
Abstract
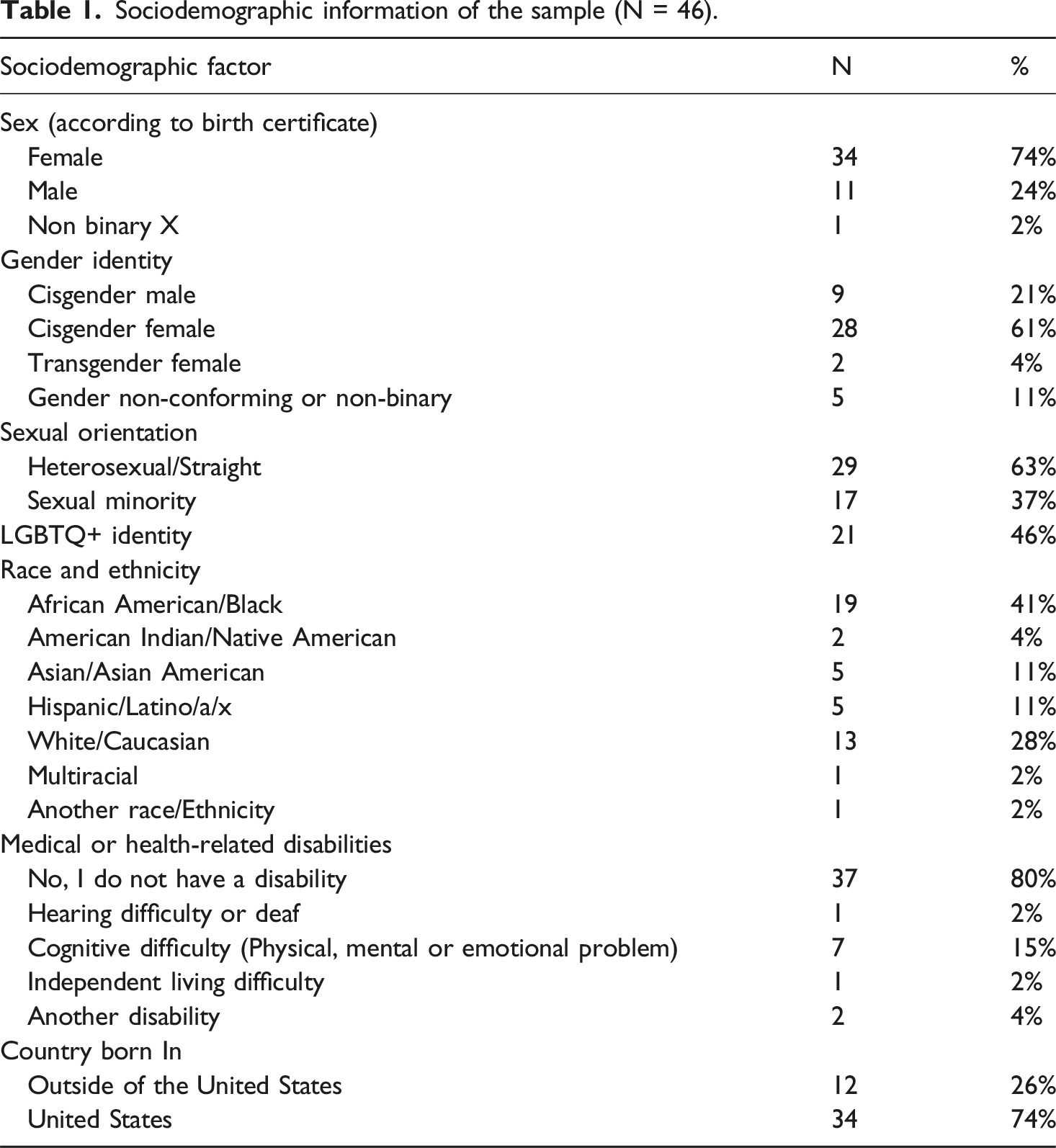
Survivors of intimate partner violence (IPV) may seek formal support across systems of care; however, those with marginalized identities, and from rural communities, may also experience more barriers while seeking help. The current study highlights findings from 13 focus groups in a needs assessment of domestic violence services in Illinois. Participants included 46 survivors of IPV who accessed formal supports in urban and rural communities; they were diverse in terms of gender (61% cisgender female, 21% cisgender male, 15% transgender/gender non-conforming), sexual identity (37% sexual minority), and race/ethnicity (41% African American/Black, 28% White, 11% Asian/Asian American, and 11% Hispanic/Latino/a/x); 26% were an immigrant and 20% had a disability. Through reflexive thematic analysis, this study highlighted the complexities of help-seeking and attainment through nine themes related to barriers. Intertwined in these barriers were aspects related to one’s identity or geography. For example, there was a lack of cultural awareness and trust within services, issues with accessibility, and perceptions of shame and stigma. Among barriers noted, many survivors were navigating formal structures that were oppressive and harmful, contributing to feelings of dehumanization. More research is necessary to continue examining intersectional identities and communities that remain at the margin of IPV services. Results highlight the urgent need to strengthen the coordination of services, emphasizing the necessity of DV advocates, and urging providers to deliver more inclusive and culturally responsive services.
Intimate partner violence (IPV), which falls under the larger umbrella of domestic violence (DV), includes physical, sexual, psychological, and financial forms of abuse from a current or previous intimate partner. Experiencing IPV can result in numerous adverse outcomes, including survivors’ physical health (Stubbs and Szoeke, 2022) and mental health (e.g., depression, post-traumatic stress disorder, and suicidality (White et al., 2024), as well as economic impacts (e.g., service expenditures, reduced productivity; Chan and Cho, 2010). Individuals who experience IPV (i.e., referred to in this paper as survivors), may seek support from direct service agencies and community-based organizations, police or law enforcement, criminal and legal systems, and medical or healthcare providers. Across these formal supports, survivors may utilize counseling services, seek legal orders of protection, engage in safety planning, seek temporary food or housing, participate in cash transfer programs, apply for housing assistance and family support services, or receive legal and medical advocacy. Survivors also may seek support, information, and referrals through helplines or hotlines.
However, access and perceptions of these services vary by geographic location and intersections of survivors’ identities. For example, Hulley et al. (2023) found that survivors with marginalized identities were less likely to access formal services due to perceptions of institutional racism, immigration laws, and a lack of culturally responsive services. Survivors in rural areas have fewer available, accessible, and quality IPV services (Edwards, 2015) and they may face additional barriers in accessing services if also experiencing poverty or are survivors of color (Collins Woods, 2020).
Receiving formal support can increase overall mental health and wellbeing among survivors (Sullivan, 2018), particularly when they are provided with holistic, individualized, and trauma-informed support (Paphitis et al., 2022). Survivors also may seek informal support from family or friends. When informal supports believe the survivor and validate their experiences, it can increase their overall psychological health benefits (Sylaska and Edwards, 2014). Thus, it is crucial to understand the help-seeking journey among IPV survivors, especially those with intersecting marginalized identities and from diverse geographical areas.
The current study sought to explore the help-seeking journey among IPV survivors in Illinois who sought formal help. Specifically, we purposively sampled survivors with one or more marginalized identities (in terms of gender identity, race/ethnicity, sexual orientation, if they had a disability, or if they were an immigrant) and geography (e.g., rural), given that researchers find that survivors with multiple marginalized identities have a higher risk of experiencing violence (e.g., Collins Woods, 2020; Gill, 2018). Survivors living in rural communities also may face a greater risk for chronic, severe forms of IPV (Edwards, 2015). As Gill (2018) highlights, IPV research needs to engage in intersectional, community-based research, to fully move the fields of violence prevention and service provision forward.
The help-seeking journey
Models of help-seeking among IPV survivors describe a journey that often is multi-directional and cyclical as survivors’ perceptions of these various steps can alter, stop, or restart the journey at man points. Help-seeking among IPV survivors has often been guided by Liang et al. (2005) model of help-seeking and change, which included defining and recognizing IPV within a relationship, deciding to get help, and selecting someone for support, all of which are influenced by individual, interpersonal, and sociocultural factors. Kennedy and colleagues (2012) expanded this model to include perceptions of one’s needs, availability, and fit of options for help; help-attainment and if needs were met; facilitators and barriers to accessing and getting help; and impacts to mental health. It also contextualizes the process, and the cumulative impact of help-seeking and attainment, by including the role of one’s social location, community context and resource availability, situational and developmental context, and prior and cumulative victimization and adversity.
Another core aspect of help-seeking is survivors’ perceptions of provider trustworthiness (i.e., benevolence, fairness, and competence) and the trust a survivor has in services (Kennedy et al., 2024). Without these elements, service providers are unable to meet a survivors’ needs (e.g., providers are untrained, and services are incongruent with survivors’ culture or values) and may be perceived as uncaring, discriminatory, or harmful, and these experiences can re-victimize the survivor. Thus, Kennedy and colleagues (2024) call for a greater focus on developing, strengthening, or rebuilding provider and service trustworthiness for IPV survivors.
These models illustrate the complexities of help-seeking processes; however, while some survivors may choose to seek formal supports, others may seek support from friends and family, others may report or disclose abuse after time has passed, and others may not choose to tell anybody about their experiences (McCart et al., 2010; Nally et al., 2021). In a recent study of survivors, 50% sought help from both formal and informal networks, 15% primarily sought support from informal supports, and 35% engaged formal systems but largely avoided legal systems (Cheng et al., 2022). Given that many survivors seek help from informal supports, more efforts are occurring to increase informal supporters’ responses to IPV disclosure (e.g., Schucan Bird et al., 2024).
Barriers to help-seeking
Barriers exist for accessing IPV services in the United States, including lack of awareness, access challenges, consequences of disclosure, lack of material resources, personal barriers, and system failures (for a review see Robinson et al., 2021). Survivors may perceive stigma related to reaching out for support (Overstreet and Quinn, 2013). They may not access formal services because they do not know about the services available to them, they do not know how to access them, and/or they do not feel safe or comfortable accessing them (Houston-Kolnik et al., 2017). Other barriers include emotional barriers (e.g., fear of retaliation, shame and embarrassment) and instrumental barriers (e.g., housing or financial concerns, deportation concerns, language and cultural barriers, and law of awareness and knowledge; McCart et al., 2010).
Intersecting marginalized identities and help-seeking
Models of help-seeking and attainment are also expanding to capture the impacts that marginalized identities can play in navigating formal systems of care. For example, White women may be more likely to seek mental health and social services, while Latina/Hispanic and African American women may be more likely to seek supports from hospitals or law enforcement (Satyen et al., 2018). Among cisgender, heterosexual men who have experienced IPV, (Lysova et al., 2022) found internal barriers related to masculine stereotypes, male roles, and not recognizing or defining IPV, as well as external barriers related to fear and not feeling like there were places to seek help. Taylor et al. (2021) also found gender stigma and discreditation as barriers to help-seeking and the responses they received from service providers. Hardesty and colleagues (2011) illuminated the help-seeking process among lesbian and bisexual mothers, highlighting barriers and experiences with discrimination and oppressive systems, especially if they were women of color or were of low socio-economic status.
Kimberlé introduction of intersectionality focused on Black women’s experiences in navigating IPV and the associated oppressions with intersecting identities, such as race, class, and gender. Her seminal work highlights that many structures designed to support survivors of IPV (e.g., many for White, middle-class, cisgender women, who are non-immigrant), may not be accessible or relevant to someone with intersecting marginalized identities, or someone who does not fit this cultural expectation of what a survivor looks like. For example, survivors in rural areas who are low-income may not be able to afford to travel to a shelter or take time off work to access services or go to court hearings. A survivor who does not speak English, or a survivor with a hearing disability, may not be able to access services if the provider does not have interpretation or translation services. A cisgender male, transgender, or gender non-conforming survivor may not know if they can access services if they are advertised “for women.”
Overstreet and Quinn (2013) presented the IPV Stigmatization Model, which identified how cultural stigma (i.e., societal beliefs that can lead to questioning the legitimization of IPV), stigma internalization (i.e., survivors believing and internalizing stereotypes about IPV survivors) and anticipated stigma (i.e., fear of what will happen when they disclose IPV) contribute to help-seeking. Additionally, the impacts of IPV and the stigmas of help-seeking can be further compounded for those with intersecting marginalized identities, as each of these identities are stigmatized. Waller et al. (2023) developed a theory of help-seeking with African American women, highlighting the ways in which race, gender, and class intersect to impact help-seeking among IPV survivors. This theory includes social and cultural context (e.g., systemic racism, community influences), beliefs about available services (e.g., historical and current experiences), and individual agency (e.g., self-efficacy and strengthen to seek help). This theory also elevates the importance of examining intersectional experiences resulting from navigating oppressive systems and policies (Waller et al., 2023).
Sweet (2019) highlights the “paradox of legibility” as women’s experiences with IPV are so intermeshed within structures that can be oppressive and amplify harm. They can be “objectified and discredited in court,” “subject to gendered standards of respectability uncommon for other crimes” and must show they are on the path from powerless to productivity to be deserving of services and supports (Sweet, 2019: 413–414). Thus, the paradox is survivors’ journey of finding credibility and deserving of services while also navigating institutional barriers and oppression.
The impact of rurality and geographic location
Research is needed to understand the impact to help-seeking from the intersection of geographic location and rurality with these marginalized identities. Peek-Asa et al. (2011) found that the average distance to an IPV-specific shelter or resource was three times greater for cisgender women living in rural areas, compared to those living in urban areas. Edwards (2015) reviewed the literature, finding that multiracial women, and those separated or divorced, who were living in rural areas were at a greater risk for IPV (than similar groups in urban areas). They also found that survivors have worse health outcomes because of the lack of IPV services, in terms of availability, accessibility, and quality of services. Further, women living in rural areas may perceive stigma about accessing services, and not reach out for formal support (Edwards, 2015). Survivors living in rural geographies face additional barriers in accessing services if they experience poverty or are survivors of color (Collins Woods, 2020). Research is needed to understand the rural help-seeking experience among more diverse samples, especially those with intersecting marginalized identities.
Current study
The IPV help-seeking and attainment journey highlights the personal, situational, cultural, and systemic barriers and facilitators of support. Models of help-seeking have been expanded to illuminate the oppressive systems and policies that survivors with one or more marginalized identities navigate. Among survivors, accessing formal supports does not always result in the care or support that is needed. Research is needed to continue learning about help-seeking from diverse samples of survivors, including intersections of survivors of color, survivors with disabilities, survivors from the Lesbian, Gay, Bisexual, Transgender, Queer, and other sexual and gender identities (LGBTQ+) community, immigrants, and those from rural communities.
The main study objectives included conducting focus groups with survivors who have accessed IPV services to hear their perspectives about these services. Survivors were asked about: (1) Their help-seeking processes with formal systems, including perceptions of services and supports, as well as barriers encountered when accessing formal services; and (2) How aspects of identity affected the services received.
Methods
Study design
The research team worked with DV agencies and community-based organizations to share information about the study. Partners were asked to post flyers at their organizations or on their organizations’ social media pages. We recruited from all member organizations from the Illinois Coalition Against Domestic Violence (ICADV), as well as from LGBTQ+ organizations, refugee centers, and cultural centers. In the flyers, we let individuals know that we were seeking input from adults (ages 18+) who lived in Illinois and had experienced IPV. If adults were interested, they were asked to complete a brief screening survey to assess their eligibility. Inclusion criteria was comprised of the following: they must be 18 years of age or older; they must reside within the state of Illinois; and they must have experienced IPV (for IPV items on the screening survey see Supplemental Materials).
The research team assessed those who completed the screening survey for eligibility inclusion criteria, and then purposive sampling methods were utilized. Within each geographic region of Illinois (Southern, Central, Northern, Northern-Collar/Cook), and we selected two to three participants who identified: (a) as a racial or ethnic minority, (b) LGBTQ+, (c) with a disability, or (d) as an immigrant. If they met criteria and were purposively sampled, they were sent a follow-up email invitation and online informed consent form.
Screening and participation rates
Of the 219 individuals who completed the screening survey, 101 were invited to participate in a focus group. Of the 101 invitations, 46 individuals completed the online consent form and participated in a focus group (46% participation rate). Participants engaged in one of the 13 focus groups conducted by the research team. Based on scheduling needs and logistics (e.g., travel, childcare, work schedules), focus groups either took place in person (n = 1) or online via Zoom (n = 12). Focus groups took approximately 75 minutes to complete. Most focus groups had 3–4 individuals who participated; the largest focus group had 7 participants. One trained facilitator led the focus group, and 1–2 notetakers were also present. All focus groups were audio recorded for transcription purposes. After the focus groups, participants were sent a brief survey to complete, which took about 15 minutes. After the focus group and surveys were completed, participants were sent a list of resources and their payment of $40 (cash for in-person participants; Amazon e-code for online participants). All focus group facilitators and notetakers on the research team were mandated reporters, trained on focus group facilitation, and had completed the ICADV Domestic Violence Foundations 20-Hour Online Training. All research procedures were approved by a university Institutional Review Board.
Focus group participants
The 46 survivors who participated in a focus group represented 12 counties across Illinois, including from Chicago, Cook, and Collar areas (n = 26), Northern (n = 4), Central (n = 13), or Southern Illinois (n = 3). About 37% of participants were from rural communities. The participants ranged in age from 22 to 59 (M = 33.87, SD = 9.53). Participants reported a diverse level of educational attainment (61% had an associate’s degree or higher), employment (34% were employed part-time and 32% were employed full-time), and current housing (64% were currently renting housing). The average gross household income was $44,686, and the median was $32,500. In terms of relationship status, 43% were divorced or separated, 25% were single or not in a relationship, 18% were in a relationship, 9% were married, and 4% were in an open relationship. About 35% were living with biological children or stepchildren. About 33% of participants indicated involvement with the criminal legal system (e.g., arrested, jailed, detained, or incarcerated, on probation or parole, etc.).
Sociodemographic information of the sample (N = 46).
Instruments: Focus group protocol
For the focus group, a semi-structured focus group protocol was developed collaboratively between ICADV and the research team. After study information was provided, participants answered 12 overarching questions. For the purposes of this study, we focused on questions related to seeking help (e.g., “When you were seeking help, did you receive the help you needed?”) and identity (e.g., “How might aspects of your identity (i.e., race or cultural background and values; gender identity; sexual orientation; having a disability; being an immigrant) have affected the services you received?”). The full focus group protocol can be found in Supplemental Materials.
Data analysis
Descriptive information about experiences with IPV and help-seeking were examined from the screening surveys using SPSS software. All focus group sessions were audio-recorded and files were transcribed. After transcription, they were verified and de-identified; after confirmation, audio files were deleted. Data analysis was conducted with de-identified transcript files and qualitative codebooks were created. Reflexive thematic analysis (Braun and Clarke, 2006, 2020) was used to identify themes (i.e., group of categories that convey similar meanings) with the qualitative data. Two trained coders reviewed the data for themes, defined and named the themes, and discussed any disagreements on coding. All of this information was carefully tracked in the codebook. For any quotes used in this paper, pseudonyms are provided, with information on gender identity, sexual orientation, race or ethnicity, disability, if they are an immigrant, and if they live in a rural or urban community, are listed. Fue to small sample sizes within characteristics, and to protect participant information, we collapsed “transgender, gender non-binary and gender non-conforming” into one category, grouped “gay/bisexual” and “lesbian/bisexual” and listed “racial minority” if they wrote in a racial identity that did not fit into other categories. We also did not assess region differences and rather grouped into “rural” or “urban” communities to ensure these data were de-identified.
Results
Experiences with DV and help-seeking
Prevalence of experiencing forms of intimate partner violence (IPV; N = 46).
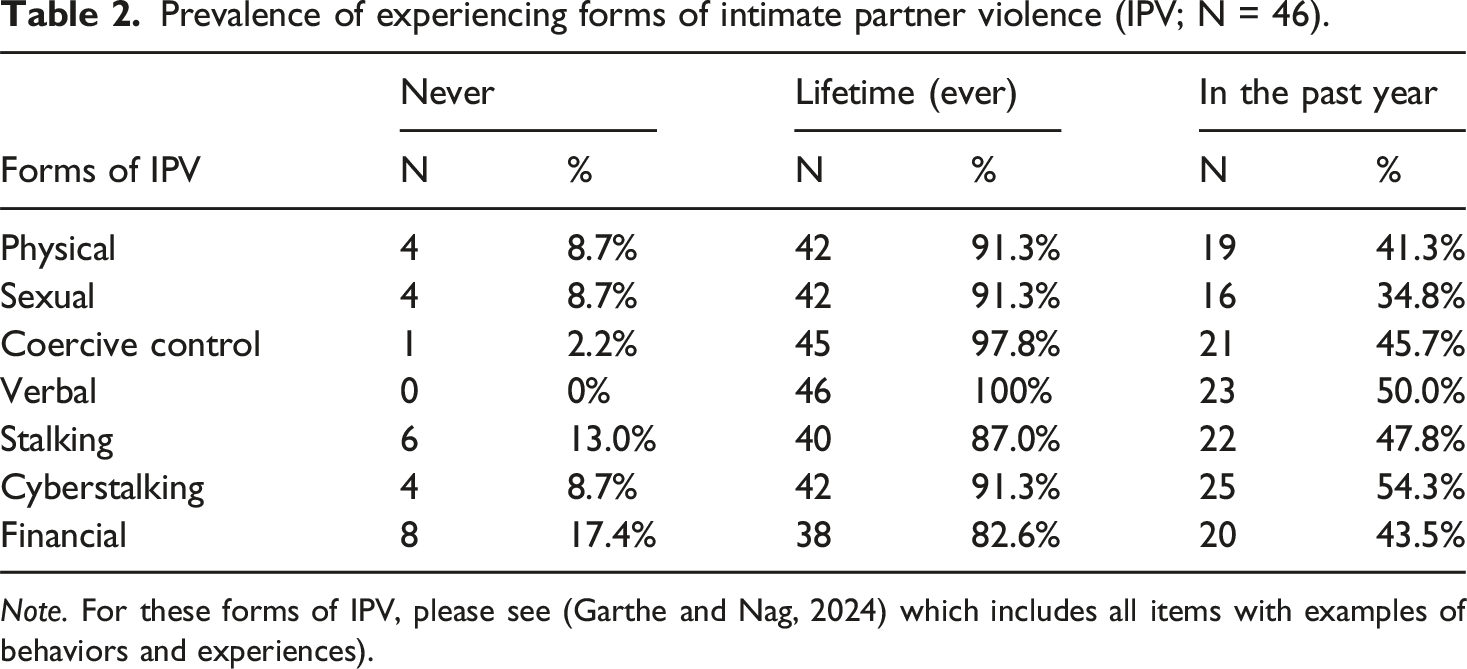
Note. For these forms of IPV, please see (Garthe and Nag, 2024) which includes all items with examples of behaviors and experiences).
Prevalence of help-seeking from formal and informal supports (N = 46).
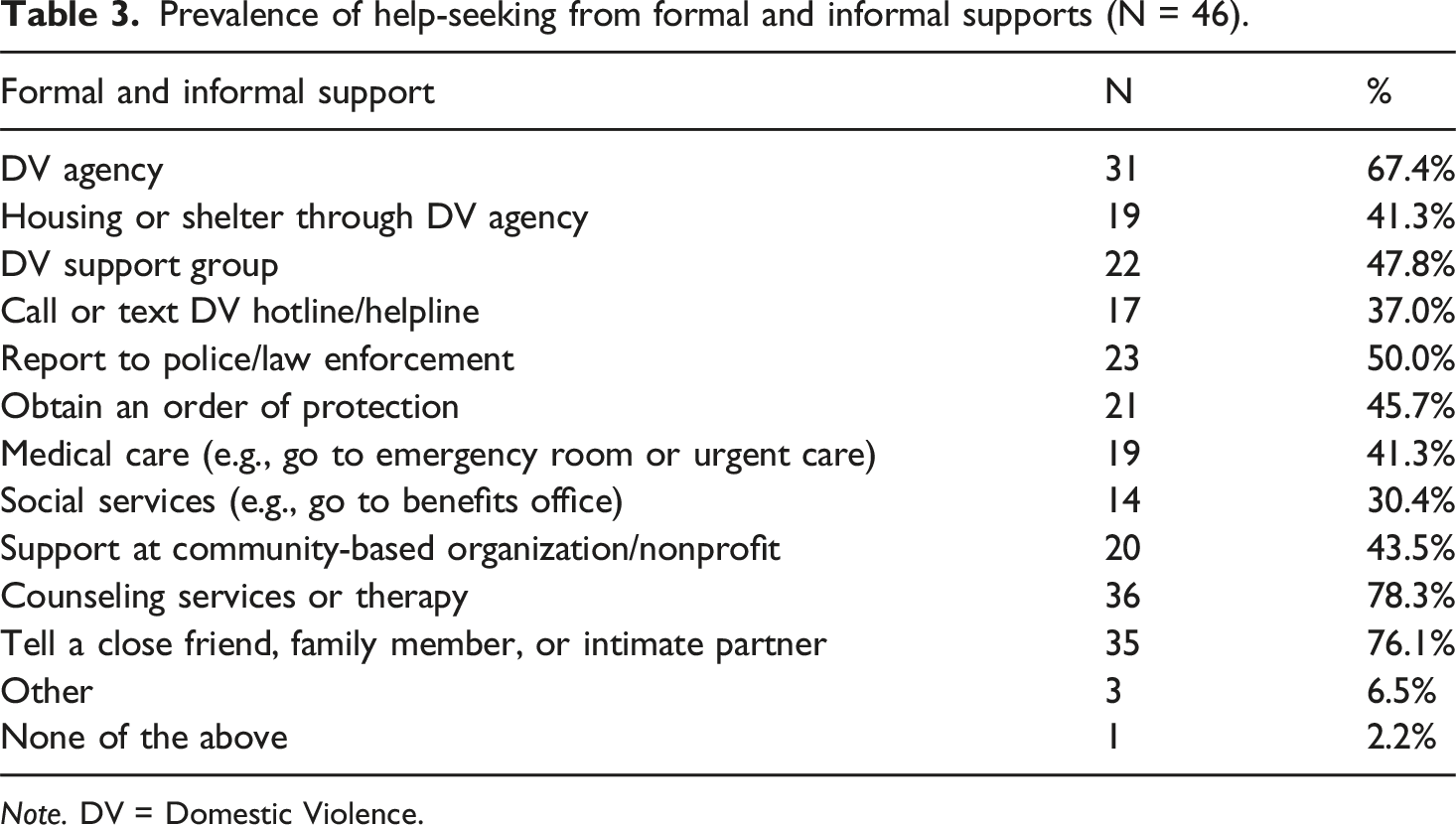
Note. DV = Domestic Violence.
Formal supports sought by participants (N = 46).
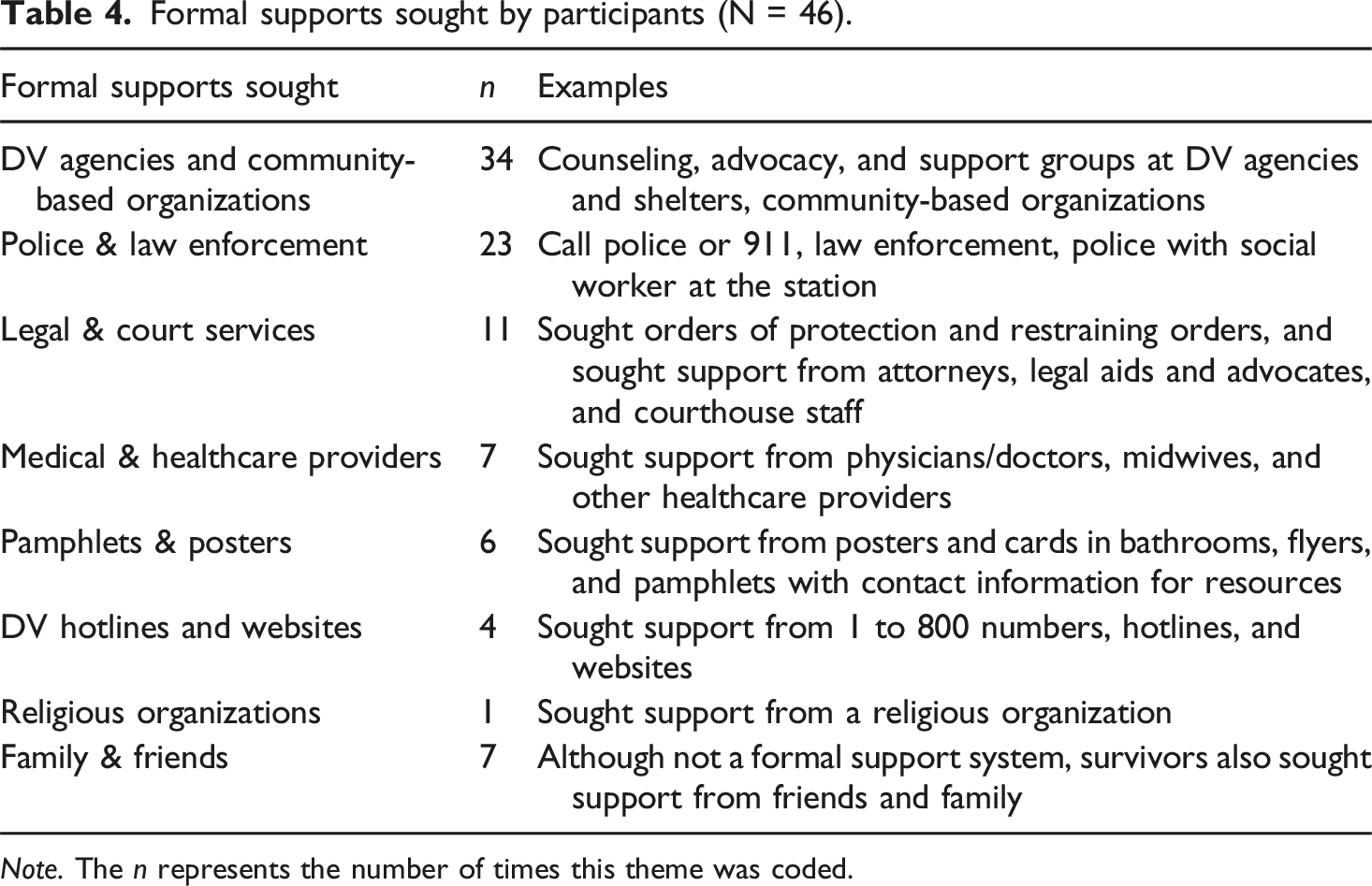
Note. The n represents the number of times this theme was coded.
Complexities of help-seeking
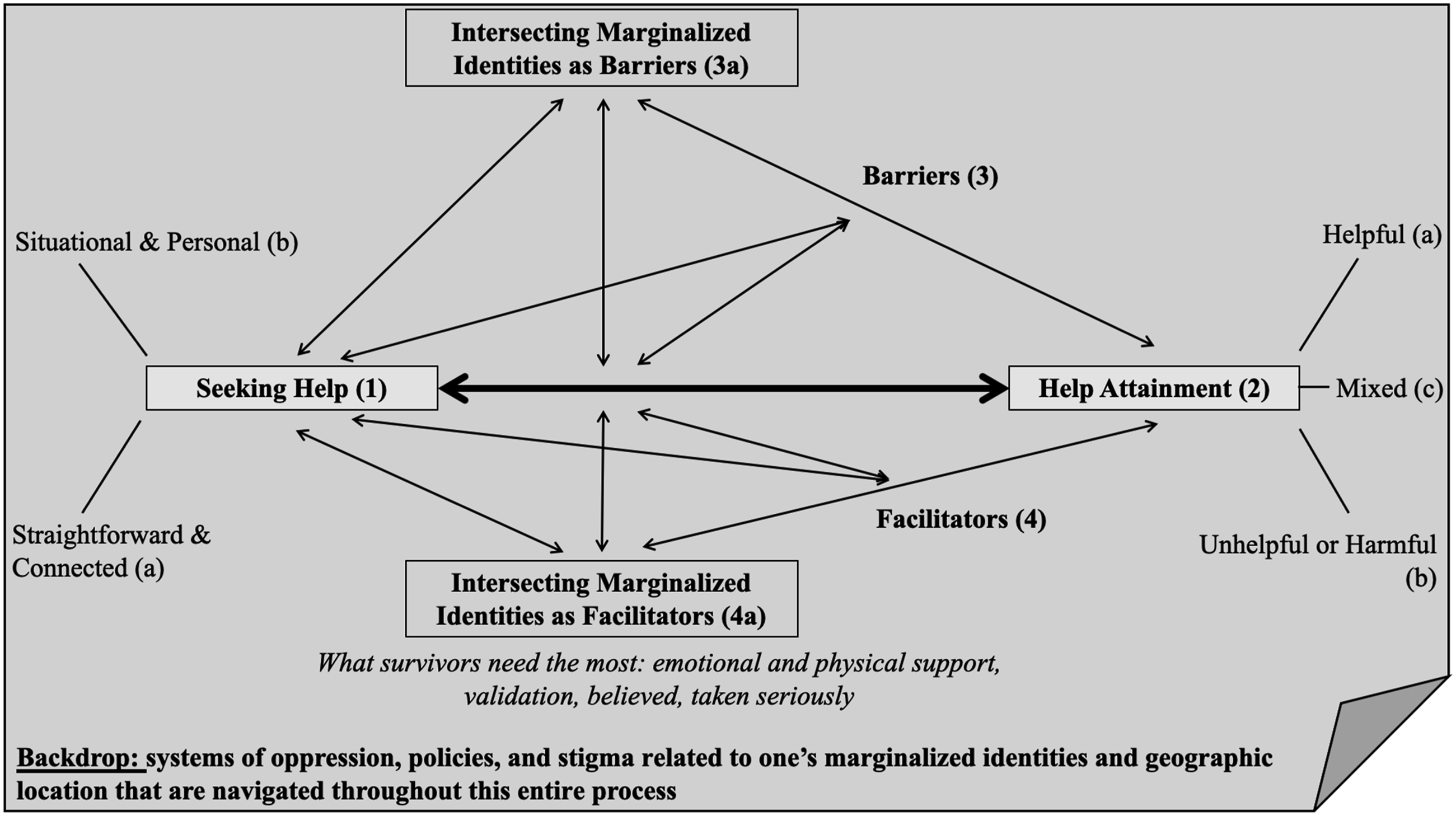
To organize our findings, Figure 1 highlights process of seeking help and help attainment. Each part of this model is discussed below, labeled with numbers and letters in the figure that correspond to the organization of this section. The backdrop for this figure is the systems of oppression, policies, and stigma related to one’s marginalized identities or geographic location that are navigated throughout this entire process. Survivors sometimes named or attributed these systemic or structural components as barriers in the help-seeking journey. However, even if not named, this sample of diverse survivors with multiple marginalized identities and geographic locations are unable to disentangle from the systems and structures in which formal IPV services and supports exist (and thus, are the backdrop of our results). (1) Seeking help: First, survivors were asked about the formal supports they sought help from. As shown in Table 4, most survivors (n = 34) sought help from DV agencies and community-based organizations, followed by police and law enforcement (n = 23). Also, about one in four survivors sought an order of protection or other legal services. Accessing these formal supports was described as a journey, and it was clear that the help-seeking process was not linear. Each journey depended on immediate needs, the survivors’ identity and geographic location, what was available, or who survivors chose to reach out to first. Journeys also depended on knowledge of services and supports, as well as the knowledge of providers across systems. (a) Straightforward and connected: Some survivors described the help-seeking process as relatively straightforward, and providers across systems helped connect the survivor to additional resources and supports. For example, several survivors talked about how they would reach out to a legal system, which would lead them to DV agencies and other social services. Others called hotlines or reached out to DV agencies who connected them to additional services (e.g., orders of protection, mental health supports). So, when services were well-connected within a community, this facilitated the help-seeking process. “I called domestic violence shelter hotlines and stuff like that. And usually they are pretty helpful at connecting me to resources. And also walking into the courthouse to file an order of protection. I was matched with a really helpful court [advocate] that helped me file the paperwork. And that was also a resource that I was really glad that I ended up having which isn't something I had thought to even look for.” – Millie, a cisgender woman, identified as lesbian/bisexual, White race, from an urban community A visual representation of the results illustrating the help-seeking and help attainment process.
(b) Situational and Personal: While some had straightforward connections and handoffs in their journey, others described it as more complex depending on their personal situations:
“Each kind of different person led me to a different branch. Once the counselor had told me she thought that the relationship was escalating, and was afraid for us, that led me to seek out shelters, but that was a rabbit hole in itself, because […] at each stage, it was a little different. And not always clear. Pretty long journey.” – Cloe, a cisgender woman, identified as lesbian/bisexual, White race, from an urban community
Personal journeys also included complex abusive situations, and reaching out for help did not always result in immediate help. One survivor described reaching out to her midwife, as she was the only person the survivor could visit without her husband there. The midwife was able to provide a phone number, but there was not much the survivor could do with that when every phone call she made was tracked. In this story, Penelope felt that “maybe I would have been able to leave sooner” if medical providers were more equipped for supporting survivors - Penelope, a cisgender woman, heterosexual, White race, from a rural community. (2) Help attainment: In relation to asking about seeking help, we asked survivors if they felt they received the help they needed. While a good number felt they did, there was also a handful of survivors who felt mixed support (e.g., not every need was addressed). Also, many discussions focused on survivors who did not feel they received the help they needed, often reflecting on barriers (described in the next section). Across help that was attained, survivors described services as helpful, harmful or unhelpful, or mixed. (a) Helpful: Overall, when survivors sought support from DV agencies and mental health providers, they felt these services were helpful, vitally important, reassuring, and validating. Four survivors specifically discussed the help they received from DV shelters. Four other survivors mentioned the importance of having advocates to guide them every step of the way and having advocates in law enforcement and legal settings. Survivors highlighted the helpfulness of services from providers within their own communities. (b) Unhelpful or harmful: Survivors felt that they did not receive the help they needed from law enforcement (n = 7), courts (n = 5), or either legal system (n = 2). These survivors discussed feeling forced into adversarial scenarios, coercive situations within systems, police not enforcing orders of protection, and not feeling cared for, describing the legal system as dehumanizing. Survivors who did not receive help from DV agencies (n = 5) also noted the difficulties qualifying for housing or other services. Survivors also disclosed how certain services were not viable due to children, housing barriers, how police questioned them, and some had to seek services at different organizations (e.g., one couldn’t obtain housing due to long waitlists, so found housing through refugee center). Barriers are highlighted again in the next section that contributed to these feelings of unhelpful or harmful outcomes. (c) Mixed: For others, the support or services they received was a mixture of helpful and unhelpful. Some survivors felt that services were not particularly helpful at various stages, while others were, or the systems were too difficult to navigate along the way. Three survivors discussed how help felt temporary and did not help in the long-term. (3) Barriers: We specifically asked survivors about barriers to accessing services. Accessibility barriers (n = 20) were described the most in focus groups, including access to DV shelters, transportation, time to respond, waitlists, and policy criteria and eligibility restrictions. In addition to accessibility barriers, other barriers included perceptions of stigma, shame, fear of retaliation; barriers within formal systems; mental health concerns; their partner was a barrier; financial barriers; language, cultural, identity and social barriers; and not being believed or questioned. Aspects of this sample of survivors’ intersecting marginalized identities were woven throughout these types of barriers. For example, survivors from rural communities highlighted barriers related to transportation and access to shelters, fear that everyone in their town would know about the situation, having family or friends related to the perpetrator working in systems of care. These barriers were exacerbated when survivors from rural geographies were cisgender men or gender non-binary. For example, not only were there fewer shelters for survivors in rural communities, but even fewer options for cisgender men to utilize.
Additionally, survivors discussed specific barriers related to their identities, including lack of translators, languages used, and cultural differences in disclosing IPV. There were feelings of stigma and shame that were intertwined with their identity, family values and beliefs, and fear of provider perceptions. Across discussions where there were barriers within formal law enforcement and legal systems, lack of trust and care was discussed, in addition to fear of discrimination.
Across these discussions of barriers (see Table 5), most survivors noted multiple barriers occurring at once, further adding to the complexity of the help-seeking process. For example, as Cam describes, these multiple barriers cumulatively impacted their help-seeking process: “I faced some stigma, some setbacks, some issues being neglected, and stereotypes accessing services. I had fears of not being understood, fears of not seeking the necessary help, and I felt that I might not get a positive outcome in my situation. I felt depressed, I lacked an approach on how to relate this information to [the advocates] and felt they might not really understand at some point. This caused me to isolate myself, and I felt lonely.” – Cam, identifies as gender non-binary and heterosexual, Black race, from a rural community, immigrant Barriers experienced during the help-seeking process (N = 46). Note. The n represents the number of times this theme was coded. Aspects of One’s identity or identities that impacted help-seeking and services (N = 46). Note. The n represents the number of times this theme was coded.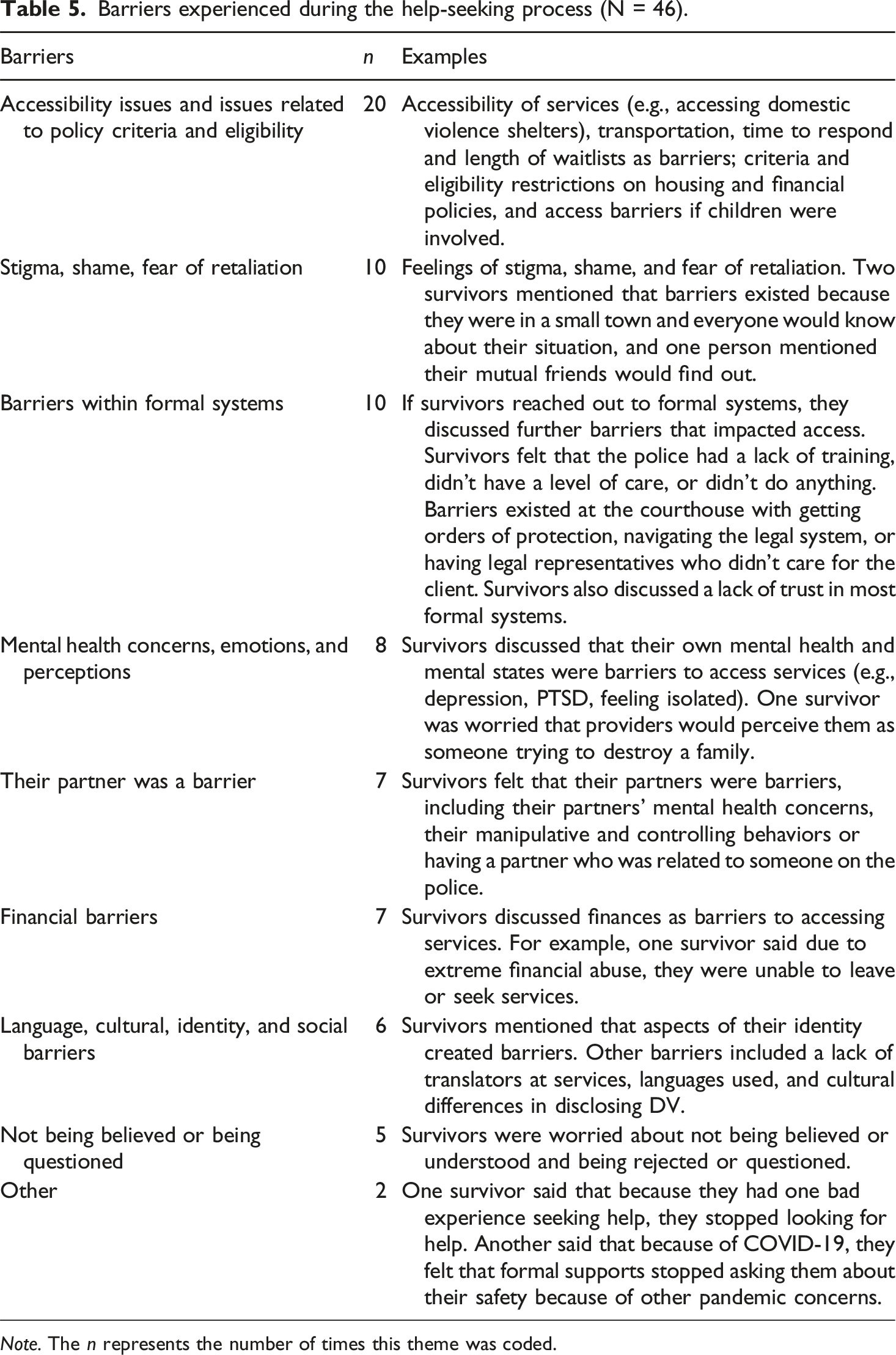
Another participant described needing education to navigate the complexities of the help-seeking journey: “Because the systems are so specialized and separated and you need them at different times, then you have to educate yourself, like you're getting a Master's or PhD in public works, or family law while you're trying to protect yourself and your kids and not lose your home or even your sanity.” - Cloe, a cisgender woman, identified as lesbian/bisexual, White race, from an urban community
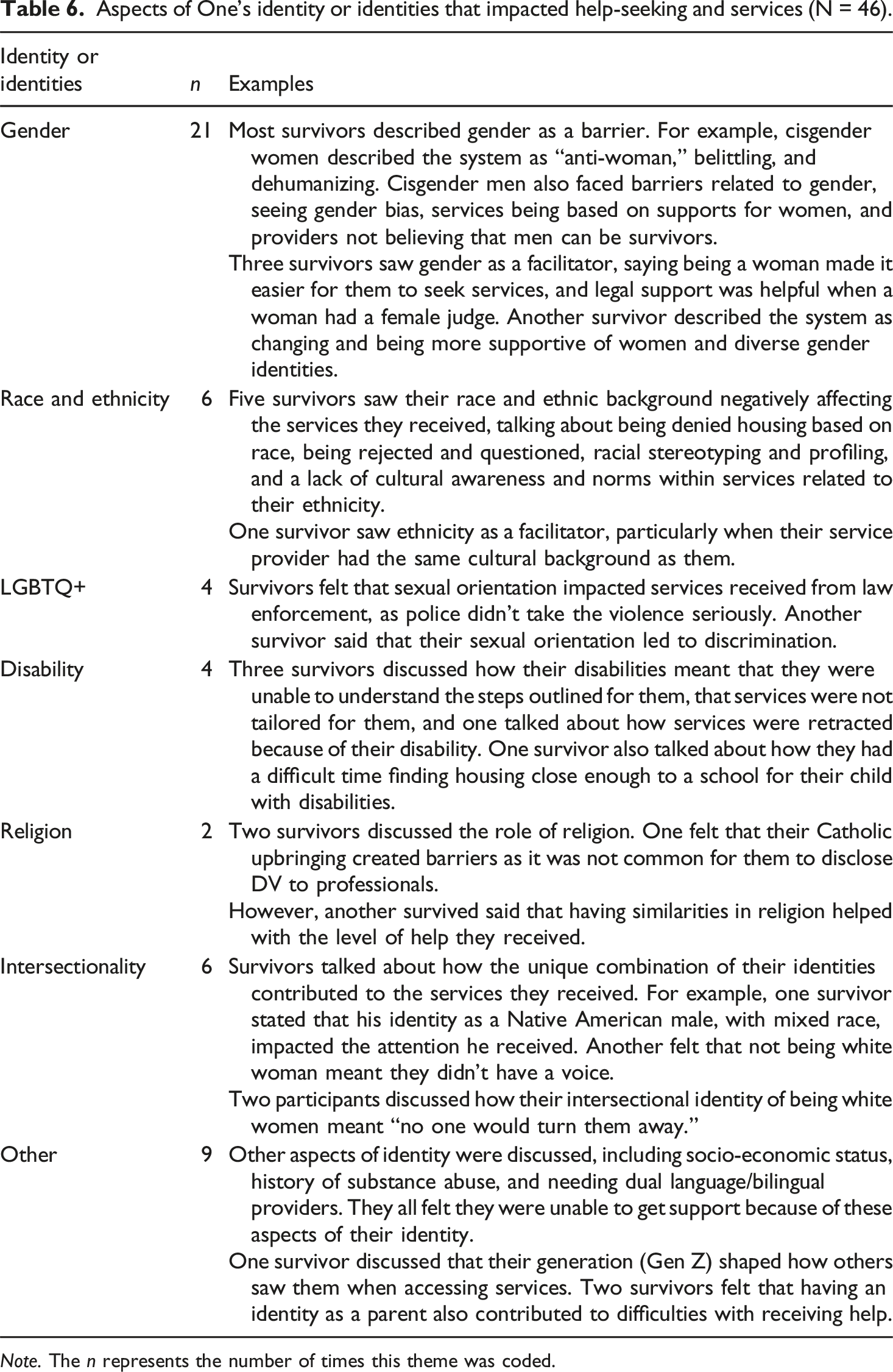
(a) Intersecting Marginalized Identities as Barriers. In addition to the barriers identified above, survivors were also asked to reflect if aspects of their identity (or identities) affected the services they received. Table 6 highlights the ways in which the aspects of one’s identity or identities impacted service provision negatively. Barriers were highlighted related to one’s gender identity (n = 21). For example, as Gemma stated: “From the get-go. That was the ultimate thing. Because I’m a woman, I’m lying.” – Gemma, cisgender woman, identifies as heterosexual, White race, from a rural community, with a disability
In our focus groups, we had two groups of cisgender men who participated. They talked about barriers related to gender, seeing a gender bias across services, services being based on supports for women, and providers not believing that men can be survivors of IPV. As Benny described: “I think my situation is unique to being a man. Many services out here are only focused on women. Seeking services as a man is difficult. The first place I went to...I did call the police because the situation was aggravated. And it wasn't easy for me.” – Benny, cisgender man, identifies as gay/bisexual, White race, from a rural community
Barriers were also discussed related to one’s race and ethnicity (n = 6), LGBTQ+ status (n = 4), disability (n = 4), and religion (n = 2). For example, Petra described how she was not taken seriously because she was in a lesbian relationship: “I couldn’t get a restraining order because the judge said I wasn’t scared of her enough to keep my doors locked. So, because I forgot to lock my door, it gave her an okay. I feel that was because we’re both two women.” - Petra, cisgender woman, identifies as lesbian/bisexual, Asian, from a rural community.
Others described not receiving the accommodations they needed related to their disability, while also facing bias and discrimination. Fear of bias and discrimination were also seen when describing worrying about “if the available services are culturally sensitive or that there was an awareness of my cultural norms and values” – Nico, cisgender man, identifies as heterosexual, Asian, from an urban community, immigrant.
Six participants explicitly talked about the unique intersection of their identities and how they contributed to the services they received. Mato described, “I think that I probably waited longer than I should have to try to reach out and seek help. Not only because I’m a male, but also, I’m mixed race. Being Native American, there’s a lot of domestic violence within the Native American community. There’s also a lot of apathy.” Mato, cisgender man, identifies as heterosexual, Multiracial, from an urban community. Similarly, Michal described: “I feel my financial stability, my cultural identity, and probably disability status actually played a part… in services being retracted at some point.” – Michal, cisgender man, identifies as heterosexual, Black race, from an urban community, with a disability. Carla shared that the police did not help her because “they probably didn’t take me seriously. They probably thought I was young woman, and I was going to keep taking him back or something.” Carla, gender non-binary, identifies as heterosexual, Latina, from an urban community, immigrant.
Finally, other factors were discussed that intersected with other aspects of survivors’ identities, including one’s socio-economic status, history of substance abuse, and needing dual language/bilingual providers. One discussed generational differences, and two felt that being a parent also contributed to the difficulties in receiving help.
Facilitators
Survivors also reflected on what they needed the most when they sought help. Many survivors (n = 28) talked about needing support, including emotional support from therapists, counselors, and advocates; service supports, including assistance filling out paperwork at the courthouse or support at a hospital following a sexual assault; and physical supports like safe places to stay and financial resources. These emotional and physical supports were seen as facilitators in the help-seeking journey. Across the need for supports, survivors echoed the critical role of having support from DV advocates: “Having an advocate at court changes everything. Not only in so many obvious ways, but also when you are experiencing trauma and or PTSD, having that person physically sitting beside you.” – Paige, cisgender woman, identifies as lesbian/bisexual, a racial minority, from an urban community, with a disability, immigrant
Additionally, survivors discussed needing to receive validation, needing to be taken seriously, having others believe them, and having people ask if they are okay. “What I needed the most at that time was someone, validating my experience, because when you tell someone that this is happening most people don't even believe you. There's no proof whatsoever. So, I would love to be acknowledged and be told that someone can help me and that I can do this.” -Marcel, cisgender male, identifies as gay/bisexual, White race from an urban community, immigrant
Liza also stressed the importance of finding “a place of safety, belief, and validation.” – Liza, cisgender woman, identifies as heterosexual, Black race, from an urban community, immigrant. (1) Intersecting Marginalized Identities as Facilitators. A few survivors talked about how their identity served as a facilitator to services. As shown in Table 6, facilitators were related to one’s gender (e.g., cisgender women saw it was easier for them to seek services) and culture (e.g., if service providers had the same cultural backgrounds as the survivor, this allowed for better understanding). For example, Karly describes services as helpful as they were “dual language for Spanish speaking families, and I’m not sure, maybe even other languages. If I needed that bilingual option whether a therapist or just volunteers… my experience was handled with care and respect. And that helped me feel safe.” – Karly, cisgender woman, identifies as heterosexual, Latina, from an urban community, with a disability
Discussion
Forty-six survivors of IPV, representing an array of diverse identities, with two or more intersecting marginalized identities and communities, shared their stories about seeking formal help, navigating systems, and finding support. We heard about the complexities of their help-seeking to attainment processes, including aspects they found particularly helpful and facilitators to support, as well as barriers they encountered. Intertwined with these stories were how aspects of their identities and geography, and how oppressive systems and stigma related to these marginalizations, impacted the services they sought or received.
Help-seeking and help attainment: The integral roles of marginalized identities and communities
Existing models illustrate the help-seeking (Liang et al., 2005) and help-attainment (Kennedy et al., 2012) processes among IPV survivors. Models also pull in aspects of stigma (e.g., cultural, internalized, and anticipated; Overstreet and Quinn, 2013), the social and cultural context (Kennedy et al., 2012; Waller et al., 2023), and provider trustworthiness and trust (Kennedy et al., 2024). These frameworks highlight the importance of including intersectional experiences in IPV help-seeking research, as navigating oppressive structures can lead survivors to feeling discrimination, uncared for, harmed further, or re-victimized.
Many of the core themes found in this paper aligned with these existing help-seeking models (Figure 1). Each journey described was unique, depending on the survivors’ immediate needs, the availability of services, their knowledge of supports, and situational and personal factors. From these unique stories, though, the role of marginalized identities and communities, and the structures and systems they were situated, played a significant role. Most of the discussions centered around barriers, including how one or more aspects of their identities impacted help-seeking and services. Most commonly gender was described as a barrier; cisgender women faced discrimination across systems, describing most formal spaces as “anti-woman.” Cisgender men also faced barriers related to gender bias and providers not believing men can be survivors. Individuals with diverse gender identities and were a sexual minority also discussed discrimination and how police did not take violence seriously. Marginalized race and ethnicity identities led to stereotyping, profiling, and housing discrimination. Survivors with a disability perceived services to not be applicable or outlined for them or had services retracted. A handful of survivors articulated intersectionality in their experiences, linking gendered racism, and ableism and racism.
In addition, about a third of this sample were participants from rural communities. For survivors living in rural communities, aspects of their marginalized identities intersected with rurality, seeing barriers related to accessibility (e.g., transportation, financial constraints, lack of culturally appropriate services), stigma, fear of retaliation, fear that everyone in their town would find out about their situation, and barriers within formal systems and policies. Cisgender men and gender non-binary survivors also highlighted that there were fewer domestic violence shelters in rural areas, and even fewer for those who are not cisgender women. More research is needed to keep learning about the rural experiences of navigating help-seeking for IPV, especially with one or more marginalized identities, or experiencing poverty (Hulley et al., 2023).
Across the barriers highlighted, themes relate to Sweet’s (2019) paradox of legibility, as these survivors are navigating formal structures that are often oppressive and harmful. Like Sweet’s research, this sample discussed trying to find credibility in their IPV experiences from formal structures by just wanting to be believed and supported. These formal structures contributed to feelings of dehumanization and belittlement. There was a lack of cultural awareness within services, and survivors felt that may of the services were not tailored for them, leading to confusion and/or termination of services. Despite these barriers, and a lack of trust in these formal systems, many needed these systems to get out of abusive relationships or find safety.
For example, survivors in this sample commonly sought help from police, law enforcement, obtained an order of protection, or sought help from other legal services. This finding was surprising, as other researchers have found marginalized survivors may be fearful to call the police (e.g., Schmidt et al., 2023). A review found that while some IPV survivors (i.e., women with substance use issues, immigrant women, women in rural communities, heterosexual men, racial and ethnic minoritized women, and sexual minority women) had positive experiences with seeking help from law enforcement, many reported revictimization, discrimination, police negligence, and cultural differences (Belisle et al., 2024). In this study, while quite a few survivors sought help from law enforcement, a sizeable group felt that they did not receive the help they needed. Survivors discussed feeling coercive situations within systems, police not enforcing orders of protection, or not feeling cared for. Survivors also noted that situational factors, like risk of lethality and physical safety, or the presence of children, was the reason they felt they needed to call police for help. Survivors living in rural communities also described police as their first point of contact, as they may have lived further away from other resources like a domestic violence shelter.
Survivors sought help from a variety of formal response systems, though the most common was DV agencies and community-based organizations. It should be noted that these survivors were recruited from agencies and community-based organizations; however, this research provides further insight into the supports they received, what they found helpful, and barriers they encountered. Survivors also sought help from legal and medical providers, hotlines and websites, and informational materials. Thus, this variety of sources for help-seeking calls for more inclusive, culturally responsive services cannot just exist for DV agencies. All systems of care need to strengthen service provision (Green et al., 2024).
Survivors are not a homogenous group; services need to build and continue to strengthen their capacity to deliver services that are inclusive and responsive, in aims of building trustworthiness (Kennedy et al., 2024). Law enforcement and legal systems are common contexts for survivors to seek help, especially in potentially lethal and unsafe situations. As survivors are seeking help across a variety of formal systems, service provision is changing to accommodate. For example, coordinated community response is one growing area of work, pairing police and victim advocates, although more rigorous research is needed (Johnson and Stylianou, 2020). Karina’s Law in Illinois improves protections for survivors, by removing firearms from perpetrators when there is an order of protection in place (The Network). Thus, research and policy efforts are gaining momentum to find more responsive supports for survivors across systems of care.
Facilitators
Survivors need to feel supported, safe, validated, and believed. No matter a survivors’ identity or community, these remain consistent facilitators to help-seeking and attainment (Ravi et al., 2021). DV advocates were a key support mentioned throughout the help-seeking process. They played a crucial role by empowering survivors through access to essential resources and opportunities such as legal and medical support, housing, and employment (Sullivan and Goodman, 2019). Moreover, survivors emphasized the importance of DV advocates’ ability to provide support through an intersectional lens that acknowledged their diverse identities and experiences (e.g., gender, race, sexuality socioeconomic status, parental responsibilities, and access to resources; Goodman et al., 2015; Kulkarni, 2018). These findings add to previous literature that highlight the importance of DV advocates in supporting survivors’ overall well-being and quality of life (Beeble et al., 2009; Goodman et al., 2016), assistance with securing stable housing (Sullivan and Goodman, 2019) , impact on survivors’ increased likelihood of participating in legal proceedings (Camacho and Alarid, 2008; Taylor-Dunn, 2015), and decreasing future experiences of violence or abuse (Wood et al., 2021). Intersecting marginalized identities were also seen as facilitators to receiving help when one or more of their identities matched or were like their service provider. As stressed in Kennedy et al. (2024), these matched identities and experiences can help build trustworthiness between providers and survivors.
Limitations and future directions
The current study utilized a purposive sampling strategy to ensure we heard from a large proportion of marginalized groups in Illinois. However, this means that our sample was not representative of all IPV survivors in Illinois. Additionally, we recruited survivors from DV agencies and community-based organizations, so the survivors who participated in the screening survey were still connected to those networks in some capacity. This sample was also unique in that survivors had reached out for some type of formal and/or informal support.
Thus, although this sampling strategy provided us an in-depth look at a diverse sample of IPV survivors, there are groups that are not represented in this report. For example, missing from this study are the perceptions of survivors who have not yet sought help, those who are unable to access services, those who are not knowledgeable about IPV services available to them, those who are still currently experiencing IPV and are unable to seek help, and/or those who are no longer connected to a DV agency or organization in their community. Future research is needed to expand these results and further understand the help-seeking process among adult survivors. Additionally, we had lower participation from Northern and Southern regions of the state. More focus groups are necessary to ensure we hear from more diverse perspectives of survivors in these regions of Illinois.
Researchers are exploring differences in help-seeking by aspects of one’s identity (e.g., race, Satyen et al., 2018; gender and sexual orientation, Scheer et al., 2023), including barriers experienced by men (e.g., Taylor et al., 2021). Additionally, research has found that institutional racism, immigration laws, and a lack of culturally responsive services may prevent marginalized groups from accessing formal services (Hulley et al., 2023). The current study expanded this body of work to highlight additional barriers and facilitators related to different aspects of one’s identities and communities. Some aspects of identity were also discussed by one or two participants in these focus groups that also warrant future research, including survivors with varying socioeconomic status, and those with a history of substance abuse. Overall, more research is necessary to continue examining intersectional identities and communities that are currently at the margin of IPV services.
Implications
These findings highlight important steps forward for ICADV, as well as for other systems of care. This research adds to a growing body of recommendations posited by researchers and practitioners, including providing comprehensive, trauma-informed care (Paphitis et al., 2022), the importance of empowering survivors to direct their help-seeking journey in finding safety (Cattaneo et al., 2020), systems-specific improvements (Klein and Klein, 2016; Kulkarni, 2018), and better collaboration and coordination across systems (O’Neal and Beckman, 2017).
First, practitioners working with DV survivors highlight the importance of trauma-informed care (Paphitis et al., 2022), which is the knowledge of trauma and responding to its signs and symptoms through organizational practices and policies that prevent further trauma or re-traumatization (SAMHSA, 2014). Despite a push for more trauma-informed care in many nonprofit and healthcare spaces, many law enforcement departments are resistant (Ravi et al., 2021). A survivor remains in a heightened state of awareness and survival mode, even after imminent harm has passed, and this trauma can manifest in physical and emotional ways. Thus, any provider who is interacting with a survivor needs to be aware of the effects of trauma so that they can begin to foster safety and trustworthiness with the survivor. Without this, the survivor is likely to feel uncared for or revictimized and can prevent a survivor from obtaining the help they need (National Network to End Domestic Violence, n.d.). Providing trauma-informed care across systems is critical, especially as we found that survivors sought formal help in a variety of settings.
Second, empowering survivors gives them options and choices in directing their help-seeking (Goodman et al., 2016). When survivors may feel that their sense of safety and control is undermined or gone in situations of abuse, empowering survivors to direct their help-seeking journey is paramount (Sullivan and Goodman, 2019). Empowerment can lead to more effective safety planning and advocacy, all beginning with the survivors’ wants, needs, and priorities (Cattaneo et al., 2020).
Additionally, this study contributes to ongoing conversations on how to improve system-specific services, as well as coordination among services that support of survivors, centering their perspectives on where such efforts are falling short and how they can be strengthened. While much of the existing literature emphasizes the development of coordinated community responses (CCRs) as a strategy for enhancing collaboration among stakeholders—such as law enforcement, social services, healthcare providers, and community organizations—this study highlights survivors’ insights as a critical yet often overlooked component (Boots et al., 2018; Johnson and Stylianou, 2020). These findings offer guidance for building more effective CCRs and underscore the need for future research to examine the unique help-seeking pathways adopted by underserved survivors to foster stronger, more responsive formal interagency connections and response.
Finally, this research highlighted the pivotal role of DV advocates in navigating the help-seeking journey. Advocates play a vital role in offering support that is empowering, trauma-informed, and culturally inclusive, ensuring that survivors’ unique needs and diverse intersecting identities are recognized (Sullivan and Goodman, 2019). Given their significance, research, policy and practice should prioritize centering advocates across DV services. This involves examining collaborations between DV advocates (Stauss et al., 2025) and with other formal support systems to improve survivor support, as well as increasing funding to enhance their capacity to help.
Survivors in this study, and anecdotally far and wide, have long asked for more comprehensive, collaborative support systems. The consistent echoing of the importance of the DV advocate and their role in a survivor’s help-seeking journey is critical to this need. After all, a DV advocate, in and of themselves is a connector to broader systems. This study is both a reminder of the critical services DV agencies and DV advocates provide, and an urgent sign that services across all systems of care should be strengthened to better serve and support all survivors.
Supplemental material
Supplemental Material - Navigating the complexities of help-seeking: Amplifying the voices of marginalized survivors of intimate partner violence
Supplemental Material for Navigating the complexities of help-seeking: Amplifying the voices of marginalized survivors of intimate partner violence by Rachel C. Garthe, Apoorva Nag, Chloé McMurray, Emily Strickland, Samantha Dickens in Qualitative Social Work
Footnotes
Acknowledgments
A special note of gratitude to students and staff within the Violence Prevention Research Lab who were essential to this work, including Nick Cannon, Emily Dailey, Alina Loewenstein, Ayla Makris, Haley Miller, and Nia Welch. Also, a thank you to Ema Phelps at ICADV for assisting with recruitment and reviewing drafts. We thank the domestic violence agencies and organizations across Illinois that assisted with advertising this study with their networks. Finally, we are extremely grateful for the survivors who participated in the focus groups; participating in these groups took immense courage and bravery.
Ethical considerations
All research procedures were approved by the Institutional Review Board at the University of Illinois Urbana-Champaign.
Consent to participate
All participants completed online informed consent before participation.
Author contributions
All authors collaboratively conceptualized this study; RG led the research design, analyses, and writing of the paper. AN led data collection, contributed to the analyses and writing of the paper. CM, ES, and SD all contributed to the writing of the paper.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by an interagency agreement between the Illinois Coalition Against Domestic Violence and the University of Illinois Urbana-Champaign, awarded to Dr. Rachel Garthe. Funding was provided in whole or in part by the Illinois Department of Human Services.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is not available due to the small sample size and research procedures approved by the institutional review board.
Disclaimer
Points of view or opinions in the document are those of the authors and do not represent those of the Illinois Department of Human Services.
Supplemental material
Supplemental material for this article is available online.