
Abstract
It is well documented that intimate partner violence and housing instability can profoundly impair survivors’ mental health, help-seeking efforts, and coping strategies. Few studies, however, focus on this population’s experiences in mental health therapy, and even fewer explore their thoughts on what therapists and survivors can do to facilitate a sustained, beneficial therapy experience. Informed by feminist therapy theory, this descriptive qualitative study addressed this gap by conducting phone interviews with intimate partner violence survivors who had a federal housing voucher (n = 21) recruited from a social work agency in a Mid-Atlantic U.S. city and a focus group with therapists employed by the agency (n = 3). We analyzed data using qualitative content analysis, involving a two-cycle coding process and constant comparison. Most of the participants were engaged in therapy at the time of the interview, and almost all had been in therapy previously. Participants’ advice for survivors coalesced into three main themes (i.e., “give it a try,” you need therapy to heal and move forward, and therapy is hard but worth it), as did their advice for therapists (i.e., “domestic violence is a deep subject” that requires specialized education, “follow the survivor,” and “have a holistic approach”). Findings suggest that supporting the mental health of survivors who have experienced housing instability requires increased access to low-cost, long-term therapy; use of survivor-defined, trauma-informed approaches; specialized training for therapists; and creative avenues to encourage survivor engagement in therapy. Social workers are uniquely positioned to advance these goals, given their person-in-environment approach and social justice orientation.
Keywords
It is well documented that intimate partner violence (IPV) or domestic violence (DV) victimization, terms used interchangeably in this paper, increases risk for a range of mental health (MH) concerns, including but not limited to, depression, anxiety, post-traumatic stress disorder, and suicidal thoughts and behaviors (Lohmann et al., 2024; McLaughlin et al., 2012; Trevillion et al., 2012). These MH impacts are even more severe when IPV co-occurs with housing instability, which is profoundly stressful and destabilizing by itself (Marçal et al., 2022; Rollins et al., 2012; Suglia et al., 2011). Moreover, IPV survivors face unique challenges to finding and maintaining stable housing, which can lead to a vicious cycle of re-abuse and homelessness that is difficult to escape and further erodes MH (Hargrave et al., 2025; Kulkarni and Notario, 2024; Kuskoff et al., 2025; O’Campo et al., 2016).
Evidence suggests that survivors consider MH improvement to be an essential element in their recovery from IPV (Carman et al., 2023); however, a range of barriers hinder their ability and willingness to engage in therapeutic interventions (Kennedy et al., 2023; Rodríguez et al., 2009). Survivors often encounter providers who are not receptive to IPV disclosure, lack IPV knowledge, ask victim-blaming and stigmatizing questions, and are discriminatory toward minoritized survivors (Kennedy et al., 2023; Murray et al., 2018; Rodríguez et al., 2009; Trevillion et al., 2014; Voth Schrag et al., 2021). Another barrier is availability. For example, in 2023, only 42% of DV agencies provided therapeutic services such as individual and group counseling, typically offered on-site in congregate residential programs such as shelters—a number that is declining due to ongoing budget cuts (National Network to End Domestic Violence, 2024; Yakubovich et al., 2022).
Access is also a challenge. Many unstably housed IPV survivors do not live in DV residential programs, either because they cannot or would rather not (Fraga Rizo et al., 2022; Lander, 2023; National Network to End Domestic Violence, 2024). Thus, they cannot access the therapeutic services offered at these programs due to location confidentiality (Goodman et al., 2022). Instead, a substantial number of these survivors seek help from the homeless service system and are placed in an emergency shelter or motel if they meet eligibility criteria (Lander, 2023). To illustrate, in New York City in 2023, the homeless system served 2,911 households that reported DV as primary reason for shelter, which was only 30.7% fewer than the 4,200 households served by the DV shelter system (Office of Domestic Violence Services, 2023). In addition, some unstably housed survivors move into their own residence, typically with help from flexible funding, rapid-rehousing, or voucher programs (New Destiny Housing, 2024; Stylianou and Pich, 2021; Veneri, 2021); however, this option is increasingly scarce due to a lack of affordable housing and shrinking social safety nets (Colburn et al., 2025).
Despite a rather robust literature on survivors’ help-seeking and service use, only a few studies have focused on experiences with MH therapy specifically (Grillo et al., 2021; Sorrentino et al., 2021; Trevillion et al., 2014). Informed by tenets of feminist therapy theory (Brown, 2018)—especially as applied to IPV (Goodman and Epstein, 2008)—this study centered the voices and perspectives of survivors dealing with multiple, intersecting sources of oppression (e.g., IPV, poverty, housing instability) to explore their perspectives on MH therapy. Specifically, we were interested in their thoughts on what therapists need to know about working with this population, and what IPV survivors need to know about MH therapy—an especially overlooked area of research. Beyond adding to research, this study can advance two of the 14 Grand Challenges of Social Work (i.e., “end homelessness” and “build healthy relationships to end violence”; Teixeira et al., 2021) by improving services for people at the intersection these crises.
Literature review
Intimate partner violence, housing instability, and mental health
Intimate partner violence, defined by the Centers for Disease Control and Prevention, as “contact sexual violence, physical violence, stalking, and psychological aggression” by a current or former partner, is a pervasive social problem in the United States (Leemis et al., 2022, p. 2). Other forms of IPV are also pervasive, such as economic abuse, which involves economic control, exploitation, employment sabotage (Postmus et al., 2020), and social abuse, which can involve monitoring, limiting, or cutting off social relations (Park and Jeon, 2022). Many survivors experience some combination of these forms as part of coercive control, a type of IPV (Kelly and Johnson, 2008) in which one partner uses a variety of individualized tactics to subjugate the other partner and entrap them physically and mentally (Stark, 2009, 2023). Coercive control is particularly pernicious for MH because it involves intentionally sabotaging survivors’ trust in their own sanity and sense of safety in the world through tactics such as gaslighting, exploiting their vulnerabilities, and surveilling them (Dutton and Goodman, 2005; Stark, 2009; Sweet, 2019).
Although they often co-occur, experiencing any form of IPV, especially in the context of coercive control, can affect survivors’ housing stability by making it unsafe for them to stay in their home or by impairing their physical and MH functioning in ways that erode their financial resources and social networks (Bullock et al., 2020). Housing instability can manifest for survivors in many ways, such as ongoing eviction threats, frequent moves, doubling up, shelter use, and having to live with an abusive partner. These experiences are traumatic, disruptive, and further diminish survivors’ MH (Gezinski and Gonzalez-Pons, 2021; Marçal et al., 2022; Rollins et al., 2012). To illustrate, in a study with over 400 unstably housed IPV survivors, the sample exceeded the clinical cutoff scores for depression, anxiety, and PTSD (Sullivan et al., 2023).
The risk for housing instability and homelessness is especially high among survivors struggling with intergenerational poverty and structural racism, given the dearth of resources available to help them with safety and stable housing (Bullock et al., 2020; Kulkarni and Notario, 2024). Goodman and Colleagues (2009b) described the intersection of IPV and poverty as a collision of crises that result in feelings of stress, powerlessness, and social isolation, which have dire effects on MH. They coined the term “survival-focused coping,” to highlight the centrality of poverty and instability in survivors’ responses to IPV (Goodman, Smyth, et al., 2009, p. 306) and the costly tradeoffs they must make to stay alive (Thomas et al., 2015).
Help-seeking and service engagement among IPV survivors
The abundant literature on help-seeking and service engagement among IPV survivors has identified a range of influences on survivors’ behaviors that fall along multiple levels of the ecological model. For example, a recent systematic review on facilitators identified the following factors: survivors’ knowledge of services and rights; desire to receive services; fear of future harm, especially for children; provider knowledge; extent of accessibility; and level of support from informal network members and service providers (Ravi et al., 2022). A qualitative study with unhoused IPV survivors specifically found similar facilitators such as readiness, supportive networks, respectful treatment, and accessibility; however, it also highlighted the importance of affordability for this population (Rakus and Singleton-Jackson, 2024).
Research has also identified other influential factors. In the Intimate Partner Violence Stigmatization Model, Overstreet and Quinn (2013) identified three constructs of IPV-related stigma that serve as a barrier for survivors: anticipated stigma (e.g., fear of judgment), stigma internalization (e.g., guilt and shame), and cultural stigma (e.g., victim-blaming reactions and attitudes from providers). An expanded version of this model added perpetrator stigma, which refers to abusive messages and actions that perpetuate IPV stigma (Murray et al., 2018). Racism and discrimination also affect help-seeking. Survivors of Color and foreign-born survivors are less likely to seek help from formal supports compared to their White peers—with differences particularly pronounced regarding MH services— due to providers and systems that threaten survivors’ wellbeing, lack representation and cultural responsiveness, and reinforce survivors’ internalized identity-based oppression (Bent-Goodley et al., 2023; Cho et al., 2020; Fiolet et al., 2021; Kennedy et al., 2023; Satyen et al., 2019; Waller et al., 2022).
Research focused specifically on IPV survivors’ MH help-seeking and engagement aligns with the factors just described and offers other ones. In their review of provider trustworthiness in IPV help-seeking, Kennedy and colleagues (2023) identified three domains that providers (including MH providers) should demonstrate: benevolence (e.g., accessible, supportive), fairness (e.g., non-discriminatory), and competence (e.g., evidence-based and trauma-informed). Another study on providers’ thoughts about barriers to MH services for IPV survivors identified the following: dearth of providers trained in IPV, few options for long-term therapy, immediate crisis needs, fear and stigma, and abuser control (Simmons et al., 2015). Finally, the therapeutic alliance is important for sustaining engagement for survivors (Goodman, Fauci, et al., 2016).
Mental health interventions for IPV survivors
Many therapeutic interventions have been developed to address the MH needs of IPV survivors. Findings from several systematic reviews indicate that interventions typically fall into empowerment-based advocacy services, clinical interventions of differing modalities (e.g., cognitive behavioral, motivational interviewing, and art therapy), or a mix of both; that participation is associated with decreases in depression, anxiety, and PTSD; and the most impactful interventions are those that use a trauma-informed approach (Arroyo et al., 2017; Craven et al., 2023; Hackett et al., 2016; Ogbe et al., 2020; Paphitis et al., 2022; Trabold et al., 2020). An individualized approach is also critical: aspects of a survivor’s situation (e.g., housing status) influence which intervention components, delivery method, and outcomes are possible and desired (Paphitis et al., 2022). That said, in a study on how survivors define recovery from IPV, a commonly identified outcome was improved MH in the form of freedom from triggers, flashbacks, and shame, anxiety, and depression (Carman et al., 2023).
Survivors’ experiences with mental health therapy
Several studies offer the groundwork for understanding survivors’ experiences with MH therapy. Trevillion and colleagues (2014) conducted a qualitative meta-synthesis of 12 studies on the experiences and expectations of MH service users experiencing IPV. Findings fell into three main categories: IPV identification, immediate responses to disclosure, and acknowledgement of disclosure. Within these categories were a range of negative experiences such as providers failing to do the following: identify abuse, believe them, give them the opportunity to process IPV, give them control over sessions and care plans, acknowledge the impact of IPV on their MH, and realize they were too focused on the medical model (Trevillion et al., 2014).
Two recent studies support and extend these findings. Sorrentino and colleagues (2021) interviewed 50 female IPV survivors recruited from the Veterans Health Administration (VHA) to explore their thoughts on client-centered care in psychotherapy. Findings support a desire for a flexible, individualized approach that offers a safe space and choice to decide what to share and when. An individualized approach also included respecting participants’ complex situations and supporting their self-determination with difficult decisions. In addition to feeling validated and supported, making progress in outcomes was an important part of client-centered care, namely strengthening internal resources and increasing access to external resources related to safety from IPV (Sorrentino et al., 2021). Grillo and colleagues (2021) also recruited a sample of 25 female IPV survivors from the VHA to explore their thoughts on client-centered care. Data fell into five categories of desired outcomes from the brief counseling intervention: empowerment, social connectedness and support, self-esteem, knowledge, and valued action and goal setting.
Taken together, these studies offer valuable findings and illuminate gaps for additional research. For example, the findings of the meta-analysis by Trevillion et al. (2014) are limited by the fact that all studies were conducted outside of the U.S., and seven of the studies had samples in which only a few survivors had had any contact with a MH provider. These limitations are not present in Sorrentino et al. (2021) and Grillo et al. (2021); however, these studies focused on a very specific population (VHA patients) and therapy type (psychotherapy and brief counseling).
The current study: Conceptual framework and research questions
The lack of research on survivors’ experiences with MH therapy is not all that surprising when history and theory are considered. As Goodman and Epstein (2008) have chronicled, the MH system’s initial response to IPV survivors was to pathologize them, discourage leaving, and treat them with “internally focused psychotherapeutic solutions” (p. 50). The advent of the DV movement introduced a new type of professional helper (i.e., advocates), who developed a network of DV programs focused on advocacy and empowerment, blamed IPV on structural inequalities, and distrusted MH providers and perspectives (Goodman and Epstein, 2008). As a result, research on services for IPV survivors has focused more on advocacy than MH therapy.
This relatively siloed service approach has abated but not disappeared completely, even with the development of feminist therapy, “a theory that derives its inspiration and wisdom from an in-depth interrogation of standpoints that are unavailable to the dominant culture simply because they have been relegated to the margins” (Brown, 2018, p. 1). Feminist therapy aims to empower clients through collaborative, individualized treatment; ongoing analysis of structural and political power dynamics; and prioritization of client expertise and liberation (Brown, 2018). According to Goodman and Epstein (2008), feminist therapy offers a bridge between MH and advocacy interventions, because it “attempts to integrate the internal and external difficulties survivors face” (p. 59). They stressed, however, that not all MH providers utilize a feminist therapy approach or even help survivors address the external barriers that exacerbate their internal ones, either because they lack the necessary knowledge or see such help as outside their role. They noted social workers are somewhat of an exception (Goodman and Epstein, 2008)—which is not surprising given the profession’s emphasis on social justice, person-in-environment, and anti-oppressive practice (Reisch and Jani, 2025)—however, research has yet to fully examine IPV survivors’ perspectives on MH therapy, including when it is provided by social workers.
Informed by feminist therapy theory and the literature gaps, the goal of this study was to better understand how MH providers, including social workers, can improve outreach and response to IPV survivors who have experienced housing instability. To achieve this goal, we centered the expertise of survivors in MH therapy (n = 21) and social work therapists (n = 3) who work with IPV survivors to address the following research question: how can MH therapists and clients at the intersection of IPV and housing instability facilitate sustained and beneficial MH therapy engagement? We were specifically interested in their thoughts on 1) what therapists need to know and do when working with clients who have experienced IPV, and 2) what survivors need to know and do when engaging in therapy, or contemplating engaging in therapy.
Methods
This study used a descriptive qualitative methodology (Kim et al., 2017) and was part of a larger project: an external evaluation of a voluntary program developed for IPV survivors who had recently leased up with an emergency housing voucher. The program was administered by a DV agency located in a major metropolitan area in the Mid-Atlantic region of the United States, and provided aftercare services in the form of advocacy, case management, and targeted referrals for up to nine months post move-in. A primary referral was for free MH therapy provided by master-level social work therapists employed by a social service agency that was a partner in the project (herein, “therapy agency”). All study procedures were approved by Simmons University’s Institutional Review Board.
Participants and recruitment
We recruited two groups of participants for this study: (a) aftercare clients who received services from the MH therapy agency, and (b) MH therapists who had served aftercare clients (to triangulate client data). Client recruitment consisted of the following steps. First, when aftercare clients (who had already consented to participate in the larger evaluation) requested a referral to the therapy agency, they were asked if they would like to learn more about the opportunity to participate in an in-depth interview about their experiences with therapy. Staff were instructed to stress that the interview would be confidential and that whatever they decided would not affect their services from the DV agency or therapy agency. Those who said yes were asked to sign a consent form and a HIPPA Release of Information form so the research team could be given their contact information. Those who agreed were emailed with information about participating in the interview and asked to respond if interested. Between March to August 2023, the first author invited all clients to participate who met the study eligibility criteria (n = 46): aged 18+, had engaged in MH therapy for at least two months, and had consented to be contacted.
Identity and experience characteristics of participants.
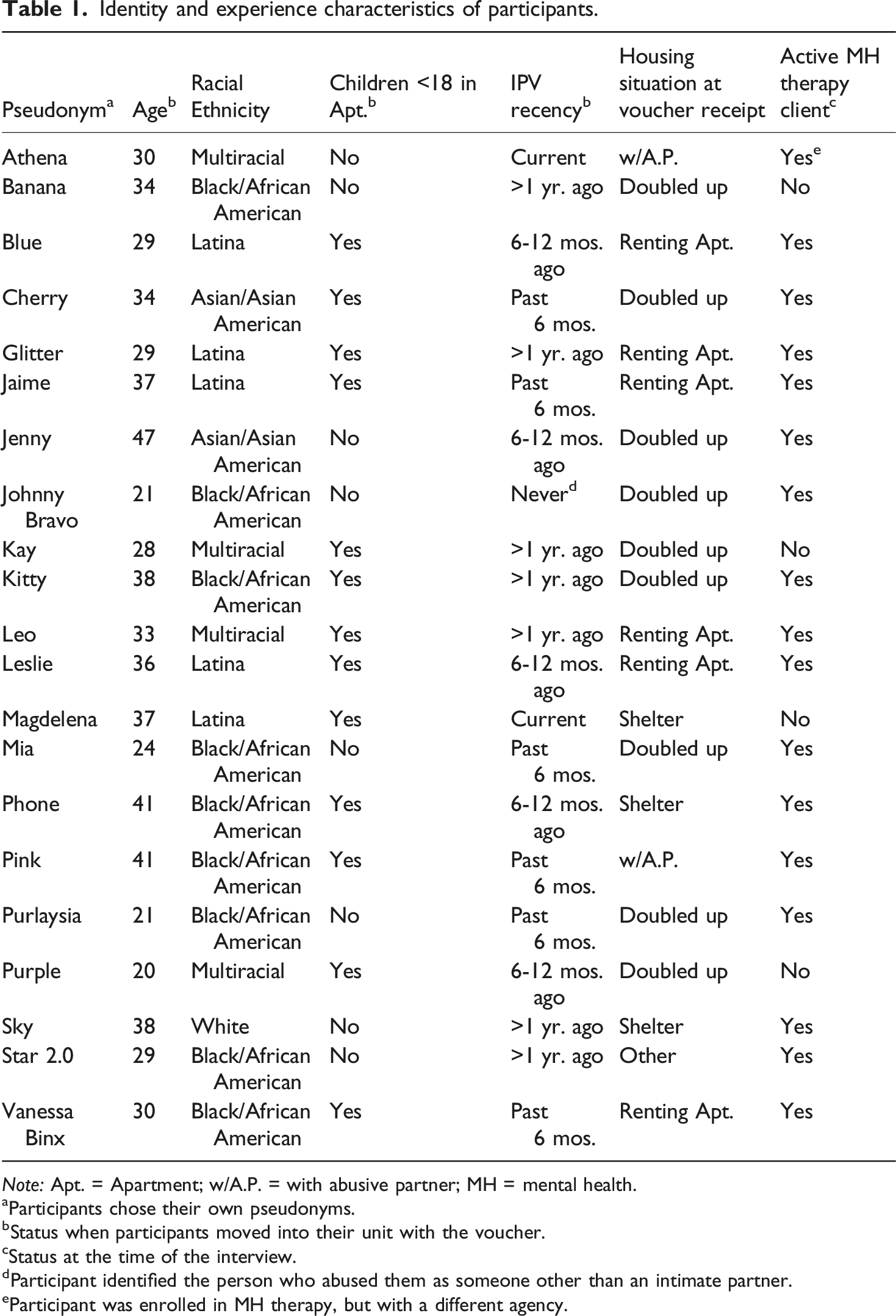
Note: Apt. = Apartment; w/A.P. = with abusive partner; MH = mental health.
aParticipants chose their own pseudonyms.
bStatus when participants moved into their unit with the voucher.
cStatus at the time of the interview.
dParticipant identified the person who abused them as someone other than an intimate partner.
eParticipant was enrolled in MH therapy, but with a different agency.
To recruit the second group of participants, the first author emailed the three therapists with aftercare clients on their caseload at the therapy agency and invited them to participate in a focus group. All three agreed and identified as female social workers, with one holding clinical licensure, one pursuing clinical licensure, and one about to graduate from an MSW program in clinical practice. To protect confidentiality, no other demographic data were collected.
Measurement and data collection
Client therapy data
We collected qualitative data using a semi-structured interview guide developed with input from the DV and therapy agency staff (Bender, 2017) that followed an hourglass format (SRAENE, 2022): questions started out broad (e.g., “How would you describe your overall experience so far?”), became more specific (e.g., “Were there things the therapist said or did in therapy that really stand out as helpful to you?”), and then ended broad (e.g., “What is the most important thing that I should know about your experiences in therapy?”). To address the current study’s research questions, participants were asked what advice they would give to therapists who work with survivors, and to survivors who are engaged or interested in therapy. The interview guide began with the following statement: “Let’s start by having you pick a name that is not your actual name or nickname that I can call you during the interview and if I quote you in the findings. It can be anything: a different name, flower, feeling, color, food, or whatever else you would like it to be.” This statement acted as an icebreaker, de-identified the audio-file and transcript, increased participant’s sense of being “in the driver’s seat”—a message we said repeatedly throughout the process to help mitigate the inherent power dynamic between interviewers and interviewees (Bender, 2017). It is worth noting that the first author developed this approach for a prior study with IPV survivors and has continued using it because it is consistently well received; in fact, a recent study argued that asking participants to select their own pseudonyms can advance epistemic justice (Pretorius and Patel, 2025).
We collected data using phone interviews that lasted between 45 and 60 minutes. The first author, who has extensive research experience with IPV survivors, conducted the interviews, except for one conducted in Spanish by a bi-lingual research team member trained by the first author. We were acutely aware of the need for extra precautions when conducting research with IPV survivors (Bender, 2017); thus, we used a variety of strategies to protect participants’ safety and confidentiality. As mentioned, we only contacted clients who consented to be contacted, and we did so via the email address they said was safe. In our email, we stressed that participation was voluntary, confidential, and would not affect service involvement. Respondents who wanted to participate were asked to provide days and times that were safe and convenient, a safe number to call for the interview, and anything important to know when we called. Even though we knew from the survey data that none of the participants were living with an abusive partner at the time, we created a brief script for calling and leaving messages. The interviewer started the interview by identifying herself, confirming the participant’s identity, asking if it was still a good time, and obtaining informed consent. During the interview, she paused to check in with participants and reminded them to skip topics they did not want to discuss. She ended the interview by debriefing participants’ feelings. It is worth noting that, although some participants chose to share details about their IPV experiences, we did not ask about IPV directly. Finally, we destroyed audio files, deidentified transcripts, and used unique ID numbers to link interview data to quantitative data.
Therapist data
We conducted a virtual, one-hour focus group with therapists, which was held one year after the agency began serving EHVA clients to ensure therapists had enough time to build a varied caseload of IPV clients. They were sent the consent form and questions ahead of time, gave verbal consent at the start of the group, were asked to provide pseudonyms using the same icebreaker used with survivor participants, and asked to debrief at the end. The first author was the primary moderator; a research team member was a secondary moderator and note taker.
Data analysis
Analysis of interview data followed a qualitative content analysis approach (Kim et al., 2017) that utilized a two-cycle coding approach informed by Saldaña (2021) and included the grounded theory technique of constant comparison (Charmaz and Thornberg, 2021). In the first cycle of coding, we conducted descriptive, in-vivo, and concept coding to develop initial codes and categories as well as attribute coding to determine if participants had prior experiences with MH therapy. In-vivo coding was particularly helpful for keeping codes close to the data and participants’ language. We also engaged in “theming the data categorically” to develop short phased codes (vs one word) when necessary (Saldaña, 2021, p. 259). For the second cycle, we engaged in several rounds of focused coding to distill codes into the most salient categories and themes without attention to attributes and dimensions (Saldaña, 2021). All authors were engaged in the analysis process, by first coding three transcripts together to develop the initial codebook. The second and third author split the remaining transcripts and coded them with the first author. The first and second author conducted the bulk of the focused coding, with the third author included for review, resolution, and refinement. The first and second author also coded the focus group data using Massey’s (2011) framework for categorizing and coding focus group data.
Informed by Stahl and King (2020), we tended to trustworthiness in the following ways. To enhance credibility, we used triangulation of data source (clients, therapists) and investigator (three coders), member checking during the interviews, and heavy reliance on verbatim quotes. To enhance transferability, we have included rich detail about the participants and methods and collected data until saturation was reached. To enhance dependability, we practiced reflexivity throughout, such as ongoing peer debriefing, including consulting with colleagues who possess content and methodological expertise; memo-writing; and discussing our positionality. For example, we are all white and cisgender, with graduate degrees in social work; it was essential for us to talk openly and often about the impact of our sources of privilege. In addition, the second and third authors are practicing social work clinicians, and all of us have been therapy clients; we discussed how these roles could influence coding. Finally, we all have some personal connection to IPV, which required constant work on self-awareness regarding how our own experiences could affect how we interacted with participants during the interviews (to help avoid over-identification), our window of tolerance when reading and coding the data (to help avoid secondary traumatization), and our interpretation of findings (to help minimize bias).
Results
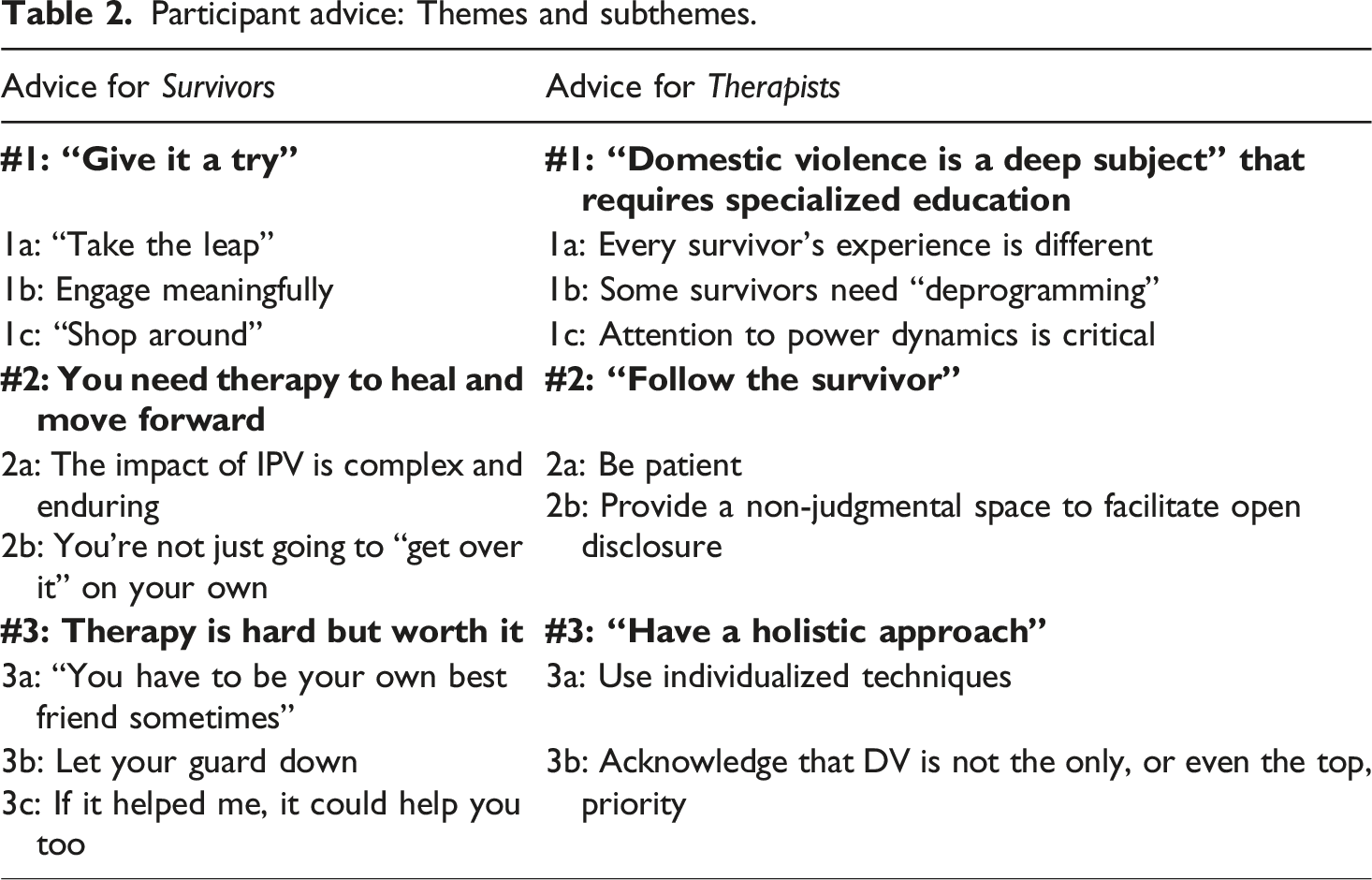
Participant advice: Themes and subthemes.
Advice for survivors
Participants overwhelmingly asserted that MH therapy is necessary and beneficial for people who have experienced IPV, and they strongly recommended all survivors engage at some point. That said, they were candid about the complex and unique challenges survivors often encounter during the therapy process, and they stressed how important it is for survivors to know what to expect from therapy and how to respond. Not surprisingly, participants drew heavily from their own experiences to inform the advice they offered, which fell into three main themes.
Theme #1 for survivors: “Give it a try.”
The most common advice participants had for IPV survivors was to “give it a try.” This phrase, which was said often, reflected the spirit of encouragement that permeated the interviews and consisted of three sub-themes: “take the leap,” engage meaningfully, and “shop around.” Embedded in the advice to “try” therapy was an acknowledgement of how daunting it can be for survivors to simply start the process or “take the leap,” due to barriers related to the dynamics of IPV (e.g., shame, fear) as well as logistics (e.g., time, money), especially among survivors who are struggling to pay bills and maintain housing. Ultimately, though, participants argued that taking the leap into therapy was absolutely worth it because if it did not help, they could stop. As Sky said, “I think I would probably say, what do you have to lose? If you’re in a dark place and you can’t see the door, why not invite someone into your life who can show you where it is?” Likewise, Leo said, “Just give it a shot. What’s the worst that could happen?”
Although participants asserted that therapy should be a choice and that survivors could stop whenever they want, they were not suggesting survivors adopt a cavalier approach to therapy. Instead, they were clear that “giving it a try” meant “giving it a real try” by engaging meaningfully in the therapeutic process. Meaningful engagement was defined as giving 100%, being honest about needs and challenges, and participating authentically. They stressed that meaningful engagement was the only way to truly benefit from therapy and heal from IPV. I would say use it, because it does work… And be honest of what you need, how you need things, how do you expect your therapy to go. Let them know of things that you are uncomfortable with, what are some other things you are comfortable with. And also, just be open, but in the best way that you feel like is open to you. Write it down for yourself, what it will look like, write it down. If you are hesitant, write why you are hesitant. And write if you are hesitant with boundaries you can create, so you can have a safe space. Because this is your therapy session. So, make it your own. Make it what you want to talk about. (Vanessa Binx)
Finally, participants encouraged survivors to “shop around” until they found the best therapist for their needs and style. They stressed that the right fit is critical but can be elusive, so survivors should be ready to try out a few therapists in the process. Implicit in this advice is for survivors to be persistent in their healing journey and not give up due to a bad match. If you feel like something is off, and you feel like you can't express that to the therapist right away, then you need to find a new therapist. Because a therapist should make you feel like you can talk to them. It's okay to shop around. (Athena)
Participants also noted that it is especially important for IPV survivors to “shop around” because it puts them in control of their healing and can help them regain some of the power and agency that abusive partners took from them. They also wanted survivors to know they have the right to shop around at any point, even if there had been a good fit. For example, Jaime talked about ending a situation with a therapist that grew to feel “enmeshed” and “stagnant.”
Theme #2 for survivors: You need therapy to heal and move forward
Participants were emphatic that IPV survivors need therapy to heal and move forward. They asserted that therapists have the expertise, skills, and objectivity to help survivors recover from the negative effects of IPV and other traumatic experiences. Two sub-themes emerged: the impact of IPV is complex and enduring and you are not just going to “get over it” on your own.
Drawing on their own experiences, participants described IPV victimization as deeply traumatic with long-lasting negative effects on a range of domains, including basic functioning. You're not going to be able to heal if you don't address the things that hurt you. I mean, everyone is constructed differently, so some people are able to just bury it in their mind and keep going forward. But I don't know. From my experience, it had to be dealt with because I was there for so long. … I was worried when I first moved into my apartment. I don't know why these thoughts were so intrusive, but I just felt like he was going to come get me. He was going to do something to me and the kids. I used to sleep with a bat on the couch. ... That's craziness, but that's trauma, not just paranoia. (Kitty)
The enduring nature of IPV means that healing can take time because survivors “have a lot of rebuilding to do,” and there will be good days and bad days—even with a therapist’s support: Most persons, after going through a traumatic experience, tend to lock themselves. So, therapy is like a driving force that gets you back on track into finding yourself and provides you with resources as to how to get back to where you were. It's not like something that's going to happen overnight, but as time progresses, then you'll feel like you’re getting somewhere. (Pink)
Additionally, participants stressed that survivors are not going to just “get over it” without some sort of therapeutic intervention. Although participants understood the urge to adopt a “mask,” pretend it never happened, or process it with friends and family, they had experienced firsthand that these strategies were unhelpful and even counterproductive to healing, with many reporting only seeing positive change when they started therapy. But for victims, please. It is so helpful, it's so helpful to your ... just living beyond what you've experienced. It helps you to be a better mom, a better parent, a better individual. It's just been so helpful to me. I would just recommend it to everyone. Please don't just brush it under the rug and say, “Okay, I'm out of this situation now. I'm good. I can move on with my life.” No. Don't do it because it's going to pop up and it might pop up in a negative way, and you're like, “Why am I feeling this way?” (Phone)
Theme #3 for survivors: Therapy is hard but worth it
The third and final theme regarding advice for survivors was the acknowledgement that therapy is hard (and requires hard work), but the struggle is worth the outcome. According to Mia, “when it comes to domestic violence, or any type of abuse, it’s very hard at first because, well, it is going to be hard, and to be honest, it’s going to be hard at first because you might not know if this person can even help you,” but that doing the work is much better than “being scared and not doing it.” Three sub themes emerged: “you have to be your own best friend sometimes,” let your guard down, and if it helped me, it could help you too.
Participants encouraged survivors to “be their own best friend,” which meant speaking up in therapy, sharing at their own pace, and focusing on their needs. They discussed how doing so can be hard for survivors, even unnatural, because they have had to do the opposite with their abusive partners. Blue said, “Love yourself enough to know that you at least deserve someone to hear you out, hear your problems out so that they can be on the alert, and they can be able to even maybe save your life.” Although related to the prior subtheme of meaningful engagement, being your own best friend refers to the hard work of learning to prioritize oneself.
Participants also advised survivors to let their guard down, which can also be hard due to fear of being shamed and victim-blaming. Participants acknowledged that this fear was valid, as many of them had experienced such treatment by former therapists. Nevertheless, they argued that taking the risk was worth the reward, which will elude them if they stay guarded. As Jaime explained, “Yeah, that would be my advice, to be patient with yourself. This is a journey, not a destination. This is not overnight. … This is work. You need to want to do the work.”
Finally, most participants shared details of traumatic experiences in their past and present (e.g., homelessness, poverty, child abuse) that compounded the MH effects of IPV. They argued that if therapy could help them, it could help any survivor and pointed to the improvements they had experienced domains such as emotion regulation, self-awareness, parenting, and overall quality of life. The following quote from Sky speaks to the three sub-themes just discussed: Your future depends on it. So I would say, don't give up on yourself. You matter, and your life is so important, and you need to do everything in your power to help yourself, because you have to be there for yourself. You have to be your own best friend sometimes. And there are times where you may not have been able to change your circumstances when you were younger, let's say, but maybe now you can be the person that you wish you had when you were younger for yourself and surround yourself with other people, professionals, who can be there by your side and lead you along this journey that feels scary. And they could help you, and they could lead you to the other side, to safety and to happiness, and to a good life. (Sky)
Advice for therapists
Participants offered nuanced advice for therapists on how to improve the duration and effectiveness of their work with clients who have experienced IPV and housing instability. Three major themes emerged: domestic violence is a “deep subject” that requires specialized education, “follow the survivor,” and “have a holistic approach.” These themes were supported by findings from the focus group with therapists, with quotes from them woven throughout.
Theme #1 for therapists: IPV is a “deep subject” that requires specialized education
Participants talked at length about the complicated dynamics of IPV and the unique needs survivors have as a result. One participant called IPV a “deep subject,” and many stressed that therapists must receive specialized education on the different types of abuse and range of negative effects. Within this theme, three sub-themes emerged: every survivor’s experience is different, some survivors need “deprogramming,” and attention to power dynamics is critical.
Participants advised therapists to know that every IPV survivor’s experience is different; thus, survivors’ needs and trauma symptoms will manifest differently, especially if they have survived other types of interpersonal violence. For example, one of the therapists, Feline, spoke of a client in her 70s who “has never seen a therapist in her whole life” and “has so much in her family history that has been unprocessed—so much addiction, so many other kinds of violence.”
Client participants offered the following advice on how to approach this diversity of experience. First, therapists need to learn all that they can about IPV’s forms, tactics, and effects. I think the most important thing for therapists working with domestic violence survivors, is for the therapist to be armed with domestic violence information. It’s a really deep subject. So they have to know about domestic violence issues. They have to know about different forms of abuse that a person may have had and how that affected them and what kind of traumas they encountered as result of how it affects them in their daily lives, and what kind of challenges they may have as a result of what they’ve been through. (Sky)
One participant, Athena, was adamant that therapists need special training to work with people who “just left” versus “out long enough,” because “the first few months out is torture.” Second, therapists should know that IPV can elicit certain responses in therapy, such as saying what the therapist wants to hear, trouble trusting them, and being “easily triggered.” Sunshine, a therapist, concurred: “just a warning letter from housing management really triggers their trauma reactions and responses. And, you know, that could be like an hour and a half of just holding space for them about it.” Third, participants warned therapists to never say they know what a survivor is going through even if they are survivors or have worked with many IPV clients. Be careful with what you say to the person. I had another therapist who would tell me “I know what you're going through.” And I told her, you don't know, just because you have an idea, but each person is individual and sometimes you have to be very careful with words that can be misinterpreted and the tone they use. (Leslie)
The second subtheme was that some survivors need “deprogramming.” Participants advised therapists to be prepared to work with survivors who have internalized aspects of IPV so deeply that they carry them long after the abusive situation ends. They described how survivors “lose themselves,” “doubt their own voice,” and not recognize their experience as abuse, due to having been “gaslighted,” “dehumanized,” and “trauma bonded.” Johnny Bravo said: In some situations, people stayed in that situation for so long, that’s all they know. … Even though they did seek out to get help, they still believe that person is still a good person like I’ve done. As a result, some survivors need “deprogramming and rehabilitation of basic human function.” A lot of survivors will live in an abuser mindset. … I was gaslighted a lot, and I was almost brainwashed to the point where I was believing the things that he was saying to be true. And sometimes you need to just have someone tell you, ‘yeah, that's not healthy, that's not accurate, you may think that that's your reality right now, but that's actually not true.’ And that's the kind of thing that helps break the chain, break the cycle, and just help the survivor to come back to themselves in a sense. (Kay)
The third subtheme was attention to power dynamics is critical. Although many therapists are trained to acknowledge power dynamics and differentials in the provider/client relationship, participants stressed that this dynamic requires special care when working with IPV survivors. Participants explained that the power dynamics between a therapist and an IPV client can imitate or replicate power dynamics between a survivor and their abusive partner. For example, a therapist’s approach can make survivors feel like they cannot be in control of the process, decide what they disclose, advocate for themselves, or shop around for a different therapist. Therefore, it is critical for therapists to be hypervigilant about these dynamics and acknowledge them directly with the survivor—especially when survivors have children, due to the very real fear of child welfare involvement and loss of custody. I remember the first few times I met with different therapists. Again, I was coming from a place of fear, and I felt small. I mean, I didn't feel heard. So now you're being vulnerable and talking to someone that does have some power. This person had the ability to write something down in her notes that could impact the psychiatrist's judgment about you or anybody reading your case notes. … You feel like everyone is coming for you, you feel paranoid, you feel scared. There's a state of anxiety and power dynamics. (Jaime)
Theme #2 for therapists: “Follow the survivor”
The second theme was to “follow the survivor.” Participants advised therapists to create a safe environment where survivors can feel comfortable choosing when and how much to discuss their experiences, thoughts, and feelings. They described the pillars of this approach as patience, validation, active listening, empathy, and genuine interest in clients’ wellbeing. Two sub-themes comprise the theme: be patient and provide a non-judgmental space to facilitate open disclosure.
Participants stressed the importance of being patient, especially in terms of taking time to know what survivors feel comfortable discussing. They advised therapists to avoid asking too many questions about IPV, especially initially, or survivors might “shut down.” For the reasons already mentioned, survivors might not be ready to talk about IPV or only want to share a few details. Survivors also might have times when they are not able to process IPV. As Star 2.0 said, “Sometimes I don’t really want to try to work through it. You know? I don’t want no one looking at me crying, … feeling sorry for me. I don’t like that feeling. …I just want to be in myself.”
The second sub-theme was for therapists to provide a non-judgmental space to facilitate open disclosure. Participants explained how many survivors are too ashamed or embarrassed to discuss details of their IPV or other personal details, and they either anticipate being judged or have been judged in the past by other professionals. They urged therapists to listen, demonstrate empathy, validate, provide supportive reflection, and display unconditional positive regard: I think that it takes a very unique skillset. I think the person delivering these services has to be very compassionate, empathetic. I think that being very patient and making sure that the person receiving these services does feel supported by allowing them to tell their story. ... Of course everyone is different race, creed and life experience, but I think that the reason I say patience and also being aware, is because what I found in myself was that there was almost a level, a level of shame of my bringing up certain situations for fear that the person would say certain words that maybe sounded judgmental. (Jaime)
Therapists echoed these sentiments. For example, Feline described validation as “at the core of any transformation to take place,” and Sunshine concurred: “It’s challenging. I want to comfort and assure them it’s going to be okay. But their reality is definitely, very, very, very different.”
Theme #3 for therapists: “Have a holistic approach”
The third theme for therapists was to “have a holistic approach,” which included two sub-themes: use individualized techniques, and acknowledge that DV is not the only, or even the top, priority. Essentially, participants’ advised therapists to view survivors as whole people and include all aspects of their lives into the therapeutic process. The first subtheme that therapists should use individualized techniques connects to and builds on everyone’s experience of abuse is different and follow the survivor. Therapists should use what they learn from listening to provide helpful therapeutic techniques that align with the survivors’ needs and desires, encourage them to practice techniques outside of therapy sessions, and tweak them as needed. As one therapist, Sunshine said, “[given] their array of experiences, interventions kind of have to like, really shift in mold according to what is best for the client, not even what’s best for the situation.”
The second subtheme was to acknowledge that DV is not the only, or even the top, priority. Participants stressed that many survivors, especially those in situations like their own, are dealing with many major stressors that are harmful to their MH. Thus, therapists need to understand that survivors might have other aspects of their lives that they want to process before even mentioning DV. For example, participants described how they had to prioritize other MH diagnoses (e.g., agoraphobia), physical health (e.g., hospitalization), and housing incidents (e.g., abusive neighbor) over DV. In addition, therapists must be willing to step outside of traditional MH support and provide light case management (e.g., referrals, warm handoffs) to help alleviate stressful practical needs. Finally, these stressors sap survivors’ time and energy for therapy. Thus, tending to practical needs might include being flexible in terms of meeting virtually versus in-person, giving frequent reminders, and being understanding of last-minute cancellations or disruptions due to demands such as single parenting and unreliable transportation. Depending on what the therapist is, if it's a clinical social worker, then they may be able to provide more stuff. It's like, “Hey, I'm able to provide X, Y, Z.” Sometimes the survivor might be like, “I have no idea what to ask for. They have no idea what's out there unless they ask.” … Some people don't ask. It's hard. (Glitter)
Therapists’ discussions of their work reinforced this sub-theme, especially in terms of housing instability as a major stressor for survivors. Lollipop said, “they have so many needs—housing, employment, childcare—and they are moving to a new neighborhood, a new community that they know nothing about,” which can cause “panic” and “being cut off” from informal and formal support. They described how housing stressors loom large in sessions: “it becomes like 60% of sessions when it is their time to recertify, or when they get notices that they’re not paying certain parts, or when interpersonal conflicts with their landlords.” Thus, they felt they should “support our clients with legal resources or housing resources or support groups.” Sunshine summed it up well: “We’re social workers, right? We are helping them navigate systems.”
Discussion
The goal of this descriptive qualitative study was to better understand how MH providers, including social workers, can improve outreach and response to IPV survivors who have experienced housing instability. Our study offers several valuable contributions. First, it centered the expertise of an understudied, multiply marginalized population with unique MH therapy needs. Second, it explored how IPV survivors can maximize their experience as therapy clients. To our knowledge, prior research has focused exclusively on improvements for therapists and systems. Finally, our findings (see Table 2) offer useful strategies that social work therapists and programs can use to facilitate sustained and beneficial MH therapy with this population. Before describing study implications, we place the findings in the context of prior research.
Study findings overwhelmingly underscore the importance of what has been called survivor-centered or survivor-defined practice (Goodman, Thomas, et al., 2016), which involves applying many of the tenets of feminist therapy theory (Brown, 2018) to work with IPV survivors. For example, survivor-defined practice is characterized by facilitating choice and control, being collaborative, and respecting survivors’ unique situations and needs (Goodman, Thomas, et al., 2016). Aspects of a survivor-defined approach were threaded throughout participants’ advice for therapists; for example, they encouraged them to know that every IPV survivor’s experience is different, “follow the survivor,” and “have a holistic approach,” because doing so puts the survivor in control of their therapeutic journey. Aspects of survivor-defined practice were also evident in the advice for survivors. By advising survivors to “take the leap,” “be their own best friend,” and “shop around,” participants encouraged survivors to center themselves and be the person to define the therapy experience. These findings align with those of prior studies on survivors’ MH therapy experiences, especially the need for self-determination, an individualized approach (Sorrentino et al., 2021), and empowerment (Grillo et al., 2021).
Being in control of the therapy process appears to be especially important for survivors who are dealing with housing instability. The participants in this study (therapists and clients) described housing as an acute source of stress due to aspects such as trouble paying rent, unsafe buildings and neighborhoods, conflicts with landlords, and the voucher recertification process. Therapists should be aware that housing stressors can supersede other concerns, exacerbate existing trauma symptoms, and overwhelm coping strategies; thus, these stressors become the therapy work. Moreover, survivors might not be able to process anything until these stressors subside; thus, participants encouraged therapists to assist with practical needs as part of their MH care. These findings align with feminist therapy’s prioritization of structural oppression (Brown, 2018), underscore the notion of survival-focused coping among survivors caught in a cycle of poverty and housing instability (Goodman, Smyth, et al., 2009), and support research demonstrating that provision of instrumental support is a key facilitator of relationship-building between service providers and survivors (Goodman, Glenn, et al., 2009; Sorrentino et al., 2021).
Findings also support the need for a trauma-informed approach, a widely-acknowledged best practice for IPV survivors (Kulkarni, 2019). In their advice for survivors, participants expressed a deep understanding of how difficult it can be for survivors to take the leap with therapy due to the impact of IPV and other forms of trauma. However, that same understanding of trauma is what informed their emphatic assertion that survivors need it to heal and that the benefit is worth the hard work. Likewise, participants identified elements of a trauma-informed approach in their advice to therapists. For example, they encouraged therapists to have a solid knowledge of trauma, understand that trauma symptoms manifest differently for each survivor and that survivors are likely carrying other traumatic experiences into therapy that need to be processed. Indeed, research supports the prevalence of other forms of trauma among survivors who have been homeless or unstably housed (Chiaramonte et al., 2022; O’Campo et al., 2016).
Limitations and implications for future research
Several limitations should be considered. First, participants were recruited from one agency, which reduces the level of transferability (Stahl and King, 2020). That said, participants drew from a wealth of prior experiences in MH therapy to inform the advice they offered. Second, although participants had experienced housing instability recently, all were living in their own units with a housing voucher at the time of the interview, making their level of housing stability considerably higher than that of survivors in shelters, doubled up, or with abusive partners. Third, this study cannot speak to survivors’ advice on IPV disclosure to therapists because our participants entered the therapeutic relationship having been identified as an IPV survivor at outset via the warm handoff. Finally, this study used a qualitative design, which was necessary due to scarce research. Findings can be used to inform quantitative studies on topics warranting attention, such as the scope of MH therapy use among this population, training and intervention needs for therapists, and integration of case management as part of therapy practice.
Implications for practice and policy
Study findings illuminate how social workers are uniquely well-equipped to provide MH therapy to IPV survivors with experiences of housing instability and homelessness. First, social workers are trained to practice using a “person-in-environment” lens, in which the environment includes factors at the interpersonal, organizational, community, policy, and structural levels (Kondrat, 2013). Consideration of contextual factors inevitably translates into therapy practices that avoid a “one-size-fits-all” intervention approach and support clients with their emotional and practical needs. In addition, the social work field has adopted trauma-informed care as a core approach; thus, social workers are taught to ask questions about what happened to clients (rather than why something happened), and they consider the trauma of structural forms of oppression (e.g., housing discrimination) in addition to interpersonal violence and abuse (Levenson, 2017).
Despite a natural alignment between social work approaches and our findings to “follow the survivor,” and “have a holistic approach,” social workers rarely receive specialized education on the “deep subject” of IPV (e.g., types, dynamics, and differing impact and response). Thus, many are unprepared to deliver therapy in the ways that our study participants advised. Indeed, research has demonstrated that social workers often lack the knowledge and skills to assess and support clients who have experienced IPV (Fedina et al., 2018; Sutton et al., 2021). In addition, negative attitudes and stereotypes about people experiencing homelessness exist even among social workers (Gallup et al., 2023), which can further stymie the ability to provide empowering MH therapy to unstably housed survivors. Study findings highlight the need for curricular change to ensure that social workers—and all MH professionals— are provided with a depth of knowledge about IPV that survivors desire and deserve, including pathways into homelessness and housing instability and the intensely stressful and overwhelming nature of these experiences. Students in other MH programs should also be encouraged to adopt a feminist therapy approach when working with this vulnerable population, including recognizing that practical support is a critical part of their role and essential to the therapeutic alliance (Goodman, Fauci et al., 2016).
Second, low-cost MH therapy for survivors is often scarce, inaccessible, and short-term (Bent-Goodley et al., 2023; Kennedy et al., 2023). Our findings are a call to action for increased options for affordable, long-term therapy so that survivors have an opportunity to fully process their experiences and, ultimately, heal. This call aligns with the Social Work Grand Challenges, an ambitious initiative that aims to eliminate society’s most entrenched problems through the coordinated efforts of researchers and practitioners (Teixeira et al., 2021). Finally, findings highlight a need for creative strategies to educate IPV survivors about therapy and encourage them to participate (e.g., targeted social marketing campaigns). Peer-mentor programs, whereby survivors who have participated in MH therapy share their own experiences and tips for success with other survivors (e.g., “shop around” “it’s hard but worth it,”), might be helpful in increasing interest and sustaining engagement. Preliminary evidence suggests that survivors and staff welcome the opportunity to learn from peer-mentors (Garnsey et al., 2025; Kulkarni, 2019). These programs also align with feminist therapy theory (Brown, 2018), because they elevate the expertise of people at the margins, which is necessary for individual and structural change.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Leona M. and Harry B. Helmsley Charitable Trust.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.