
Abstract
Introduction:
Continuous ketone monitoring (CKM) could optimize diabetic ketoacidosis (DKA) treatment by monitoring beta-hydroxybutyrate (BOHB) continuously and minimally invasively. However, data on the agreement between interstitial and venous BOHB during DKA is lacking. Our objectives were to assess the feasibility of CKM during DKA and the agreement between interstitial and venous BOHB.
Methods:
This was a prospective multicenter method-comparison study conducted at two U.S. emergency departments. Adults (>18 years) in DKA were included. BOHB was measured via SiBio CKM and compared with simultaneously collected venous BOHB every 2 h during DKA treatment. Following DKA resolution, study staff removed CKM and assessed for complications. The primary outcome was level of agreement via Bland–Altman analysis between simultaneously collected CKM and venous BOHB values. Additional outcomes included correlation (r) between concurrent CKM and venous BOHB values, first detection of DKA resolution, and feasibility (uncomplicated application and removal of CKM).
Results:
Thirty-four patients were enrolled, with a mean age of 40.8 years, 56% male, 50% Black, 79% type I diabetes, and mean presenting BOHB 7.0 mmol/L (range 2.5–13.5). We analyzed 164 paired CKM and venous BOHB values (mean [standard deviation (SD)] paired values per patient: 4.8 [3.8], range 1–16). Bland–Altman analysis found the average difference between CKM and venous BOHB was −0.38 mmol/L (95% confidence interval [CI] −1.63, 0.88). CKM values were strongly correlated with venous BOHB (r = 0.96, p < 0.001). The CKM value was lower than venous for 79% of paired values. DKA resolution was detected 55 min earlier (mean, 95% CI 26–84, p = 0.001) via CKM than standard care. No device-related complications occurred, and CKM application and removal were well tolerated by all patients.
Conclusion:
CKM during DKA treatment was feasible, provided clinically accurate BOHB readings, and detected DKA resolution earlier than standard care. CKM-guided DKA treatment is a promising strategy with the potential to improve the quality and value of DKA care.
Introduction
Diabetic ketoacidosis (DKA) is a common, severe complication of diabetes mellitus. Management of DKA requires frequent monitoring of laboratory values that guide titrations of insulin, dextrose, and electrolytes. A recent international consensus report recommends trending ketone values (beta-hydroxybutyrate [BOHB]) every 4 h during DKA treatment, and defines the resolution of DKA as BOHB < 0.6 mmol/L. 1 The ability to collect frequent BOHB measurements is essential for optimizing patient outcomes and safety. However, frequent phlebotomy is uncomfortable for patients, resource-intensive, and often necessitates intensive care unit (ICU) admission with substantial associated cost. 2
Continuous ketone monitoring (CKM) is an innovation that might aid in providing frequent ketone measurements during DKA treatment.3–5 Like widely used continuous glucose monitoring (CGM) devices, 6 CKM utilizes a temporarily implanted sensor in the skin of the abdomen or arm, but measures ketone (BOHB) values continuously and minimally invasively from interstitial fluid, providing ketone readings to a receiver without the need for repeated fingersticks or phlebotomy. Use of CKM could optimize DKA treatment by improving patient comfort, replacing the need for frequent phlebotomy, providing real-time monitoring of response to DKA treatment, and promoting earlier detection of DKA resolution.
However, a major barrier is the lack of published data on the agreement between interstitial fluid ketone concentrations measured using CKM and venous BOHB concentrations obtained via standard clinical laboratory assays during DKA. The Continuous Ketone Monitoring Consensus Report highlighted the unmet need to assess the analytical accuracy of CKM in the highest ketone concentration range (DKA), 7 and a 2024 consensus report from five major international societies concluded “areas of research interest include… continuous interstitial ketone monitoring in the hospital.” 1 While potential uses of CKM in the inpatient setting have been described, 3 to our knowledge, no prior peer-reviewed studies have demonstrated the feasibility of CKM during DKA treatment (uncomplicated application and removal of CKM during DKA treatment). The objectives of this study were to determine the feasibility of CKM during DKA treatment and to assess agreement between interstitial fluid (via CKM) and venous BOHB concentrations, to inform future clinical use of this emerging diabetes technology.
Materials and Methods
Study design
This was a prospective multicenter method-comparison8,9 pilot study, designed to assess the feasibility of CKM during DKA treatment and to evaluate the agreement between interstitial and venous BOHB. Feasibility was determined by uncomplicated application and removal of CKM during DKA treatment. Agreement was determined by comparing interstitial fluid BOHB levels obtained from SiBio CKM (index test) to simultaneously collected venous BOHB values (reference standard) that were obtained at regular intervals (every 2 h) during DKA treatment. Treating clinicians were blinded to values from the CKM devices, and values were not used for any clinical decision-making. This study was approved by institutional review boards at the University of Michigan (HUM00249706) and Washington University (202409067), and is presented in accordance with the Standards for Reporting Diagnostic accuracy studies (STARD) statement. 10
Setting and population
This study was conducted at two sites in the United States: both academic emergency departments (EDs) with 75,000 and 87,000 adult ED visits per year, respectively. At the first site (University of Michigan) most adult ED patients with DKA are managed in an ED-ICU until resolution, 11 and at the second site (Washington University) patients are either treated with subcutaneous insulin and admitted to the medical floor, treated with intravenous insulin and admitted to the ICU, or treated in the ED until DKA resolution and admitted to the medical floor, depending on DKA severity and ICU bed availability. 12 Patients were enrolled from August 2024 to August 2025, and data analysis was completed in 2025. Adult ED patients were screened by study personnel for lab values diagnostic of DKA, and at one site were approached primarily between 8:30 am and 5 pm, and at the other site, enrollment also included evenings and nights. Sample size (n = 34) was determined based on guidelines for pilot and feasibility studies, 13 with a focus on achieving a reasonable balance between maximizing precision of estimates of bias and minimizing resources required for adequate assessment of feasibility. 14
Eligible patients were adults (>18 years) in the ED with DKA, meeting either of two definitions provided by the American Diabetes Association in 2009 and 2024.1,15 The first includes (i) glucose ≥250 mg/dL, (ii) pH ≤ 7.30, (iii) serum bicarbonate ≤18 mEq/L, (iv) anion gap ≥12, and (v) presence of serum and/or urine ketones; and the second includes (i) glucose ≥ 200 mg/dL or prior history of diabetes, (ii) venous BOHB ≥ 3.0 mmol/L or urine ketone strip ≥2+, and (iii) venous pH < 7.3 and/or bicarbonate <18 mEq/L. These were both used, as the updated definition was published during this study period and subsequently adapted. Exclusion criteria were inability to provide informed consent (e.g., altered mental status) or currently incarcerated.
Measurements
Following written informed consent, the CKM (SiBio; China) was applied according to manufacturer’s recommendations (Figure 1). It consists of a sticker with a microneedle (approximate sensor dimensions: 3 × 2 × 0.2 cm3) attached to the skin of the arm, similar to the functionality and application of a CGM, and application is typically painless. Following device application, blood draws occurred at regular intervals (approximately every 2 h) to measure venous BOHB until the resolution of DKA. The SiBio CKM provides a reading of “HIGH” for BOHB above 8.0 mmol/L, and for purposes of data analysis, these paired measurements with CKM reading “HIGH” were excluded. To allow statistical analysis, we excluded 12 paired readings with CKM reading HIGH, of which 10 of the reference (lab-based) BOHB values were ≥8 mmol/L, and two were < 8 mmol/L (7.2 and 7.4 mmol/L). Serum BOHB values were measured via the StanBio assay on Siemens Atellica CH analyzers at one site and Abbott Precision Xceed Pro at the other site. Following resolution of DKA (defined as venous BOHB < 0.6 mmol/L and pH ≥ 7.3 or bicarbonate ≥ 18 mmol/L), the CKM was removed prior to the participant leaving the hospital, and study staff assessed for CKM-related complications (e.g., infection, skin reaction).

Continuous ketone monitor applied to the skin on the back of the upper arm.
Outcome measures
The primary outcome was the level of agreement assessed via Bland–Altman analysis between simultaneously collected CKM and venous BOHB values during DKA treatment. The secondary outcome was correlation via Pearson’s r between simultaneously collected CKM and venous BOHB. Exploratory analyses tested correlations via Pearson’s r between CKM BOHB with simultaneous serum pH, bicarbonate, and anion gap values. These (serum pH, bicarbonate, and anion gap) were selected as they are routinely monitored during DKA treatment as surrogates for ketone levels, particularly in lower-resource settings where ketone measurement is unavailable. 1 Additionally, the time of first detection of DKA resolution was compared between CKM (interstitial fluid BOHB measured every 5 min) and standard of care (serum BOHB measured every 4 h). Feasibility was determined by uncomplicated application and removal of CKM during DKA treatment.
Statistical analysis
Statistical analyses were conducted using R statistical software (v4.2.2, 2022), and Bland–Altman analysis 16 was conducted using the ggplot2 R package. 17 The 95% limits of agreement, defined as those values that “define the range within which most differences between measurements by the two methods will lie,” were quantified. 16
Results
Thirty-four patients from two sites were enrolled. Demographics and presenting laboratory values of participants are summarized in Table 1 and include a mean age of 40.8 years, 56% male, 50% Black, 79% type I diabetes, and a mean presenting pH 7.20, bicarbonate 14.7 mmol/L, anion gap 24.8, glucose 557 mg/dL. The mean presenting serum BOHB was 7.0 mmol/L (SD 2.6, range 2.5–13.5). Total of 164 paired simultaneous CKM and venous BOHB values were analyzed, and the mean [SD] paired measurements per patient was 4.8 [3.8], range 1–16. Bland–Altman analysis (Figure 2) observed the average difference between CKM and serum BOHB values was −0.38 mmol/L (95% confidence interval [CI] −1.63, 0.88). CKM values were strongly positively correlated with serum BOHB (r = 0.96, p < 0.001) (Figure 3). The mean CKM value (1.99) was 0.38 lower than the mean venous BOHB value (2.37), and CKM values were lower than corresponding venous values for 79% of paired observations. The variability of CKM and venous BOHB measures was similar (SD = 2.2 and 2.3, respectively).
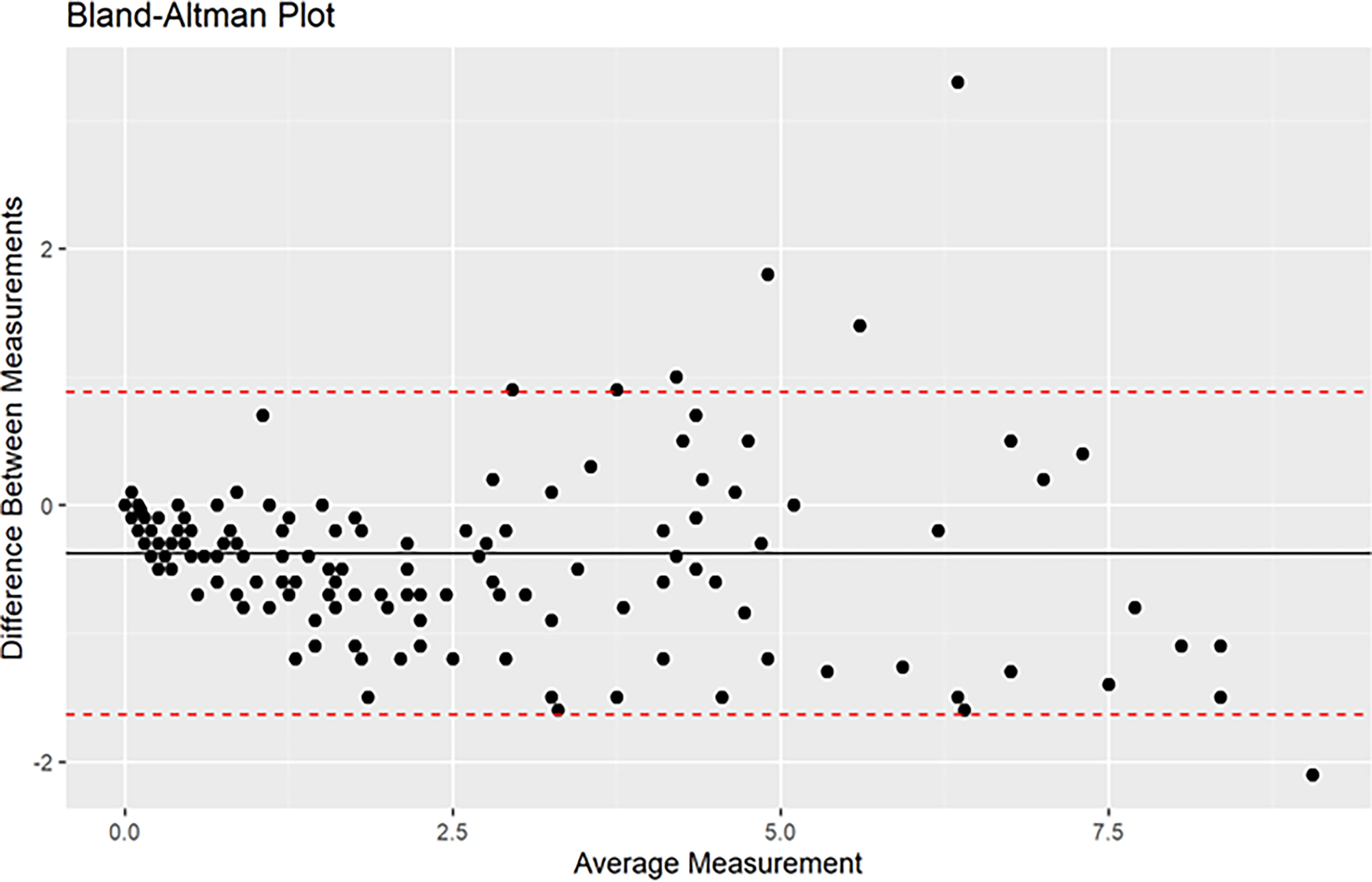
Bland–Altman plot comparing interstitial fluid BOHB levels obtained from SiBio CKM (index test) to simultaneously collected venous BOHB values (reference standard). The black line represents the average difference in measurements between the two methods, while the two red dashed lines represent the 95% confidence interval limits for the average difference. BOHB, beta-hydroxybutyrate; CKM, continuous ketone monitoring.
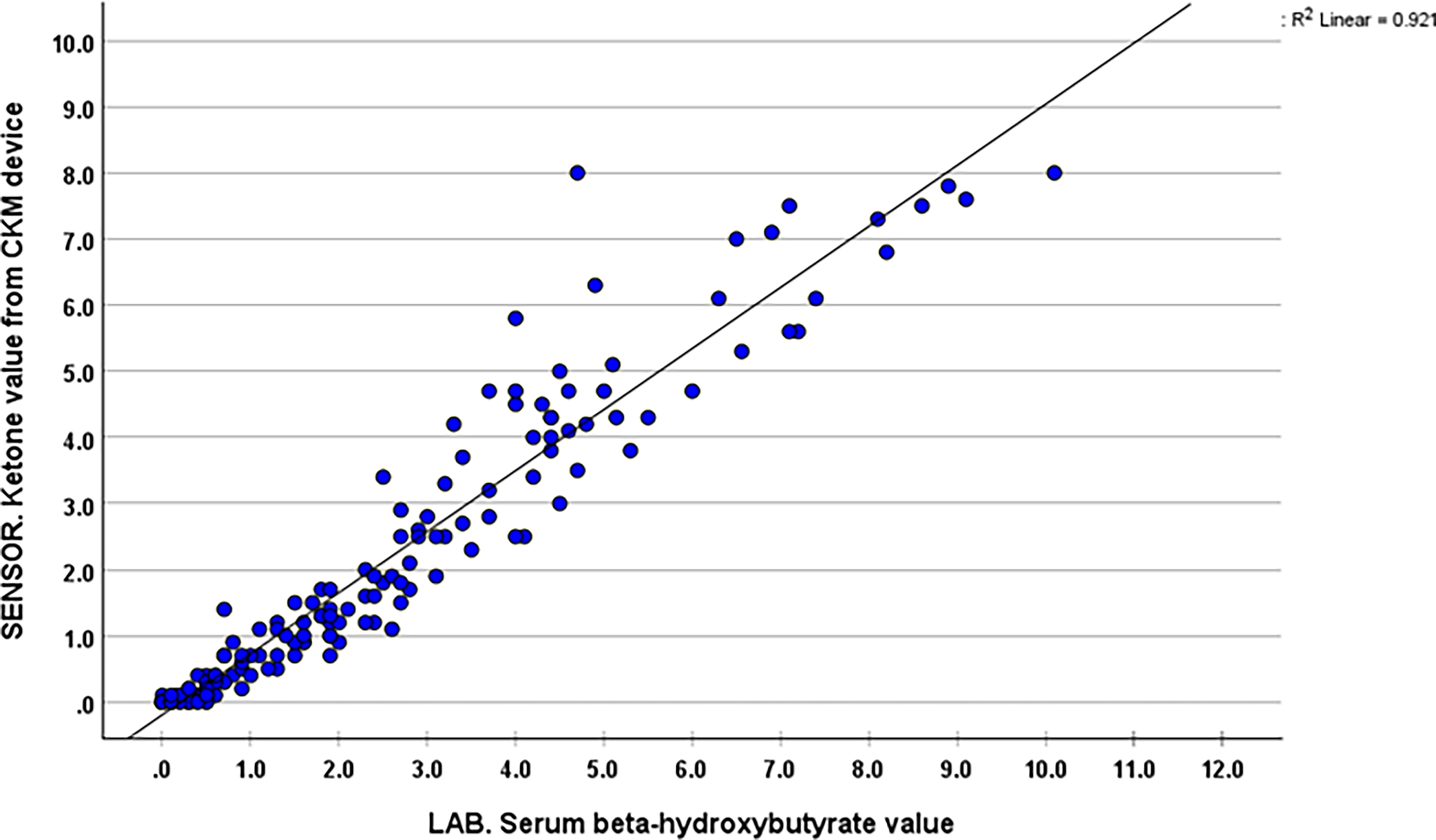
Correlation between venous and continuous ketone monitor beta-hydroxybutyrate values.
Patient Demographics and Presenting Laboratory Valuesa
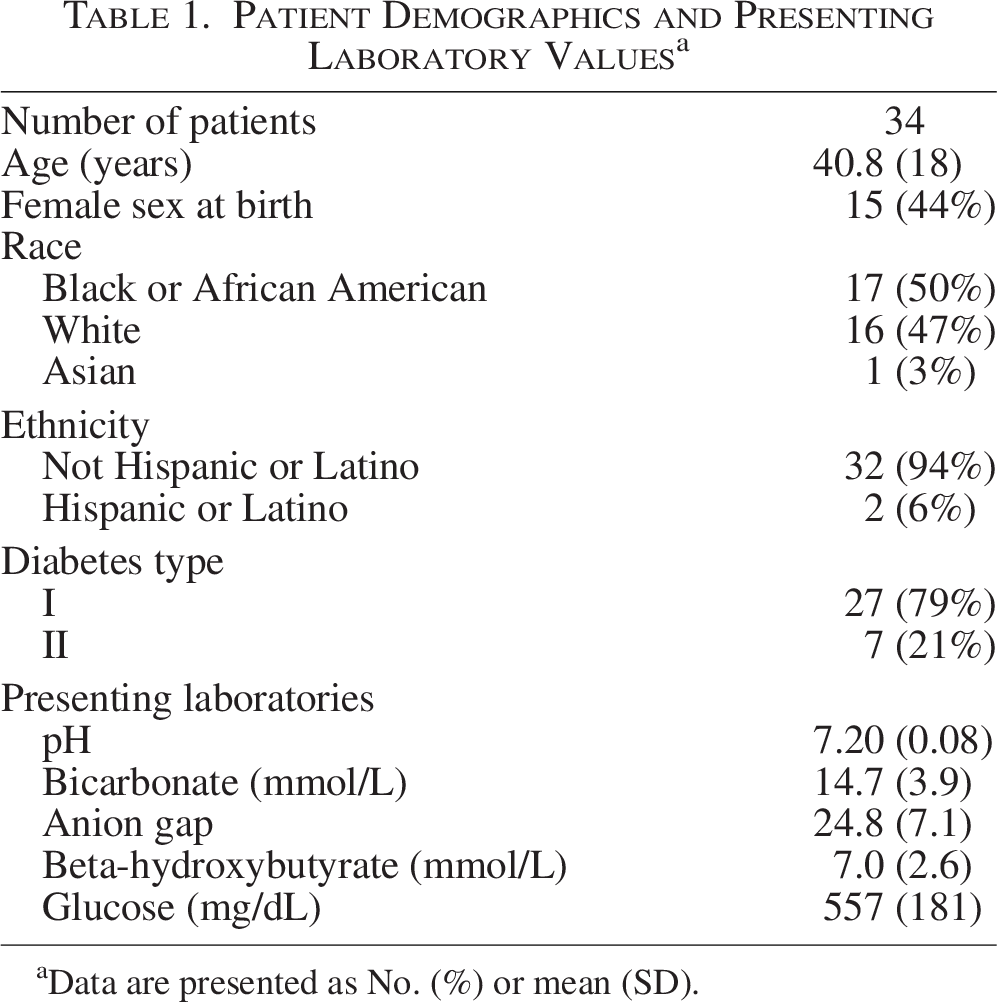
Data are presented as No. (%) or mean (SD).
Exploratory analyses showed that CKM values were positively correlated with anion gap (n = 63 paired measurements, r = 0.88, p < 0.001) and negatively correlated with serum pH (n = 79 paired measurements, r = −0.60, p < 0.001) and bicarbonate levels (n = 63 paired measurements, r = −0.57, p < 0.001). DKA resolution (first incidence of BOHB < 0.6 mmol/L and pH ≥ 7.3 or bicarbonate ≥ 18 mmol/L) was detected 55.4 min earlier (mean, 95% CI 26–84, p = 0.001) via CKM than standard of care (serum BOHB measurements every 4 h). No device-related complications occurred, and CKM application and removal were well tolerated by all patients.
Discussion
Use of CKM could optimize DKA treatment by improving patient comfort (replacement of frequent venipunctures with one-time painless monitor application), providing real-time monitoring of response to DKA treatment and earlier detection of DKA resolution, although published data to inform adoption of this emerging diabetes technology is lacking. In this prospective multicenter method-comparison pilot study conducted at two hospitals in the United States with 164 paired CKM and venous BOHB values from 34 patients, CKM during DKA treatment was feasible, provided clinically accurate readings of BOHB, and detected DKA resolution earlier than the standard of care.
A major strength of this study is the novelty of CKM during DKA. To our knowledge, no prior peer-reviewed studies have reported the agreement between interstitial fluid and venous BOHB concentrations during DKA or the feasibility of CKM in the ED or hospital. Previously, a 2024 international consensus report identified a research priority of exploring CKM in the hospital, 1 the Continuous Ketone Monitoring Consensus Report called for assessment of CKM analytical accuracy in the highest ketone concentration range (DKA), 7 and theoretical inpatient uses of CKM, including management of DKA and recognition of DKA resolution, have been described.3,5 While these publications highlight the growing interest in CKM for in-hospital use, including management of DKA, to our knowledge ours is the first study to demonstrate the feasibility of use in the ED or hospital and quantify agreement between interstitial and venous BOHB concentrations during DKA, and provides preliminary data to address questions of major clinical importance. If approved by the United States Food and Drug Administration for inpatient use, these findings can begin to inform the adoption of CKM in the inpatient setting, including during the treatment of DKA.
A primary intended role for CKM is to reduce ED visits or hospitalizations for DKA, 7 and a case report highlighted the potential for CKM to act as an early warning system to facilitate timely intervention for ketonemia and reduce the risk of DKA. 18 While early detection to promote intervention and prevent DKA is of utmost importance, our study helps define an additional avenue for CKM to improve the care of patients with diabetes: CKM-guided DKA treatment [Fig 4]. Management of DKA requires frequent venipunctures (typically every 2–4 h), and often ICU admission is required to facilitate the frequency of these (e.g., need for an ICU nurse with 1:1 or 1:2 patient ratio). ICU admission is associated with high costs, 2 clinical staff workload, and patient discomfort, though many cases of DKA have been considered “inappropriate” uses of ICU resources due to low mortality rate (<1%) and short ICU length of stay. 19 Patients with DKA compete with other high-acuity conditions for ICU access, which results in ED boarding and crowding with increased mortality. 20 As ICU capacity is under increasing strain,19,20 and national ICU admissions for DKA have increased annually by 17.4% from 2012 to 2022, 21 new strategies to safely avoid ICU admissions for adults with DKA are critically needed. Use of CKM (and CGM 6 ) could potentially prevent the need for ICU admission for DKA, especially in cases in which the primary indication for ICU admission is the frequency of lab draws needed. CKM-guided DKA treatment is a promising strategy to improve the value and quality of DKA care, and future interventional trials can assess CKM-guided DKA treatment’s impact on clinical outcomes, patient experience, clinician comfort and workload, and cost-effectiveness.
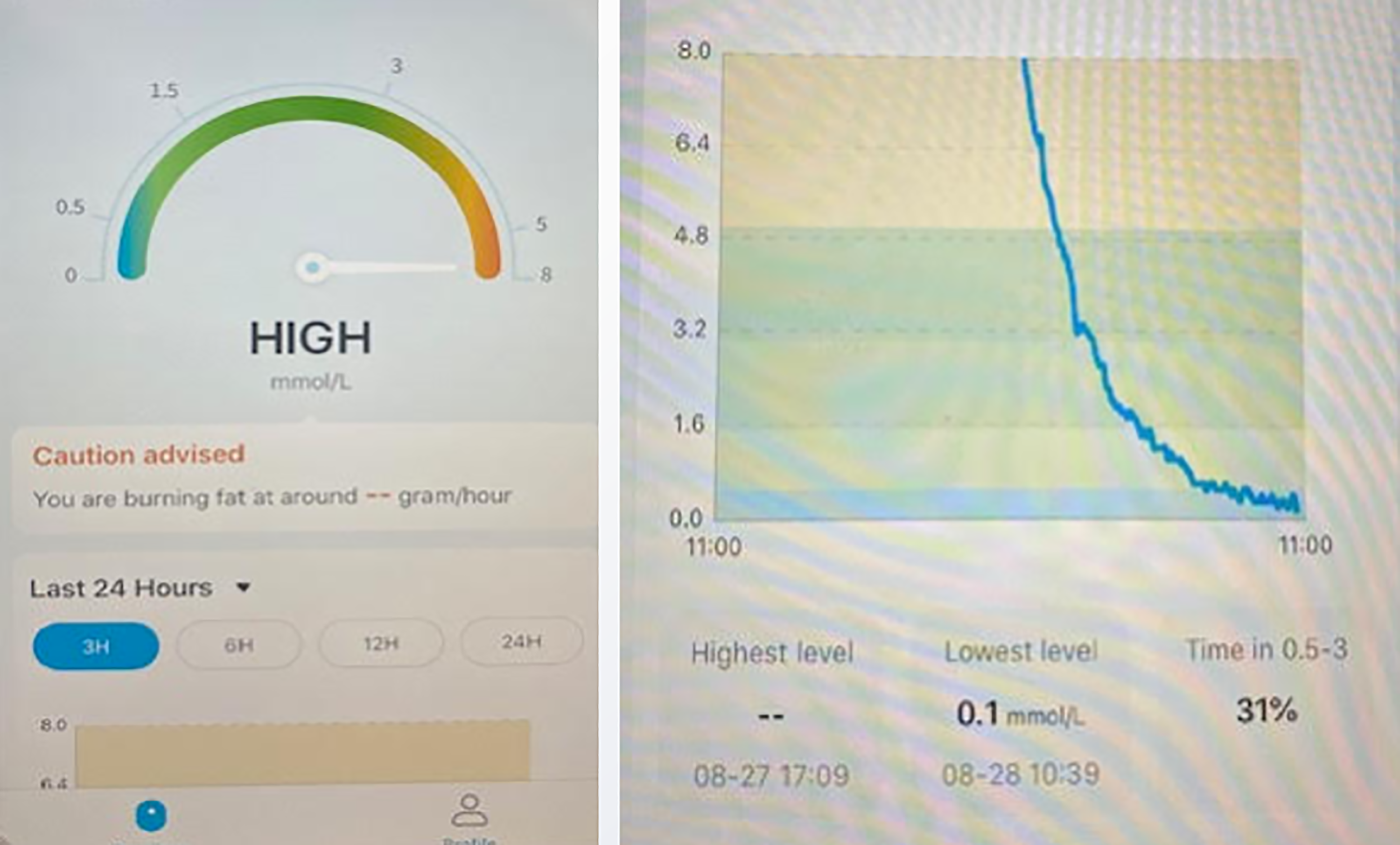
Continuous ketone monitor data from a study participant, demonstrating high beta-hydroxybutyrate concentration with subsequent normalization during treatment of diabetic ketoacidosis.
Limitations of this study include the modest/pilot-scale sample size (34 patients with 164 paired measurements) and the convenience sample of patients (rather than consecutive patients with DKA) based on study coordinator availability. While there is potential for unaccounted for patient-specific factors affecting observed agreement/bias, this risk is lower given the diverse patient population enrolled in this study: two sites from different areas of the country, with roughly half of patients being female and half being Black (Table 1). Additionally, we conducted a sensitivity analysis to assess whether the site or assay impacted the observed agreement/bias of CKM values. In the full sample (164 paired values from 34 patients), the average difference between CKM ketone measures and serum BOHB values was −0.38 (95% CI −1.63, 0.88). At Site 1 (N = 130 observations from N = 20 patients), the average difference between CKM ketone measures and serum BOHB values was −0.45 (95% CI −1.52, 0.61). At Site 2 (N = 34 observations from N = 14 patients), the average difference between CKM ketone measures and serum BOHB values was −0.07 (95% CI −1.77, 1.62). This suggests the site or specific assay used (StanBio assay on Siemens Atellica CH analyzers at Site 1 and Abbott Precision Xceed Pro at Site 2) did not impact the level of agreement between CKM and BOHB values. We did not compare CKM BOHB values to capillary BOHB values in favor of venous BOHB. While quantitative capillary ketone testing is desirable given its convenience and rapidity, 22 point-of-care blood ketone measurement may have analytical limitations compared with laboratory measurement, 23 and concern exists about the accuracy of point-of-care instruments for measuring BOHB levels ≥5 mmol/L. 1 Thus, for our study population of patients with DKA with initial BOHB up to 13.5 mmol/L, we considered venous (rather than capillary) BOHB to serve as a better reference test for assessment of agreement with CKM values. As CKM values tended to be slightly lower than simultaneous venous BOHB values, earlier detection of DKA resolution using CKM could be partially due to this bias. A potential for bias exists as CKM sensor wear time and data collection duration varied between patients, with a range of 1–16 paired data points per patient.
Conclusions
In conclusion, CKM during DKA treatment was feasible, provided clinically accurate readings of BOHB, and detected DKA resolution earlier than the standard of care. CKM-guided DKA treatment is a promising strategy to improve the value and quality of DKA care and could contribute to reduced need for ICU admission for DKA. Future trials can assess CKM’s impact on clinical outcomes, patient experience, and cost-effectiveness in DKA treatment.
Authors’ Contributions
N.L.H., F.K.K., and Y.K.L.: Conceptualization, Funding Acquisition, Investigation, Methodology, Project Administration, Writing-Original Draft, and Writing-Review & Editing. R.M.S., S.L.M., E.H., and R.T.G.: Data Curation, Project Administration, Writing-Review & Editing. J.A.C.: Formal Analysis, Writing-Review & Editing.
Consent for Publication
Figure 1 is an image of one of the study authors, NLH, used as an example. He provides consent for the publication of this image.
Data Availability
Upon reasonable request, subject to appropriate ethical and legal consideration, the authors will share data on a case-by-case basis.
Footnotes
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
This work was funded by the Caswell Diabetes Institute Clinical and Translational Research Scholars Program, and a cost share by the Department of Emergency Medicine at the University of Michigan. Additionally, grant support via UM1TR004404 supported REDCap, a secure web platform for building and managing online databases and surveys utilized in this study.