
Abstract
Social egg freezing has become an expanding clinical practice and there is a growing body of empirical literature on women's attitudes and the sociocultural implications of this phenomenon. Yet, its impact remains subject to ethical controversy. This article reports on a qualitative study, drawing on 18 interviews with women who had elected to initiate at least one egg freezing cycle in Belgium. Our findings, facilitated by a ‘symbiotic empirical ethics’ approach, shed light on the concerns and perceptions that accompany women's decisions while supporting a more context-sensitive reading of the ethical debate. We identified three key themes: feeling overwhelmed with uncertainty and a threatening future, bodily discomfort and distress during the medical process, and the endless pursuit of peace of mind. One of the issues that emerges from these findings is the risk ritual function of social egg freezing, referring to routine actions of risk anticipation that mitigate uncertainty and express a sense of individual responsibility. While more research is needed, this conceptualisation provides a starting point to flesh out the wider context of this moral practice and its symbolic meaning for women.
Introduction
Social egg freezing (SEF), 1 one of the newer techniques in the landscape of assisted reproductive technology, has become an expanding clinical practice and a common topic in media discussions.2,3 It is generally conceived as a means through which women may delay the decision for motherhood and genetic parenthood. Now that SEF has been in use for a decade, there is a growing body of scientific literature from various perspectives.
However, SEF remains subject to ethical controversy. On one side of the spectrum, there are bioethics scholars who argue that SEF is a welcome solution for women's changing status in modern societies, referring to trends of delaying marriage and childbearing.4,5 In this view, SEF can (on the condition that candidates receive adequate information) enhance women's empowerment and reproductive autonomy.6,7 Meanwhile, other researchers express concern about what benefits, if any, this technology can bring for women. 8 There are feminist bioethicists forewarning of the medicalisation, commercialisation and exploitation of presumably healthy women's bodies. They have argued that the social constraints confronting women, such as patriarchal norms and heteronormativity, do not receive sufficient attention.9,10 In addition, it has been suggested that SEF may give women a false sense of security and result in further harm through varying success rates and limited cost-effectiveness. 11
Clinicians have studied women's attitudes toward SEF using survey methods.12,13 These studies have connected users’ interest with being single professional women in their mid and late thirties. It has also been shown that a large majority of women find high levels of satisfaction from their choice and generally have a low prevalence of decision regret.14,15 A growing number of qualitative studies have been undertaken to explore women's motivations, mostly articulating problems with relationship dissolution and formation as key factors leading to SEF.16–19 Furthermore, research into the sociological dimension of SEF demonstrates how the practice is emblematic of the neoliberal risk society, in which individuals are proactively encouraged to take responsibility for health risks. 20 As early as 2010, Martin described SEF ‘as a tool of risk management’ that could ameliorate ‘fears of childlessness and the reproductive and genetic unknown’. 21 Other authors have highlighted how this risk management of reproduction is inherently gendered.16,22,23 As a consequence, women are positioned in a double bind: stimulated to take responsibility and to take matters into their hands but also rebuked for wanting too much in life.
To better understand the multiple meanings of SEF, we performed in-depth interviews in which women were invited to reflect on the concerns and perceptions that accompanied their SEF decisions. Three key recurrent themes appeared in our findings: (1) feeling overwhelmed with uncertainty and a threatening future, (2) bodily discomfort and distress during the medical process, and (3) the endless pursuit of peace of mind. As we will discuss, one of the issues that emerges from these findings is the risk ritual function of SEF, referring to routine actions of risk anticipation that mitigate uncertainty and express a sense of individual responsibility. By raising the issue of risk ritual in the context of bioethics and SEF, this study provides a starting point to flesh out the wider conditions and the symbolic meaning of this moral practice for women. In sum, this exploratory research supports a more context-sensitive reading of the ethical debate that often only focuses on rational considerations. It does so by taking into account the potential broader function of this particular decision.
Methods
Design
For this study, we adopted Frith's ‘symbiotic empirical ethics’ approach as a meta-ethical background position allowing us to integrate social-scientific and ethical analyses.24,25 This approach perceives theory and empirical data as mutually informing and symbiotically related. Theory can be used to highlight tensions within qualitative data while practice can expose and amend the limits of theory. As the results section of this paper shows, we did what Frith calls ‘setting out the circumstances’ and provided a more detailed and transparent description of respondents’ reasonings than is commonly found in normative discussions about this issue. In the discussion section, we connect respondents’ considerations with existing social-scientific literature on SEF, thereby introducing the theoretical framework of risk ritual to further analyse the data. Within the scope of this exploratory paper, we do not engage in normative arguments.
Participants
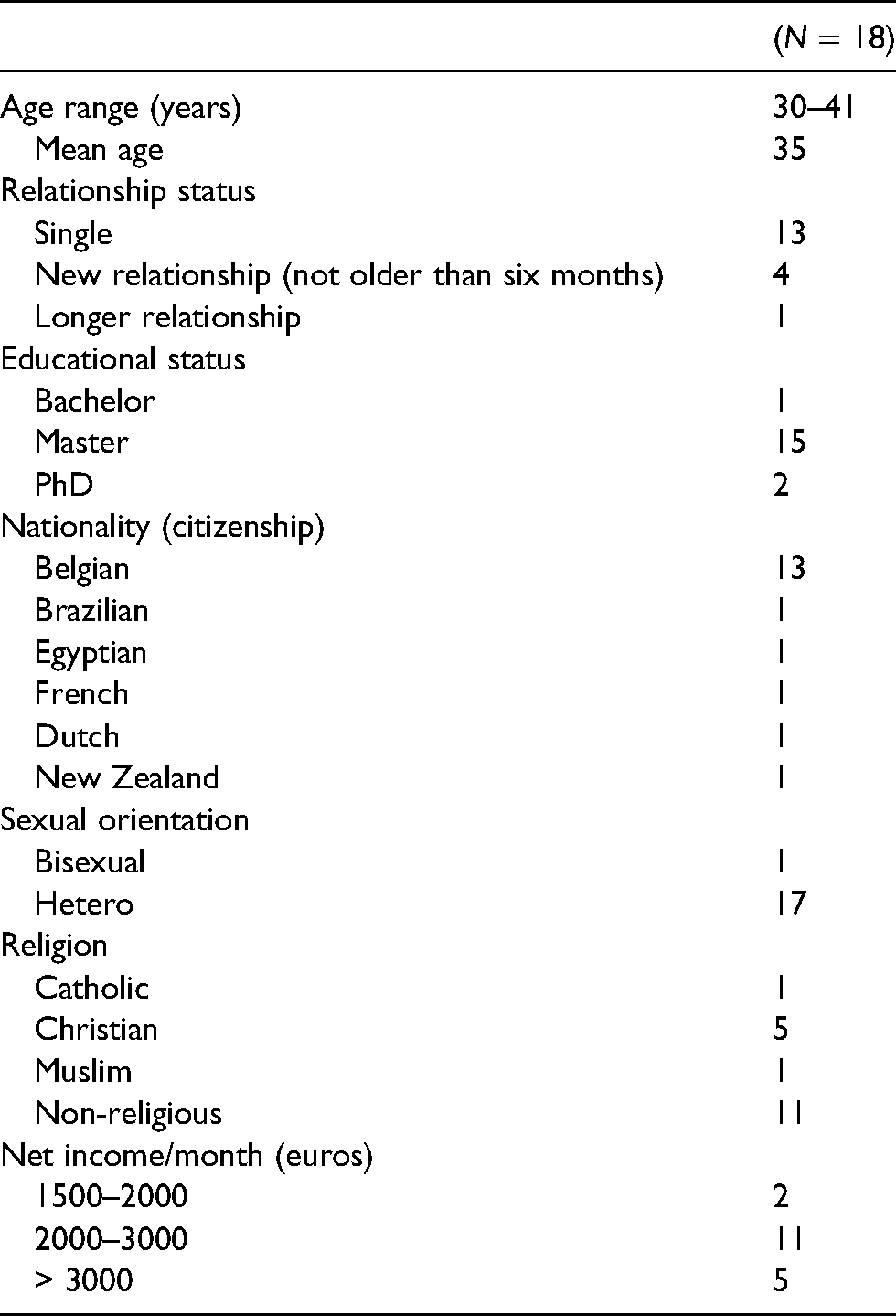
This study was approved by the Medical Ethics Committee of the University Hospital Brussels and Ghent. Seventeen participants were recruited by psychologists working at two centres for reproductive medicine in Belgium. All women who presented themselves at these centres for SEF, in a time frame of two years, were invited to participate in this study. The psychologists introduced the study and asked the permission to pass potential participants’ telephone numbers to the first author who is not affiliated to these centres. It was indicated that their participation was voluntary and would not affect the quality of their future treatment. After receiving the participants’ permission, the first author contacted each of them following an appointment for consultation or treatment. The researcher provided more information about the study and gave a copy of the informed consent form. If the participants agreed, an interview was scheduled, and the informed consent form was signed. An additional participant was recruited through social networking. The participants were primarily affluent, highly educated, and heterosexual (see Table 1).
Participants’ background.
Below, we present quotes from these participants, along with the age of each participant and a letter code expressing whether she had already frozen her eggs (f) or was still considering freezing (pf) her eggs.
Interviews
The first author performed all interviews between February 2019 and February 2021, asking open questions at the beginning of each interview to invite the participant to speak about SEF in her own words. The second part of the interview focused on four cards with controversial statements based on a previous study of bioethics literature on SEF (see Supplementary Material for the interview guide). 26 The aim was to encourage the participant to reflect on ethical concerns through Socratic dialogue.27–29 We also conducted follow-up interviews with six participants who in their initial interviews had indicated they anticipated there could soon be changes in their decision-making processes. The interviews ranged from forty minutes to two hours (on average one hour and thirty minutes). Each interview was audio-recorded and transcribed verbatim using pseudonyms. Transcripts were checked for accuracy.
Analysis
Data from these interviews were analysed using a reflexive and inductive thematic analysis combined with a hermeneutic of demystification to better understand contradictions in participants’ experiences.30,31 This means, rather than relying only on what the women made explicit, we worked to decode meanings that were more disguised. To facilitate this analysis, we made use of interdisciplinary collaborative auditing designed for empirical ethics projects. 32 The first author carried out the initial coding and, with the assistance of QSR International's NVivo 12 data analysis software, organised the codes into a potential thematic map. Auditing meetings were held during the analysis where the co-authors examined a sample of codes and discussed a possible conceptual framework. This auditing process enhanced the validity and rigour of the analysis and resulted in a more reflexive reading of the data.
Results
We identified three themes indicating that the SEF decision process is cyclical in nature (see Figure 1). The first theme was the horizon of emotions and desired outcomes moving the participants to act. The second theme was how participants perceived the medical procedure and its risks. The third theme revealed the initial state of emotions recurring after the procedure, when the participants seemed still riven by uncertainty.
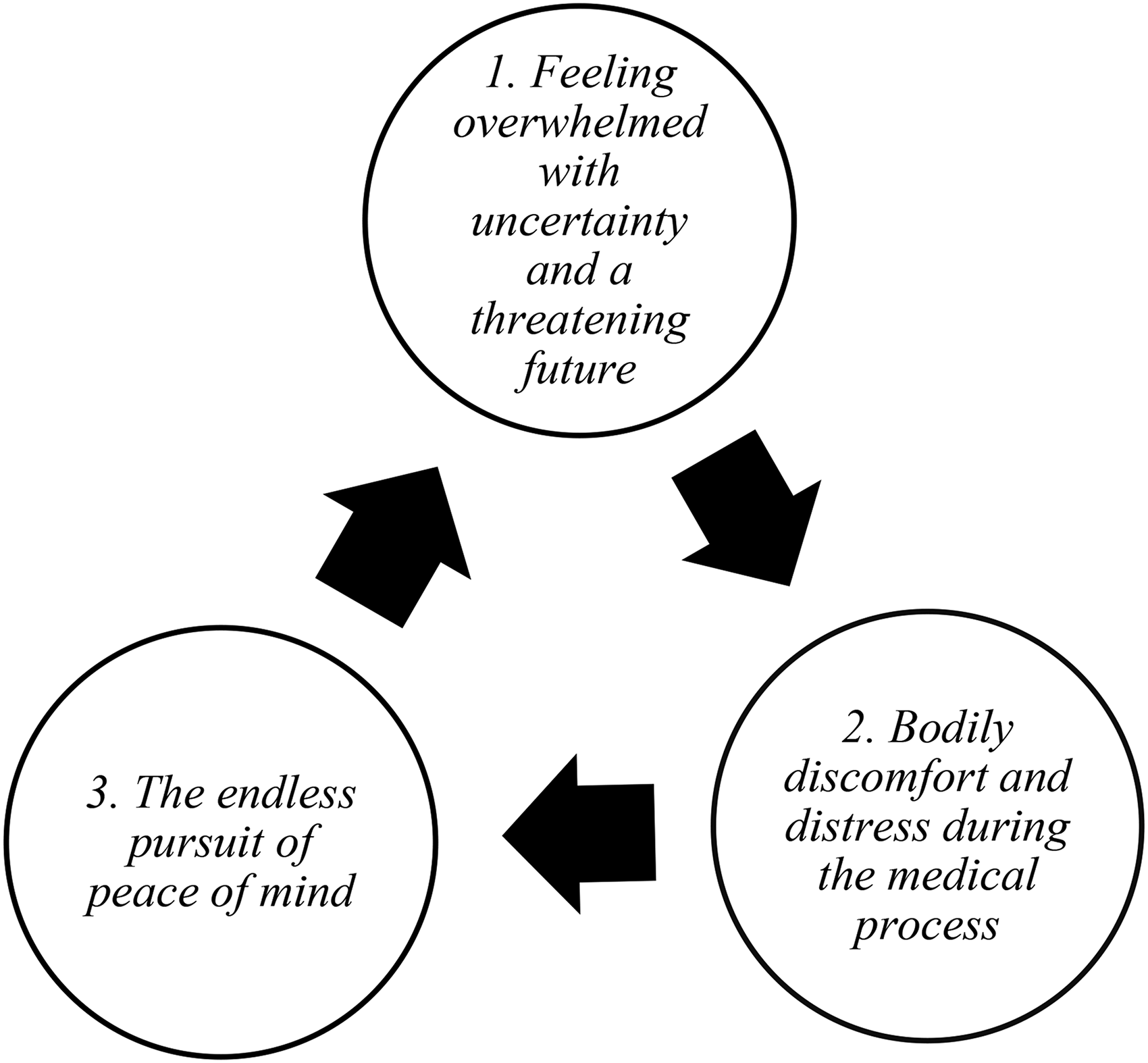
Thematic map, showing three main themes.
Feeling overwhelmed with uncertainty and a threatening future
Most participants’ accounts were pervaded by the many uncertainties they faced, especially regarding family formation – for example, finding a suitable partner and having a child. Lotte explained this as follows: I look to the future with a bit of fear because I have no certainty about what's going to happen in the coming years. And I’m a bit frightened that it might not work out. Now I have something to go back to. I’ve done something to secure my future – with the realisation that there are no guarantees but at least I have done something, and I cannot blame myself later. (Lotte, 35, f)
As Lotte's example illustrates, anticipating decision regret and related feelings of potential self-blame seemed to offer a portrait of doom. Almost every participant mentioned this feeling and they often spoke of wishing to avoid it, even at a high cost. Julia (37, f) said ‘if I have the chance to do something I would regret it more if I didn't do it’. Erika (37, pf) said, of taking action, ‘then I can't blame myself for the fact that I’m 45 years old and it didn't happen’.
The idea of staying single and never being able to have a mothering role in a child's life was difficult to accept, and this revealed feelings of failure and sadness. Nina put it this way: The fact that I’m still alone and have no family feels like a failure and is actually the result of a failure. That's a bit of a problem: Why be proud? You should have married by now and have a family, then you could have been proud. (Nina, 33, f)
Most participants did not anticipate their current life situations. These situations disrupted the participants’ ideal pictures of being married, as Isla (38, f) said, ‘to a man and have children around the age of 30’. Lan (35, pf) was one of several who said, ‘I didn't plan to have a breakup with my ex, and I didn't know that people would change their mind in a long relationship’. This chain of events seemed to give rise to a desperate need for control and to plan aspects of life's course that participants considered ‘normal’ for their age, such as a having ‘the classic family with a partner and a child with my partner’ (Emma, 35, f).
Participants seemed to long for peace of mind as the outcome of the procedure. Nina (33, f) expressed this, illustrating: ‘you’re actually buying peace of mind; the product for me is not the eggs, the product is the peace of mind’. Similarly, Lotte (35, f) said: ‘I don't think about it too much and I just do it to give myself a little peace of mind for the future’. They hoped that SEF would give them a sense of relief and relaxation about the emotionally charged decision of having children in the future.
Interestingly, this search for reassurance was usually so dominant that the preservation of a participant's own biological material became almost secondary. Rather than looking for the immediate fulfilment of genetic motherhood, it seemed that participants first wanted to forestall a lived existential deadlock of relationship uncertainties and thereby enact the transition to a ‘normal family life’ (Elmira, 38, pf).
Bodily discomfort and distress during the medical process
Although most participants in our study stated what one respondent described as ‘becoming part of the medical factory’ (Nina, 33, f), this experience was accompanied by a variety of ambivalent feelings. In a way, participants stated they believed seeking medical solutions would simplify their situation overall, but at the same time they also knew it would make their lifeworld more complex.
The medical procedure of SEF, with daily hormone injections and regular check-ups before vaginal egg retrieval, was perceived as demanding and burdensome. ‘When I’m occupied with this, it's also going on in my head’ said Julie (34, f), ‘and I have to physically look for symptoms and just be attentive. … It gives a completely different meaning to your days, especially during those injections’. They needed to discipline their bodies to a medical regime they were not used to, and some said they wanted to shield their body from the negative physical aspects of it. As Lan (35, pf) said, ‘I’m just a bit anxious about how it will go because I don't like needles – I mean mandatorily having those injections’. Several participants described experiences of bodily discomfort, such as dizziness or bloating, that confronted them with a latent pregnant body: You know a follicle is quite large, that's two centimetres. I had 20 in my belly so that was almost a pregnant belly – I didn't expect that – and it makes it extra challenging because you’re busy with that process and then suddenly you look like you’re early pregnant; that's a bit weird. (Nina, 33, f)
This quote illustrates the ambivalent feelings of the participants: unsure about becoming pregnant in the future while already being confronted with similar symptoms.
Participants often described a form of resignation during the procedure. A few interviewees said they, in Nina's (33, f) words, ‘very passively just showed up and then went with the flow’. They explained that they actively downplayed initial concerns and that their behaviour during the procedure was rather unreflexively, even wilfully, ignorant. For instance, Nina (33, f) compared herself with pregnant women who also ‘don't want to know in advance what happens and then see when it's there’. In a similar vein, Annemie (36, f) and Julie (34, f) confessed that they wanted to be ignorant to a particular level and had not consciously read all the information. They looked only at the most important things because they did not want to worry about every aspect of the procedure. As Julie (34, f) said, the focus was to get ‘to the point where I was sure I could take those injections. … I didn't need to know much more about that beforehand’.
During two interviews, it specifically emerged that the egg retrieval was a particularly painful experience: ‘that was with a needle in your ovaries, that's the worst pain possible’ (Melissa, 41, f) or ‘it was hurting a lot, I was crying because it hurt’ (Julia, 37, f). In these extracts, the operation was depicted as a distressing, traumatic experience. Whereas no other participant reported similar experiences, some described the procedure as emotionally difficult: ‘two minutes before the operation, I was lying in that bed and then I suddenly started to cry but that was pure stress or adrenaline’ (Julie, 34, f). Moreover, the egg removal seemed to evoke strong feelings of emptiness: ‘I can't really put a word on it because it's such a vague feeling of a lack in your body. … I’m not pregnant or actually there's nothing at all growing anymore’ (Laura, 31, f).
The endless pursuit of peace of mind
For some participants SEF was self-worth-enhancing and established the ability to be seen as worthwhile individuals: ‘all the pieces of my life are falling right into place, and I feel really good now’ was Nina's (33, f) way of putting it. They had done their bit and were reassured against the negative scenario of future regret: ‘it gives me some peace of mind’ were Erika's (37, pf) words, ‘that I have taken it into my own hands to the extent that I can do something at this moment’. The procedure enabled them to look beyond their current suffering and turmoil and to maintain some hope for the future.
However, the initial fear described in the first theme was still present and they were still riven by uncertainty after the procedure (cf. first quote of Lotte). Several participants stated that SEF is ‘a feeling and not an absolute certainty, you never have this, for the rest you just have to let fate take its course’ (Annemie, 36, f). Isla (38, f) described it as ‘a false sense of peace of mind’ because ‘you don't really know what the future holds.’ In the same vein, Erika (37, pf) articulated how ‘it doesn't guarantee success’ and how it gave her ‘a bit of a false form of reassurance or control’.
Melissa (41, f) described a feeling of resignation after a few years of not using her eggs: Time passes and I remain convinced that I wouldn't be able to cope with a child on my own – and I don't fall in love. So, I can look for a man, that is a completely different story but if it doesn't succeed, it doesn't succeed. … Time is just disappearing. (Melissa, 41, f)
This quote illustrates a certain awareness that some things could not be controlled and that the initial search for peace of mind moved slowly to a resigned attitude in Melissa's experience. This form of coping indicated a lack of hope and expectations of poor outcome. As Isla (38, f) highlighted it, ‘you’re still in the same boat’ and initial concerns and anxious feelings seemed to return. For these participants, SEF triggered a mourning process and a state of acceptance, a sort of ‘letting go’ while their lives unfolded: ‘By taking this step, you’re somehow admitting you don't expect it to turn out well in the very near future’ (Nina, 33, f).
Discussion
One of the most salient points is that women yearned for peace of mind and a sense of reassurance. Our interviews showed how concerns related to future uncertainties shaped this longing: this finding was linked with expectations of normalcy and desires for greater control over important life-course events related to family formation which remained in a way uncontrollable. In other words, the participants expressed a specific paradox in SEF, namely the promise of control this assisted reproductive technology encourages, makes them equally aware of the uncontrollable and may in turn reinforce anxiety and uncertainty.
Participants were aware of the limitations of SEF with respect to mitigating this paradox, but they wanted to sublimate these feelings of uncertainty. This suggested a link to what sociological literature on risk behaviour described as a risk ritual.33,34 Recent studies have introduced this concept to portray perpetual behavioural adaptations, such as wearing surgical facemasks or self-checking for cancer, that anticipate risks and result from states of uncertainty and spirals of anxiety. Risk-avoiding behaviour can be seen in symbolic acts that bring reassurance – that one is doing something in the face of a strong sense of uncertainty. The disciplined set of actions related to SEF, including interactions during consultations, reception of hormone injections, moments of egg retrieval and bodily recovery, seems to function as a set of risk ritual practices that brings feelings of uncertainty temporarily under control.
Interrogating SEF through this lens provides an entry point to understand how the socio-moral context and embodied experiences flow together in this practice. Moore and Burgess suggested that risk rituals symbolise moral imperatives about who has the responsibility to act and protect. 33 Many women in our study indicated that they should take responsibility for their fertility to avoid any future blame about childlessness. Consistent with other qualitative research on SEF and in-vitro fertilisation more broadly,35–39 we found that the participants feared decision regret and were particularly vulnerable to the appeal of the moral imperative to do everything within their power. This broadly supports previous work on risk and SEF, work that has highlighted how women's discourses are often saturated with a neoliberal ideology that validates self-responsibilisation for reproduction as higher good.16,38
The third theme we identified in this study, the endless pursuit of peace of mind, indicates how the threat of an uncontrollable future loomed like an ever-present shadow and made it impossible to completely resolve the control-anxiety paradox. For some participants, the procedure restored confidence and self-worth and gave new meaning to their existence – what Inhorn et al. have described as ‘a tool of recovery’. 17 Others however were more sceptical about its transformative potential, pointing out the liminal and ambiguous space in which they were located: neither infertility nor pregnancy was confirmed or excluded. Their social position was perceived as fallen into the interstices of singlehood and motherhood, also characterised by scholars as ‘otherhood’. 40 Indeed, Kroløkke et al. have suggested how the concept of liminality could help to illustrate the moral tension that SEF produces because of its endless possibilities for transgressing natural boundaries without any clear, firm sign of success. 41 As Franklin already noted in Embodied Progress, the rite of assisted reproductive technology does not immediately provide passage. 35
This study, complementing the existing body of empirical research with a new understanding why some women pursue SEF, offers a unique springboard to inform the ethical debate around it. Some bioethicists only focus on these women as having prerogatives of choice and strong patterns of rationality in their motivation to freeze their eggs.4,5 Such a view is problematic, as feminist bioethicists have argued, because it decontextualises and removes the social reality of this practice. 42 Rather than as a means chosen (merely) rationally to obtain a clearly defined end, SEF could be seen as a symbolic act involving the negotiation of moral responsibilities to finally create a sense of reassurance in a wider social context of uncertainty and risk.
Limitations
There are some limitations to this study that we need to bear in mind when interpreting the results. Firstly, our study foregrounds the voices of highly educated women who were able to afford this technology. Future work should investigate how the use of SEF is conceptualised by women with various socio-demographic characteristics. For example, studying how ethnic minorities perceive egg freezing could expand this area of scholarship. Secondly, the topic of risk ritual was not the principal framework for the study during the construction of the interview guide. Although we observed the importance of this framework, a study beginning with this specific focus could explore the issue in greater depth. Thirdly, the sensitivity of this personal topic might have urged women to give socially desirable responses. To safeguard their own or health professionals’ credibility, they may have minimised concerns about the procedure while speaking to the (male) interviewer. We took this into account by using a hermeneutic of demystification during the analysis. Finally, because all interviews were conducted over the course of about 24 months, this study is limited in its ability to speak to how participants’ feelings and decisions might change over a longer period. Follow-up research with women who have frozen their eggs could open many avenues for future research.
Conclusion
The mainstream bioethics debate on SEF often focusses on individuals as rational agents and reduces the complexity of women's embodied feelings and considerations of their social contexts. This study, by giving insight into women's concerns and perceptions accompanying their SEF decisions, provides an important addition to previous depictions of SEF.
We identified three key themes that emerged from our qualitative analysis: feeling overwhelmed with uncertainty and a threatening future, bodily discomfort and distress during the medical process, and the endless pursuit of peace of mind. In discussing these findings, we have suggested that a risk ritual function may underpin its use, and this could be one factor making SEF so compelling. By providing a new understanding of SEF as a disciplined pattern of risk ritual, we hope to inspire future studies in bioethics seeking to better understand those experiences and ultimately to inform clinical practice.
Footnotes
Acknowledgements
The authors would like to thank all the women who participated in this research. Eveline Buyse, Lize Leunens, Isabelle Stuyver, and Lien Van Glabeke are acknowledged for their efforts in recruitment.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.