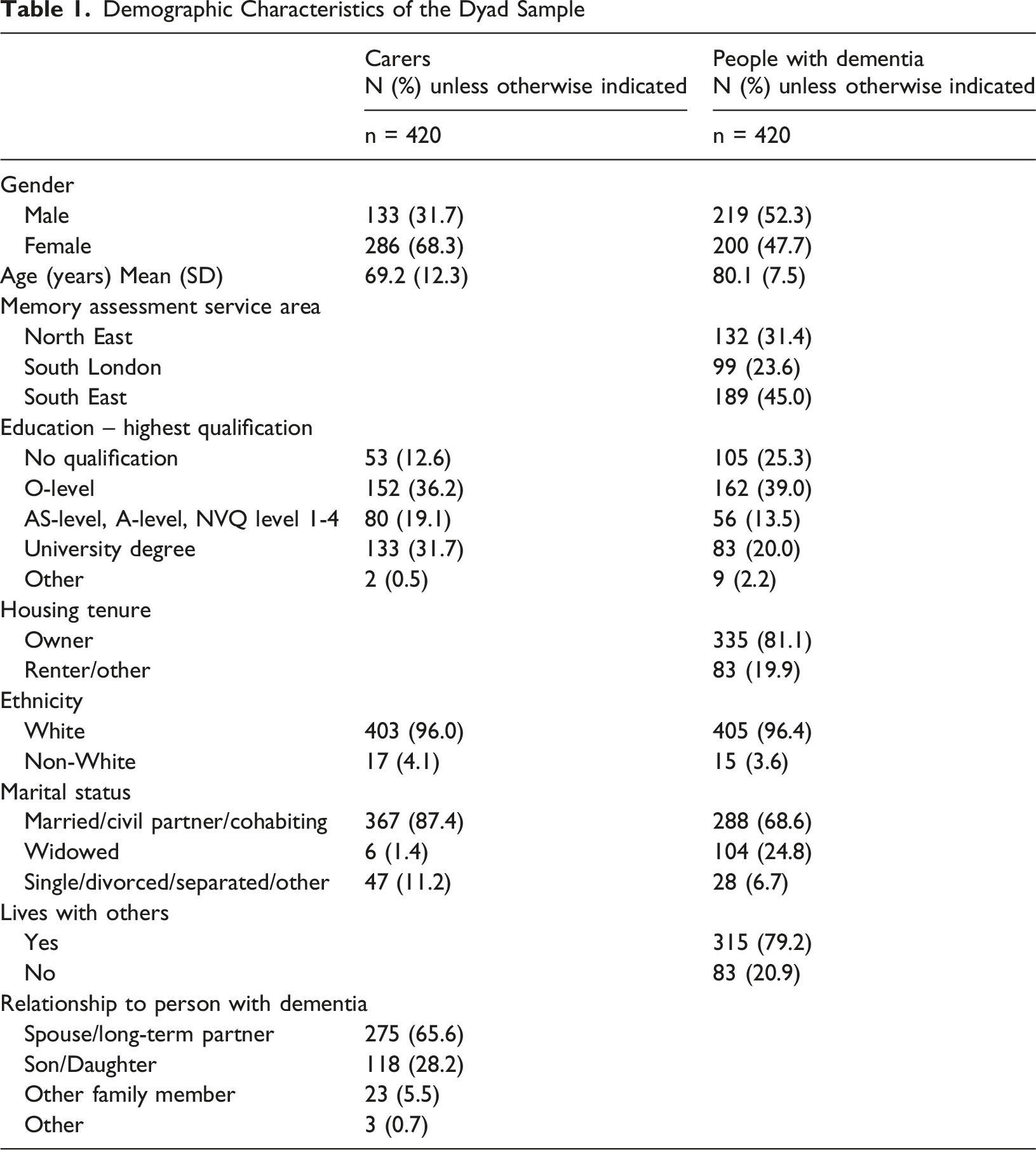
Demographic Characteristics of the Dyad Sample
Attrition of dyads between baseline (n = 698) and 1-year follow-up (n = 420) was 39.8%. While relatively high, this is consistent with expectations for older populations with dementia, where attrition is typically non-random and linked to health status, age, caregiving context, and sample composition (Burke et al., 2019; Hernandez et al., 2024). The COVID-19 pandemic may also have influenced participation patterns.
Demographic Characteristics of the Dyad Sample by Follow-Up Status: Retained at One-Year Follow-Up vs Not Retained
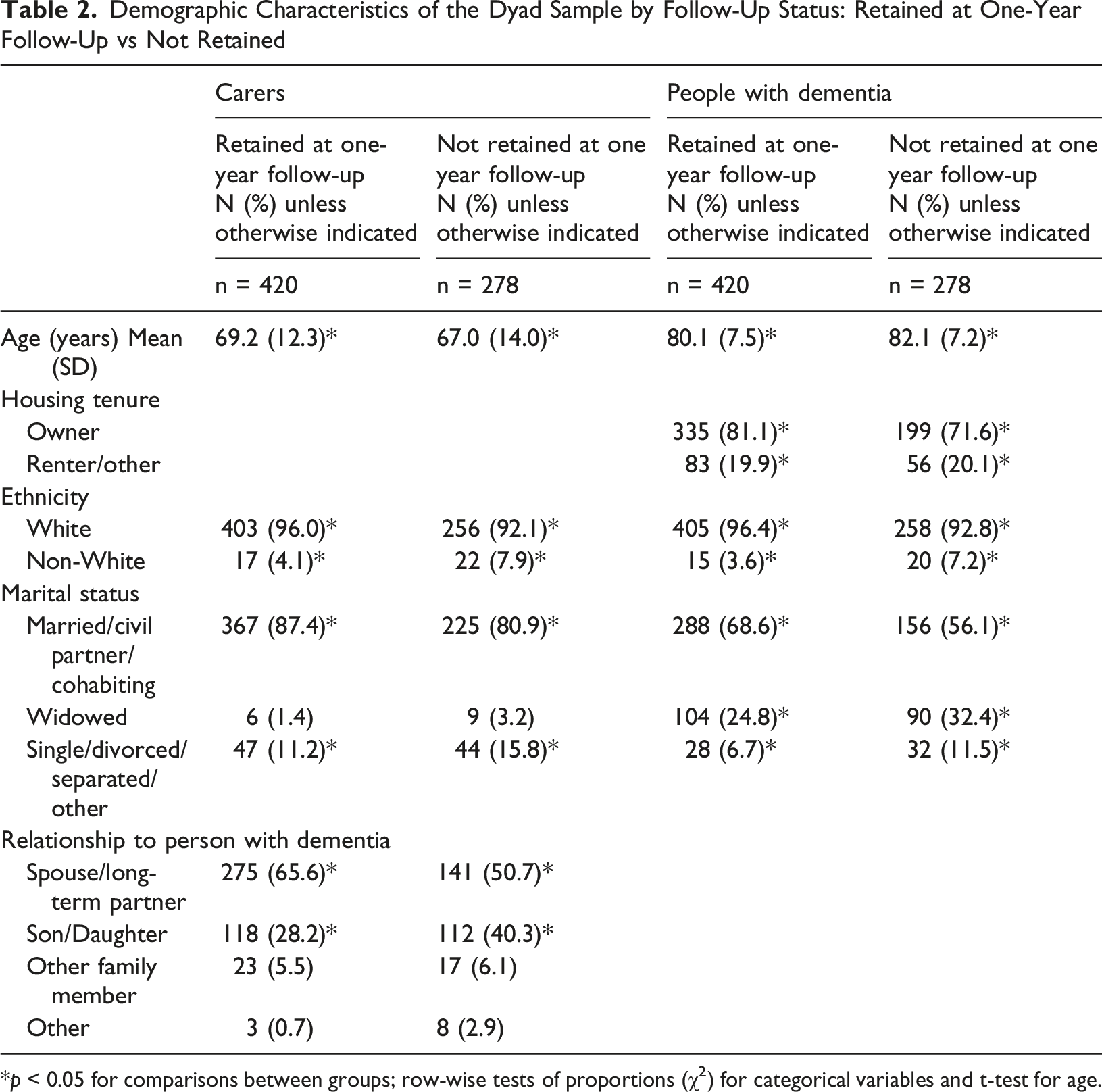
*p < 0.05 for comparisons between groups; row-wise tests of proportions (χ2) for categorical variables and t-test for age.
Prevalence of Future Care Planning Activities
Distribution of Responses to Advance Care Planning Questions
Conversation With a GP or Other Professional About Future Care
Factors Associated With Having a Conversation With a GP or Other Professional About Future Care
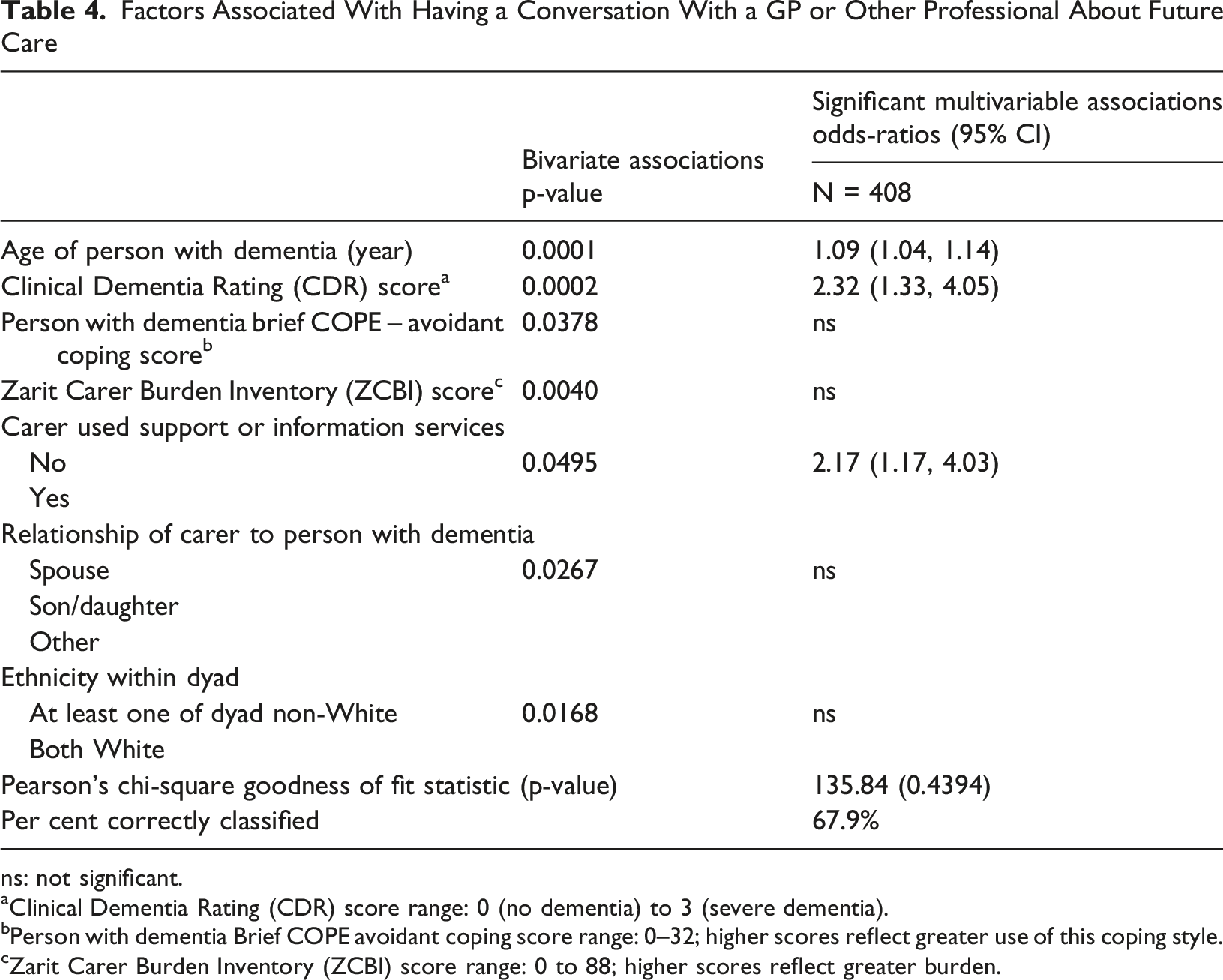
ns: not significant.
aClinical Dementia Rating (CDR) score range: 0 (no dementia) to 3 (severe dementia).
bPerson with dementia Brief COPE avoidant coping score range: 0–32; higher scores reflect greater use of this coping style.
cZarit Carer Burden Inventory (ZCBI) score range: 0 to 88; higher scores reflect greater burden.
In multivariable analysis, factors remaining statistically significant were the person with dementia being older and having more severe dementia, and carers’ use of support and information services. A one-year increase in the person with dementia’s age was associated with a 9% increase in the odds of having such a conversation and a one-unit increase on the CDR more than doubled the odds of this outcome. Where the carer had used support and information services, the person with dementia had over double the odds of a conversation with a GP or other professional.
Advance Statement
Factors Associated With Having an Advance Statement
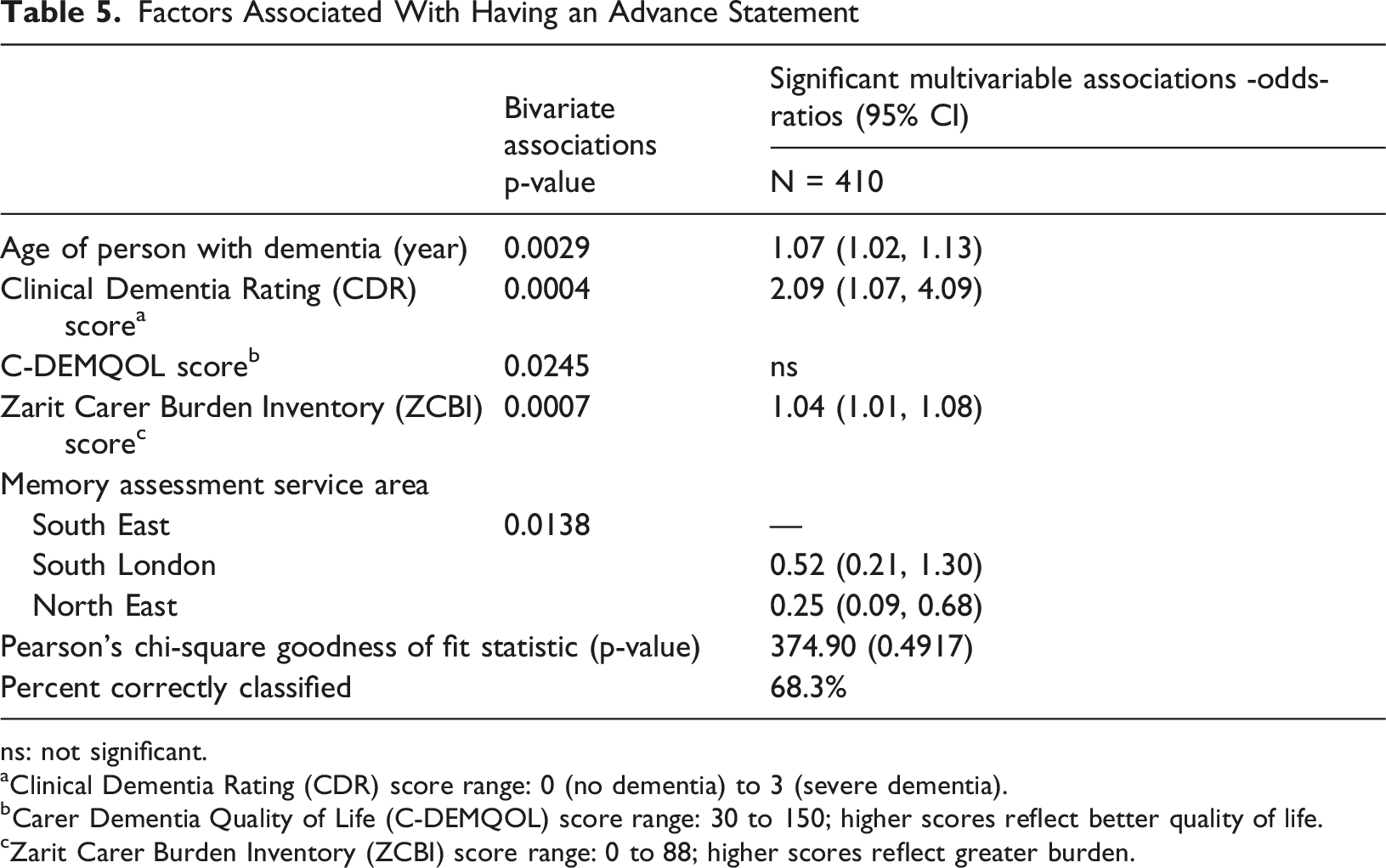
ns: not significant.
aClinical Dementia Rating (CDR) score range: 0 (no dementia) to 3 (severe dementia).
bCarer Dementia Quality of Life (C-DEMQOL) score range: 30 to 150; higher scores reflect better quality of life.
cZarit Carer Burden Inventory (ZCBI) score range: 0 to 88; higher scores reflect greater burden.
In multivariable analysis, factors remaining statistically significant were the person with dementia being older and having more severe dementia, increased carer burden and memory assessment service area. A one-year increase in the person with dementia’s age was associated with a 7% increase in the odds of having an advance statement, and a one-unit increase on the CDR more than doubled the odds. A one-unit increase in the ZCBI score was associated with a 4% increase in the odds of this outcome. Those in the South East of England had almost four times the odds of having an advance statement compared with the North East of England.
Advance Decision
Factors Associated With Having an Advance Decision
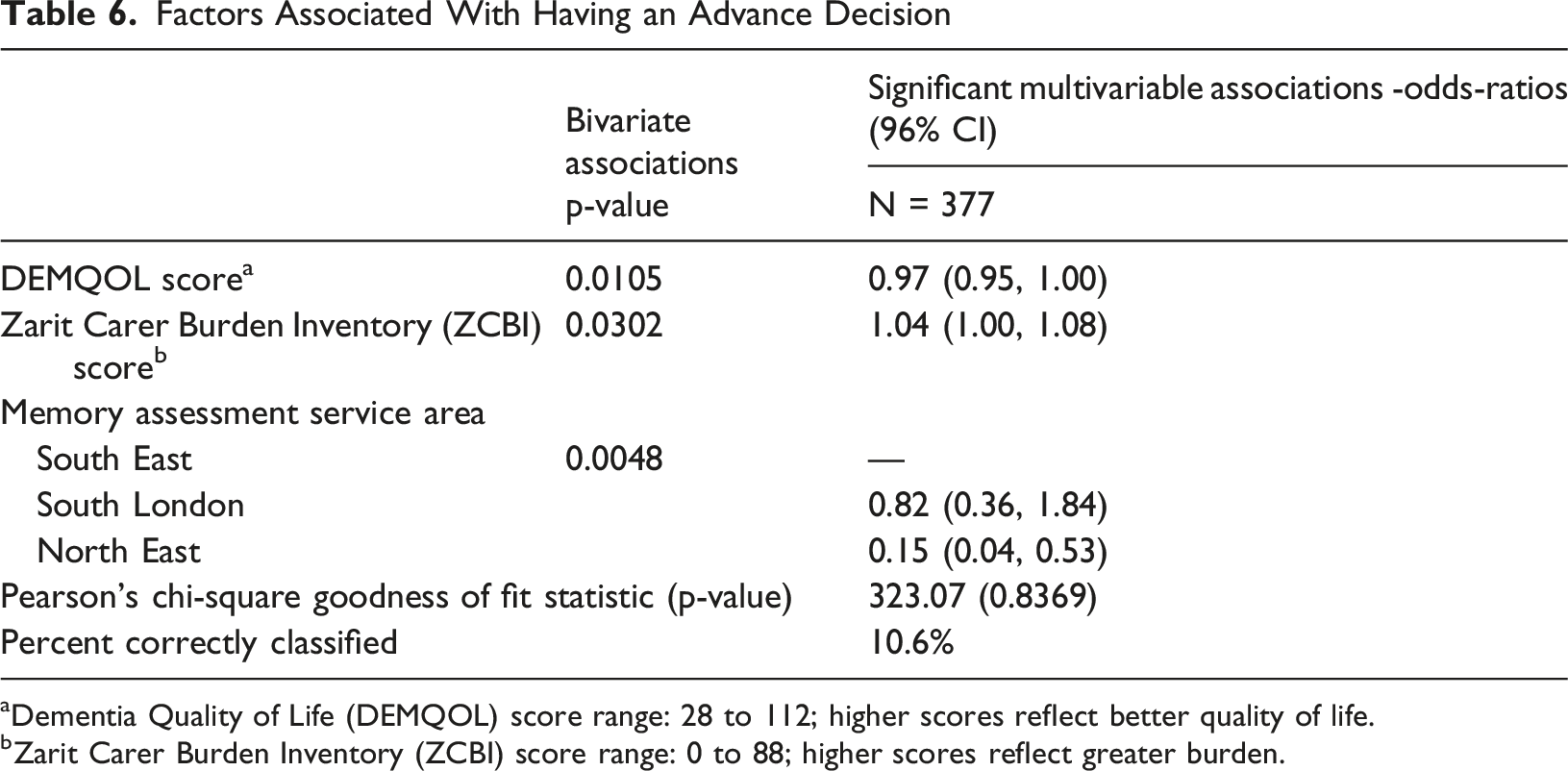
aDementia Quality of Life (DEMQOL) score range: 28 to 112; higher scores reflect better quality of life.
bZarit Carer Burden Inventory (ZCBI) score range: 0 to 88; higher scores reflect greater burden.
In multivariable analysis, all factors remained statistically significant. A one-unit decrease in the person with dementia’s quality of life score (DEMQOL) was associated with a 3% increase in the odds of having an advance decision. A one-unit increase in the ZCBI score was associated with a 4% increase in the odds of this outcome. Those in the South East of England had almost seven times the odds of having an advance decision compared to those in the North East.
Informal Conversation With Carer About Future Care
Factors Associated With Having an Informal Conversation With a Carer About Their Future Care
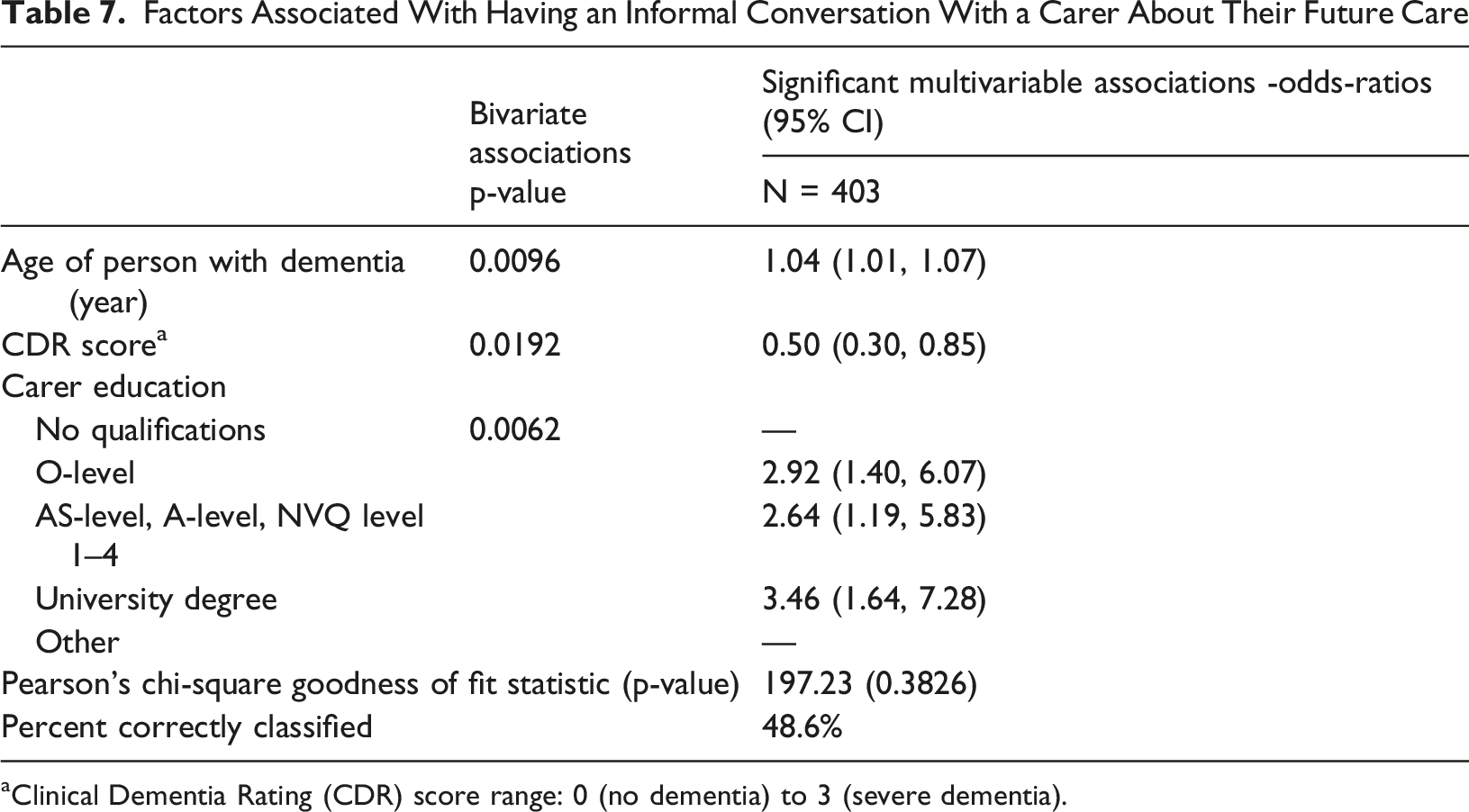
aClinical Dementia Rating (CDR) score range: 0 (no dementia) to 3 (severe dementia).
In multivariable analysis, all factors remained statistically significant. A one-year increase in the person with dementia’s age was associated with a 4% increase in the odds of having an informal conversation, while a one-unit increase in the CDR score halved the odds. Compared to people with dementia whose carers had no qualifications, those whose carers had O-levels or equivalent had three times the odds of having an informal conversation, while those whose carers had a university degree had almost three and a half times the odds of this outcome.
Lasting Power of Attorney for Health and Welfare
Factors Associated With Having a Lasting Power of Attorney for Health and Welfare
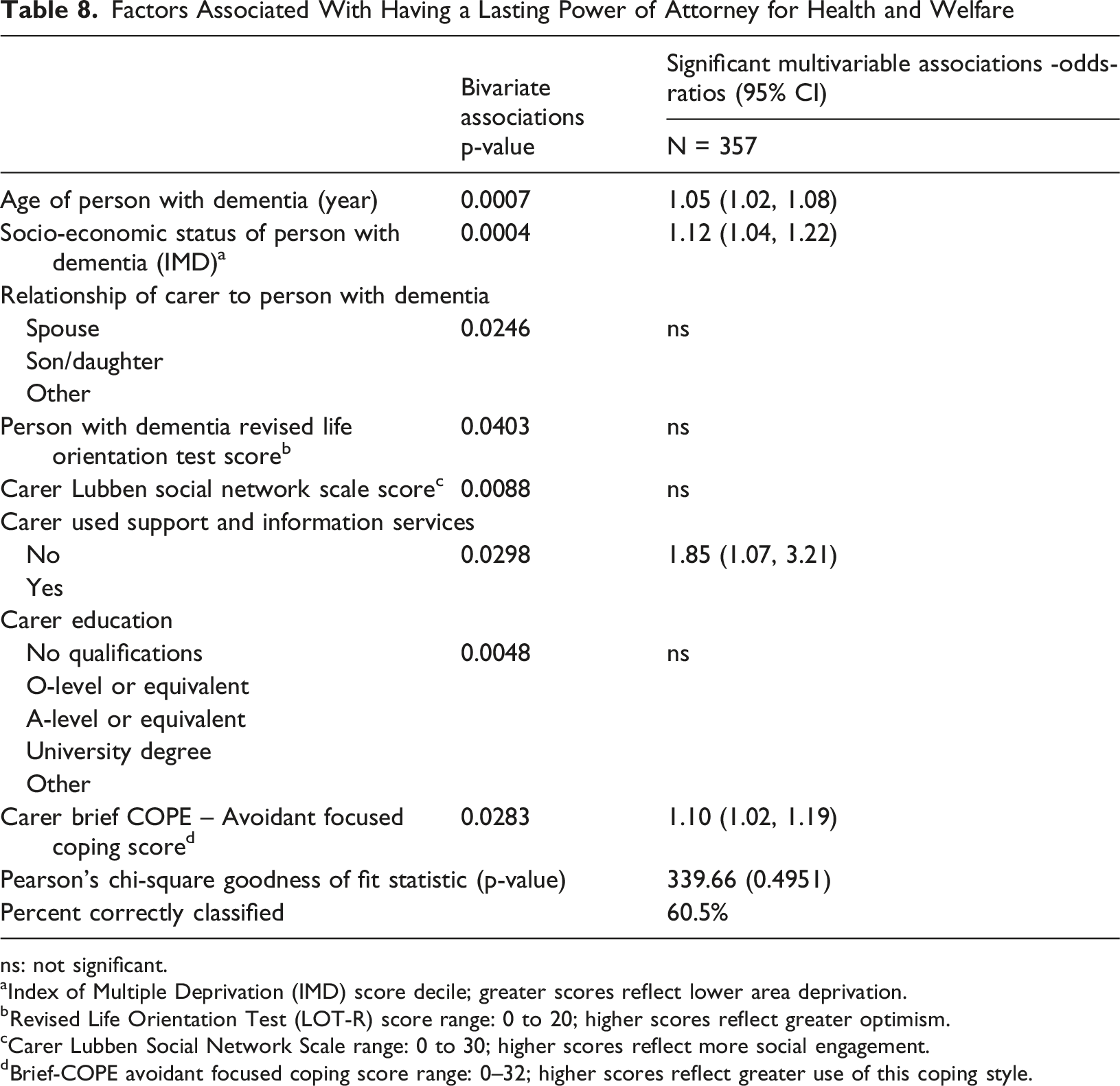
ns: not significant.
aIndex of Multiple Deprivation (IMD) score decile; greater scores reflect lower area deprivation.
bRevised Life Orientation Test (LOT-R) score range: 0 to 20; higher scores reflect greater optimism.
cCarer Lubben Social Network Scale range: 0 to 30; higher scores reflect more social engagement.
dBrief-COPE avoidant focused coping score range: 0–32; higher scores reflect greater use of this coping style.
In multivariable analysis, factors remaining statistically significant were the person with dementia being older and living in a less deprived area, carer use of support and information services, and carers having an avoidant coping style. A one-year increase in the person with dementia’s age was associated with a 5% increase in the odds of having a lasting power of attorney for health and welfare, and each one-decile increase in IMD was associated with a 12% increase in the odds for this outcome. Carer use of support and information services was associated with an 85% increase in the odds of having a lasting power of attorney for health and welfare. A one-unit increase on the carer Brief-COPE avoidant coping score was associated with 10% greater odds of this outcome.
Discussion
Analysing data from 420 dyads of people with dementia and carers drawn from DETERMIND, we examined factors associated with planning for future care in the first 18 months following diagnosis. We adopted a relational perspective, using factors related to people with dementia and carers to consider their respective contributions. Five types of future care planning were examined: conversations with a GP or other professional, advance statements, advance decisions, informal conversations with family carers, and lasting power of attorney for health and welfare. Our findings indicate that within the critical first 18 months following diagnosis just under a quarter of people with dementia undertake no planning for their future care at all, not even through informal conversations with their carers. Lasting power of attorney for health and welfare was common but often not underpinned by conversations with carers, with other types of future care planning tending to occur late, at points of deterioration and carer strain. Carer resources were associated with having a conversation with a GP or other professional, informal conversation and lasting power of attorney for health and welfare.
Prevalence of Future Care Planning Activities
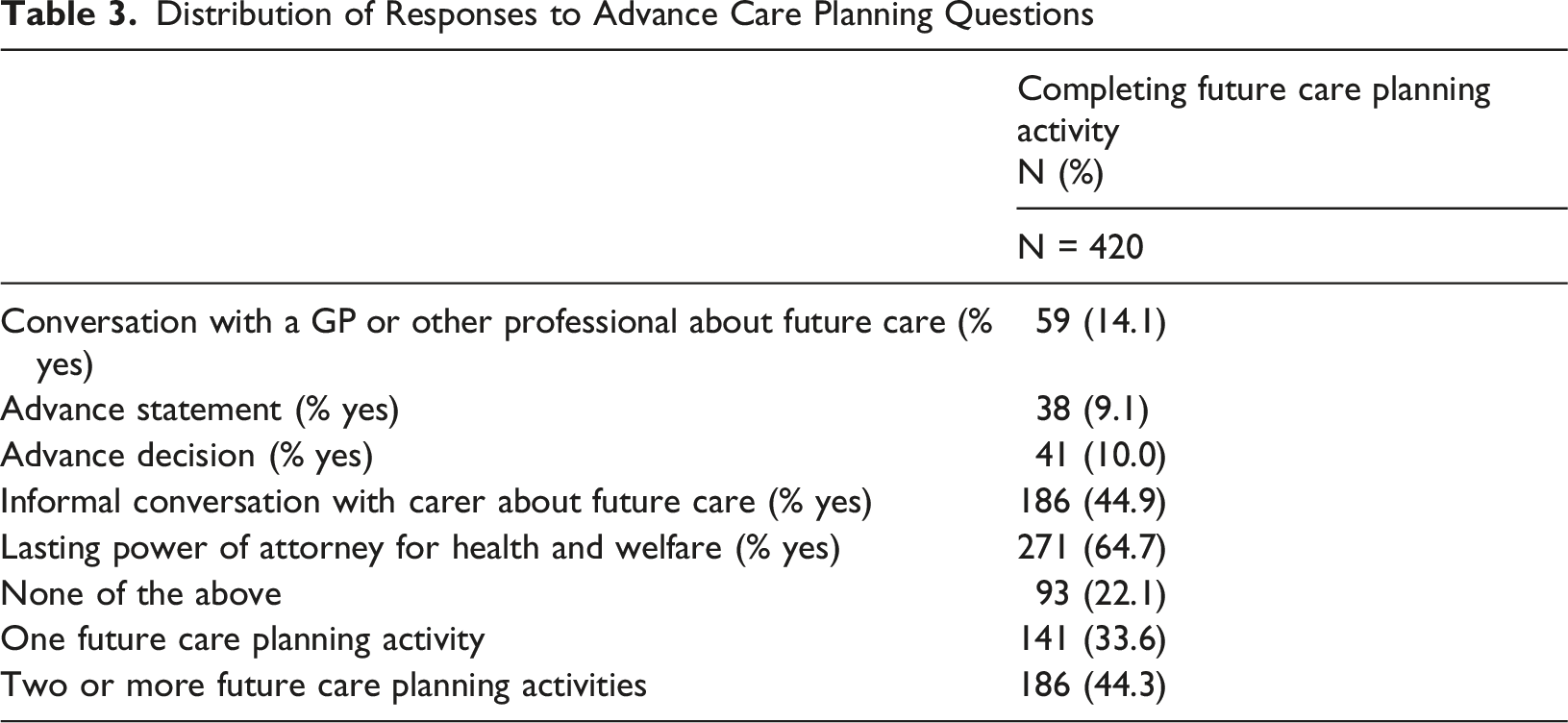
Lasting power of attorney for health and welfare was the most common activity. Although nearly two-thirds of the sample had one (64.7%), this still left around one in three without a legally appointed decision-maker. Notably too, even though two-thirds of the sample had a lasting power of attorney for health and welfare, only just over half of these (33.2%) had also had had an informal conversation with their carer. This may leave carers who are appointed as attorneys feeling unprepared for decision-making and vulnerable to the risk of decisional conflict and distress (Sellars et al., 2019).
Informal family conversations were reported by just under half (44.9%) of participants, although only 16.9% reported ‘definitely’ having such a conversation with the remainder (28%) reporting doing so only ‘to some degree’. While qualitative evidence suggests that much future care planning occurs informally in everyday conversations (e.g. de Vries & Drury-Ruddlesden, 2019; Dickinson et al., 2013; Ryan et al., 2017) our findings indicate that such discussions are not universal among people with dementia and their carers and may be limited in depth. Other forms of future care planning were less common; conversations with a GP or other professional occurred in just over 14% of cases, while advance statements and advance decisions were each reported by around 10%.
Overall, just under a quarter (22.1%) had undertaken no future care planning at all, not even by having an informal conversation with a carer. Including only informal conversations where participants had responded ‘definitely’ rather than just ‘to some degree’ increases this proportion to 29.3%. These various limitations in future care planning engagement increase the risk of crisis-driven decision-making and also sit uneasily alongside policy ambitions for early diagnosis to support timely, informed planning for people with dementia and their families (Hampel et al., 2022).
Carer-Related Factors That Support Planning
In several models, carer-related factors were associated with the outcome. One of these was educational attainment. Existing research finds an association between people with dementia’s higher educational attainment and advance care planning (Breslin et al., 2022; Gallagher et al., 2020; Hirschman et al., 2012), including in a meta-analysis across eight dementia-specific samples (Zhai et al., 2024). Our findings show a similar association with having an informal conversation, but in relation to the carer’s educational attainment rather than the person with dementia’s. This finding highlights the risk of health and care inequalities and emphasises the need to provide better support to help families initiate and sustain these conversations (Sussman et al., 2021; Van den Block, 2019).
Another factor was carers’ use of support and information services such as education groups, expert relative groups, advice lines, online support, Alzheimer’s Café, and/or an Admiral Nurse. This was strongly associated with having a lasting power of attorney for health and welfare and with having a conversation with a GP or other professional. Use of these services may have helped to inform, prompt and support carers so they could better assist their relative. For example, some dementia support services introduce advance care planning and then advise following up with a GP. However, it may also reflect carers' greater engagement, health literacy, and forward planning orientation more generally. In any case, these results suggest that engaged and well-supported carers are important in helping people with dementia undertake future care planning activities.
Coping Style
We found that having a lasting power of attorney for health and welfare was positively associated with carers having an avoidant coping style. This was unexpected. Although there is evidence that some people with dementia (Ashworth, 2020; Lai et al., 2019; Lemos Dekker & Bolt, 2022) and some carers (Sellars et al., 2019) prefer to avoid thinking about the future, avoidant coping is generally associated with less rather than more future care planning. One possible interpretation is that having a lasting power of attorney for health and welfare is more normative than other types of planning, such that it it captures a wide range of coping styles, including avoidant ones, rather than being driven by especially engaged planners. Establishing a lasting power of attorney for health and welfare is also bounded and procedurally discrete and, compared to other types of future care planning, can be low in requirements for reflecting on or discussing possible future health states. This is supported by the fact that only around half of those with a lasting power of attorney for health and welfare (51.3%) also reported an informal conversation with their carer, with only a fifth (19.7%) saying that they had ‘definitely’ had such a conversation.
Age, Severity of Dementia, Poor Quality of Life and Carer Burden
Having a conversation with a GP or other professional and having an advance statement were each associated with the person with dementia being older and having more severe dementia, suggesting that these activities tended to occur later in the illness trajectory. However, having a conversation with a GP or other professional was also associated with carers’ use of support and information services, suggesting that this particular activity was not driven by deterioration alone. Advance statements and advance decisions, however, both appeared to occur at points of strain or crisis; they were both associated with higher levels of carer burden, and advance decisions were also associated with the person with dementia having lower quality of life. In the existing literature, the relationship between carer burden and advance care planning remains unclear, with limited studies producing mixed findings (Kermel Schiffman & Werner, 2021; Kim et al., 2020). Evidence about quality of life and advance care planning is also not well-established, with only some limited evidence of an association with potentially related factors such as depression and anxiety (Dao-Tran et al., 2026; McMahan et al., 2020; Nakanishi et al., 2022). Taken together, these findings point to a pattern of late engagement, which may reflect both delays in initiation by professionals (Azizi et al., 2022; Dixon & Knapp, 2018; Tetrault et al., 2022; Visser et al., 2022) and/or preferences among some people with dementia and carers to defer planning (Ashworth, 2020; Lai et al., 2019).
On the other hand, we found that participation in an informal conversation about future care was strongly associated with having less severe dementia, as well as carers’ higher educational attainment, suggesting a more active role for people with dementia. This highlights the capacity of people with dementia to engage in early discussions when given appropriate relational support (Dixon et al., 2022).
The Role of Services in Implementing Advance Statements and Advance Decisions
Advance statements and advance decisions were strongly associated with memory assessment service area, with those in the South East having around four times the odds of an advance statement and nearly seven times the odds of an advance decision compared with the North East. This suggests a service effect, reflecting variation in professional involvement or practice between areas.
Socio-Economic Status
Those with a lasting power of attorney for health and welfare tended to be older and live in less deprived areas. It seems possible that those in less deprived areas may find the process of establishing a lasting power of attorney for health and welfare easier to navigate and be better able to meet the costs involved, which include a registration fee and, potentially, solicitors’ costs. Similar associations between socio-economic status and advance care planning are found in existing studies (Barwise et al., 2019; Davies et al., 2019; Nouri et al., 2020), although some targeted studies have found no association (Khosla et al., 2016). Area deprivation, however, is only one measure of socio-economic status, and findings may vary depending on how socio-economic status is operationalised. For dementia-specific samples, there is only evidence of an association with the potentially related factor of income, based on two studies in a recent meta-analysis (Zhai et al., 2024).
Factors That Were Not Statistically Significant
It is worth noting that many factors were not statistically significant in any of our multivariable models. Demographic factors included sex, despite existing research finding women more likely to engage with advance care planning (Baughman et al., 2024; Gallagher et al., 2022; Kalousová & Carr, 2024), including in dementia-specific samples (Zhai et al., 2024). Ethnicity was also non-significant, except in bivariate analysis with having a conversation with a GP or other professional. While some literature points to disparities (Hirschman et al., 2012; Inoue, 2016; Lovell & Yates, 2014; McDermott & Selman, 2018; Pettigrew et al., 2020; Sanders et al., 2016), including in dementia (van der Steen et al., 2014b), much of this evidence comes from the US (Crooks et al., 2023; Dixon et al., 2015; Zhai et al., 2024), with others arguing that differences by ethnicity commonly disappear when factors such as socioeconomic status and education are accounted for (Han & Nam, 2020).
We tested for a number of relationship-related factors that proved non-significant in multivariable models. These included the relationship of the carer to the person with dementia (spouse, son/daughter, other) despite existing evidence that offspring may be more comfortable discussing the future than spouses (Cheung et al., 2018). These also included the perceived quality of the relationship between the person with dementia and the carer (Positive Affect Index), despite some existing evidence that relationship quality may support advance care planning (Bloom & Fisher, 2021; Carr et al., 2013). The Lubben Social Network scale was also non-significant, except in bivariate analysis with having a lasting power of attorney for health and welfare, despite some existing evidence that carers with greater social capital and networks are better positioned to plan for future care (Miyashita et al., 2019).
Optimism (LOT-R) was also non-significant in multivariable models, as was having more comorbid health conditions (CCI), supporting existing evidence of no relationship (Krishnappa et al., 2023). Finally, provision of information at diagnosis about dementia or advance care planning was non-significant in multivariable models, despite existing evidence that poor understanding is a barrier to engagement (Lai et al., 2019). This may, however, not be because information is not important, but may be because people feel overwhelmed at this time and cannot absorb all the information they receive (Dixon et al., 2025; Song et al., 2024) or because they find the information they receive difficult to understand or act on (Dixon et al., 2025; Mansfield et al., 2022).
Summary and Implications for Policy
People with dementia should have the opportunity to help plan their future care, starting early in the disease trajectory and contributing for as long as possible (Van den Block, 2019; van der Steen et al., 2014a, 2024). Our findings indicate that within the important first 18 months following diagnosis many people with dementia are not undertaking any planning for their future care at all, not even through informal conversations with their carers. Lasting power of attorney for health and welfare was the most common planning activity but these often appeared not to be underpinned by conversations with carers about preferences for care, leaving carers vulnerable to the risk of later decisional uncertainty, burden and distress (Sellars et al., 2019). Our findings echo those found in other studies showing professional support for future care planning tending to occur late, at points of health deterioration and carer strain (Azizi et al., 2022; Dixon & Knapp, 2018; Tetrault et al., 2022; Visser et al., 2022). Our findings also add to growing evidence that carer characteristics significantly influence whether and how people with dementia plan for future care (van der Steen et al., 2014b). This suggests a potential for inequalities in access and emphasises the need to develop more relational approaches (Colclough et al., 2023; Malhotra, 2023; Phenwan et al., 2025; Sussman et al., 2021).
Supporting people to initiate and sustain informal conversations about future care may be especially valuable (Van den Block, 2019). This may help to improve the quality of formal processes, ensuring they are more relationally grounded and lay ground for evolving discussions, both within families and potentially with professionals, allowing people with dementia to continue to express their wishes even as their capacity diminishes (Phenwan et al., 2025; Ryan, 2020; van der Steen et al., 2024). Such conversations may also better position carers for in-the-moment decision-making when the need arises (Malhotra, 2023; Phenwan et al., 2025). Our findings draw attention to the need for good quality support for carers (Malhotra, 2023; Van den Block, 2019; van der Steen et al., 2024) and targeted support for those without carers (Cudjoe et al., 2020).
Strengths and Limitations
Much existing evidence focuses on formal advance care planning, with US-based studies dominant. Our study contributes new evidence from a large cohort of dyads of people with dementia and carers in England and additionally includes factors associated with informal conversations with carers about future care. The inclusion of person with dementia and carer factors in the same models allows for an examination of their relative contributions. Limitations include analyses being restricted to dyads providing data at two time points. Comparison of the analytic sample of dyads with those dyads not retained suggested some differences in age, housing tenure, ethnicity, marital status, and carer relationship to person with dementia, indicating that findings may not be fully generalisable to all people recently diagnosed with dementia and their carers. Equally we did not include people with dementia without a participating carer, who may differ in their future planning. We were also limited by variables available in the DETERMIND dataset. Although our analysis uses data from two time points, all analyses are cross-sectional and causal inferences cannot be made. We have not tested lagged effects or attempted to model causal relationships. Further analysis is required to better understand the causal pathways between the various factors and approaches to future care planning; these are planned with data covering further waves of assessment.
Conclusion
The exploratory analyses presented in this paper extend existing evidence by conceptualising future care planning as a relational process, modelling characteristics of people with dementia and carers together to assess their relative contributions. It also extends existing evidence by examining informal conversations with carers alongside conversations with professionals and documented advance care planning.
We found lasting power of attorney for health and welfare to be common but frequently not underpinned with meaningful discussion with carers, while informal conversations with carers remained limited and professional involvement reactive, occurring late in the trajectory. Pro-active planning is strongly shaped by carer resources, raising concerns about inequalities of access. Our findings suggest a need for more relational approaches to future care planning, including support for informal conversations, high-quality carer support, timely and consistent professional involvement and additional support for those without close carers.
Supplemental Material
Supplemental Material - Factors Associated With Advance Care Planning and Informal Family Discussions About Future Care in a UK Cohort of People With Dementia and Their Carers From the Observational DETERMIND Study
Supplemental Material for Factors Associated With Advance Care Planning and Informal Family Discussions About Future Care in a UK Cohort of People With Dementia and Their Carers From the Observational DETERMIND Study by Josie Dixon, King Derek, Ben Hicks, Sube Banerjee in Dementia
Footnotes
Acknowledgments
We are deeply grateful to everyone involved in the DETERMIND study, which made this linked study possible and all people with dementia and carers who took part. We are also grateful to the Alzheimer’s Society for their ongoing support.
Ethical Considerations
This research was conducted in accordance with relevant guidelines and regulations with ethical approval provided by the Health Research Authority (HRA) Social Care Research Ethics Committee (SCREC), Reference: 19/IEC08/0048.
Consent to Participate
Informed consent was obtained from all participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The DETERMIND Programme was funded by the Economic and Social Research Council (ESRC), grant reference ES/S010351/1. This linked study was funded by the Alzheimer’s Society, Grant reference: 401 (AS-PG-17b-015).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
DETERMIND data will be made publicly available by 2028. In the meantime, data can be made available on request by contacting Sube Banerjee. Faculty of Medicine and Health Sciences, The University of Nottingham, Nottingham, UK.
Supplemental Material
Supplemental material for this article is available online.
Note
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.