
Abstract
Aims:
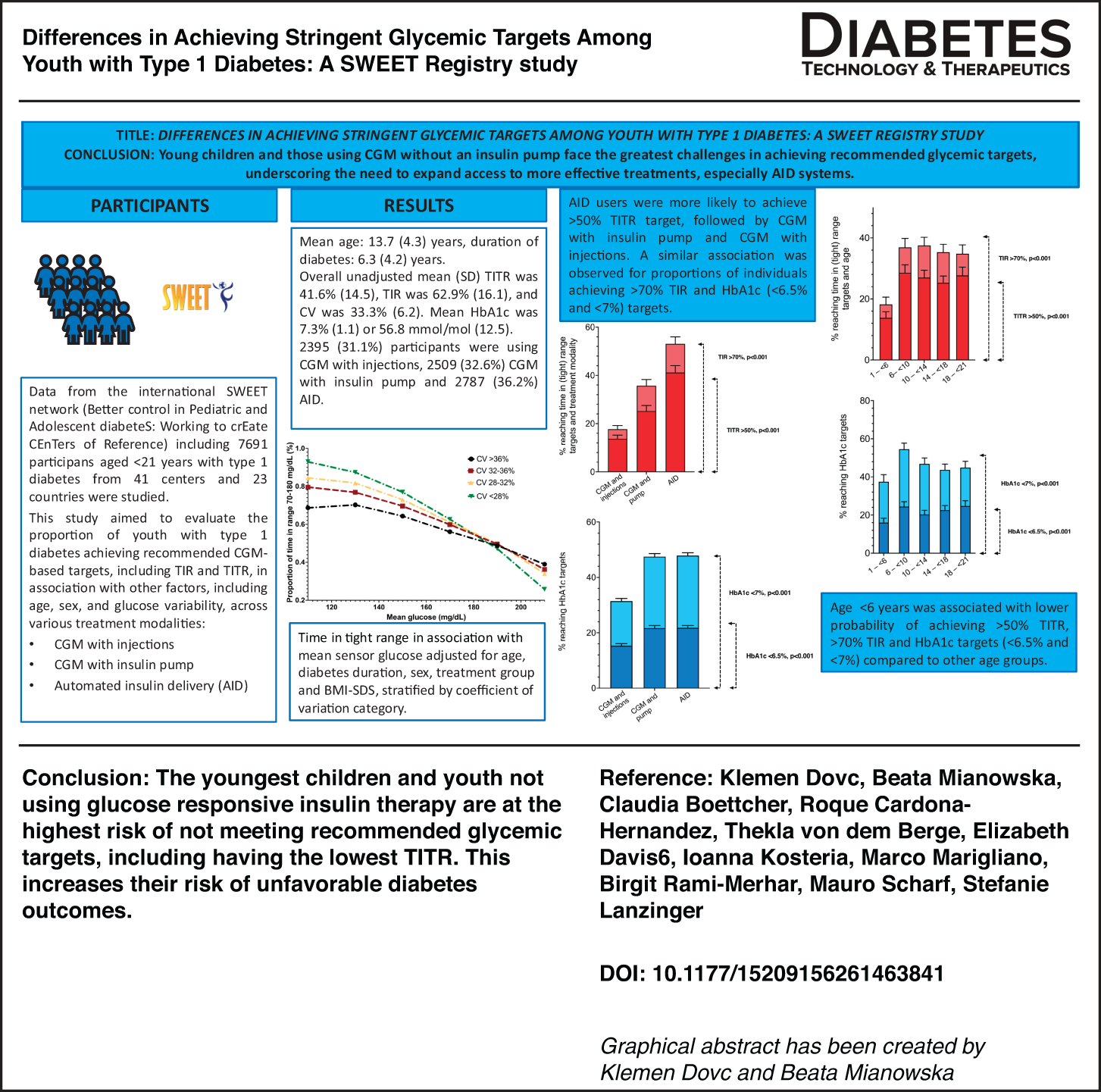
This study aimed to investigate the associations between glycemic outcomes and a range of clinical and demographic factors, including treatment modality, sex, age, diabetes duration, and body mass index, in youth with type 1 diabetes in an international registry.
Methods:
This observational, cross-sectional cohort study included youth <21 years from 23 countries. Proportions of individuals using different treatment modalities (continuous glucose monitoring [CGM] with injections, CGM with pump, automated insulin delivery [AID]) and achieving recommended time in tight range (TITR >50%), time in range (TIR >70%), and glycated hemoglobin (HbA1c) (≤6.5% [48 mmol/mol] and ≤7% [53 mmol/mol]) were assessed using mixed-effects fractional logistic and linear regression models. Sex, age (categorized), diabetes duration (categorized), body mass index standard deviation score (categorized), and treatment modality were included as covariates.
Results:
Data of 7691 individuals (mean [standard deviation] age of 13.7 [4.3] years, diabetes duration 6.3 [4.2] years, 47.8% female) were included. AID users were the most likely to achieve TITR target (adjusted mean [standard error of the mean] 41.2% [2.9]), followed by CGM with insulin pump (25.2% [2.3]) and CGM with injections (13.7% [1.5], P < 0.001). A similar association was observed for proportions of individuals achieving TIR and HbA1c targets (P < 0.001). Age <6 years was associated with a higher coefficient of variation (CV) (P < 0.001) and a lower probability of achieving both TITR and TIR targets compared with other age groups (P < 0.001). In analyses of TITR associated with mean sensor glucose stratified by CV, a higher TITR for a lower CV was observed only at mean glucose levels below 150–160 mg/dL; above this threshold, the pattern reversed, with lower CV associated with lower TITR at a given mean glucose level.
Conclusions:
Children younger than 6 years and individuals not using glucose-responsive insulin therapy were less likely to meet the recommended glycemic targets. It is imperative to minimize these disadvantages.
Introduction
Maintaining glucose levels as close to normal as possible throughout lifelong insulin replacement therapy is a cornerstone in managing type 1 diabetes and is fundamental for the prevention or delay of long-term complications. Consequently, glycemic targets have been optimized in recent years and current International Society for Pediatric and Adolescent Diabetes guidelines recommend targeting a glycated hemoglobin (HbA1c) of ≤6.5% (48 mmol/mol) for all children and adolescents with diabetes, provided that adequate technology and health care professional support are available, when these targets can be safely achieved without increasing the risk of hypoglycemia or adding to the care burdens. 1 A key continuous glucose monitoring (CGM)-derived metric used to monitor glycemic outcomes is time in range (TIR), defined as the percentage of time glucose levels are between 70 and 180 mg/dL (3.9–10 mmol/L) with the target set as >70%. 2 A newer metric, time in tight range (TITR; 70–140 mg/dL or 3.9–7.8 mmol/L), has been proposed to better reflect glucose levels within normoglycemia. 3 Moreover, TITR is recognized as particularly valuable when aiming for lower HbA1c targets, as it is more sensitive to changes at lower mean glucose levels. 4
Achieving recommended glycemic targets poses a significant everyday challenge and a burden, particularly for children diagnosed who are younger than 6 years. 5 Onset of type 1 diabetes at a young age may expose individuals to prolonged periods of hyperglycemia and high glycemic variability, significantly increasing the risk of early onset of chronic complications, including adverse effects on brain structure and neurodevelopment.6–9 However, by endorsing TITR as a metric in preschool children with type 1 diabetes together with lower treatment targets, TITR proved to be both beneficial and feasible when aiming for better glycemic outcomes. For instance, in Sweden, pediatric diabetes teams began targeting TITR decades ago, and registry data show that more than 50% of children younger than 7 years now achieve TITR >50%.10,11
CGM is now recommended as a global standard of care that provides real-time access to glucose levels and enables timely adjustments in insulin dosing. This allows for more precise glycemic management and improved outcomes.12,13 The uptake of CGM has increased in the past decade, and substantial evidence now supports the efficacy and effectiveness of CGM in individuals with type 1 diabetes regardless of their age.14–17 Registry data and longitudinal studies also indicate that early adoption of CGM following diagnosis can improve glycemic outcomes and reduce acute complications.18–22 There are two insulin delivery modalities: multiple daily injections or insulin pump therapy, both of which can be used with or without CGM. Automated insulin delivery (AID) is the most advanced insulin delivery option that enables constant automatic adjustment of insulin delivery by an insulin pump in response to variations in glucose levels as measured by CGM levels and is currently recommended as a treatment modality of choice for children and adolescents with type 1 diabetes. 23 The glycemic efficacy and effectiveness of different AID systems are described in numerous randomized clinical trials and real-world studies, demonstrating the potential to optimize glycemic management, improve quality of life, and reduce the burden of type 1 diabetes, thereby leading to their broader adoption.24–27
This study aimed to evaluate the proportion of youth with type 1 diabetes using CGM who are achieving recommended glycemic targets, including TIR and TITR, with adjustment for available clinical and demographic factors, in a large international registry, encompassing a diverse cohort of children, adolescents, and young adults with type 1 diabetes.
Research Design and Methods
Study design and population
The international SWEET network (Better control in Pediatric and Adolescent diabeteS: Working to crEate CEnTers of Reference) is a global collaboration of centers specializing in the care of children, adolescents, and young adults with diabetes, with a mission to enhance clinical outcomes, standardize diabetes care, and develop best practices for pediatric diabetes management. 28 The centers participating in the SWEET registry biannually share a set of standardized data, validated for credibility, to the Institute of Epidemiology and Medical Biometry, Ulm University, in Ulm, Germany. This study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines, and all participating centers complied with current data protection regulations and ethical standards based on national regulations in the respective countries. As of December 2024, the SWEET database contained information on 128,332 participants from 126 centers worldwide. In this observational, cross-sectional multinational cohort study, data from children, adolescents, and young adults younger than 21 years with type 1 diabetes duration of at least 6 months who were using CGM and had at least 10 consecutive days of valid raw sensor data were included. Demographic data included age, sex, age at diabetes onset and diabetes duration, total daily insulin dose per kilogram of body weight, type of insulin administration (i.e., treatment modality), and HbA1c. CGM, demographic, and clinical data were collected between January 1, 2020, and December 31, 2024, and the most recent treatment year per person was aggregated for the analysis. Treatment modalities were categorized as CGM with injections, CGM with insulin pump (including predictive low-glucose suspend function), and AID. HbA1c was standardized to the Diabetes Control and Complications Trial reference of 20–42 mmol/mol (4%–6%). CGM-derived coefficient of variation (CV) was categorized as <28%, 28% to <32%, 32% to <36%, and ≥36%. Age was categorized as <6 years, 6 to <10 years, 10 to <14 years, 14 to <18 years, and ≥18 years. Diabetes duration was divided into <2 years, 2 to <5 years, 5 to <10 years, and ≥10 years. Body mass index standard deviation score (BMI–SDS) was derived from the World Health Organization growth curves. 29 BMI–SDS was categorized as underweight (–<−2), normal weight (–2 to ≤1), overweight (>1 to ≤2), and obese (>2). 29
Outcomes and measures
Glycemic variables included CGM metrics calculated from the available CGM profiles (TIR, TITR, time below range [TBR; below 70 mg/dL], time above range [TAR; above 180 mg/dL], above 250 mg/dL [TAR2], mean sensor glucose [mg/dL], and CV [%]) and HbA1c. Proportions of individuals achieving recommended glycemic targets (>50% TITR, >70% TIR) and HbA1c targets (≤6.5% [≤48 mmol/mol] and ≤7% [≤53 mmol/mol]) for the different treatment modalities were calculated and subsequently associated with collected variables.
Statistical analyses
Continuous outcomes were presented as mean (standard deviation [SD]) or median (interquartile range [IQR]) and binary outcomes as percentages. The proportion of individuals achieving recommended targets of TIR, TITR, and HbA1c was analyzed using multivariable mixed-effects logistic regression models. Mixed-effects fractional logistic and linear regression models were used to study CGM metrics. A random intercept for center was included in each model. Sex, age (categorized), diabetes duration (categorized), BMI–SDS (categorized), and treatment modality were included as covariates. Relationships between mean sensor glucose and TIR and TITR for different CV categories were presented in graphs.
Statistical analyses were conducted using SAS version 9.4 (SAS Institute Inc., Cary, NC), and a two-sided P value of <0.05 was considered statistically significant.
Results
Participant characteristics
We included 7691 eligible individuals (47.8% female) with type 1 diabetes from 41 participating centers and 23 countries (Supplementary Material: List of SWEET centers participating in the study and Supplementary Fig. S1— shows the study flowchart). Mean age (SD) was 13.7 (4.3) years, and duration of diabetes was 6.3 (4.2) years. The mean time difference between CGM measurements and clinical data such as HbA1c was 42 days, and the median was 0 days. On average, participants had 247 days (IQR: 103–358) of CGM data available for this study. Overall unadjusted mean (SD) TITR was 41.6% (14.5), TIR was 62.9% (16.1), and CV was 33.3% (6.2). Mean HbA1c was 7.3% (1.1) or 56.8 mmol/mol (12.5).
Demographic data, clinical characteristics, and unadjusted CGM-based metrics, overall and stratified by treatment modality, are listed in Supplementary Table S1. The distribution of treatment modalities was as follows: 2395 (31.1%) participants were using CGM with injections, 2509 (32.6%) were using CGM with an insulin pump, and 2787 (36.2%) were using AID. The proportion of AID users increased from 22.2% in young adults ≥18 years to 33% in older teenagers 14 to <18 years, to 38.2% in very young children (<6 years), to 42.6% in 10 to <14 years, and was highest at 46.3% in the 6 to <10-year-old age group (Supplementary Table S2).
Adjusted regression results
The results of logistic regression, fractional logistic, and linear regression analyses are shown in Tables 1 and 2 and Figures 1 and 2. Adjusted for sex, age, diabetes duration, and BMI–SDS, treatment modality was significantly associated with the proportion of persons achieving recommended TITR, TIR, and both HbA1c (≤6.5% [≤48 mmol/mol] and ≤7% [≤53 mmol/mol]) glycemic targets (P < 0.001 for all four comparisons). AID use was the modality most likely to achieve greater than 50% TITR (adjusted mean [standard error of the mean] was 41.2% [2.9] users), followed by CGM with insulin pump (25.2% [2.3] users) and CGM with injections (13.7% [1.5] users, P < 0.001). A similar association was observed for proportions of individuals achieving TIR greater than 70% and HbA1c lower than 6.5% (48 mmol/mol) or lower than 7% (53 mmol/mol) (P < 0.001 for all three comparisons; Table 1 and Fig. 1).
Proportions of Youths with Type 1 Diabetes Reaching Recommended Targets in Association with Treatment Modality, Sex, Age, Diabetes Duration, and Body Mass Index–Standard Deviation Score
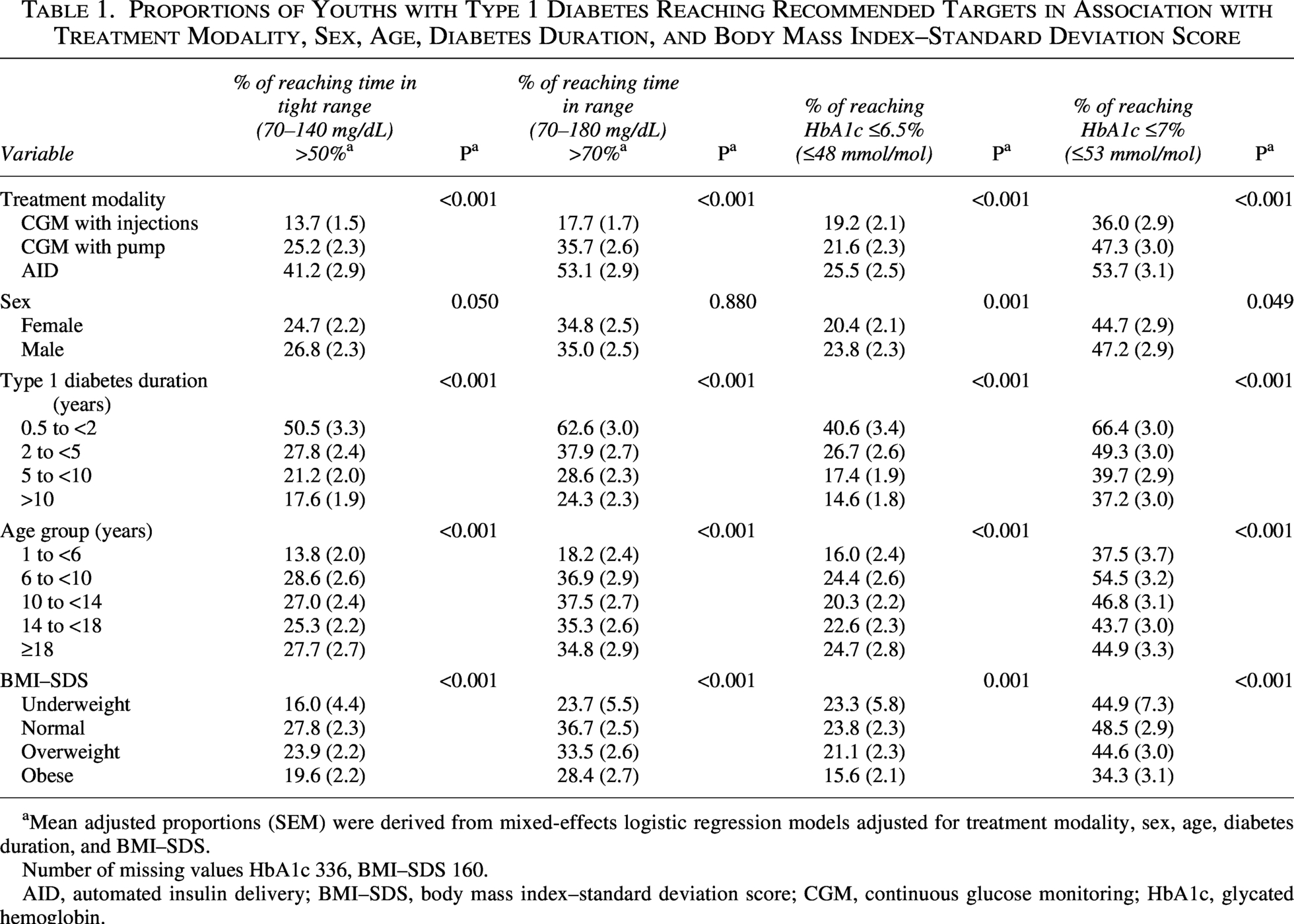
Mean adjusted proportions (SEM) were derived from mixed-effects logistic regression models adjusted for treatment modality, sex, age, diabetes duration, and BMI–SDS.
Number of missing values HbA1c 336, BMI–SDS 160.
AID, automated insulin delivery; BMI–SDS, body mass index–standard deviation score; CGM, continuous glucose monitoring; HbA1c, glycated hemoglobin.
Time in Range, Time in Tight Range, and Coefficient of Variation in Association with Treatment Modality, Sex, Age, Diabetes Duration, and Body Mass Index–Standard Deviation Score
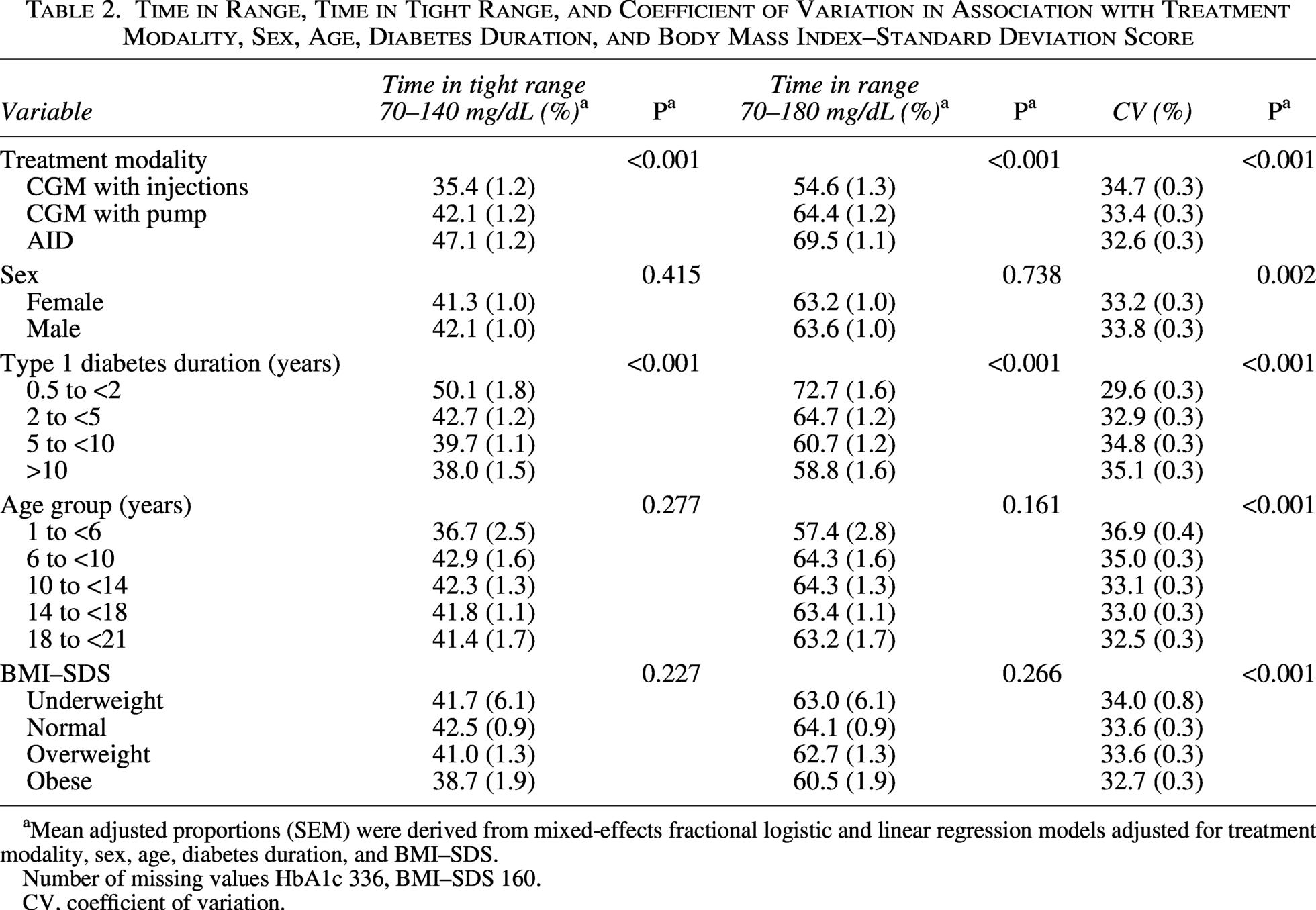
Mean adjusted proportions (SEM) were derived from mixed-effects fractional logistic and linear regression models adjusted for treatment modality, sex, age, diabetes duration, and BMI–SDS.
Number of missing values HbA1c 336, BMI–SDS 160.
CV, coefficient of variation.
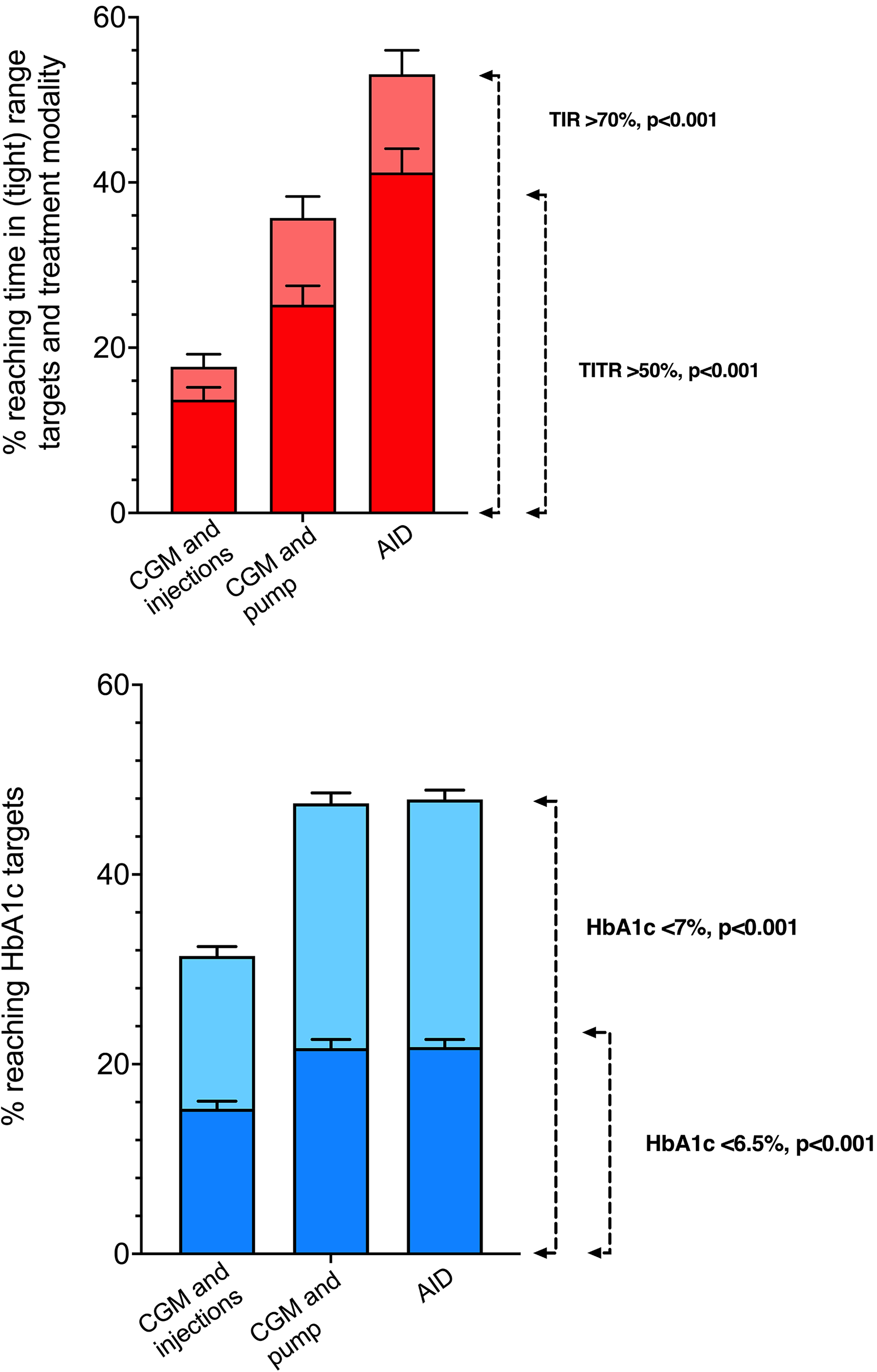
Proportions of individuals reaching recommended glycemic targets in association with different treatment modalities: Upper panel—proportions of individuals reaching >50% time in tight range 70–140 mg/dL, TITR (dark red) and >70% time in range 70–180 mg/dL, TIR (light red). Lower panel: Proportions of individuals reaching glycated hemoglobin (HbA1c) ≤6.5% (≤48 mmol/mol) (dark blue) and ≤7% (≤53 mmol/mol) (light blue). Mean adjusted proportions (SEM) were derived from fractional logistic and linear regression models adjusted for treatment modality, sex, age, diabetes duration, and body mass index–standard deviation score, stratified by treatment modality. AID, automated insulin delivery; CGM, continuous glucose monitoring; SEM, standard error of the mean.
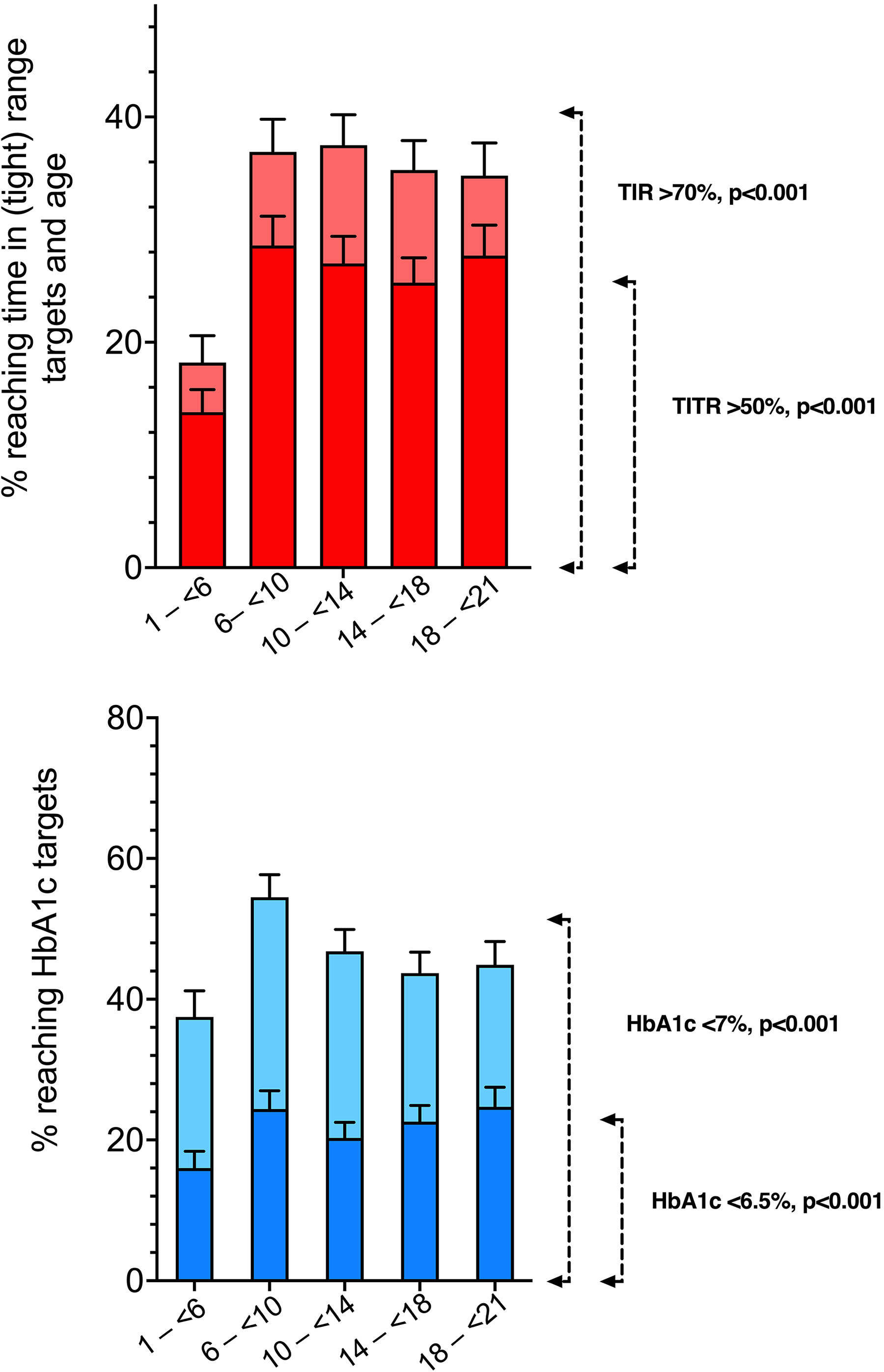
Proportions of individuals reaching recommended glycemic targets in association with different age groups: Upper panel—proportions of individuals reaching >50% time in tight range 70–140 mg/dL, TITR (dark red) and >70% time in range 70–180 mg/dL, TIR (light red). Lower panel: Proportions of individuals reaching HbA1c ≤6.5% (≤48 mmol/mol) (dark blue) and ≤7% (≤53 mmol/mol) (light blue). Mean adjusted proportions (SEM) were derived from fractional logistic and linear regression models adjusted for treatment modality, sex, age, diabetes duration, and body mass index–standard deviation score, stratified by age groups.
Age group, diabetes duration group, and BMI–SDS category were also associated with achieving >50% TITR and >70% TIR targets (Table 1). Younger age (<6 years) was associated with a lower probability of achieving >50% TITR (1.38% [2.0]) or >70% TIR (18.2% [2.4]) compared with all other age groups (P < 0.001 for both comparisons, Table 1). In addition, younger age was associated with higher CV values (P < 0.001), while there were no age-related differences in other glycemic outcomes (Table 2). Similarly, a longer duration of type 1 diabetes was associated with a lower probability of reaching >50% TITR, >70% TIR, ≤6.5% (≤48 mmol/mol) HbA1c, and ≤7% (≤53 mmol/mol) HbA1c (P < 0.001 for all four comparisons, Table 1). Normal weight and overweight BMI–SDS were associated with a higher probability of achieving the recommended TITR, TIR (both P < 0001), and HbA1c targets (P = 0.001 for <6.5% and P < 0.001 for <7.0%) compared with both underweight and obese.
Likewise, treatment modality was strongly associated with other glycemic outcomes (Table 2, Supplementary Table S3). The highest adjusted TITR and TIR were observed among AID users (TITR 47.1% [1.2] and TIR 69.5% [1.1]), followed by CGM with insulin pump (42.1% [1.2] and 64.4% [1.2]) and CGM with injections (35.4% [1.2] and 54.6% [1.3], respectively, P < 0.001 for all comparisons) (Table 2).
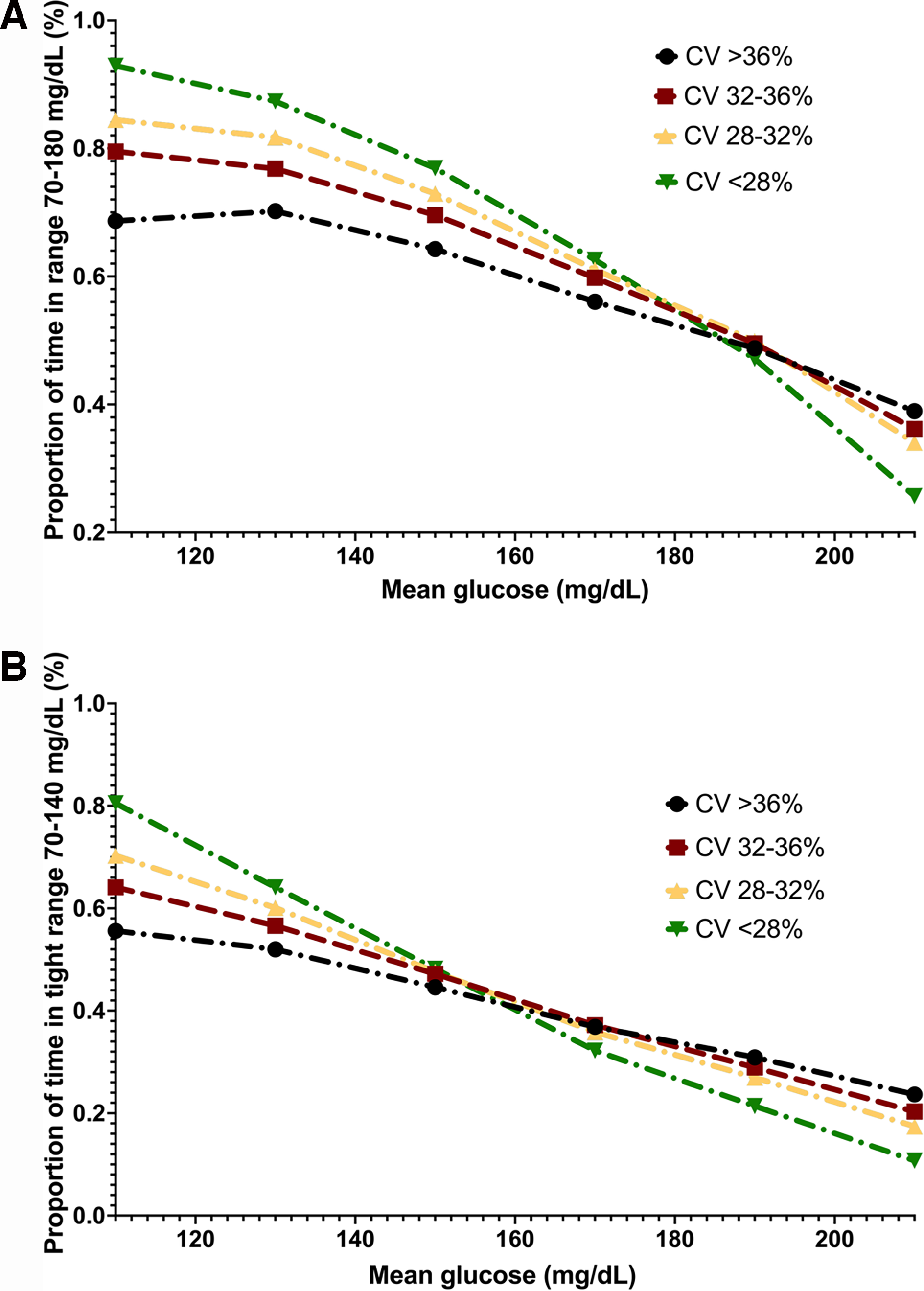
Relationship between TITR, TIR, mean glucose, and CV
Figure 3A and B presents the relationship between TITR or TIR and mean sensor glucose for individuals categorized by different CV percentages. Higher TITR for lower CV categories was only demonstrated for mean glucose values below 150–160 mg/dL, that is, TITR was the highest for the lowest CV category for any chosen mean glucose value within this range. Conversely, when the mean glucose value exceeded 150–160 mg/dL, a lower CV category represented lower TITR for a chosen mean glucose value (Fig. 3B). Similarly, for a mean glucose level below approximately 190 mg/dL, there was an inverse relationship between TIR and CV, with the highest TIR in the lowest CV category, and in contrast, the lowest TIR in the lowest CV category was observed above a mean glucose of 190 mg/dL (Fig. 3A).
Time in range
Discussion
In this multicenter, international study of youth with type 1 diabetes, factors associated with glycemic outcomes have been investigated. While several factors are unmodifiable, treatment modality constitutes the principal modifiable component of diabetes care, thereby representing a critical opportunity for intervention and improvement.
The use of AID was associated with the highest proportion of participants reaching the recommended glycemic targets. Notably, differences were greatest for the TITR >50% target and for the TIR >70% target, with nearly half the AID users meeting these goals—an approximately 10% difference compared with other treatment modalities. In addition, AID use was associated with higher TITR and TIR, as well as lower TAR >180 mg/dL, TAR >250 mg/dL, and CV, while differences in TBR were less pronounced. The overall unadjusted mean TIR of the study cohort was 62.9%, which is higher than previously reported values in the SWEET database (59.3%) and was getting closer to the recommended clinical target of 70%. 30
Although previous studies have evaluated glycemic outcomes associated with different treatment modalities,5,9 few have focused on CGM-based metrics, particularly TITR targets.30–33 In a recent two-center study from Italy, Passanisi et al. reported data from 854 youth with type 1 diabetes. AID use was associated with a higher average TITR (45%), and 34.3% of AID users achieved TITR >50%, compared with less than 20% in all other treatment groups. 32 Similarly, a single-center study from Denmark involving children and adults with type 1 diabetes reported higher TIR values and greater odds of achieving TIR >70% target with AID use. However, TITR targets were not assessed. 33
In our study, preschoolers with type 1 diabetes were less likely to meet the recommended glycemic targets than school-aged children. Only a minority of preschoolers achieved TITR >50% and TIR >70% targets, respectively, less than half the proportion of older children.
Managing type 1 diabetes in preschoolers presents unique challenges: Young children rely entirely on caregivers, have very high insulin sensitivity, unpredictable eating and activity patterns, and often cannot recognize or communicate hypoglycemic symptoms. This leads to substantial day-to-day variability in insulin needs. 34 Consequently, early-onset diabetes with possible long-term dysglycemia increases the risk of premature complications. 35 Early glycemic optimization is therefore critical in this vulnerable group. However, this might be challenging to overcome without glucose-responsive insulin delivery. Current international guidelines support AID as a treatment modality of choice for all adults and children, including preschoolers, living with diabetes. 23 This recommendation is supported by clinical trials demonstrating the safety and efficacy of AID use in young children.24,27,36,37 While AID systems are increasingly available to children with type 1 diabetes in many countries, significant inequities remain in their adoption across age groups. 5 A recent SWEET study of 42,349 children with type 1 diabetes demonstrated that universal access to and reimbursement for advanced diabetes technologies and insulin are significantly associated with lower HbA1c levels, highlighting the need to improve equitable access worldwide to enhance glycemic outcomes. 38
At the time these data were collected, preschoolers had reduced access to AID, as limited systems were approved for use in this age group. In our study, close to half of the children aged 6 to <10 or 10 to <14 years used AID, whereas roughly only one in three preschoolers (<6 years) and adolescents (>14 years) benefited from these systems. For the >14-year-old group, the reason for a relatively low AID uptake may be that they have already been previous non-AID pump users, and their pump guaranties had not expired yet (which does not permit them to get a newer system), or simply, despite being encouraged, some teenagers were hesitant to use pumps. The same, together with less favorable reimbursement strategies for adults in some countries, may apply to participants aged >18–21, whose AID uptake was only one in five. Our results indicate that individuals with BMI–SDS closer to the normal range were more likely to achieve the recommended glycemic targets than those who were either underweight or obese. This finding suggests that both extremes of the BMI spectrum may be associated with challenges in optimizing glycemic outcomes, potentially reflecting differences in insulin sensitivity and nutritional status.
When the changing insulin requirements are not appropriately addressed, it can result in more glycemic variability that limits the achievement of recommended glycemic targets. In participants with lower glycemic variability, there is an association with greater achievement of glycemic targets. Where possible, attempts to reduce variability should be considered by clinicians. Our results showed that preschoolers had a CV of 36.7%, roughly 2% higher than the other age groups, whose CVs ranged from 32.8% to 34.7%. In contrast, AID use was associated with a lower CV than other treatment modalities (33.1%–34.3%).
Although recommended glycemic outcomes involve high TIR or TITR together with low CV, real-world data in adults suggest that this relationship holds only when mean glucose levels remain below specific thresholds: <180 mg/dL for TIR and <140 mg/dL for TITR.1,38,39 Above these thresholds, a lower CV may correlate with lower TIR and TITR as individuals continuously have elevated glucose. This phenomenon is most apparent in adults with type 1 diabetes and, to a lesser extent, in those with type 2 diabetes.38,39 Our analysis of the relationship between mean glucose and TIR or TITR stratified by CV levels revealed slightly distinct patterns with respect to that specific mean glucose thresholds. In our study, including children and young adults with type 1 diabetes, a gradual decline in TIR and TITR despite the lower CV was observed only when mean sensor glucose surpassed 190 mg/dL for TIR and 150–160 mg/dL for TITR. Although the mean glucose values at which the favorable relationship between higher TIR, TITR, and lower CV is lost are slightly higher than in adults, our findings still suggest that, also in children and young adults, TITR represents a valuable, physiologically relevant target metric—particularly for individuals exhibiting very high TIR and near-normal mean glucose levels (up to 150–160 mg/L), such as users of AID systems, individuals in early stages (stage 1 or 2) of type 1 diabetes, or those experiencing partial remission.4,40,41
Limitations of our study should be considered, primarily those related to its observational, cross-sectional design utilizing data from a prospective, global, however, not population-based registry. This design limits our ability to determine causal relationships between glycemic outcomes and the modifiable and unmodifiable factors assessed.
In addition, the SWEET database does not collect race, ethnicity, or socioeconomic status information, as it is an international registry comprising heterogeneous countries and regions. These factors, along with center-level differences in technology adoption and availability of specialized diabetes care staff, may influence glycemic outcomes and could not be fully accounted for in this analysis.
Strengths of this study include the use of CGM-based glycemic metrics in addition to HbA1c, the inclusion of different treatment modalities, and global representation. Data were collected from 23 countries within the SWEET registry, which includes standardized data under a quality control process to ensure reliability.
Conclusions
In this study where CGM use was an inclusion criterion, the youngest children and youth not using glucose-responsive insulin therapy are at the highest risk of not meeting recommended glycemic targets, including having the lowest TITR. This increases their risk of unfavorable diabetes outcomes. It is therefore crucial to prioritize advocacy efforts that improve access to, and promote the wider use of, treatment options that offer better and safer glycemic control, particularly AID.
Authors’ Contributions
K.D., B.M., T.v.d.B., and S.L. designed the study, participated in data interpretation, and wrote the article. S.L. designed the study, performed the statistical analysis, participated in data interpretation, and reviewed and edited the article. C.B. and R.C.-H. researched the data, participated in data interpretation, and reviewed and edited the article. K.D., B.M., S.L., C.B., R.C.-H., T.v.d.B., E.D., I.K., M.M., B.R.-M., and M.S. substantially contributed to acquisition of data for the work and revised the work critically for important intellectual content. All authors approved the final version of the article. K.D., B.M., and S.L. are the guarantors of this work, had full access to all the data in the study, and take responsibility for the integrity of the data and the accuracy of the data analysis.
Supplemental Material
sj-docx-1-dtt-10.1177_15209156261463841 — Supplemental material for Differences in Achieving Stringent Glycemic Targets Among Youth with Type 1 Diabetes: A SWEET Registry Study
Supplemental material, sj-docx-1-dtt-10.1177_15209156261463841 for Differences in Achieving Stringent Glycemic Targets Among Youth with Type 1 Diabetes: A SWEET Registry Study by Klemen Dovc, Beata Mianowska, Claudia Boettcher, Roque Cardona-Hernandez, Thekla von dem Berge, Elizabeth Davis, Ioanna Kosteria, Marco Marigliano, Birgit Rami-Merhar, Mauro Scharf, and Stefanie Lanzinger
Footnotes
Acknowledgments
There was no commercial sponsor for this study. The authors thank the following individuals for their support to this study: Eva Hauser for data management, as well as Andreas Hungele and Ramona Ranz for the SWEET-DPV software (all Ulm University, Germany), Michael Witsch (Centre Hospitalier de Luxembourg, Luxembourg) for center integration, Thomas Danne and Olga Kordonouri (Kinder– und Jugendkrankenhaus AUF DER BULT, Hannover, Germany) for initiating the SWEET collaboration, Katharina Klee (Kinder– und Jugendkrankenhaus AUF DER BULT, Hannover, Germany), and Ananta Addala, Tadej Battelino, and Reinhard Holl for their invaluable support. Finally, the authors also thank all the participating centers of the SWEET network, especially the collaboration centers in this investigation (![]() ).
).
Ethical Considerations
This study adhered to the STROBE guidelines, and all participating SWEET centers complied with current data protection regulations and ethical standards based on national regulations in the respective countries.
Data Availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Authors’ Disclosure Statement
K.D. received honoraria for participation on the speaker’s bureau of Abbott, Dexcom, Medtronic, Novo Nordisk, and advisory board honoraria from Novo Nordisk and Medtronic. B.M. received honoraria for participation on the speaker’s bureau of Abbot, Dexcom, Ypsomed, Synoptis/Neuca, and advisory board honoraria from Medtronic. C.B. is a consultant for/has received honoraria from Novo Nordisk and Sanofi. R.C.-H. has received honoraria on the speaker’s bureau and/or advisory boards from Abbott, Dexcom, Lilly, Medtronic, Novo Nordisk, and Sanofi. E.D.’s organization received honoraria from Sanofi. I.K. received honoraria for participation on the speaker’s bureau of Abbott, Eli Lilly, Menarini, Novo Nordisk, and advisory board honoraria from Eli Lilly. M.M. received honoraria on the speaker’s bureau and/or advisory boards from Movi, Medtronic, Novo Nordisk, Theras, and Ypsomed. B.R.-M. received honoraria for participation on the speaker’s bureau of advisory boards from Eli Lilly, Medtronic, Insulet, Abbott, Sanofi, and Ypsomed. M.S. received honoraria on the speaker’s bureau and/or advisory boards and medical consultancy from Medtronic, Abbott, Novo Nordisk, Pfizer, Roche, and Cristalia. No other potential conflicts of interest relevant to this study were reported.
Funding Information
This work was supported by the SWEET corporate members, namely, Abbott, Boehringer Ingelheim, Dexcom, Insulet, Lilly, Medtronic, and Sanofi. The content is solely the responsibility of the authors and does not necessarily represent the official views of the corporate members. K.D. was supported in part by the
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.