
Abstract
Diabetic ketoacidosis (DKA) is a life-threatening diabetes emergency associated with mortality and severe morbidities in individuals with diabetes. DKA mainly presents with significant hyperglycemia (>250 mg/dL); however, with the increasing use of sodium-glucose transporter 2 inhibitors, we are seeing an increase in euglycemic DKA (euDKA) in both type 1 diabetes and type 2 diabetes. Although severe DKA generally requires emergency department services or inpatient hospitalization, clinicians can play an important role in helping patients prevent DKA by providing comprehensive education to their patients regarding early identification of elevated ketone states and intervention for improvement in ketone production, thus potentially preventing the severity of DKA. Although ketone monitoring is recommended for all patients at risk for developing DKA or euDKA, current ketone monitoring methods have significant limitations. Abbott Diabetes Care (Alameda, CA) is developing a dual monitoring system that continuously measures interstitial glucose and β-hydroxybutyrate using a single sensor. This article discusses how continuous dual glucose-ketone monitoring can be integrated into primary care practice when it becomes available.
Introduction
Diabetic ketoacidosis (DKA) is a life-threatening diabetes emergency associated with mortality and severe morbidities in individuals with diabetes. 1 Most patients who are hospitalized for DKA have type 1 diabetes (T1D). 2 Although approximately one-third of adults hospitalized for DKA occur in individuals with poorly controlled or new-onset type 2 diabetes (T2D),3,4 the incidence of DKA in T2D continues to rise, particularly among those with poorly controlled glycemia and newly diagnosed patients.2,5
DKA mainly presents with significant hyperglycemia (>250 mg/dL), which prompts the body to metabolize fat as the energy source due to insulin deficiency, necessary for the transmission of glucose into the cell. 6 The byproducts of fat metabolism produce ketone bodies that build up in the blood, altering the body’s pH and overall homeostasis. 6 However, with the increasing use of sodium-glucose transporter-2 inhibitors (SGLT-2i), we are seeing an increase in euglycemic DKA (euDKA) in which glucose levels are only slightly elevated (<250 mg/dL), making detection of DKA difficult. 6 Although the increases in euDKA associated with SGLT-2i therapy mostly occur in individuals with T1D, we are also seeing increases in DKA associated with SGLT-2i therapy in T2D patients. 7
Because treatment of severe DKA requires initiation of rapid rehydration with intravenous (IV) fluids, insulin therapy, and frequent monitoring of the patient’s clinical and laboratory status, 8 treatment and resolution of severe DKA usually require emergency department services or inpatient hospitalization. However, clinicians can play an important role in helping patients prevent DKA by providing comprehensive education to their patients regarding early identification of elevated ketone states and intervention for improvement in ketone production, thus potentially preventing the severity of DKA. Continuous dual glucose-ketone monitoring would identify when risk is elevated, guide remedial steps patients should take to prevent its progression, and when they should seek emergency care.
Although ketone monitoring is recommended for all patients at risk for developing DKA and/or euDKA during times of acute illness, physical or emotional trauma, heart attack or stroke, and other conditions, 9 adherence to ketone testing remains suboptimal.10,11 In their audit of 205 adults with T1D, Larsson et al. reported that 31% did not have in‐date ketone testing strips at home, and only a minority were carrying these with them. 10 Similar findings were reported in a survey of 2995 individuals with T1D, which found that only 18% had a blood ketone meter at home, while 32% had no ketone testing supplies. 11 Although continuous glucose monitoring (CGM) has been shown to reduce hospital admissions for DKA,12–14 it does not directly measure ketone levels; thus, euDKA, in which the lower glucose threshold ketosis will stay hidden as the glucose level does not prompt the individual to check ketone levels.
However, innovations in continuous dual glucose-ketone monitoring (DGK) technology show promise in addressing many of the limitations of current methods. Abbott Diabetes Care (Alameda, CA) is developing a dual monitoring system that continuously measures both interstitial glucose and β-hydroxybutyrate (BHB) using a single sensor. Data are automatically transmitted to a smartphone app or clinician portal for review, enabling earlier detection of moderate to high BHB levels and facilitating timely interventions to reduce ketosis.
In this article, we discuss how DGK can be integrated into primary care practice when it becomes available to aid patients in preventing the development and progression of DKA.
Limitations of Current Ketone Monitoring Methods
The two most common methods for home ketone measurement are urine testing and blood ketone testing using a meter and strip, both of which have significant limitations. For example, urine ketone testing is a semi-quantitative measurement that only indicates trace, moderate, or large amounts of acetoacetate in the urine. Apart from the inconvenience of a urine dipstick test strip, this method does not directly measure BHB, the main metabolic product of fat breakdown and blood ketone elevation. This can lead to misinterpretation of ketone status. Moreover, this method is prone to user variability in interpreting color changes. 15 Although blood ketone monitoring with a meter and test strips provides direct and accurate measurements of BHB within their designed ranges, it is more costly than urine testing, and it requires fingerstick sampling.
Applications in Diabetes
Daily management
DGK is particularly relevant for patients with T1D, who are at high risk for DKA, and serves as a standard of care for all T1D patients, facilitating early detection of ketosis and preventing severe complications. It could also be valuable in T2D patients who are ketosis-prone, such as those with insulin deficiency or those treated with SGLT-2i inhibitors, which can increase the risk of euDKA. In short, DGK would enable clinicians to identify at-risk individuals, monitor BHB levels in real-time, and intervene early to avoid the acute and chronic complications of severe DKA. For example, patients who experience rapid ketone accumulation or baseline elevated ketones could be flagged for closer monitoring and personalized interventions.
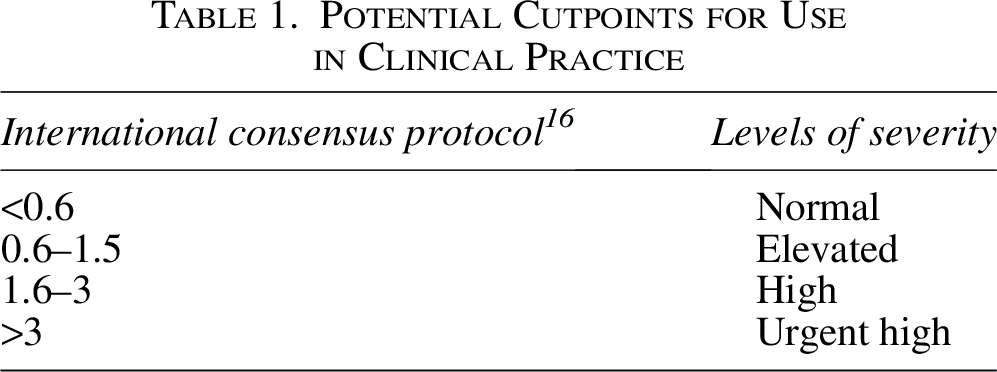
While real-time use of DGK can warn patients about impending ketonemia, retrospective analysis of DGK data could also provide useful information about patient variability in the development and progression of DKA (Table 1). For example, while some patients can progress to DKA within hours of insulin pump failure, others may remain stable for days. 3 DGK could assist in identifying these individual differences or phenotypes, which would provide a better understanding of metabolic risk factors and aid clinicians in offering more personalized counseling and education based on each patient’s physiological response to DKA progression. When viewed in combination with CGM data, these data will enhance the assessment of both glycemic and ketone levels. For example, clinicians could begin to correlate the time spent in glucose ranges with the time spent in ketone ranges. We assume that the Abbott DGK system will offer a retrospective component (similar to CGM), with the same automatic data upload capability as CGM for both patients and clinicians.
Potential Cutpoints for Use in Clinical Practice
Surgical and illness-related applications
Patients undergoing surgery or experiencing acute illness are at higher risk for ketosis due to stress-induced metabolic changes. 17 DGK could be used intermittently in these situations to monitor ketone levels and guide interventions, thereby reducing hospitalization rates and overall health care costs. DGK can also be used in patients with other conditions, such as chronic kidney disease and heart failure, where the risk of ketosis and ketoacidosis exists. 18
Pregnancy
Gestation is a high metabolic state, and those with diabetes who are pregnant have a significantly higher risk of developing DKA during pregnancy. Maternal mortality due to DKA is rare, but fetal mortality rates can reach up to 35% during a single DKA episode, despite advancements in perinatal and neonatal care. 19 Early detection of blood ketones (ketonemia), even without progression to DKA, is crucial for safeguarding fetal health.20,21 However, identifying and preventing DKA remain challenging for health care providers. DGK could be particularly beneficial in pregnancies complicated by diabetes, as insulin resistance and increased glucose demands heighten the risk of ketosis. Tracking ketones in pregnant women may help clinicians distinguish between harmless ketone levels and problematic ketosis, ultimately preventing complications and improving fetal outcomes.22,23
Applications Beyond Diabetes
DGK could also be helpful in nondiabetic populations. For example, lean individuals with prediabetes who exhibit mildly elevated fasting glucose levels due to glucagon dysregulation often mobilize glucose rapidly during exercise or stress. 24 DGK could provide insights into their individual metabolic patterns.
While non-DKA is a rare condition, it can be caused by excessive fasting and the use of ketogenic or other calorie-restrictive diets in which the lack of glucose forces the body into ketogenesis. 25 Unchecked, this could lead to ketonemia and eventually progress to ketosis.
Challenges to DGK Integration
One major challenge in implementing DGK into clinical practice is providing clinicians with standardized baseline metrics for specific ketone thresholds and other metrics that would prompt intervention in various populations, including pediatric patients, elderly patients, patients using automated insulin delivery technology, and patients compromised by acute and chronic conditions that increase DKA risk. It would also be helpful to provide evidence-based guidance for differentiating between nutritional ketosis from ketogenic diets and pathological ketosis from insulin deficiency. However, the variability observed in individual metabolic responses complicates the creation of universal guidelines. Nevertheless, without clear-cut points or individualized thresholds, clinician adoption of DGK will be slow, and patients may struggle to understand the significance of their readings, leading to confusion or skepticism about the value of this technology.
However, implementing DGK in clinical practice will also require tools and strategies to address the needs and concerns of clinicians and patients. As with CGM, clinicians will need to learn to use the new metrics for interpreting the combined DGK/CGM data, and they will require training in how DGK will integrate with other diabetes management technologies (e.g., automated insulin delivery), how DGK devices operate, and how to train their patients to use DGK in their daily self-management. However, even with this training, clinicians may be resistant to using the new technology due to skepticism about its efficacy and concerns about how the integration of DGK may interrupt office workflows.
Similarly, patients may resist using DGK due to fears of complexity, concerns about lifestyle changes and added burden, and cost concerns, especially if they do not perceive themselves to be at risk for DKA. Patients may also be slow to trust the technology’s accuracy and reliability. However, providing effective education, clear communication of benefits, and addressing individual needs can overcome these barriers.
Recommendations for DGK Integration
Although the final configuration of the DGK system that is currently under development has not been made public, we can provide recommendations for the type of training patients will need once the system becomes available.
Clinician training
Clinician training should include timely information about the prevalence and severity of outcomes of DKA in all patients with diabetes, and evidence from the clinical and observational studies currently underway that support the rationale for using DGK and how this technology can reduce DKA. We anticipate publication of the results from many of these studies later this year, which could be used to determine specific metrics and thresholds for interpreting DGK data. Once these guidelines are established, clinicians will require training in how these metrics can be used in combination with CGM data for interpretation and intervention strategies. Guidance on how to counsel patients about DGK should also be provided. This information should include communicating the importance of preventing DKA, the causes and severity of DKA, the rationale for DGK, and taking remedial action based on the DGK data, along with training in device setup and operation. Continuing medical education (CME) programs, podcasts, and national/international medical meetings are potential vehicles for delivering clinician training.
Discussion
At this time, DGK is in uncharted territory that could revolutionize metabolic research. Assuming that it is effective in reducing DKA incidence, we believe that DGK has the potential to become the standard of care for all T1D patients, high-risk T2D patients, and pregnant patients within the next 2 years. Leveraging data that demonstrate improved outcomes and the ability to integrate technology seamlessly into existing care models can help build confidence and drive adoption. As the technology evolves, it may become a standard tool not only for diabetes care but also for broader metabolic health management. Moreover, the potential cost savings associated with DGK by preventing hospitalizations could significantly reduce overall health care expenditures. Beyond its immediate applications, DGK could open new avenues for understanding metabolic disorders, identifying risk factors, and developing targeted therapies. However, further research, clinician education, and patient engagement are needed to fully realize its benefits.
Authors’ Contributions
E.M., K.M., and R.M.B.: Conceptualization, original draft; review and editing.
Footnotes
Acknowledgments
The authors wish to thank Christopher G. Parkin, MS, CGParkin Communications, Inc., for his editorial assistance.
Funding Information
Abbot Diabetes Care funded the development of this article.
Disclosures Statement
E.M. has received consulting fees from Abbott, Astra Zeneca, Novo Nordisk Boehringer Ingelheim, Eli Lilly, Merck, Sanofi US, and has acted as a speaker for Abbott, Boehringer Ingelheim, Eli Lilly, and Novo Nordisk. K.M. has served as a consultant to Semler and Novo Nordisk. R.M.B. has received research support, consulted, or has been on a scientific advisory board for Abbott Diabetes Care, Ascensia, CeQur Corporation, DexCom, Hygieia, Insulet, Johnson & Johnson, Lilly, Medtronic, Novo Nordisk, Onduo, Roche, Sanofi, United Healthcare and Zealand.