
Abstract
Background:
Physical and psychological self care coping styles affect the quality of life among patients with heart failure. Understanding coping styles and related factors is important.
Aims:
1) To understand coping involved with self care of physical and psychological aspects in chronic heart failure patients and 2) to understand the associated factors with self care coping.
Method:
A systemic review of databases PubMed, CINHAL, PsycINFO and Airti Library were searched with key terms: ‘heart failure’, ‘coping’ and ‘self-care’ for the period of January 1984 to October 2013.
Results:
Twenty-six studies were included. Emotion-focused coping (acceptance and disavowal) and problem-focused coping are positively associated with better physical and psychological self care, whereas an emotional approach with escape avoidance was negatively related to adaptive self care. Enhancing the use of emotion-focused coping with acceptance could facilitate problem-focused coping regarding physical self care (medication and dietary adherence) and reduce adverse drug effects. The associated factors in coping styles of physical and psychological self care included socio-demographic factors, health condition-related factors, patient-related factors and spirituality and religion factors.
Conclusion:
Emotion-focused coping with acceptance and disavowal, as well as problem-focused coping, may positively influence physical and psychological self care. Health care professionals should accept and allow patients to use emotion-focused coping, then help patients to use problem-focused coping skills. The influencing factors have important roles in individuals’ coping styles. There is a lack of experimental and qualitative research to determine how the influencing factors affect self care coping, since this review is primarily of revealed correlational studies.
Keywords
Introduction
Heart failure is a serious disease with poor prognosis. The prevalence rate is around 5%–10% in the United States of America, 1 0.4%–2% in the European Union, 2 and approximately 5.5% in Taiwan. 3 Heart failure patients experience multiple symptoms of physical and psychological distress including dyspnea, exercise intolerance, fatigue, pain, depression,4,5 and problems regarding concentration and memory.6,7 The patient’s decreased physical and psychological functioning often contributes to poor quality of life (QoL). Self care can influence QoL and the ability to carry out activities of daily living. 8 Insufficient self care appears to be the major contributor to hospital readmission;9,10 more than 50% of heart failure re-hospitalizations and disease exacerbations are due to poor heart failure self care.11,12 An increase in the quality of self care could avoid the deterioration of symptoms and improve QoL. 13
Self care is a complex set of activities fundamental to the maintenance of health and QoL. 14 The World Health Organization defines self care as ‘all health decisions people make for themselves and their families to become and remain physically and mentally fit.’ 15 Self care includes daily activities aimed at maintaining physical stability as well as psychological status. 16 Physical self care in heart failure patients traditionally focuses on the behaviors of medication adherence, dietary restriction,14,16 daily weight monitoring and exercise adherence.18,19 The psychological aspect of self care includes mental responses and the ability to cope with the stress and challenges of heart failure.
Coping with the physical and psychological impacts of the illness is an important aspect of long-term life adaptation and self-care efficacy for heart failure patients. 20 Individuals deal with stresses using both emotion-focused coping and problem-focused coping mechanisms. Emotion-focused coping involves strategies such as avoidance, disavowal, denial, withdrawal and behavior disengagement, while problem-focused coping includes active coping, problem solving, planning and information seeking.21-23 A integrative review by Graven and Grant 24 revealed that problem-focused coping strategies were more likely to facilitate self care and the decision making process that determines actions aimed at maintaining stability of health than emotion-focused coping.
Although several review articles have explored the experience of living with heart failure, the relationship between depression and coping, and how coping strategies influence QoL,8,25,26 however, most have not specifically addressed the relationship between coping and self care. The purpose of this review is to understand the coping of psychological and physical self care and the associated factors with self care coping in patients with CHF. The goal is to provide information that will be useful for health care professionals to promote patients’ health self-care behaviors and enhance their psychological and physical well being.
Methods
A literature review of the databases PubMed, CINHAL and PsycINFO as well as the Airti Library was performed using the following key search terms: ‘heart failure’ and ‘coping’, which were then combined with ‘self care’. The search was limited to publications from January 1984 to October 2013. (See Figure 1.)
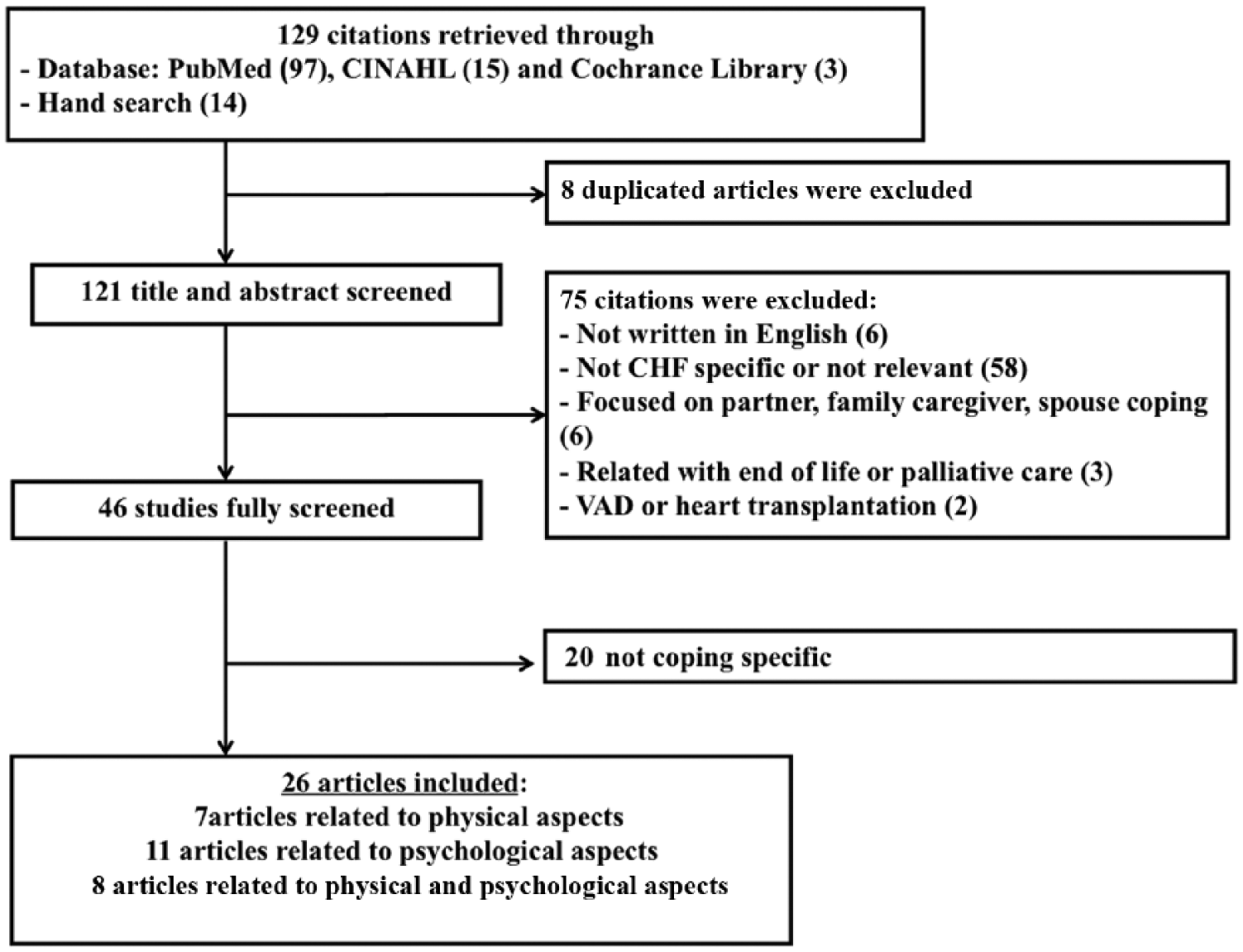
The process of selection of articles for inclusion.
Manuscripts were retrieved and reviewed utilizing the following inclusion criteria: the study investigated the association of coping and physical and/or psychological self care in heart failure patients, and its related factors. Exclusion criteria included the following: (a) the article involved patients with an implanted mechanical device, such as a ventricular assist device, because of the self care issues of these were different from patients without implanted mechanical devices; (b) the article was associated with end-of-life or terminal stage coping, because end-of-life care is not the focus of this review; (c) the study did not focus specifically on chronic heart failure (CHF) patients; (d) the publication included family caregiver, partner or spouse’s coping; (e) non-English or Chinese publications.
Studies were screened using two quality appraisal tools. The first was the Critical Appraisal Skills Program (CASP) 27 tool for qualitative studies, which ranks studies from 0 to 10 for 10 criteria. Studies evaluated by this test were rated low (0–3), moderate (4–6) or high (7–10). The other was Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) 28 for longitudinal and cross-sectional studies which uses scoring for 21 criteria to rank studies as low (0–7), moderate (8–14) or high (15–21). All studies used for this review were ranked from moderate to high according to CASP and STROBE criteria. Data extraction was conducted by a single reviewer and discussed with the co-author. Information about study characteristics (population of the study, subjects’ baseline characteristics, variables, and measurement instruments) and details of the results were extracted. All articles chosen (n=26) for inclusion are presented in Tables 1, 2 and 3 in the Supplementary Material online.
Results
Study characteristics
A total of 129 articles from the databases were identified, 121 were screened through title and abstract. Articles which did not meet the inclusion criteria were excluded (n=75). A total of 46 articles were fully screened, leading to additional exclusion of articles that were not coping or self care specific (n=15) and candidate review articles with purposes different from this study (n=5). Post-screening, 26 papers met the criteria for inclusion in the review and also reflected the concepts of physical and psychological self care coping strategies. The selected papers included qualitative studies (n=5), quantitative studies (n=20) and one study using mixed methods (n=1). Papers ranked moderate (n=3) or high (n=23) for quality, with primary weaknesses being an overreliance on convenience sampling and vague information regarding recruitment strategy.
The final 26 studies involved a cross-sectional design (n=19),20,21,29-45 with one longitudinal design study, 46 five qualitative studies6,10,47-49 and one mixed methods design study. 50 The sample sizes ranged from 11 to 116 patients. The majority of studies utilized convenience sampling (n=18), though two studies were based on race/ethnicity sampling48,50 and one study used gender-based (female) sampling. 32 The mean age of study participants ranged from 59 to 74.4 years old. Participants with a New York Heart Association (NYHA) classification ranging from class I to IV were included in all studies. Many of these studies (n=10) defined the concept of coping according to Lazarus and Folkman’s Process Theory of Coping; one study additionally applied segments of the Moos Crisis Theory as their theoretical framework 29 and one study applied the commonsense model of illness theoretical framework to their study to investigate the association of accuracy of heart failure illness beliefs and depression. 44 Three studies defined physical self care as the ‘cognitive and behavioral process aimed at maintaining hemodynamic stability and managing symptoms’.10,40,48 However, no study evaluated in this review used a clear definition of psychological self care.
Furthermore, several studies (n=7) investigated the relationship between coping and physical self care maintenance, such as compliance or adherence.10,31,33,36,37,40,45,48 Eleven studies particularly focused on exploring the relationship of coping and psychological symptoms such as depression and anxiety.6,29,30,35,38,39,42-44,46,47,49 Eight studies explored the coping and related factors on both physical and psychological aspects of self care. The main characteristics and results of the selected studies in coping in physical self care, coping in psychological self care and coping in physical and psychological self care are shown in Tables 1, 2 and 3 respectively in the Supplementary Material online.
Coping styles in physical self care
Fifteen studies investigated the impact of coping strategies related to physical self care (Tables 1 and 3 online), such as studies focused on physical symptoms and functional status,10,20,21,34,40,48 dietary adherence,10,40,45 daily weight monitoring,31,45,48 medication adherence,10,31,40,45,48 exercise adherence 45 and adverse drug effects (ADEs).36,37
Patients that engaged in more problem solving and acceptance coping were more likely to engage in self care. 10 A qualitative study explained that during times of high levels of physical or social turbulence, patients tended to use problem-solving strategies to cope. 48 The use of problem-focused coping strategies had a significant positive correlation with good physical self care, such as medication adherence,10,40,45,48 dietary adherence,10,45,48 exercise adherence 45 and daily weigh-ins.45,48 A qualitative study explained problem-focused coping as ‘operating’ and ‘being piloted’ (e.g. ‘I try to walk every morning to keep healthy’ or ‘[I am] relying on the health professionals; they tell you how to cope’). However, this study also pointed out that ‘operating’ was sometimes also related to negative self care behaviors (e.g. ‘I grab a cigarette and it helps to calm me down’). 48
Moreover, the use of certain emotion-focused coping strategies, such as acceptance, was positively associated with less physical limitation. 21 In contrast, the use of some emotion-focused coping strategies, such as avoidance, denial, guilt, ignoring issues, withdrawal and venting, were positively related to poorer physical functioning.10,20,21,34 Additionally, participants reported that social support seeking (emotion-focused coping) and information seeking (problem-focused coping) were the most common strategies for patients with heart failure to cope with ADEs. Also, the study found that patients using more acceptance-based coping and engaging in seeking social support (emotion-focused coping) had a tendency to use problem-focused coping to adapt to ADEs. 36
Problem-focused coping (e.g. problem solving, information seeking) and certain emotion-focused coping (e.g. acceptance, social support seeking, emotion support) were associated with better physical self care in the form of medication adherence, dietary and exercise adherence and daily weigh-ins. This section has shown that more use of problem-focused coping is correlated with more positive physical self care outcomes. Furthermore, enhancing the use of acceptance coping (emotion-focused coping) could facilitate the use of problem-focused coping to cope with the physical self care, such as medication and dietary adherence, and reduce ADEs.
Coping in psychological self care
Nineteen studies investigated coping related to the psychological aspects of self care, most commonly related to depressive and anxiety symptoms (Tables 2 and 3 online). Problem-focused coping was associated with a positive impact on psychological self care. Problem-focused coping, such as problem solving, was associated with less depression, anxiety,29,34,38,43 less fatigue and more vigor. 35 One study further indicated that adaptive coping strategies, such as task-focused coping, problem-solving coping, or engagement, were significantly associated with better well being. 39
Emotion-focused coping, such as acceptance and disavowal approaches, was related to mental adaptation in psychological self care. 47 Acceptance was found to be associated with positive mental status and reduced emotional problems such as depression.20,21,47 Disavowal is a way of palliating emotional reaction to the fact of disease threatening one’s life; one qualitative finding revealed that disavowal was the most common coping style among heart failure participants with moderate-to-severe physical limitations, as it helped to moderate the impact of heart failure. 47
In contrast, several studies indicated that greater use of the emotion-focused coping strategies of escape avoidance,29,34,35,42,47 denial, venting, behavioral disengagement20,21,29,42 and self blame20,21,29 was significantly related to higher anger, anxiety and depression. Furthermore, maladaptive emotion-focused coping styles predicted negative effects that subsume a variety of adverse mood states such as guilt, fear and nervousness. 29 In addition, another study discussed coping styles such as anger-in (withholding anger) and anger-out (expressing anger) to measure the coping styles among female participants. The results revealed that high anger-in individuals displayed greater depressive symptoms than high anger-out individuals. 32
In conclusion, the findings of this review suggest that both emotion-focused and problem-focused coping strategies are associated with psychological self care. Patients who used the specific emotion-focused coping of escape avoidance, denial, behavioral disengagement, venting and self blame were more prone to experience worse psychological self care outcomes.20,34,35,39,43,47 The problem-focused coping strategies (e.g. problem solving and seeking social support)6,20,35,38,42,43 and certain emotion-focused coping strategies (e.g. acceptance6,20,35,38,5,42,47 and disavowal 47 ) were positively associated with less depressive symptoms, anxiety, and anger.
Factors associated with coping in both physical and psychological self care
Additional factors potentially associated with physical and psychological self care can be broadly categorized into socio-demographic factors, health condition-related factors, patient-related factors, and spirituality and religion factors.
Socio-demographic factors considered in the studies reviewed here included age,33,47 gender,32,39,50 ethnicity, 41 employment status, 31 marital status41,43 and social support.10,40,49 Two studies found that older age was associated with higher use of acceptance and avoidance coping strategies.33,47 Three studies did not find a significant relationship between age and coping styles in physical and psychological self care.21,29,41 Additionally, Nahlen and Saboonchi claimed that there were no significant correlations between age and any coping styles used in self care. 29 Three studies described associations between gender and physical and psychological self care coping.32,39,50 A study reported that women used more problem-focused coping strategies and had better physical self care maintenance than men. 50 Another study using homogenous ethnic sampling (Black adults) reported similar results. 50 However, one study reported that male patients used more problem-focused coping mechanisms and had higher well being than female patients. 39
Only one study focused on ethnicity in correlation to coping strategies and self care, and found that problem-focused coping (self care maintenance behaviours) were significantly lower in participants of aboriginal descent compared with those of European ethnic background. 41 In terms of marital status, one study found that single heart failure individuals used more escape avoidance coping and less problem-solving coping in psychological self care, 43 while another study stated that marital status was not significantly correlated to either physical or psychological self care coping. 41 Only one study reported a relationship between employment status and self care coping. 31 Researchers stated that being employed was associated with behavioral disengagement (negative emotion-focused coping) and poor adherence to physical self care. 31
The final socio-demographic factor is social support. Riegel and Carlson found an association between physical self care, social support and problem-focused coping, such as seeking information support from physicians and emotional support from family, friends, nurses, physicians and pets. 10 Similarly, studies’ findings indicated that social support from family/friends was positively related to emotion-focused coping (acceptance), problem-focused coping and better physical and psychological self care.40,49 Additionally, the study reported that health professionals provided mental support for patients (e.g. ‘The visiting nurse…is very attentive…provides a feeling of security’; ‘I really like my doctors. I feel comfortable with them’). 10 Health provider support is obviously an important aspect; however, only one study discussed the nurses’ involvement in patients’ self care.
Health condition-related factors, such as physical impairment or limitation20,21,43 or underlying disease,31, 40 were included in this study. Increased physical impairments were associated with negative emotion-focused coping such as self blame, venting and denial.20,36,43 However, one study reported that physical functional states were not significantly related to better psychological self care coping. 21 Moreover, one study described that the presence of an underlying disease, such as diabetes mellitus, was associated with certain emotional coping strategies, such as behavior disengagement coping in physical self care. 31
Patient-related factors associated with coping with physical and psychological self care included knowledge, 32 self care confidence33,36 and personality. 30 One study found that patients with greater illness knowledge displayed more emotion-focused coping (avoidance). 32 Furthermore, one study indicated that higher self-care confidence was associated with problem-focused coping and better physical self care, 33 while a third study reported no significant relationship between self care coping and self care confidence. 36 Additionally, researchers examined the relationship between coping styles and personality in heart failure patients. 30 The findings indicated that extroverted personalities were positively associated with problem-focused coping. In contrast, neurotic personalities were moderately-to-strongly positively associated with the emotion-focused coping strategies of mental and behavior disengagement and venting of emotions. Further result also indicated that patients with neuroticism tended to have more depressive symptoms.
Two studies found that spiritual support is related to the emotion-focused coping of acceptance in psychological self care.49,50 A third study, which used mixed qualitative and cross-sectional methods, also found that spirituality helped participants to cope with depressive symptoms. 50 Furthermore, Park et al. indicated that religious coping mechanisms such as seeking God’s help reflected a mix of problem-focused and emotion-focused coping. 38 In contrast, one study found that no significant relationship exists between spirituality and physical self care compliance coping. 45
Moreover, a qualitative study revealed that some individuals came to terms with their illness and self-care experience by placing it in a larger context of meaning or life philosophy (e.g. ‘You realize God didn’t give us tomorrow. Today may be our last day and you best realize it and live that way. I think you appreciate what you have now, because there is a time coming when you will not be here’). 50
Discussion
This integrative review was aimed at examining research literature on the coping styles, self care behaviors and related variables in heart failure patients. Twenty-six studies that used a cross-sectional, longitudinal or qualitative approach to measure the associations of these factors were reviewed. Patients who used acceptance, disavowal and problem-focused coping strategies were more likely to have better physical and psychological self care. Influential factors such as being elderly, having better disease management knowledge, being employed, having an extroverted personality, and experiencing social support from spouses were more likely to produce better self-care outcomes.
Both emotion-focused coping (e.g. acceptance and disavowal) and problem-focused coping (e.g. problem solving) were positively associated with better physical and psychological self care. Previous review articles indicated that only problem-focused coping was associated with less depression and better QoL.8,26 Moreover, these findings also indicated that heart failure patients who used the emotion-focused coping strategy of acceptance tended to use problem-focused coping. Several studies agreed with this finding; emotion-focused coping could mobilize problem-focused coping and have a more positive impact on patient outcomes.51,52 Thus, it is not appropriate to only focus on developing problem-focused coping skills. Health care providers should also pay attention to helping patients have good adaptive physical self care through enhancing emotion-focused coping (acceptance) in addition to problem-focused coping. Additionally, disavowal is a coping style different from denial and it can be a way of palliating emotional strain. 47 Early research described a patient who showed a positive outlook on their situation and unusual courage facing death/illness as ‘healthy denial’.53,54 Therefore, disavowal is not a problem to be dealt with; it is a process that health care professionals should accept and respect. 53
A previous review article concluded that social support is associated with QoL. 8 Likewise, this review also demonstrates that the heart failure patients’ perceptions of support from spouses and health care providers are positively related to both physical and psychological self care. Moreover, spiritual and religious support affects heart failure patients coping with both physical and psychological self care,48,50 although one study 45 indicated insignificant results between spirituality and compliance. This may indicate that spirituality and religion may help patients to have better mental status, but can have a different result with regard to physical self-care compliance. Although spirituality and religion could be important coping resources for patients, health care professionals should avoid preconceived biases that a higher level of spirituality of patients will produce higher self-care compliance. 55
As previous studies reviewed here indicated that emotional support from nurses supported heart failure patients coping with self-care chanllenges, 10 a heart failure specialist nurse serves a vital role when involved in patient care. Several studies have shown that heart failure patient support from nurse specialists can considerably improve self-care adherence and health outcomes.56,57 According to a scientific statement from the American Heart Association, there are several ways for heart failure specialist nurses to promote heart failure self-care. 57 These include providing not only emotional support, but also strategies for enhancing patients’ problem-focused coping skills and increasing heart failure patients’ self care independency.
Limitations
There are some limitations in this study. A cross-sectional design gives a snapshot of the coping styles in self-care, but it excluded the variable of time; most findings were based on cross-sectional studies. The convenience and purposive sampling methods in the majority of studies may have selection bias. Among studies selected for this review, the heterogeneous population varied broadly from NYHA Class I to IV. However, study designs that specifically focused on one class (e.g. Class IV) might represent unique results which are not applicable to a broader population. Performing further studies with in-depth interviewing of homogenous participants is suggested for understanding more coping styles of self care in specific groups of people. Measurement tool selection should be considered for studies. Four studies used instruments with low reliability coefficients or did not report reliability.20,30,38,43
Implications for practice
Based upon this review, one can make several recommendations for the health practice and future research regarding the coping strategies and self care in heart failure patients. First, health care professionals should recognize and understand disavowal coping in patients, and create a suitable self care plan depending on the individual patient’s coping status. Second, social support from spouses is an important coping resource for heart failure patients; health care professionals could encourage spouses to provide more emotional support and also participate in heart failure patients’ self care. Last, socio-demographic characteristics, such as personality, are playing a role in coping and self care. Future intervention design or further study should consider different personalities or other factors influencing patents’ coping styles.
Conclusion
This paper presents an integrative review of the literature on understanding coping styles related to self care in patients with chronic heart failure. Emotion-focused coping, such as acceptance, and problem-focused coping may positively influence physical and psychological self care. Moreover, influencing factors play important roles in influencing an individual’s coping styles, but there is a lack of research to explore how those factors influence the coping with self care in the long term.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Health care professionals should recognize and understand disavowal coping in patients, and create a suitable self-care plan depending on the individual patient’s coping status. Health care professionals could encourage spouses to provide more emotional support and also participate in heart failure patients’ self care. Future intervention design or further study should consider different personalities or other factors influencing patents’ coping styles.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.