
Abstract
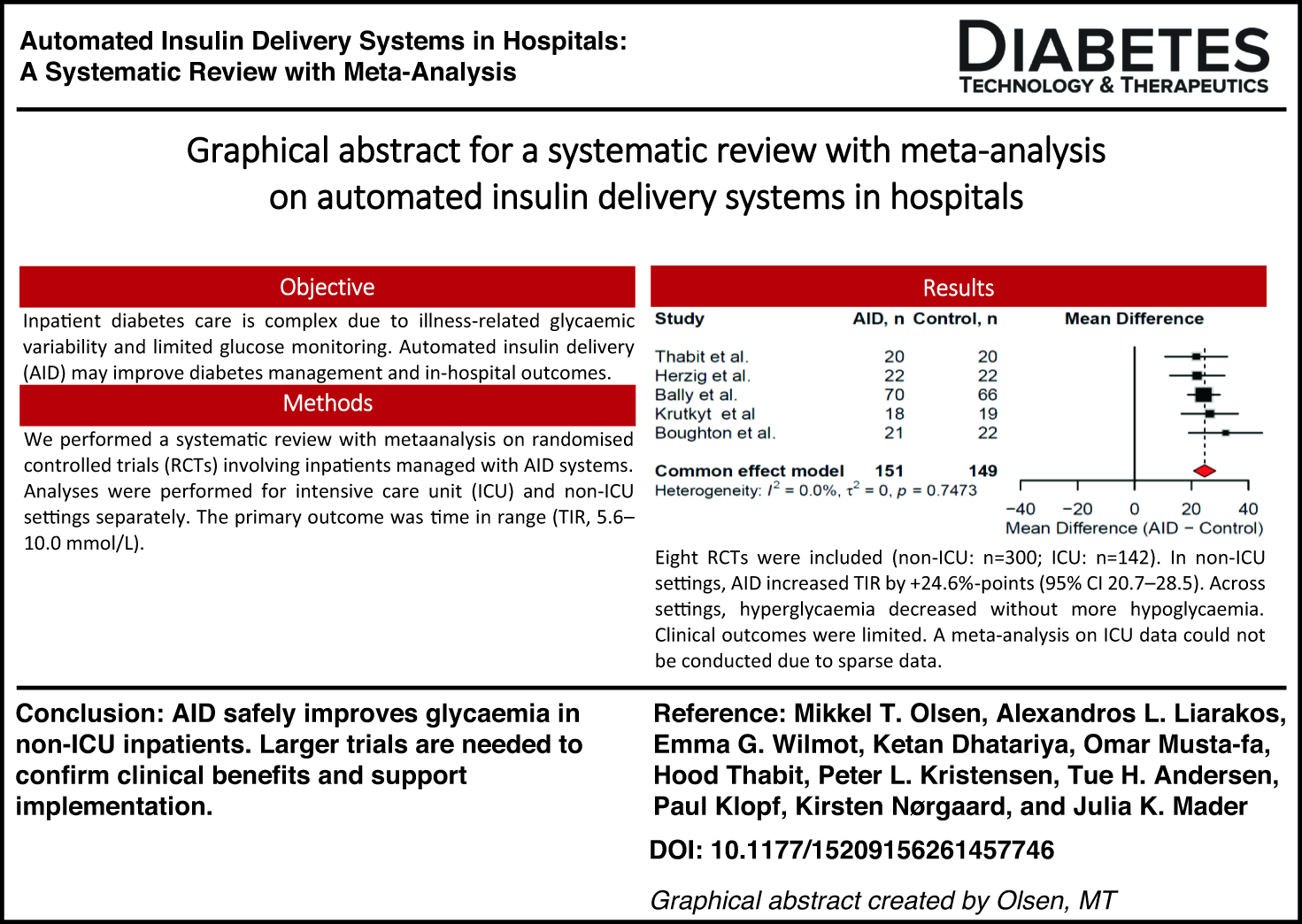
Inpatient diabetes management is challenging due to acute illness, variable insulin requirements, and reliance on intermittent point-of-care glucose testing. Both hyperglycemia and hypoglycemia are associated with increased costs, length of stay, morbidity, and mortality. However, efforts to achieve tighter glycemic targets are often limited by the risk of iatrogenic hypoglycemia. Notably, hypoglycemia (glucose <3.9 mmol/L, <70 mg/dL) occurs in approximately 10% of patients in intensive care unit (ICU) settings and 3.5% of non-ICU patients and is strongly linked to mortality. Automated insulin delivery (AID) systems may improve inpatient glycemic targets while minimizing the risk of hypoglycemia. This systematic review aimed to evaluate the effects of AID systems in hospital settings. A systematic literature search was conducted on March 27, 2026, in MEDLINE, Embase, and CENTRAL, without restrictions on publication date. Randomized controlled trials (RCTs) involving inpatients managed with AID systems were included if they reported glycemic and/or clinical outcomes. Analyses were performed for ICU and non-ICU settings separately. The primary outcome was time in range (TIR) 5.6–10.0 mmol/L (100–180 mg/dL). The reporting follows the PRISMA 2020 guidelines, and the protocol was registered with PROSPERO (CRD420261308501). A total of 4858 references were screened. Five RCTs from the non-ICU setting (N = 300 participants [>80% with type 2 diabetes]) and three RCTs from the ICU setting (N = 142 [with and without preexisting diabetes]) were identified. Meta-analysis of RCTs in the non-ICU setting showed that AID increased TIR by 24.6 percentage points (95% confidence interval 20.7–28.5). A meta-analysis on ICU data could not be conducted. Across all settings, AID was associated with reduced hyperglycemia without an increase in hypoglycemia. Clinical outcomes were sparsely reported. AID systems can be safely and effectively used in non-ICU hospital settings to improve glycemic outcomes. Larger, multicenter trials are needed to confirm clinical benefits and address implementation challenges.
Introduction
Diabetes affects up to 20% of hospitalized patients. 1 Inpatient glucose management is particularly challenging due to acute illness, the use of medications that interfere with insulin action, infections, surgical stress, altered nutritional intake, reduced physical activity, and frequent changes in insulin sensitivity. These factors contribute to glycemic variability and increase the risk of both hyperglycemia and hypoglycemia, each of which has been independently linked to adverse clinical outcomes, including prolonged hospital stays, higher complication rates, and increased mortality.2–4
Conventional inpatient diabetes management relies on intermittent point-of-care (POC) capillary glucose testing combined with subcutaneous or intravenous insulin regimens manually titrated by health care staff. Although widely implemented, this approach has several limitations. Intermittent glucose measurements fail to capture rapid glycemic excursions, nocturnal hypoglycemia, and postprandial hyperglycemia.5,6 Moreover, POC-based workflows and insulin administration by multiple daily injections are labor-intensive, place a substantial burden on nursing staff, and are associated with variable adherence to recommended guidelines.7–10
The introduction of automated insulin delivery (AID) systems has transformed outpatient diabetes care in people with type 1 diabetes and has generated increasing interest in their potential application in hospital settings. AID systems—also referred to as closed-loop or artificial pancreas systems—integrate real-time continuous glucose monitoring (CGM) data with algorithm-driven pump-based insulin delivery, allowing dynamic automatic adjustment of insulin dosing in response to changing glucose concentrations.11,12 Inpatient CGM is a critical enabler of AID systems, and its performance and regulatory acceptance directly influence the acceptability of AID use in hospital care. Despite increasing evidence over the past years supporting the accuracy and clinical utility of CGM in non–critically ill hospitalized populations, variability in institutional policies continues to limit both CGM-driven insulin delivery and AID implementation.13–16 Finally, restrictions on continuing personal CGM and AID devices during hospitalization may also create unnecessary disruption for patients who are otherwise well-established on these technologies in daily life, highlighting an important area for future policy and guideline development. 17
This systematic review aims to synthesize the available evidence on glycemic and clinical outcomes associated with the use of AID systems in hospital settings.
Materials and Methods
This systematic review is registered with PROSPERO (CRD420261308501), and the reporting follows the PRISMA 2020 guidelines. 18
Eligibility criteria
Inclusion criteria
Hospitalized adults (≥18 years) with diabetes (all types) and/or hyperglycemia; use of AID systems, either fully closed loop (“artificial pancreas”) or hybrid closed loop (i.e., requiring meal announcement); studies reporting glycemic and/or clinical outcomes during hospitalization; randomized controlled trials (RCTs); peer-reviewed publications; articles in English, Danish, Swedish, Norwegian, German, or Greek language or available translations.
Exclusion criteria
Device-only comparisons without standard-of-care control; trials in which patients were hospitalized solely for device safety testing or monitoring, rather than a real-life scenario for diabetes management during an acute illness causing hospitalization.
Search strategy
We conducted a systematic literature search on March 12, 2025, without restrictions on publication date or language. The search was updated on March 27, 2026, prior to article submission to ensure inclusion of the most recent evidence. We searched the databases MEDLINE, Embase, and the Cochrane Central Register of Controlled Trials (CENTRAL). An information specialist (T.H.A.) assisted the reviewers in developing the search strategy and defining the search strings (Supplementary Data), using both Medical Subject Heading terms and free-text words.
Important search words included “Automated insulin delivery system,” “insulin pump,” “inpatient,” and “hospitalization.” The search string was developed in MEDLINE and subsequently translated to the other databases and was evaluated by testing if 10 key articles were retrieved. After the screening process, references of included studies were screened for eligibility. Titles and abstracts from the search were imported to EPPI Reviewer 6 (EPPI Center, UCL Social Research Institute, University College London), 19 and duplicates were removed.
Selection process and data extraction
The titles, abstracts, and full-text articles were screened independently for eligibility by reviewer 1 (M.T.O.) and reviewer 2 (A.L.L.) in EPPI. We extracted prespecified data points in relation to trial design, setting, population, intervention, and outcomes (Tables 1 and 2). Full-text articles were examined by reviewer 1 (M.T.O.) and reviewer 2 (A.L.L.). Disagreements were resolved by discussion. If an agreement could not be met, the decision of whether or not to include an article was resolved by reviewer 3 (J.K.M.). The corresponding author of the included articles was contacted for additional information in case of missing information.
Study Design and Baseline Patient Characteristics of Trials Using Automated Insulin Delivery Systems in Hospital Settings
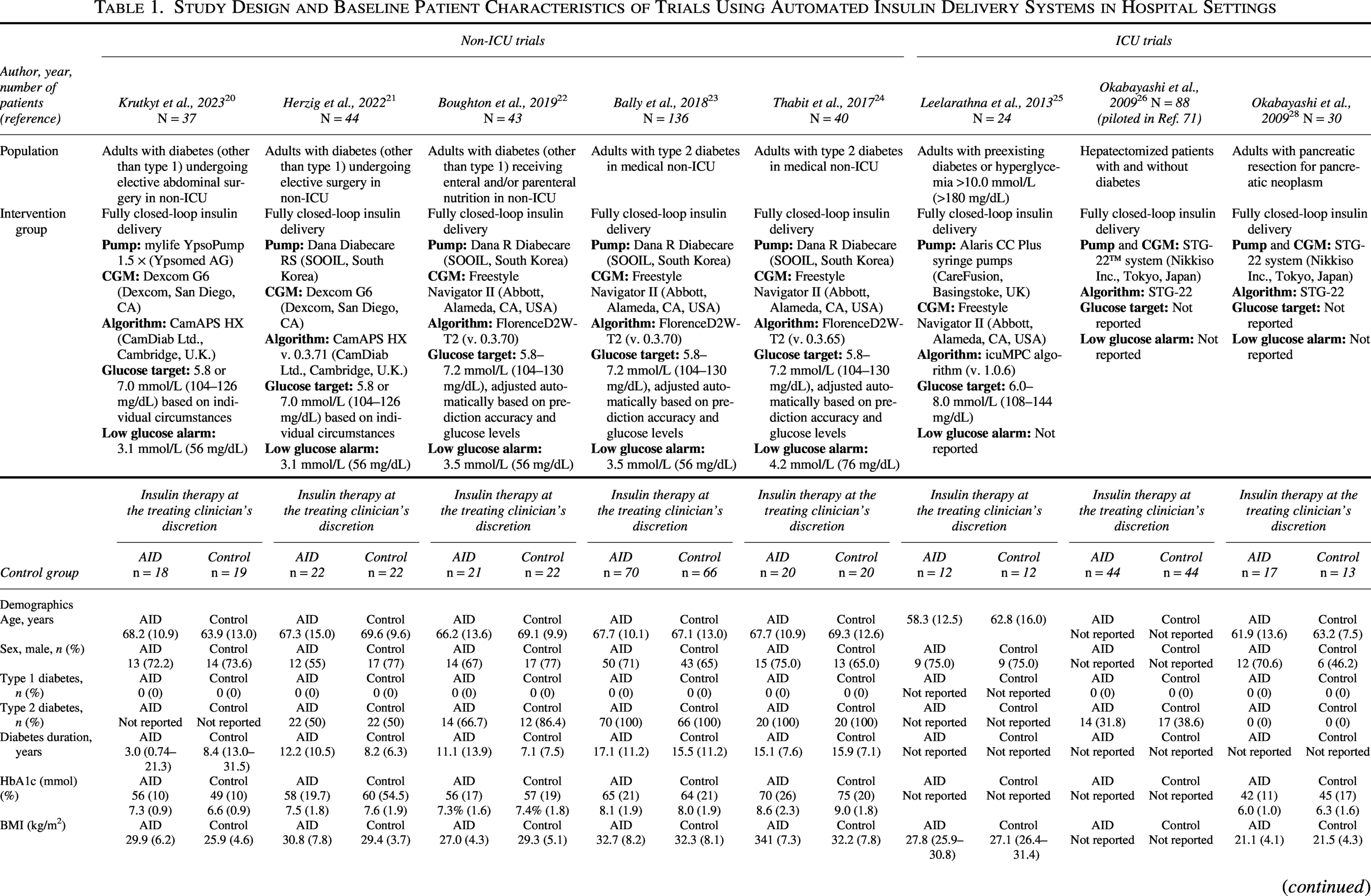
Data are presented as mean (SD) or median with interquartile range unless otherwise stated.
AID, automated insulin delivery; CGM, continuous glucose monitoring; ICU, intensive care unit; SD, standard deviation.
Glycemic Results from Trials on Automated Insulin Delivery Systems vs. Usual-of-Care in Hospital Settings
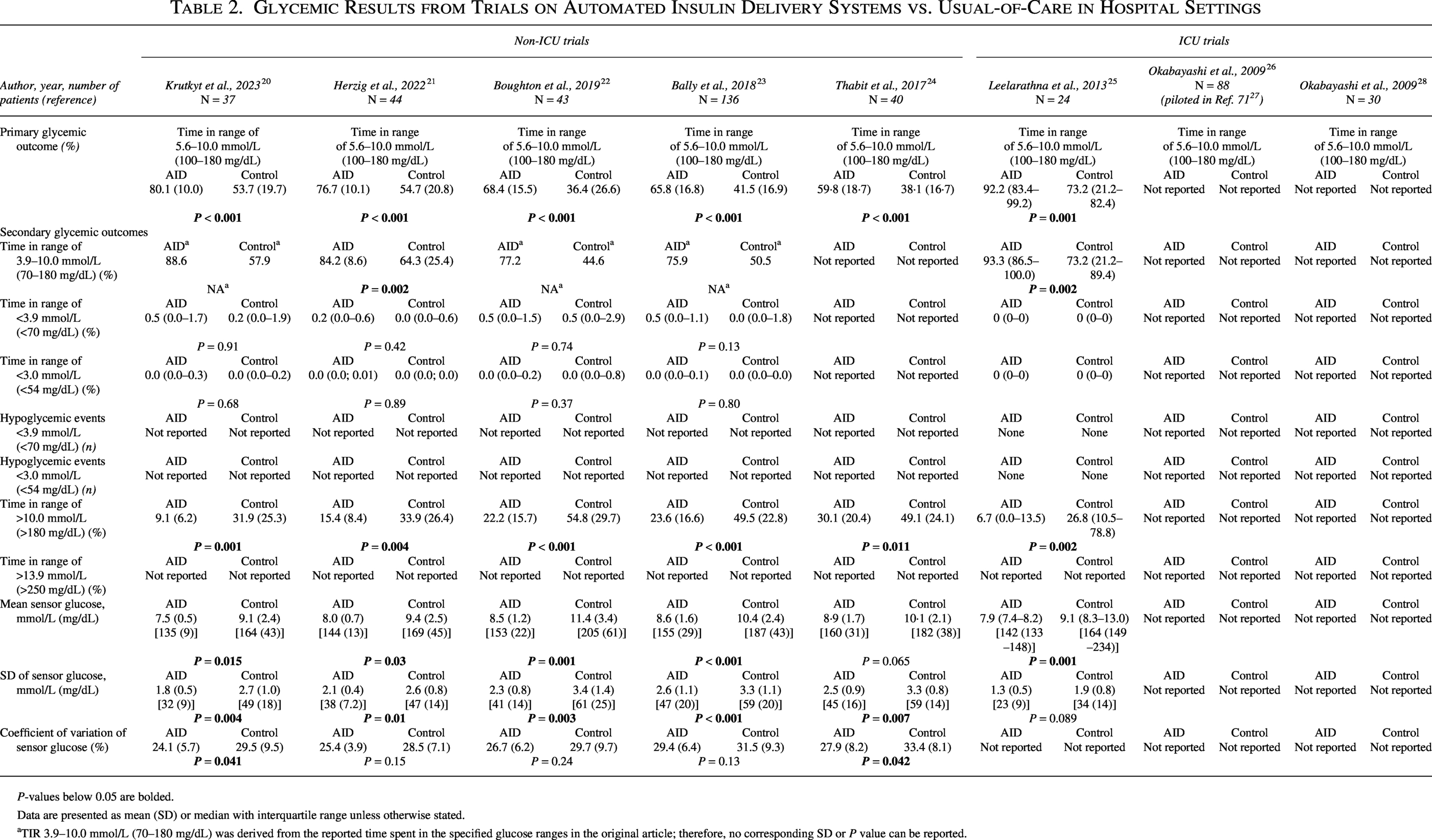
P-values below 0.05 are bolded.
Data are presented as mean (SD) or median with interquartile range unless otherwise stated.
TIR 3.9–10.0 mmol/L (70–180 mg/dL) was derived from the reported time spent in the specified glucose ranges in the original article; therefore, no corresponding SD or P value can be reported.
Outcomes
Primary outcome
Time in range (TIR) of 5.6–10.0 mmol/L (100–180 mg/dL) (%) for non-ICU (intensive care unit) trials29,30 and TIR of 7.8–10.0 mmol/L (140–180 mg/dL) (%) for ICU trials. 29
Secondary outcomes
TIRs of 3.9–10.0 mmol/L (70–180 mg/dL) (%), <3.9 mmol/L (<70 mg/dL) (%), <3.0 mmol/L (<54 mg/dL) (%), >10.0 mmol/L (>180 mg/dL) (%), >13.9 mmol/L (>250 mg/dL) (%); hypoglycemic events <3.9 mmol/L (<70 mg/dL) and <3.0 mmol/L (<54 mg/dL); mean sensor glucose; standard deviation of sensor glucose (mmol/L, mg/dL); coefficient of variation of sensor glucose (%) 31 ; and all reported clinical (i.e., nonglycemic) outcomes.
Meta-analysis
We applied both a fixed-effect inverse-variance model and a random-effects model using the Sidik–Jonkman estimator with Hartung–Knapp adjustment. We reported the estimates of the most conservative model as planned. Heterogeneity was assessed by visual inspection of forest plots and by calculating I2 statistics. The Clinical Diversity In Meta‐analyses (CDIM) tool was used to assess clinical heterogeneity among the included trials. 32 The meta-analysis was done in RStudio V4.3.0 using the “meta” package. 33
Certainty of evidence
We assessed the certainty of evidence using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework (Table 3). 34 Evidence certainty was classified as very low, low, moderate, or high, based on an overall evaluation of risk of bias, inconsistency, indirectness, imprecision, and potential publication bias.
Summary of Findings: Certainty of Evidence of the Effect of Automated Insulin Delivery Systems vs. Usual-of-Care on Glycemic Outcomes in Adult Hospitalized Individuals in Non–Intensive Care Unit Settings
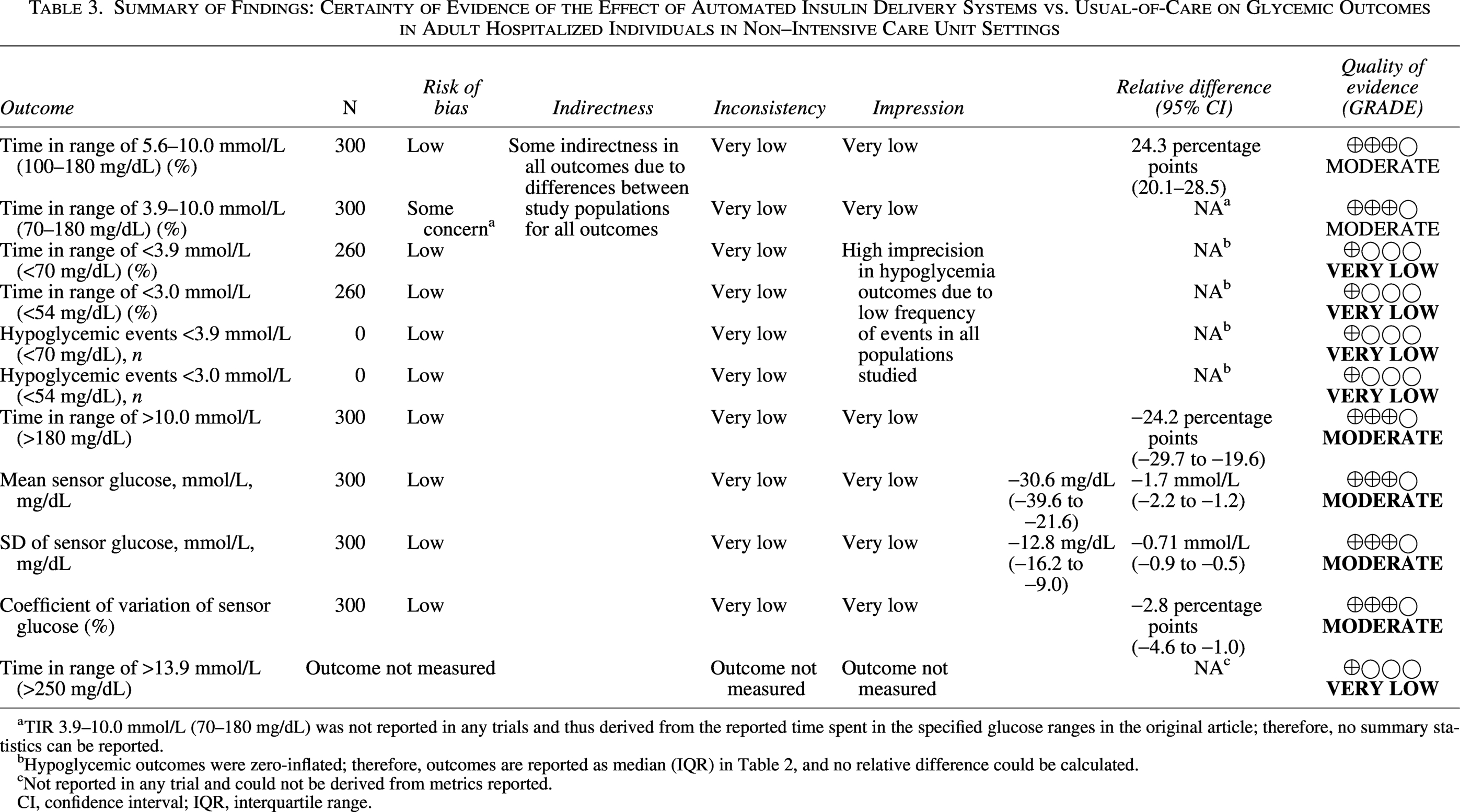
TIR 3.9–10.0 mmol/L (70–180 mg/dL) was not reported in any trials and thus derived from the reported time spent in the specified glucose ranges in the original article; therefore, no summary statistics can be reported.
Hypoglycemic outcomes were zero-inflated; therefore, outcomes are reported as median (IQR) in Table 2, and no relative difference could be calculated.
Not reported in any trial and could not be derived from metrics reported.
CI, confidence interval; IQR, interquartile range.
Risk of bias was assessed independently by two authors (M.T.O., A.L.L.) using the Cochrane RoB 2 tool. 35 Risk of bias was assessed for each of the domains: randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported results. Each domain was classified as having low risk of bias, some concerns, or high risk of bias using the algorithm provided in the RoB 2 tool. Based on the risk of bias in each domain, an overall risk of bias on the outcome level was assigned for each trial in the following way: If all domains were assessed as low risk of bias, then the overall risk of bias was adjudicated as low risk of bias. If one domain was rated as some concerns or with missing relevant information, the overall risk of bias was adjudicated as some concerns. If one or more domains had high risk of bias or two or more domains had some concerns, the overall risk of bias was adjudicated as high risk of bias.
Results
A total of 4581 references were screened, with 30 full-text references screened for eligibility. We included five RCTs from the non-ICU setting (N = 300 participants) and three RCTs from the ICU setting (N = 142) (Tables 1 and 2). A PRISMA flow diagram summarizes reference selection (Fig. 1).
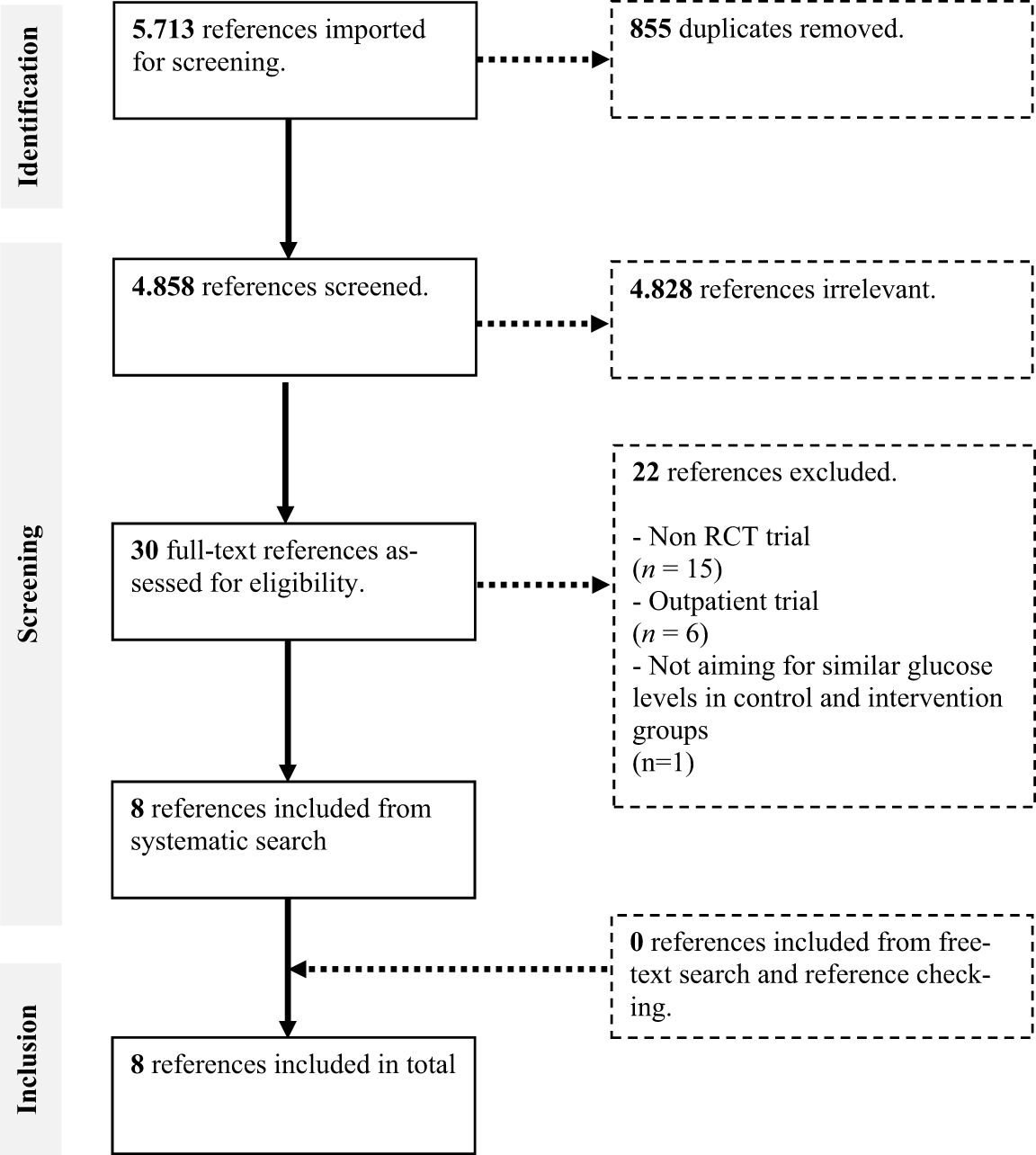
PRISMA diagram.
Risk of bias
Three trials had overall low risk of bias, four trials had some concerns, and a single trial had high risk of bias (Fig. 2). The most common reasons for some risk of bias were concerns about the randomization process.
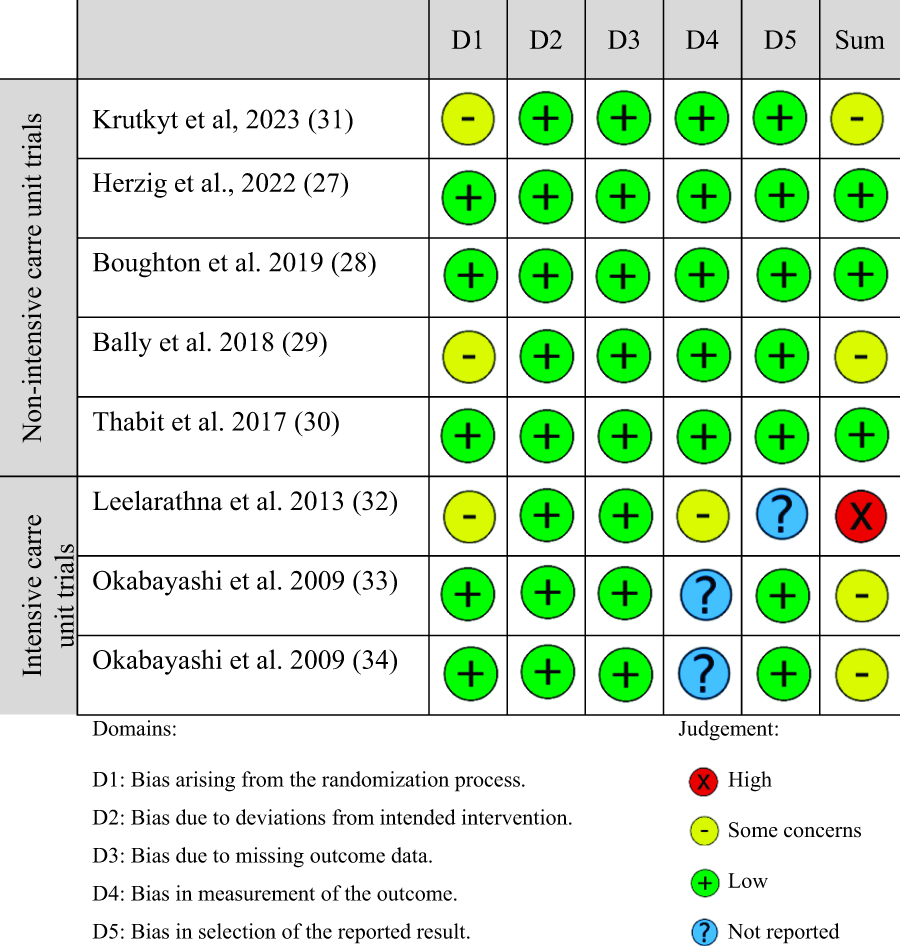
Risk of bias assessment.
Baseline characteristics
Across the non-ICU trials,20–24 participants had a mean age of 66–68 years, a predominance of type 2 diabetes (>80% with type 2 diabetes), and an average diabetes duration of 11–17 years (Table 1). Baseline HbA1c ranged from 56 to 70 mmol/mol (7.3%–8.6%), and mean body mass index was 27–32.7 kg/m2. Study populations included surgical patients undergoing elective procedures,20,21 general ward patients,23,24 and patients receiving enteral or parenteral nutrition. 22
In the three ICU trials,25,26,28 baseline characteristics were sparsely reported (Table 1). The trials included adults with preexisting diabetes or hyperglycemia >10.0 mmol/L (>180 mg/dL) in patients not known to have diabetes, 25 hepatectomized patients with and without diabetes, 26 and adults with pancreatic resection for pancreatic neoplasm. 28
Glycemic outcomes
AID systems consistently improved glycemic outcomes compared with usual care (Tables 2 and 3). Across the non-ICU trials,20–24 AID increased TIR 5.6–10.0 mmol/L (100–180 mg/dL) by 24.6 percentage points (95% confidence interval [CI] 20.7–28.5, moderate certainty) and reduced time spent in hyperglycemia >10.0 mmol/L (>180 mg/dL) by 24.2 percentage points (95% CI 19.6–29.7, moderate certainty). In AID users, mean sensor glucose decreased by 1.7 mmol/L (95% CI 1.2–2.2) (30.6 mg/dL, 95% CI 21.6–39.6 mg/dL), and glycemic variability, assessed by standard deviation and coefficient of variation, was reduced by 0.7 mmol/L (95% CI 0.5–0.9) (12.6 mg/dL, 95% CI 9.0–16.2 mg/dL) and 2.8 percentage points (95% CI 1.0–4.6), respectively (all moderate certainty).
Time spent in hypoglycemia (<3.9 mmol/L and <3.0 mmol/L) was low in both AID and control groups, with no apparent difference in hypoglycemic events; however, the certainty of evidence for these outcomes was very low. Between-study heterogeneity for primary glycemic outcomes was negligible (I2 = 0%), indicating consistent effects across diverse inpatient populations (Fig. 3).
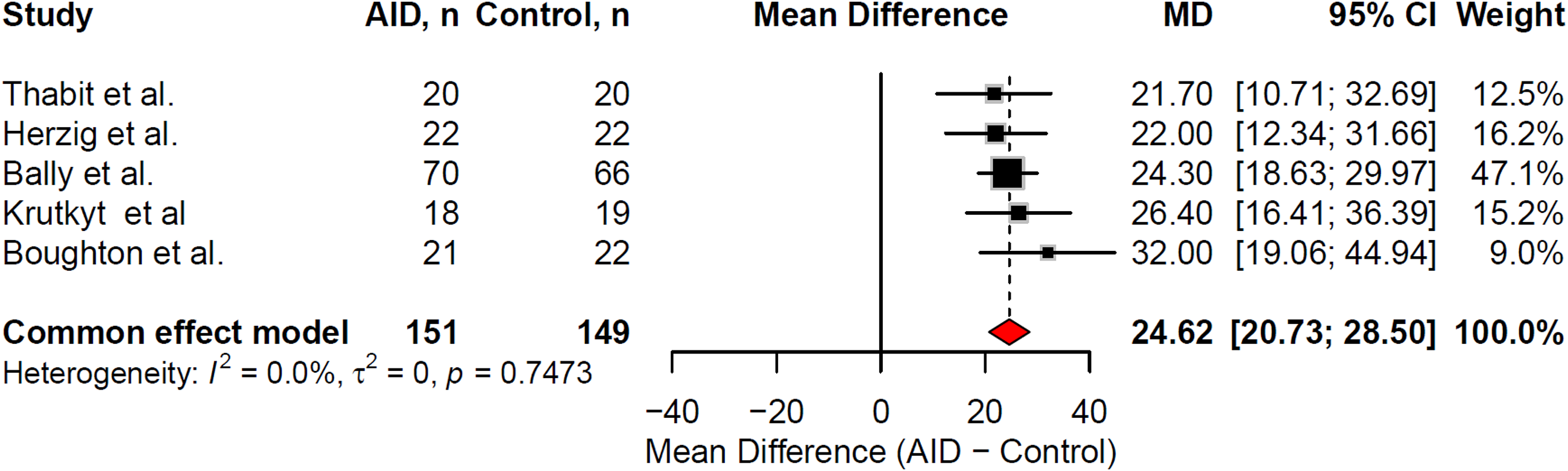
Forest plot of the effect of automated insulin delivery systems vs. usual-of-care on the primary outcome of time in range (5.6–10.0 mmol/L) (100–180 mg/dL) in adult hospitalized individuals in non–intensive care unit settings.
Similar results were found for the single ICU trial reporting traditional glycemic outcomes 25 (Table 2), while the other two ICU trials reported around a 3 mmol/L (54 mg/dL) decrease in glucose levels 18 h post-surgery from visual inspection of glucose graphs in AID users compared with usual of care.26,28 Glycemic outcomes were not consistently reported in any of the ICU trials and could not be meta-analyzed. None of the trials reported on the primary ICU glycemic outcome of TIR 7.8–10.0 mmol/L (140–180 mg/dL). None of the trials reported on the percentage of time with the AID systems in auto mode.
Clinical outcomes
Two non-ICU trials reported on patient satisfaction levels with the AID systems.23,24 Between 85% and 87% of patients were happy with their glucose levels during hospitalization, 90% and 98% were satisfied with the AID system, and 95% and 100% would recommend the AID system to a friend or family member.
Two ICU trials reported clinical outcomes. One trial demonstrated a reduction in surgical site infections in the AID group compared with usual care (2.3% vs. 18.2%, P = 0.030), as well as a reduction in length of hospital stay, although the reduction was not specified (P = 0.049). 26 One other ICU trial reported no difference in 30-day or all-cause mortality. 28 None of the non-ICU trials reported on clinical outcomes.
Discussion
In this systematic review with meta-analysis of RCTs evaluating AID systems in hospital settings, we found that AID consistently improved glycemic outcomes compared with usual care. AID increased TIR 5.6–10.0 mmol/L (100–180 mg/dL) by approximately 24 percentage points, reduced time spent in hyperglycemia, lowered mean sensor glucose, and reduced glycemic variability. Importantly, these improvements were consistent across diverse inpatient populations and clinical contexts and achieved without an increase in hypoglycemia. In addition, AID systems were associated with high levels of patient satisfaction in the non-ICU setting. Notably, exploratory subgroup analyses reported in the primary studies included in this review suggest that individuals with highly variable insulin requirements—such as patients undergoing hemodialysis or pancreatic surgery—may derive particular benefit from AID therapy, with improvements exceeding 30 percentage points in time spent within the target glucose range.36,37 In the included non-ICU trials, participants’ mean glucose levels clustered around the upper TIR threshold of 10 mmol/L (180 mg/dL) in control groups but were reduced to approximately 8 mmol/L (144 mg/dL) in AID groups (Table 2), thereby placing a greater proportion of readings within TIR in AID groups. Consequently, relatively small decreases in mean glucose with AID use may have resulted in disproportionately large increases in TIR, as observed in the present review. The clinical implications of these discordant changes in glycemic metrics in the inpatient setting remain uncertain.
The findings of the present review should be interpreted in the context of established inpatient diabetes strategies. Despite guidelines advocating target glucose ranges of 5.6–10.0 mmol/L (100–180 mg/dL) in non-ICU settings,29,30 real-world data suggest that these targets are frequently not achieved with conventional multiple daily injection regimens.38–40 Similar challenges are observed in the ICU setting, where recommended glycemic targets are slightly higher of 7.8–10.0 mmol/L (140–180 mg/dL),29,41 yet remain difficult to consistently attain in routine clinical practice.42,43
The complexities of in-hospital diabetes management often necessitate specialized diabetes teams for patients on nondiabetes wards. Such teams have been consistently linked to shorter hospital stays, fewer complications, higher patient satisfaction, and improved cost-effectiveness.44–46 The landmark RABBIT trial47,48 demonstrated that basal–bolus insulin therapy significantly improved glycemic outcomes and reduced postoperative complications compared with correctional insulin or “sliding scale insulin” alone in patients with type 2 diabetes, supporting the adoption of near-normophysiological insulin regimens over reactive (i.e., sliding scale) approaches in hospital settings. However, while basal–bolus therapy improves glycemic outcomes relative to sliding scale insulin, it requires frequent glucose monitoring and manual dose titration, which increase workload, require insulin titration experience, and may predispose to hypoglycemia.39–41,49
In this context, AID systems offer a physiologically responsive alternative. 50 By integrating CGM with algorithm-driven insulin titration, AID systems dynamically adapt to changing insulin sensitivity and carbohydrate exposure. The magnitude of improvement in TIR observed in this review—comparable to or exceeding that reported in outpatient trials 51 —suggests that algorithm-driven insulin delivery may be particularly well suited to the highly dynamic metabolic conditions encountered in hospital settings. The same findings have been observed when CGM is used alone in combination with a paper-based (nonautomatically integrated) insulin titration algorithm in the non-ICU setting.5,52,53
While glycemic effects appear consistent, implementation remains complex.17,51,54 Surveys of health care professionals indicate variable familiarity and comfort with inpatient diabetes technologies.9,55,56 Depending on institutional policies, some patients may be allowed to continue using their personal AID systems during hospitalization.29,57 Modern AID systems provide flexible glucose target settings and support adaptive insulin delivery based on daily patterns, circadian variation, and postprandial responses. Certain systems also include adjustable algorithm intensity features, such as “Boost” and “Ease-off” modes, which increase or decrease insulin delivery aggressiveness as needed.58 In addition, CamAPS FX systems offer simplified meal announcements that diminish the need for carbohydrate counting, while CamAPS HX systems—used in the two most recent non-ICU trials—operate fully automatically without any meal announcements. Several other AID companies are also developing AID systems, in which meal announcement is of less importance for achieving improved glycemic outcomes. This feature may provide substantial advantages in the inpatient setting, where carbohydrate counting is often impractical.20,21 Despite these advances, several limitations remain. The HX system is not yet commercially available, automation relies on a smartphone-hosted algorithm requiring continuous Bluetooth connectivity, and data uploads through Glooko may be delayed. Furthermore, compatibility is restricted to durable tubed insulin pumps, including the YpsoPump, which has a comparatively limited insulin reservoir capacity of 160 units.59 In addition, a limitation of AID use in general is the lack of integration of all systems directly into the electronic medical record, which would facilitate easy overview, documentation, and safety.
CGM has become increasingly integrated into inpatient diabetes care and forms the technological foundation on which AID systems rely. A meta-analysis of six RCTs (979 participants in non-ICU settings) found that CGM improved TIR 3.9–10.0 mmol/L (70–180 mg/dL) by approximately 7 percentage points compared with POC testing, although with significant between-trial variability.60 However, more recent RCTs have shown mixed findings: the TIGHT trial61 and Thabit et al.62 reported no significant glycemic benefit, whereas the DIATEC trial demonstrated that CGM combined with insulin titration protocols and inpatient diabetes team input increased TIR by approximately 15 percentage points and reduced hypoglycemia, hyperglycemia, glycemic variability, insulin requirements, in-hospital complications, and improved patient treatment satisfaction.5,52,63
Importantly, inpatient CGM accuracy is not uniform and may be affected by clinically relevant interferences. These include medications such as acetaminophen, ascorbic acid, and hydroxyurea, as well as physiological conditions such as poor peripheral perfusion, hypoglycemia, severe hyperglycemia, acidosis, anemia, and mechanical factors such as sensor compression.13,14,31,64 These accuracy limitations are particularly important in the context of AID systems, which depend directly on CGM input for automated insulin dosing, meaning that sensor error may translate into inappropriate insulin delivery. Accordingly, clinical recommendations emphasize structured inpatient CGM use, including confirmatory POC testing during initiation and when discrepancies arise, calibration of the CGM (if possible), and discontinuation or replacement in cases of persistent discordance.13,15,65–67
Most of the trials in this review were conducted in specialized centers with research oversight and experienced teams often within a small number of collaborating groups. Whether similar glycemic improvements can be achieved in broader real-world hospital environments remains to be demonstrated. While traditional insulin strategies are labor-intensive, AID systems—particularly experimental ICU setups—may introduce additional workload related to device setup, monitoring, and ensuring CGM accuracy. Therefore, a key priority for future research is to determine whether standard, commercially available AID systems can be implemented safely and effectively in typical hospital settings beyond highly specialized centers. Economic evaluations are also lacking. Although AID systems may reduce staff workload and potentially complications, device costs, and infrastructure requirements, including upgrading staff knowledge and skills, must be considered.55,68,69 It should be noted that the AID devices employed in the ICU were experimental, with no established commercialization pathway, rendering their transition to routine clinical use less clear compared with non-ICU studies. Likewise, although these RCTs were conducted in individuals without type 1 diabetes, most hospitalized patients already using AID systems have type 1 diabetes, limiting the applicability of these findings, particularly in the context of continuing established AID use rather than initiating devices in otherwise AID-naïve inpatients. In addition, the included trials typically excluded clinical scenarios in which CGM performance may be unreliable (e.g., medication interference, kidney failure, severe hypoperfusion), further limiting generalizability to real-world hospital populations. Furthermore, no internationally endorsed consensus guideline currently exists for AID use in the hospital setting, including recommendations on continuing personal AID systems during hospitalization, initiating AID in hospitalized patients, or introducing AID prior to discharge to support outpatient use. Development of such consensus guidance may represent a critical first step toward wider hospital implementation of AID systems.
Strengths and Limitations
To the best of our knowledge, this is the first systematic review assessing inpatient AID use. This review has several strengths. We conducted a comprehensive search across multiple databases without date restrictions, adhered to PRISMA 2020 standards, applied risk-of-bias assessment using RoB 2, and evaluated certainty of evidence using GRADE. Statistical heterogeneity was minimal for primary glycemic outcomes, enhancing confidence in the consistency of effect estimates.
Several important limitations should be acknowledged. First, the number of randomized trials and the total number of participants were modest. Second, three out of five of the non-ICU trials were conducted by a collaborative group of authors in Switzerland and the United Kingdom,22–24 which may limit generalizability and increase the risk of investigator-related bias. Third, study populations were restricted to adults, predominantly with type 2 diabetes, and none included individuals with type 1 diabetes in non-ICU settings. Fourth, control groups were frequently described as “insulin therapy at clinician discretion,” which may not reflect optimized basal–bolus therapy. Finally, most trials evaluated glycemic metrics only rather than hard clinical endpoints such as infection rates, length of stay, readmissions, or mortality. Consequently, although improvements in TIR represent biologically and clinically plausible surrogate outcomes in the inpatient setting, direct evidence demonstrating improved clinical outcomes remains limited for inpatient AID systems.
Conclusion
AID systems significantly improve glycemic outcomes compared with usual care, increasing TIR and reducing hyperglycemia and glycemic variability without increasing hypoglycemia in adults with diabetes in non-ICU settings. These findings support the feasibility and efficacy of AID systems in non-ICU hospital settings. The certainty of evidence for most of these outcomes is moderate but remains low for hypoglycemic and clinical endpoints. Evidence for the ICU setting remains limited. Larger, pragmatic multicenter trials powered for clinical outcomes are needed to confirm safety, cost-effectiveness, and generalizability.
Authors’ Contributions
M.T.O. conceptualized the study in collaboration with A.L.L., and J.K.M. M.T.O. drafted the first version of the manuscript. All authors contributed significantly to the interpretation of study results, structuring of the manuscript, and provided critical review of the content of the manuscript.
Author Disclosure Statement
M.T.O.: Serves on the scientific advisory board for decide Clinical Software GmbH (GlucoTab).
A.L.L.: Has received speaker fees and/or support to attend conferences from Dexcom and Novo Nordisk and research support from the Association of British Clinical Diabetologists.
E.G.W.: Has received personal fees from Abbott, AstraZeneca, Dexcom, Eli Lilly, Embecta, Insulet, Medtronic, Novo Nordisk, Roche, Sanofi, Sinocare, and Ypsomed and research support from Abbott, Embecta, Insulet, Novo Nordisk, and Sanofi.
H.T.: Has received research support from Dexcom Inc and participated in advisory groups for Dexcom, Medtronic, Sanofi, and Roche Diabetes.
K.D.: Has received honoraria, travel, or fees for speaking or advisory boards from Abbott Diabetes, AstraZeneca, Boehringer-Ingelheim, Eli Lilly, Menarini, Novo Nordisk A/S, Roche, and Sanofi Diabetes.
J.K.M.: Member of advisory boards of Abbott Diabetes Care, Becton-Dickinson, Dexcom, Eli Lilly, Embecta, Insulet, Medtronic, Novo Nordisk A/S, Pharmasens, Roche Diabetes Care, Sanofi-Aventis, Tandem, and Viatris. She has received speaker honoraria from A. Menarini Diagnostics, Abbott Diabetes Care, Buzud, Dexcom, Eli Lilly, Medtrust, Novo Nordisk A/S, Roche Diabetes Care, Sanofi, Sinocare, Viatris, and Ypsomed. She is a shareholder of decide Clinical Software GmbH and elyte Diagnostics and serves as CMO of elyte Diagnostics.
K.N.: Serves as an adviser to Medtronic, Abbott, Convatec, and Novo Nordisk; owns shares in Novo Nordisk; has received research grants to the institution from Novo Nordisk, Zealand Pharma, Dexcom, and Medtronic; and has received fees for speaking from Medtronic and Novo Nordisk.
Rest of the authors declare no conflict of interest.
Footnotes
Funding Information
European Foundation for the Study of Diabetes (grant no. 97109). The funder had no role in the making of this review.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.