
Abstract
Background:
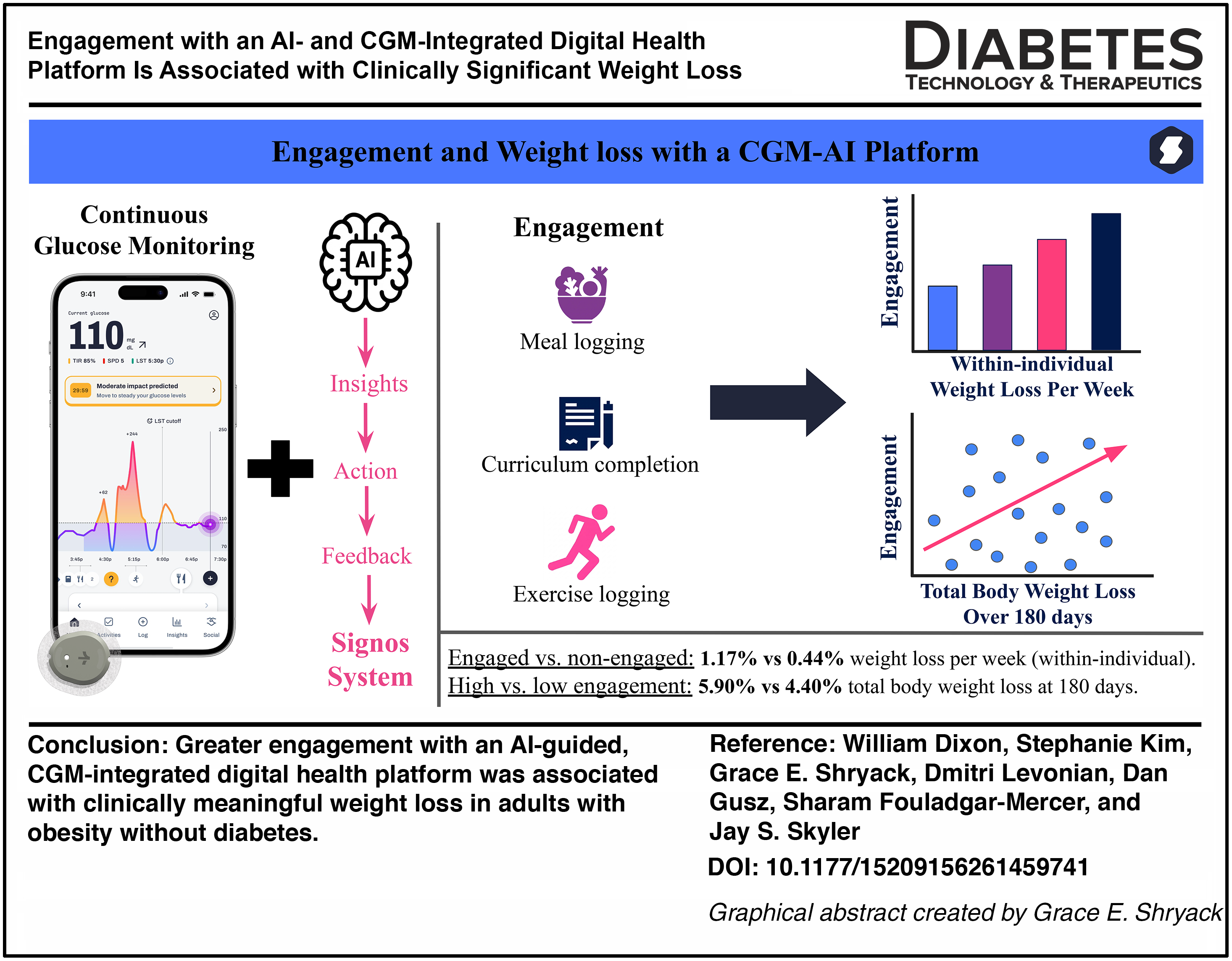
Obesity affects millions of U.S. adults and is linked to cardiometabolic disease. This study examined whether user engagement with the Signos app, which combines artificial intelligence (AI) and continuous glucose monitoring (CGM), is associated with weight loss.
Methods:
This study included adults (≥18 years) with BMI ≥ 30 kg/m2 and without diabetes who enrolled in the Signos System, a platform integrating CGM data with AI-driven behavioral recommendations informed by glucose responses, dietary intake, physical activity, and user-entered data. Engagement was quantified as total meaningful actions per day (TMAPD). Longitudinal within-participant analyses compared weight change during engaged (TMAPD > 0) and nonengaged (TMAPD = 0) periods among 3007 participants, expressed as weight loss percentage per week (WLPW%). Cross-sectional analyses evaluated 180-day total body weight loss (TBWL) among 1147 participants.
Results:
In this longitudinal cohort, weight loss was greater during periods of engagement than non-engagement (1.17% ± 0.04% vs. 0.44% ± 0.03% per week; P < 0.001). Weight loss during engaged periods did not differ significantly between early and late engagers (P > 0.05). In the 180-day cohort (n = 1,147), mean TBWL was 5.14% ± 0.19%. Participants with higher engagement (TMAPD ≥ 1.02) achieved 5.90% ± 0.25% TBWL compared with 4.38% ± 0.23% in the lower engagement group (P < 0.001).
Conclusions:
Greater engagement with the Signos System was associated with greater weight loss in adults with obesity and without diabetes. Weight loss outcomes were similar regardless of whether engagement occurred earlier or later during platform use. These findings suggest that engagement with AI-guided, CGM-informed behavioral interventions may support clinically meaningful weight reduction. Approved by the WCG Institutional Review Board (protocol no. 20212524) and conducted in accordance with the Declaration of Helsinki.
Introduction
Obesity is a chronic, multifactorial disease associated with substantial morbidity, including type 2 diabetes, cardiovascular disease, and certain cancers.1–4 Despite growing awareness and expanding treatment options, the prevalence of obesity continues to rise, underscoring the need for scalable and effective interventions that support sustained behavior change.5–7 Traditional approaches to weight management, including lifestyle counseling and self-monitoring, often rely on retrospective tracking and generalized recommendations, which may limit their effectiveness in real-world settings. Digital health platforms have emerged as a promising approach to deliver behavioral, personalized interventions at scale.8–13 However, the effectiveness of these platforms has been variable, with many applications demonstrating modest weight loss outcomes and high attrition rates.11,13–15 A key limitation of many existing digital health tools is their reliance on passive tracking or static feedback, requiring users to interpret their own data and apply generalized recommendations. Consistent with this, systematic reviews of automated digital interventions report modest weight loss outcomes, often failing to achieve clinically meaningful thresholds of ≥5% total body weight loss threshold endorsed by clinical guidelines and associated with meaningful improvement in cardiometabolic risk.16–18
Advances in continuous glucose monitoring (CGM) and artificial intelligence (AI) have enabled a more dynamic approach. Prior literature has evaluated this approach primarily in individuals with prediabetes and diabetes, where it has been used to predict diabetes-related events and support adaptive insulin management.19–21 Emerging evidence suggests growing interest in CGM use among individuals without diabetes; however, studies in these populations remain limited with respect to weight-related outcomes. 22 The Signos System integrates CGM data with AI-driven analytics to deliver personalized, real-time recommendations designed to support behavior at key decision points to aid in weight loss. 23 This represents a shift from retrospective tracking to a continuous, feedback-driven model that may better support in-the-moment decision-making.
Engagement is a well-established driver of improved outcomes in digital interventions, yet most evidence comes from platforms that rely on static feedback.14,24–26 Whether this relationship holds, and to what extent, for more dynamic, CGM-integrated, AI-driven systems remains unclear. In particular, it is unknown whether higher engagement with real-time, personalized feedback translates into greater weight loss.
This study evaluates the relationship between engagement and weight loss within the Signos System using both longitudinal within-participant analyses and cross-sectional outcomes at 180 days. The primary hypothesis was that engaged periods would be associated with greater weight loss than nonengaged periods within the same individuals, regardless of when engagement occurred during platform use. As digital health therapeutics become increasingly sophisticated, maximizing both their effectiveness and the duration of engagement remains crucial.
Methods
Study design
This retrospective cohort study evaluated adults who voluntarily enrolled in the Signos mobile metabolic health platform and was conducted in accordance with the Declaration of Helsinki and all applicable ethical guidelines and regulations under WCG Institutional Review Board (protocol no. 20212524). Participants voluntarily enrolled through the mobile application, completed app-based screening and consent, and were prescribed a CGM with access to the Signos system. Eligible participants were required to be at least 18 years-of-age, have obesity, defined as a body mass index (BMI) of at least 30 kg/m2, able to speak and read English, and owned a smartphone compatible with the Signos mobile app. 23 Participants were required to have enrolled between January 1, 2022, and June 30, 2024, and to have at least 1 day of CGM data available. Individuals with type 1 or type 2 diabetes, eating disorders, specialized dietary requirements, pregnancy, incarceration, or on certain medications (GLP-1s) were excluded. To screen for undiagnosed type 2 diabetes, a rolling 90-day mean CGM glucose was computed for each participant (minimum 9 valid CGM days). Individuals whose mean glucose reached ≥140 mg/dL (equivalent to an estimated A1C ≥6.5%) were notified, removed from the protocol, and therefore excluded from further study participation and analysis. A total of 703 enrolled users (∼2.3%) were excluded on this basis. Length of participation was not predetermined, and individuals could withdraw at any time. The race/ethnicity of the participants were not collected. Participant flow and cohort selection are summarized in Supplementary Table S1.
The Signos system
The Signos system is a digital health application integrating CGM with an AI–driven mobile application (SignosAI). 23 The system aggregates multimodal data, including CGM-derived glucose values, dietary logs, physical activity, sleep, heart rate, and other user-entered inputs. These data are processed using machine-learning algorithms to identify individualized metabolic patterns and generate personalized behavioral recommendations. Outputs are delivered within the mobile application in near real time to support decision-making related to diet, activity, and other lifestyle behaviors. The platform tracks individual glucose responses to meals and exercise, allowing users to observe how specific foods and activities affect their glucose patterns. Daily glucose metrics, including average glucose and glucose variability, are displayed on the home screen alongside day-to-day and weekly trends, and weekly summaries contextualize exercise, sleep, weight, and food intake against these glucose patterns. Behavioral recommendations emphasize switching to less-processed carbohydrates, prioritizing protein and fiber, sequencing meals (protein and vegetables before carbohydrates), and postmeal physical activity rather than outright carbohydrate restriction. In-app educational modules reinforce these principles across nutrition, activity, and lifestyle domains. Representative example screens from the Signos application are provided in Supplementary Figures S1, S2, S3, S4, S5, and S6.
Data sources
All data were collected through the Signos System and connected devices. These included CGM glucose data, participant-entered weight, meal logs, exercise logs, sleep data, hydration logs, and device-derived data from smart scales and wearable devices when available. Participants provided a baseline weight at onboarding and could log subsequent weights either manually or via synchronized devices. Across the 3007 participants, 71,507 weight measurements were logged. Of these, 80.2% were captured automatically from synchronized smart scales, and 19.8% were entered manually, including each participant’s baseline weight at onboarding. The Signos application delivered a weekly in-app check-in suggesting that participants log a weight; weighing frequency was otherwise at the participant’s discretion. Implausible weight values were excluded using predefined anomaly detection rules. Weight change for any interval was calculated only when a valid weight measurement was available within 24 h of both the start and end of that interval.
Engagement
Engagement was defined as intentional participant actions within the platform, including meal, exercise, and weight logging, curriculum participation, responses to AI-generated insights, note entry, and CGM sensor interactions. Passive data collection (e.g., CGM or wearable data streams) was not considered engagement. Intentional actions were aggregated as Total Meaningful Actions (TMA). Engagement was summarized as TMA per Day (TMAPD) over the relevant observation window. A schematic representation of the relationship between CGM data, weight logs, and engagement periods is shown in Figure 1.
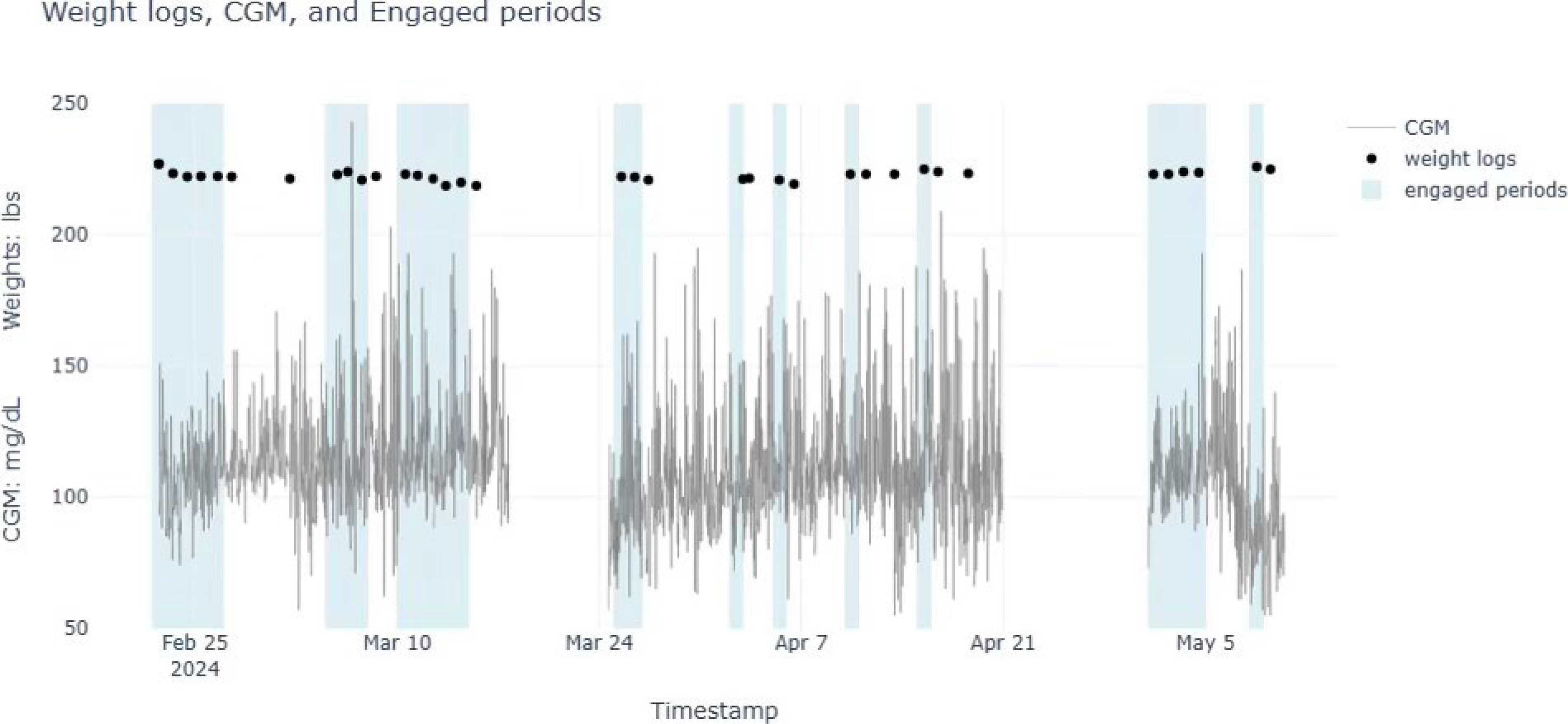
Schematic of weight logs, CGM use, and engaged periods. CGM, continuous glucose monitoring.
Longitudinal analysis
Longitudinal analysis was chosen to evaluate weight loss across different levels of engagement. Among 3007 participants, weight change was normalized to the duration of each interval and expressed as weight loss percentage per week (WLPW%). Time on Signos was divided into intervals that were classified as engaged (TMAPD > 0) or unengaged (TMAPD = 0) for each participant. Mean WLPW% was calculated separately for engaged and unengaged intervals, and these values were compared within individuals. To assess whether the association between engagement and weight loss was influenced by time on platform, participants were additionally classified according to whether their engaged intervals occurred predominantly earlier or later during their participation, and mean WLPW% during engaged intervals was compared between these groups. Anomaly detection procedures were applied to remove implausible weight entries, including extreme or physiologically impossible values (such as a weight of 0 lbs or 1800 lbs). Valid weight change required measurements within 24 h of the period start and end.
Cross-sectional 180-day analysis
Cross-sectional analyses evaluated the association between amount of engagement and weight change over 180-days on the Signos System. Of the 3007 participants in the longitudinal analysis, 1147 participants logged a weight measurement within 180 ± 5 days. Total body weight loss percentage (TBWL%) was calculated at approximately 180 days relative to baseline. Participants were included if they had a weight measurement within days 175–185 following enrollment; when multiple measurements were available, the value closest to day 180 was used. Mean TMAPD over the first 180 days was calculated for each participant, and participants were stratified into low (TMAPD < 1.02) and high engagement (TMAPD > 1.02) groups based on the cohort median TMAPD of 1.02. TBWL% was compared between engagement groups, and the association between TMAPD and TBWL% was evaluated using correlation analysis. Behavioral measures at 180 days, including exercise duration, exercise energy expenditure, and meal logging frequency, were assessed in the same cohort and compared between engagement groups.
Statistics
The primary within-subject comparison of WLPW% during engaged versus nonengaged intervals was evaluated by paired t-test; secondary between-subject comparisons (early vs. late engagers; low vs. high 180-day engagement) used two-sample t-tests. The correlation between mean TMAPD over the first 180 days and TBWL% at 180 days (Fig. 2) was assessed using Pearson’s correlation coefficient. All analyses were stratified by baseline obesity class (Class I: BMI 30.0–34.9; II: 35.0–39.9; III: ≥40.0 kg/m2), sex, and age group. Results are presented as mean ± SE; tests were two-sided with P < 0.05. The primary within-subject comparison was treated as confirmatory; all remaining analyses, including subgroup, timing, cross-sectional, and behavioral comparisons, were prespecified but interpreted as exploratory, and formal correction for multiple comparisons was not applied. Given the retrospective design, no a priori sample size calculation was performed; the analytic cohort comprised all eligible enrollees within the study window. A post-hoc sensitivity analysis (α = 0.05, two-sided; 80% power) yielded minimum detectable effects of 0.15% for the primary within-subject comparison (n = 3,007 paired; SD of paired difference = 2.84%) and 1.07% for the cross-sectional comparison (n = 569 vs. n = 578; SD = 6.47%).
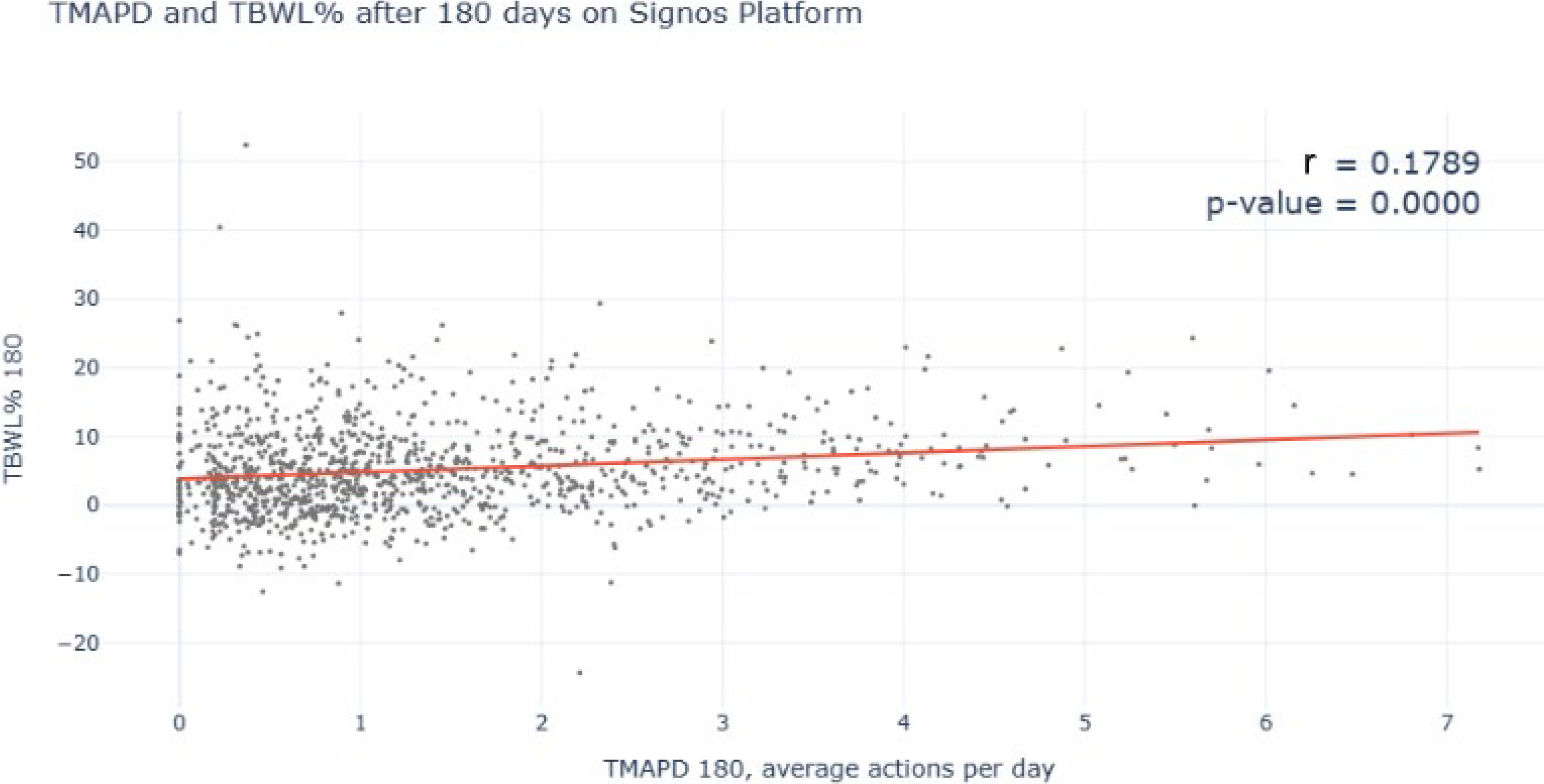
Correlational analysis between total body weight loss (%) and total meaningful actions per day across 180-days on the Signos System.
Results
Primary goals at enrollment
At onboarding, 2390 of the 3007 participants (79.5%) selected weight loss as their primary goal, representing 86.0% of those who specified a goal. The remainder selected health and wellness (6.8%), metabolic insight (5.5%), or other goals such as increased energy, optimized workouts, or increased muscle mass (0.7%); 7.5% did not report a goal.
Longitudinal engagement analysis: Unengaged versus. engaged
Among 3007 subjects identified (Table 1), longitudinal analyses evaluated periods of nonengagement (TMAPD = 0) and engagement (TMAPD > 0) within individuals. Mean WLPW% was greater during engagement compared with nonengagement (0.44% ± 0.03% vs. 1.17% ± 0.04%, P < 0.001). When stratified by baseline obesity class, greater weight loss during engagement compared with nonengagement was observed across all groups: Obesity Class I (WLPW% nonengagement 0.40% ± 0.04% vs. engagement 1.13% ± 0.05% P < 0.001), Obesity Class II (WLPW% nonengagement 0.43% ± 0.06% vs. engagement 1.21% ± 0.09%, P < 0.001), and Obesity Class III (WLPW% nonengagement 0.61% ± 0.10% vs. 1.24% ± 0.08%, P < 0.001).
Weight Loss per Week (%) During Engaged and Unengaged Periods
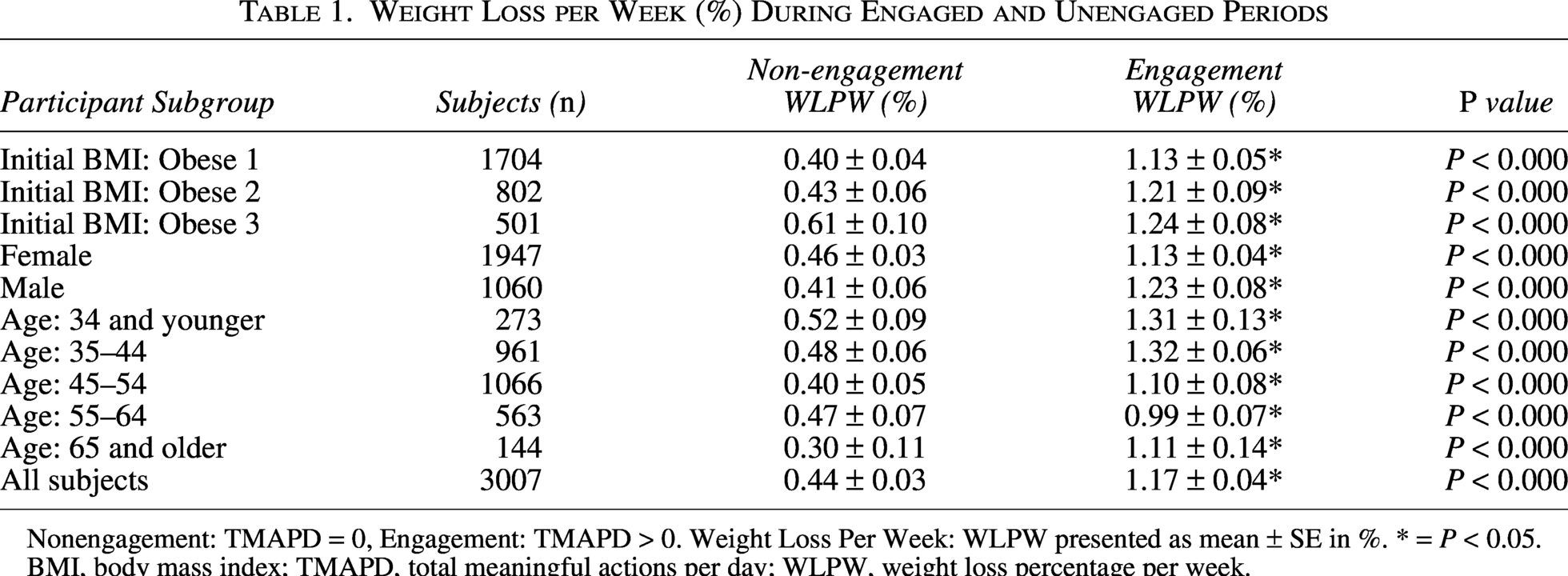
Nonengagement: TMAPD = 0, Engagement: TMAPD > 0. Weight Loss Per Week: WLPW presented as mean ± SE in %. * = P < 0.05.
BMI, body mass index; TMAPD, total meaningful actions per day; WLPW, weight loss percentage per week.
When stratified by sex, greater weight loss during engagement compared with nonengagement was also observed across both groups: female participants (WLPW% nonengagement 0.46% ± 0.03% vs. engagement 1.13% ± 0.04%, P < 0.001) and male participants (WLPW% nonengagement 0.41% ± 0.06% vs. engagement 1.23% ± 0.08%, P < 0.001). When stratified by age group, this trend was consistent across all groups: ≤34 years (WLPW% nonengagement 0.52% ± 0.09% vs. engagement 1.31% ± 0.13%, P < 0.001), 35–44 years (WLPW% nonengagement 0.48% ± 0.06% vs. engagement 1.32% ± 0.06%, P < 0.001), 45–54 years (WLPW% nonengagement 0.40% ± 0.05% vs. engagement 1.10% ± 0.08%, P < 0.001), 55–64 years (WLPW% nonengagement 0.47% ± 0.07% vs. engagement 0.99% ± 0.07%, P < 0.001), and ≥65 years (WLPW% nonengagement 0.30% ± 0.11% vs. engagement 1.11% ± 0.14%, P < 0.001).
Longitudinal engagement analysis: Late v Early engagement
To evaluate whether timing of engagement influenced weight loss outcomes, participants were stratified into early and late engagement groups (Table 2). Mean WLPW% did not differ between early and late engagement groups (1.18% ± 0.05% vs. 1.12% ± 0.07%, P = 0.484). When stratified by baseline obesity class, no significant differences were observed: Obesity Class I (WLPW% early 1.16% ± 0.06% vs. late 1.03% ± 0.09%, P = 0.257), Obesity Class II (WLPW% early 1.25% ± 0.11% vs. late 1.11% ± 0.13%, P = 0.449), and Obesity Class III (WLPW% early 1.16% ± 0.09% vs. late 1.43% ± 0.18%, P = 0.172).
Weight Loss per Week (%) during Early and Late Engagement
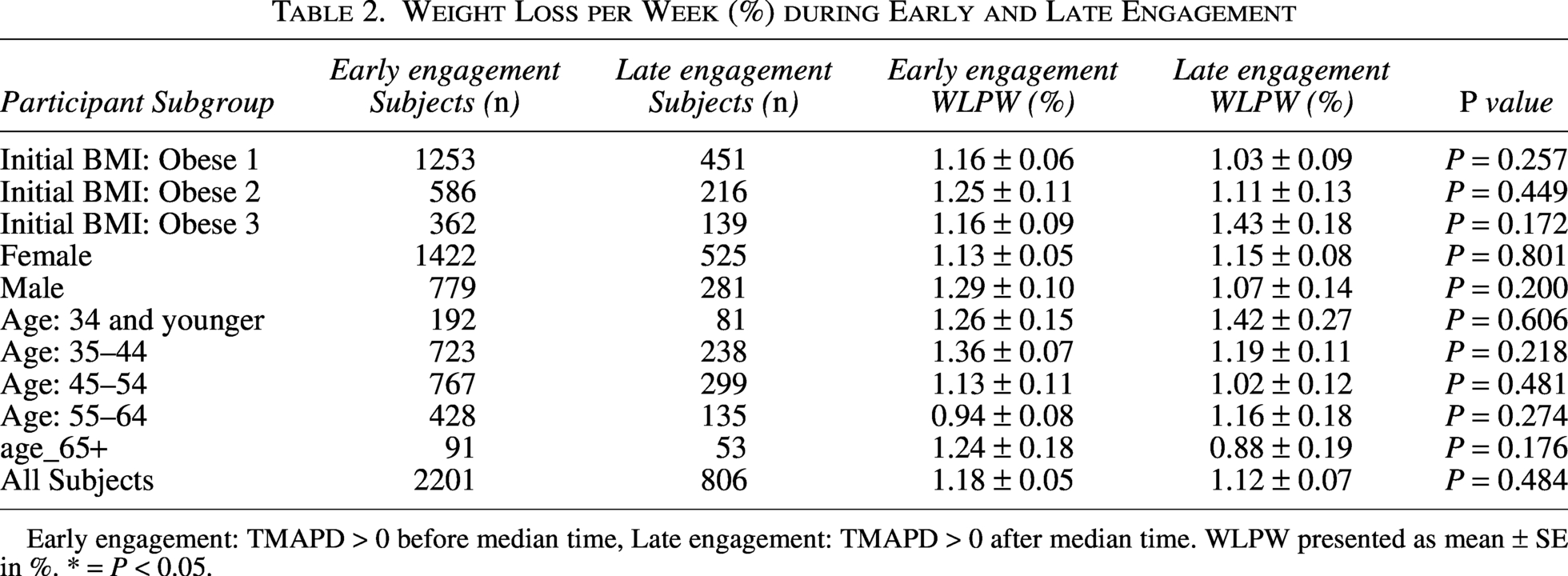
Early engagement: TMAPD > 0 before median time, Late engagement: TMAPD > 0 after median time. WLPW presented as mean ± SE in %. * = P < 0.05.
Similarly, no differences were observed when stratified by sex: female participants (WLPW% early 1.13% ± 0.05% vs. late 1.15% ± 0.08%, P = 0.801) and male participants (WLPW% early 1.29% ± 0.10% vs. late 1.07% ± 0.14%, P = 0.200).
No significant differences were observed across age groups: ≤34 years (WLPW% early 1.26% ± 0.15% vs. late 1.42% ± 0.27%, P = 0.606), 35–44 years (WLPW% early 1.36% ± 0.07% vs. late 1.19% ± 0.11%, P = 0.218), 45–54 years (WLPW% early 1.13% ± 0.11% vs. late 1.02% ± 0.12%, P = 0.481), 55–64 years (WLPW% early 0.94% ± 0.08% vs. late 1.16% ± 0.18%, P = 0.274), and ≥ 65 years (WLPW% early 1.24% ± 0.18% vs. late 0.88% ± 0.19%, P = 0.176).
Cross-sectional engagement analysis: Low versus high engagement
Among 1147 participants with weight data at 180 days, mean TBWL% was 5.91% ± 0.25% in the high engagement group (TMAPD > 1.02) compared with 4.38% ± 0.28% in the low engagement group (TMAPD < 1.02) (P < 0.001) (Table 3). When stratified by baseline obesity class, higher engagement was associated with greater weight loss across all groups: Obesity Class I (TBWL% low 4.22% ± 0.38% vs. high 5.31% ± 0.33%, P = 0.002), Obesity Class II (TBWL% low 4.65% ± 0.51% vs. high 6.52% ± 0.50%, P = 0.015), and Obesity Class III (TBWL% low 4.44% ± 0.74% vs. high 7.09% ± 0.60%, P = 0.010).
Total Body Weight Loss (%) across High and Low Engagement in 180 Days on the Signos System
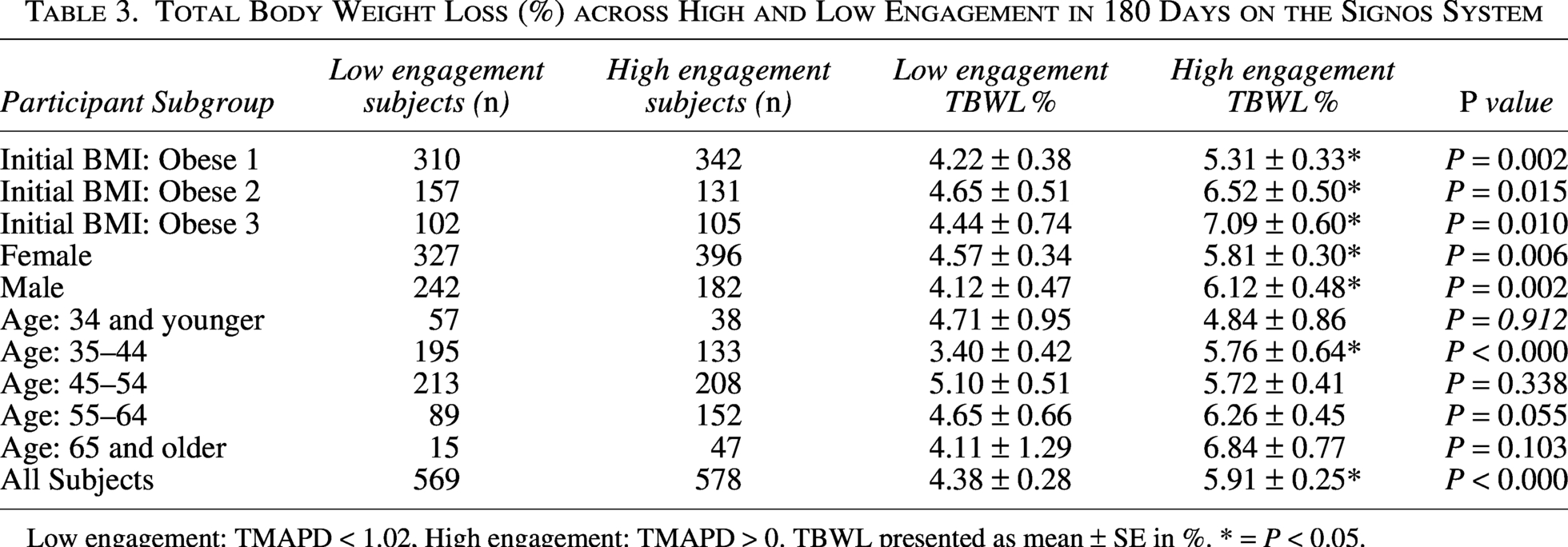
Low engagement: TMAPD < 1.02, High engagement: TMAPD > 0. TBWL presented as mean ± SE in %. * = P < 0.05.
Similarly, greater weight loss with higher engagement was observed across sex: female participants (TBWL% low 4.57% ± 0.34% vs. high 5.81% ± 0.30%, P = 0.006) and male participants (TBWL% low 4.12% ± 0.47% vs. high 6.12% ± 0.48%, P = 0.002).
Across age groups, differences in TBWL% by engagement varied: ≤34 years (TBWL% low 4.71% ± 0.95% vs high 4.84% ± 0.86%, P = 0.912), 35–44 years (TBWL% low 3.40% ± 0.42% vs. high 5.76% ± 0.64%, P < 0.001), 45–54 years (TBWL% low 5.10% ± 0.51% vs. high 5.72% ± 0.41%, P = 0.338), 55–64 years (TBWL% low 4.65% ± 0.66% vs. high 6.26% ± 0.45%, P = 0.055), and ≥65 years (TBWL% low 4.11% ± 1.29% vs. high 6.84% ± 0.77%, P = 0.103).
Cross-sectional engagement analysis: Behavioral outcomes
When stratified by engagement level at 180 days, behavioral measures differed between groups (Table 4). Mean exercise duration was greater in the high engagement group compared with the low engagement group (164.96 ± 5.64 vs. 131.03 ± 7.28 min per week, P < 0.001), as was mean exercise energy expenditure (880.68 ± 35.85 vs. 780.88 ± 52.70 kcal per week, P = 0.001) and meal logging frequency (10.48 ± 0.26 vs. 2.39 ± 0.12 logs per week, P < 0.001). A positive correlation was observed between engagement (TMAPD) and TBWL% at 180 days (r = 0.179, P < 0.001) (Fig. 2).
Behavioral Changes (Exercise and Meal Recording) during High and Low Engagement across 180-Days on the Signos System

Low engagement: TMAPD < 1.02, High engagement: TMAPD > 0. * = P < 0.05.
Discussion
The Signos System is an integrated digital platform that combines CGM data with an AI-powered mobile application to support personalized behavioral modification. In this retrospective cohort of adults with obesity without diabetes, engagement within the Signos System was associated with greater weekly weight loss. Early or late engagement was associated with similar weight loss outcomes. Participants with higher engagement achieved 5.90% TBWL at 6 months compared with 4.38% in lower engagement users.
A key finding is the consistent difference between periods of engagement and nonengagement. Greater weight loss during engagement suggests that active interaction with real-time, personalized feedback may play a central role in driving behavior change. This aligns with emerging evidence suggesting that CGM may facilitate behavior change by providing immediate physiological feedback that reinforces or discourages specific lifestyle choices.13,27 At the same time, the presence of modest weight loss during nonengaged periods indicates that initial exposure to CGM data and platform insights may initiate behavioral shifts, with continued engagement amplifying these effects over time. Recent interventional studies in individuals with obesity without diabetes have begun to explore CGM as a behavioral tool, suggesting potential benefits for adherence and lifestyle modification.22,27 This pattern supports the idea that engagement is not only a marker of use, but a mechanism through which digital interventions exert their impact.
The longitudinal within-subject analysis demonstrated that weight loss was consistently greater during periods of engagement compared with periods of nonengagement across all obesity classes, sexes, and age groups. Notably, weight loss during engagement approached approximately 1% of body weight per week, consistent with widely recommended guidelines for sustainable weight loss and preservation of lean mass.16,18,28–31
In contrast to prior digital health literature,14,25,32 the timing of engagement with the Signos did not appear to be a primary determinant of success. Participants who increased engagement later in their platform achieved comparable outcomes to those who engaged earlier. Because the within-subject design compared each participant against themselves, this finding is unlikely to be explained by differences in baseline motivation alone. This finding suggests that, unlike more static interventions, the effectiveness of the Signos System may not depend on early adherence, but rather on the ability to engage with dynamic, real-time feedback at any point. This flexibility may lower the barrier to re-engagement and support more sustained use over time.
At 6 months, weight loss among highly engaged participants exceeded the commonly cited 5% threshold for clinical significance and was at the upper range of outcomes reported for digital and automated weight loss interventions.26,33–38 Further, low technology, self-monitoring approaches alone, such as daily self-weighing or dietary food logging, have generally produced modest reductions in the range of 1%–2% of body weight over comparable durations.39,40 Pharmacotherapy with GLP-1 receptor agonists has been associated with substantially greater absolute weight loss, though real-world outcomes are typically lower. Real-world weight loss with GLP-1 receptor agonists varies substantially based on adherence and persistence. In studies of adults with obesity, mean weight loss has ranged from approximately 3%–6% over a 12-month period in cohorts that include early discontinuers to approximately 9%–12% in patients who maintain continuous therapy through 12 months.41–43 Achieving these outcomes depends on dosage, formulation, and sustained medication use over the full 12-month period. Further, GLP-1 receptor agonists are associated with cost, access, and tolerability considerations. Behavioral interventions such as those reported here may serve as an alternative or complementary approach. These findings extend prior work in digital health by suggesting that integrating physiological data streams, such as CGM, with AI-driven recommendations may enhance the effectiveness of behavioral interventions compared with passive tracking or static feedback approaches.
Taken together, these findings suggest that the effectiveness of the Signos System may be driven by its ability to deliver continuous, personalized, and physiologically informed feedback. By shifting from retrospective tracking to a real-time, closed-loop model, the platform may better support in-the-moment decision-making and reinforce behavior change as it occurs.
These results should be interpreted in the context of several limitations. The retrospective design limits causal inference, and residual confounding from time-varying factors such as fluctuating motivation or external life events cannot be excluded. A major limitation is that the cross-sectional 180-day analysis was limited to the 38.1% of analytic-cohort participants with a self-recorded weight and behavioral data in the day 175–185 window, which may introduce selection bias; lack of systematic medication tracking is an additional limitation. Future prospective studies are needed to further evaluate the causal relationship between engagement and weight loss and to assess long-term outcomes.
In summary, higher engagement with a CGM-integrated, AI-driven platform was associated with greater weight loss, with clinically meaningful reductions observed across the cohort. The findings suggest that real-time, adaptive digital interventions may represent a promising and scalable approach to weight management.
Authors’ Contributions
W.D., D.L., and S.K. conceived the study. D.L. and G.E.S. performed data analysis. W.D., G.E.S. and D.L. drafted the article. J.S.S. revised the article and contributed intellectually. All authors contributed to interpretation of data, reviewed the article, and approved the final version.
Footnotes
Data Availability
The data that support the findings of this study are not publicly available but may be available from the authors upon reasonable request.
Author Disclosure Statement
G.E.S., D.L., D.G., and S.F.-M. are employees of Signos. J.S.S. reports [consulting].
Funding Information
This study received no external funding.