
Abstract
This study aims to (a) provide updated prevalence estimates of family polyvictimization by synthesizing recent literature, (b) examine the effect sizes of how one type of family victimization impacts other types, and (c) investigate correlates of family polyvictimization. Literature databases were searched for publications from May 2018 onward. A total of 49 studies, producing 51 estimates, met the inclusion criteria and were included in this updated analysis, providing a substantial sample size of 543,196 for the general synthesis of effect sizes. Combined with a previous meta-analysis, 89 estimates were included to synthesize overall effect sizes and estimate associations among different types of family victimization and their correlates. Among the 51 new estimates, the event rate of family polyvictimization was 27.0%. When combined with the previous meta-analysis (18.3%), the overall event rate across 89 estimates decreases slightly to 23.1%. This updated meta-analysis includes more studies from continents such as Africa and South America, which consistently report higher rates of polyvictimization. Findings also show that the prevalence of family victimization co-occurrence is higher in clinical samples compared to the general population. The higher prevalence of family victimization co-occurrence in clinical samples highlights the increased likelihood of identifying a second victim in the same family once the first victim comes to the attention of health or social services. The overrepresentation of child polyvictimization and the co-occurrence of intimate partner violence and child abuse suggest that more members from extended families should be included in family violence studies.
Introduction
Family violence is a complex and pervasive issue, often involving multiple forms of victimization that co-occur within the same household. In our previous meta-analysis (Chan et al., 2021), we highlighted the significance of examining the co-occurrence of various types of family violence, reporting an overall event rate of 18.3%. Notably, co-occurrence rates were substantially higher in clinical populations (36.0%) compared to the general population (9.7%), underscoring the heightened vulnerability among families already engaged with protective or support services. Importantly, the identification of an initial victim increased the likelihood of uncovering additional victims within the same family by sixfold. These findings underscore the urgent need for early detection strategies to identify victims who might otherwise remain hidden, and they point to the importance of understanding family polyvictimization for the development of effective prevention and intervention efforts.
Despite these insights, our earlier review was limited by the small number of eligible studies, restricting our ability to explore sub-groups, moderators, and family-level risk factors associated with polyvictimization. Since then, the field has seen a notable increase in research on the co-occurrence of violence and polyvictimization, presenting a timely opportunity to update and expand upon previous findings.
A further challenge in advancing this field is the inconsistent use of terminology. While some researchers use “polyvictimization” to refer to multiple forms of victimization experienced by a single individual, our focus is on family polyvictimization—the experience of multiple types of victimization reported by different members within the same family (Chan, 2017; Chan et al., 2021). This distinction is critical, as family polyvictimization encompasses a broader range of victimization patterns, including but not limited to intimate partner violence (IPV), child abuse and neglect (CAN), elder abuse (EA), and in-law abuse (ILA), among others. Understanding family polyvictimization requires attention to both the diversity of victimization types and the relationships between victims and perpetrators within the family context.
The current definition of family polyvictimization emphasizes the presence of multiple victims within the same family, setting it apart from situations where a single individual experiences multiple forms of violence—such as repeat, recurrent, or multiple victimization, as well as child polyvictimization. Several studies define repeat or recurrent victimization as instances where a single victim reports experiencing repeated incidents of family violence (Davis et al., 2021; Goodlin & Dunn, 2010). Other research uses the term polyvictimization to refer to a single victim, whether a child or an adult woman, who has experienced multiple types of victimization or trauma, including physical, psychological, or sexual abuse, and neglect (Bridges-Curry & Newton, 2024; Burden & Roddy, 2024). While repeat or multiple victimization reflects the severity and complexity of an individual’s experiences, it does not necessarily indicate the involvement of additional victims, nor does it specify whether the perpetrators are family members.
There is an expanding body of research on child polyvictimization, frequently assessed using the Juvenile Victimization Questionnaire (JVQ; Finkelhor et al., 2007) or its revised version, the JVQ-R2 (Finkelhor et al., 2011). The JVQ captures multiple forms of victimization experienced by a child, often involving different perpetrators and occurring in various contexts. Beyond simply measuring, the prevalence and correlates of child polyvictimization, the JVQ can provide valuable insights into the involvement of multiple perpetrators, diverse contexts, and potentially even the presence of multiple victims within the same family. For example, it assesses experiences such as child maltreatment (including physical, psychological, and sexual abuse, as well as neglect by parents or family caretakers), sibling violence, witnessing domestic violence, and witnessing a parent assault a sibling. However, to date, no study has explicitly coded data according to the concept of family polyvictimization. Nevertheless, the use of the JVQ may indirectly capture cases involving multiple family victims, and such studies are included in this meta-analysis.
In this meta-analysis, family victimization is defined as the identification of multiple victims within a single family, which may include a child, an adult parent, or an elderly member. Depending on the specific perpetrator-victim relationships, these cases may be categorized as IPV, CAN, EA, ILA, and so forth. Understanding family polyvictimization is crucial for identifying which families are at risk of having multiple victims, whether harmed by one or several perpetrators. It is therefore important to focus on family-level risk factors, rather than solely individual-level ones, when studying family polyvictimization. In practice, recognizing the presence of one victim should prompt proactive screening for additional victims by health, social welfare, or criminal justice professionals. However, early identification of hidden victims of family violence remains a significant challenge.
Given the recent growth in research on child and family polyvictimization, there is a clear need to synthesize the latest evidence, update prevalence estimates, and examine the correlates and impact of different forms of family victimization. By updating our meta-analysis, we aim to advance the field by (a) providing updated prevalence estimates of family polyvictimization, (b) quantifying the effect sizes of associations between different types of family victimization, and (c) identifying key correlates and risk factors at the family level. This work will contribute to a more nuanced understanding of family violence and inform the development of more effective prevention and intervention strategies.
Method
Literature Search Strategy
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to present our findings. The studies included in this meta-analysis were identified through searches in databases such as the Applied Social Sciences Index and Abstracts, ERIC, MEDLINE, PsycINFO, Sociological Abstracts, and Social Service Abstracts. In line with the definition of family victimization as the identification of multiple victims within a single family—which may include a child, an adult parent, or an elderly member—the literature search was conducted using combinations of the following keywords: polyvictimization, multiple victimization; child abuse, child victim, child neglect, violence against child, child maltreatment, bully; partner violence, partner abuse, spouse abuse, partner aggression, couple violence, couple abuse, couple aggression, domestic violence; elder neglect, elder abuse; and ILA. We reviewed the reference lists of eligible articles and relevant review papers to identify studies and reports that were not captured in the initial database search.
Study Selection
The two authors performed the data extraction and evaluation process. Three primary criteria were used for the inclusion of articles in this meta-analysis: (a) published between May 2018 and March 2025 (i.e., after the period covered by our previous meta-analysis; Chan et al., 2021); (b) reported at least two types of family victimization, including but not limited to CAN, IPV, EA, and ILA; and (c) reported the co-occurrence of victimization among members of the same household. Articles were excluded if they: (a) reported only a single type of family victimization; (b) reported victimization occurring at different life stages for the same individual; (c) did not provide sufficient data for effect size calculation; or (d) focused on intervention evaluations or reviewed topics unrelated to family victimization. All studies meeting these criteria were considered eligible, regardless of context, participants’ age, gender, sexual orientation, religion, language, or cultural background.
The search identified a total of 5,848 records. After removing duplicates, 3,423 records remained. Of these, 3,257 records were excluded for the following reasons: 308 focused on events that occurred in childhood, 88 were intervention studies without prevalence data, 844 addressed non-family violence, 635 were qualitative studies (e.g., commentaries, legal reports), 1,206 examined a single type of victimization without co-occurrence, and 176 were review studies lacking empirical data. During full-text screening for eligibility, 117 articles were excluded from the meta-analysis due to insufficient data (n = 86), or not involving members of the same household (n = 31). As a result, 49 studies were included in the analysis. One article (Dong & Wang, 2019) provided three estimates reporting the co-occurrence of CAN and IPV, CAN and EA, and IPV and EA. These estimates were computed independently for effect size calculation. In total, we listed 51 estimates from the 49 articles. Details of the article selection process are presented in Figure 1.
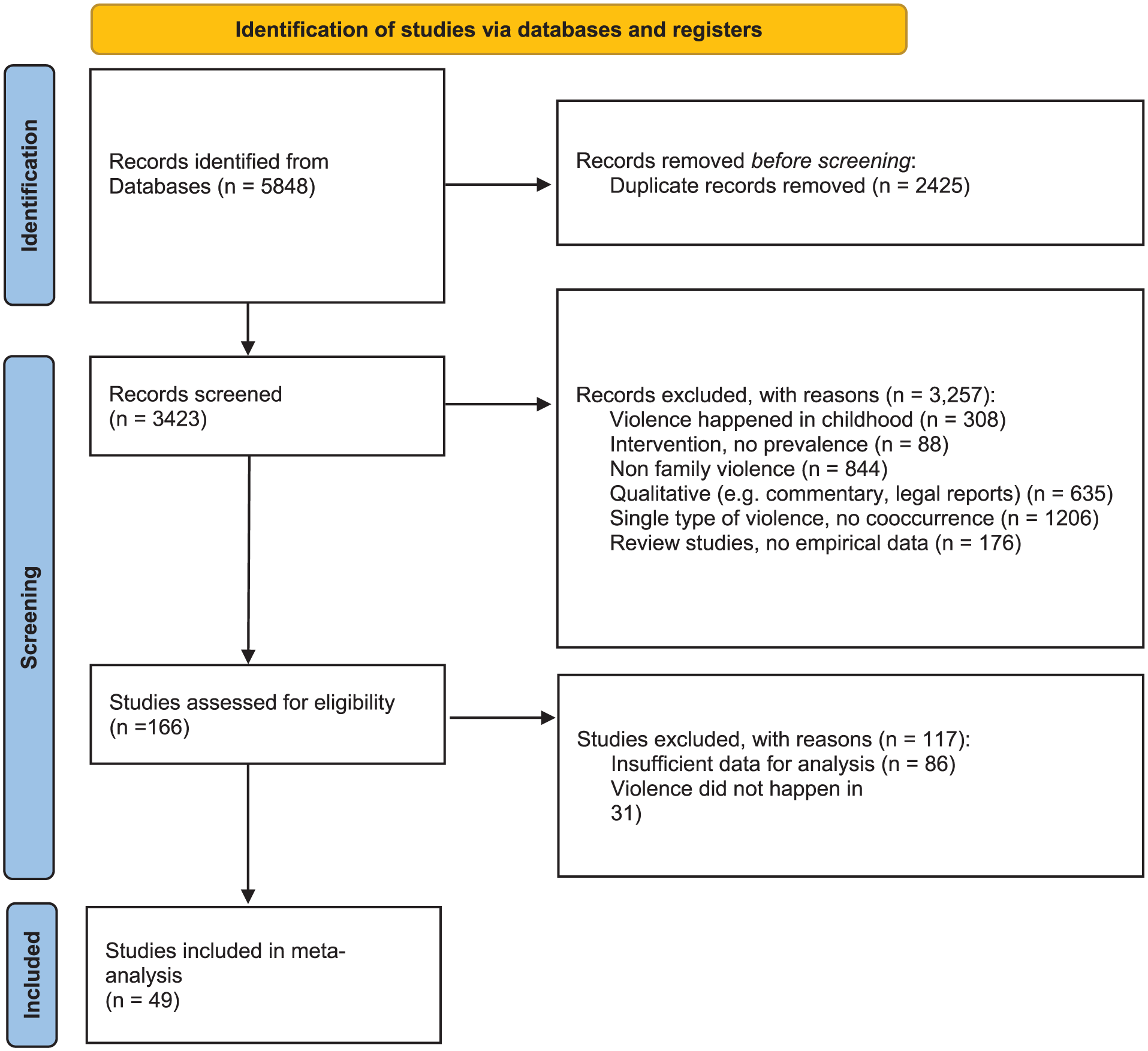
Summary of the search results and article selection procedures.
Data Extraction
The eligible articles were numbered and summarized in a spreadsheet to record the following aspects: (a) Publication information (authors, publication year, and study site); (b) Violence-related factors (types of victimization and measures); (c) Study characteristics (sampling method, setting, sample size, age distribution, gender ratio, ethnicity, and informants); and (d) Individual and family factors associated with polyvictimization. Data were extracted from the included studies for the outcome measures, including descriptive data (event rate and sample sizes) and effect sizes (e.g., Cohen’s d and odds ratios [ORs]). The 49 studies were randomly distributed among the authors for independent assessment to ensure coding reliability.
Quality Assessment
The authors independently assessed the quality of the 49 studies using a checklist covering 5 key aspects, rated on a binary “1/0” scale. Studies were evaluated based on whether they: (a) reported sample recruitment procedures, (b) described the profiles or characteristics of the sample, (c) used validated measures or scales, (d) performed appropriate statistical analyses, and (e) provided sufficient data for analysis. Scores ranged from 0 to 5, with higher scores indicating better quality for inclusion in the meta-analysis. The average score of the included studies was 4.78, indicating their overall high quality. No study was excluded due to unsatisfactory quality.
Statistical Analysis
First, we calculated pooled estimates of the co-occurrence rates of family victimization and polyvictimization using 51 estimates from the 49 studies screened during this study period (May 2018 to March 2025). As an update to the meta-analysis on this topic, we combined these 51 estimates with our previous meta-analysis (Chan et al., 2021), which included 38 studies published before April 2018, resulting in pooled estimates based on a total of 89 estimates. The 89 estimates were further categorized by sample type: (a) community samples, primarily selected through probability sampling in household or school settings; and (b) clinical samples, typically drawn via convenience sampling from child protective services (CPS), medical records, or police databases. Due to heterogeneity in victimization types and contexts across studies, we employed a random-effects model (Borenstein et al., 2010). Results were visualized using forest plots with 95% confidence intervals (CI) for each study. Second, we computed pooled ORs with 95% CIs for individual and family correlates of family polyvictimization. Heterogeneity was assessed using Cochran’s Q statistic with corresponding p-value and I2 statistic to quantify the variance proportions. To assess potential publication bias, a funnel plot was generated, supplemented by several statistical tests including the Classic Fail-Safe N, Egger’s regression test, and Duval and Tweedie’s trim-and-fill method. The Comprehensive Meta-Analysis software (version 4; Biostat, Inc.) was used to conduct all statistical analyses.
Results
Study Characteristics
As shown in Figure 1, the final pool for this meta-analysis consisted of 49 studies screened during this study period, all of which provided ORs on the co-occurrence of victimization or associated factors. The characteristics of the studies are summarized in Table 1. Sample sizes ranged from 90 to 305,867, together providing a substantial sample size of 543,196 for the general synthesis of effect sizes. This represents a significant increase compared to the 99,956 participants included in the previous review, along with an increase in the number of studies from 38 to 49. Two studies (#1–2) reported family polyvictimization (CAN, IPV, EA, and additional forms), 13 studies (#3–15) reported child polyvictimization, 31 studies (#16–46) reported the co-occurrence of CAN and IPV, 1 study (#47) on the co-occurrence of CAN and IPV, CAN and EA, and IPV and EA. Two studies (#48–49) reported the co-occurrence of IPV and ILA.
Characteristics of the Studies Included in the Overall Prevalence Synthesis.
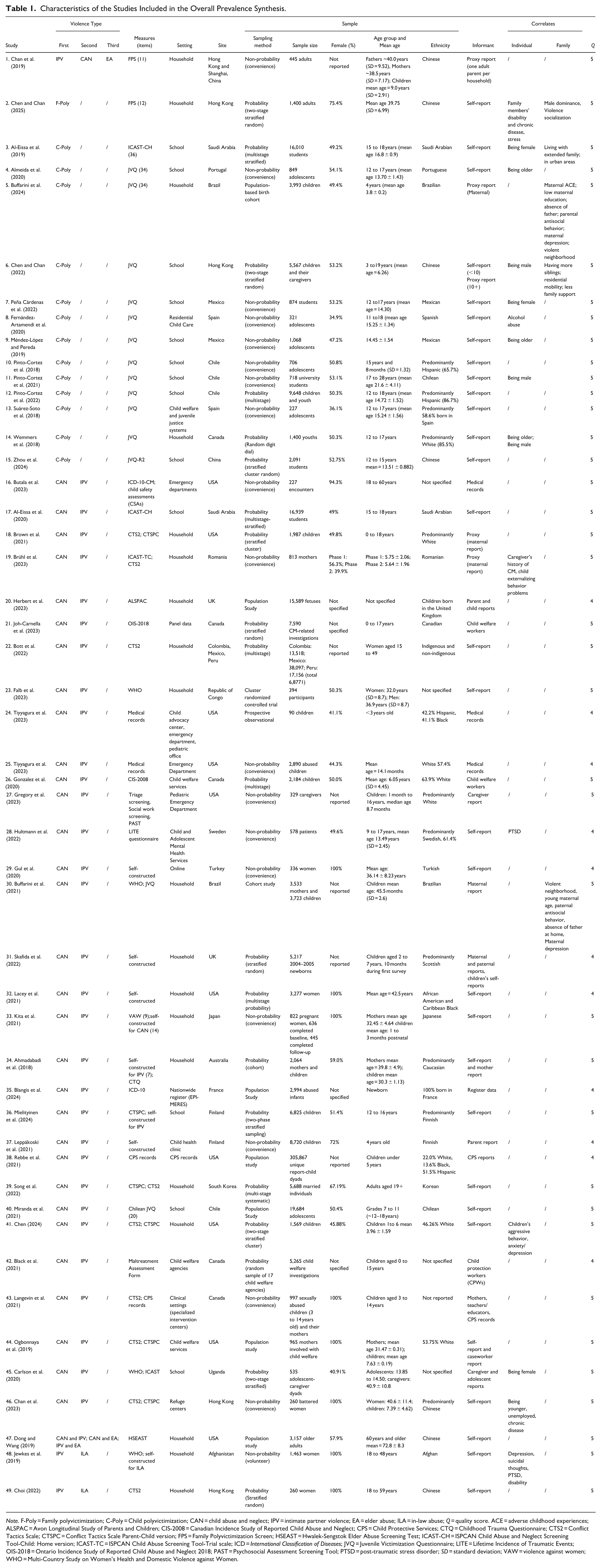
Note. F-Poly = Family polyvictimization; C-Poly = Child polyvictimization; CAN = child abuse and neglect; IPV = intimate partner violence; EA = elder abuse; ILA = in-law abuse; Q = quality score. ACE = adverse childhood experiences; ALSPAC = Avon Longitudinal Study of Parents and Children; CIS-2008 = Canadian Incidence Study of Reported Child Abuse and Neglect; CPS = Child Protective Services; CTQ = Childhood Trauma Questionnaire; CTS2 = Conflict Tactics Scale; CTSPC = Conflict Tactics Scale Parent-Child version; FPS = Family Polyvictimization Screen; HSEAST = Hwalek-Sengstok Elder Abuse Screening Test; ICAST-CH = ISPCAN Child Abuse and Neglect Screening Tool-Child: Home version; ICAST-TC = ISPCAN Child Abuse Screening Tool-Trial scale; ICD = International Classification of Diseases; JVQ = Juvenile Victimization Questionnaire; LITE = Lifetime Incidence of Traumatic Events; OIS-2018 = Ontario Incidence Study of Reported Child Abuse and Neglect 2018; PAST = Psychosocial Assessment Screening Tool; PTSD = post-traumatic stress disorder; SD = standard deviation; VAW = violence against women; WHO = Multi-Country Study on Women’s Health and Domestic Violence against Women.
Table 1 Column “measures” shows that the measures used across studies to assess family polyvictimization and related constructs include a combination of standardized tools and self-constructed instruments. The most commonly used measures across the studies include the JVQ and its variants (e.g., JVQ-R2, Chilean JVQ), which were employed in 14 studies. The JVQ assesses exposure to multiple forms of victimization, including physical abuse, sexual abuse, peer/sibling victimization, and witnessing family violence (e.g., “Has anyone ever hit or attacked you on purpose with a stick or other hard object?”). The Conflict Tactics Scales (CTS2) and its Parent-Child version (CTSPC) were employed in 10 studies. These tools measure interpersonal violence in families, such as physical assault, psychological aggression, and negotiation strategies (e.g., “How often did you push or shove your partner during an argument?” or “How often did you spank your child with your hand?”). The International Child Abuse Screening Tool (ICAST-CH and ICAST-TC) was used in four studies. ICAST measures physical, emotional, and sexual abuse, as well as neglect (e.g., “Has someone ever deliberately burned you with a cigarette, lighter, or something else hot?”). A smaller number of studies relied on self-constructed measures tailored to specific topics: Choi (2022) and Jewkes et al. (2019) used self-constructed tools to assess ILA in Afghanistan and Turkey, respectively. Ahmadabadi et al. (2018) and Langevin et al. (2021) developed instruments for IPV and its overlap with child abuse. Items in these measures included culturally specific questions, such as “Has your mother-in-law ever prevented you from leaving the house without permission?.” Additionally, three studies incorporated medical records (Chen, 2024; Tiyyagura et al., 2023) to provide objective data on injuries and abuse-related healthcare visits. Population-based studies such as ALSPAC (UK) and OIS-2018 (Canada) used comprehensive longitudinal datasets to assess adverse childhood experiences and family polyvictimization.
The studies are conducted across various global regions, including North America (USA, Canada, Mexico), South America (Brazil, Chile, Colombia, Peru), Europe (Portugal, Spain, UK, Romania, France, Finland, Sweden), Asia (mainland China, Hong Kong, Japan, South Korea, Saudi Arabia, Afghanistan, Turkey), Africa (Republic of Congo, Uganda), and Oceania (Australia). Compared to the previous meta-analysis, this review does not include studies from Vietnam, Taiwan, Tajikistan, or India, but incorporates 19 additional countries across various global regions, including North America (Mexico), South America (Brazil, Chile, Colombia, Peru), Europe (Portugal, UK, Romania, France, Finland, Sweden), Asia (Japan, South Korea, Saudi Arabia, Afghanistan, Turkey), Africa (Republic of Congo, Uganda), and Oceania (Australia). This expanded geographical distribution highlights the growing global recognition of family polyvictimization as an important issue across diverse cultural contexts.
Sample sizes ranged from small community-based studies to large-scale national surveys, offering a broad scope of representation. Participants included various age groups, such as children, adolescents, adults, and older adults, with gender representation generally balanced, though some studies focused on specific groups, such as women or children. The informants recruited across studies include a mix of proxy reports in 5 studies (e.g., parents, caregivers, maternal and paternal reports, child welfare workers, teachers, and caseworkers), self-reports in 31 studies (from children, adolescents, or adults), and official records in 9 studies (e.g., medical records, CPS reports, register data). The studies employed a mix of sampling methods, including both probability and non-probability approaches. Among these, convenience sampling was the most frequently used method in 18 studies. Probability-based methods, such as stratified, multistage, or cluster sampling, were also commonly employed in 21 studies to ensure representativeness. A smaller subset of studies used population-based sampling techniques, including birth cohorts and large-scale population studies.
Overall Synthesis of Co-occurrence Rates
The current meta-analysis (Current MA) comprises 49 studies, among which 1 study (Dong & Wang, 2019) reported 3 estimates including CAN and IPV, IPV and EA, and CAN and EA. Figure 2 and Table 2 show that these 49 studies produced 51 estimates in the overall synthesis, reporting an overall event rate of 27.0% (95% CI [22.5, 32.1]), with significant heterogeneity (Q = 48084.249, p < .001, I2 = 99.896). When combined with the previous meta-analysis, which reported an event rate of 18.3% [14.3, 23.2] (Chan et al., 2021), across a total of 89 estimates, the overall event rate decreases slightly to 23.1% [20.0, 26.6]. This analysis also shows significant heterogeneity (Q = 54,911.015, p < .001, I2 = 99.840).
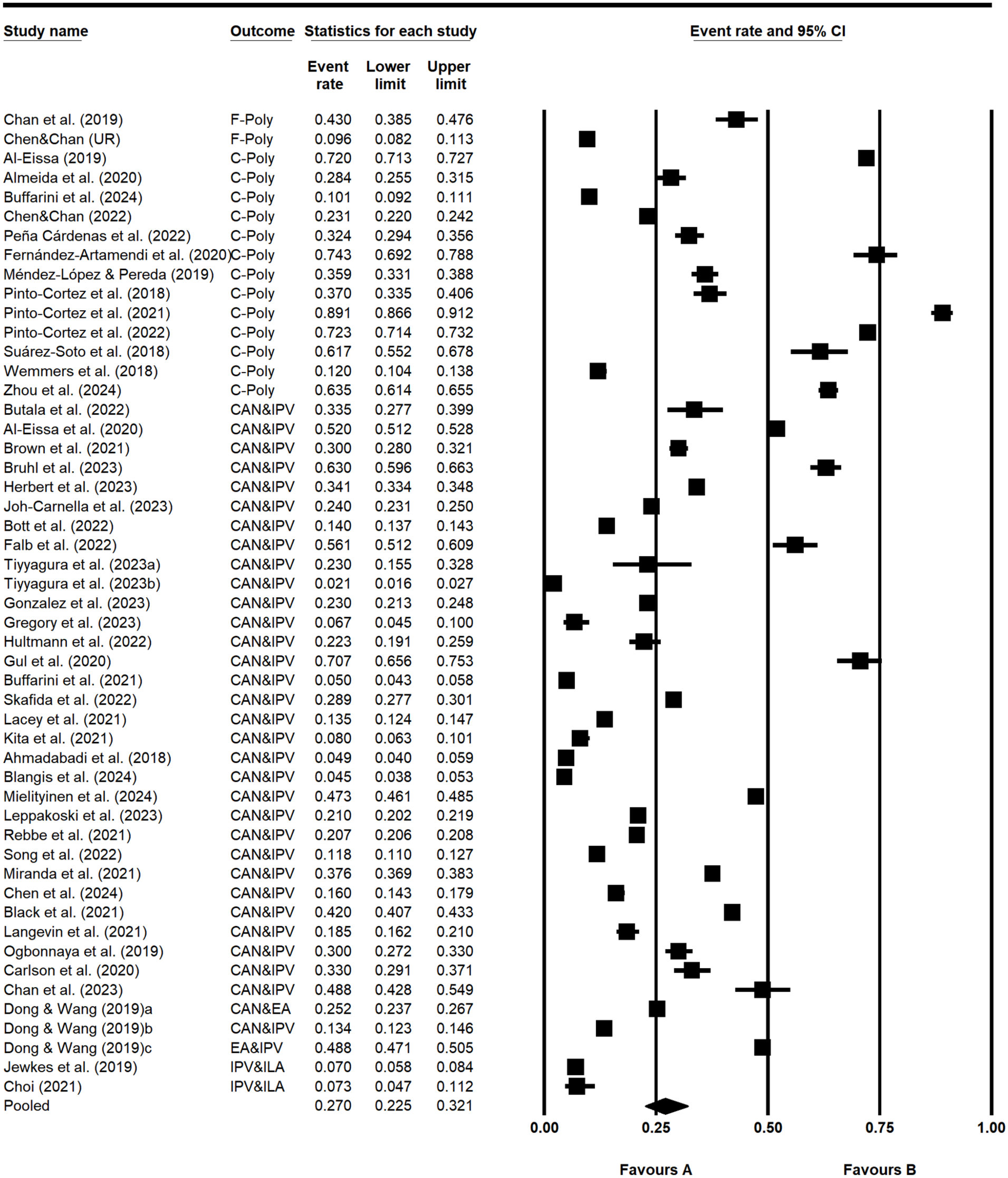
Co-occurrence rates of family violence among the included studies. Heterogeneity: Q = 48084.249, df = 50, p = .000, I2 = 99.896.
Event Rates of Different Types of Polyvictimization.
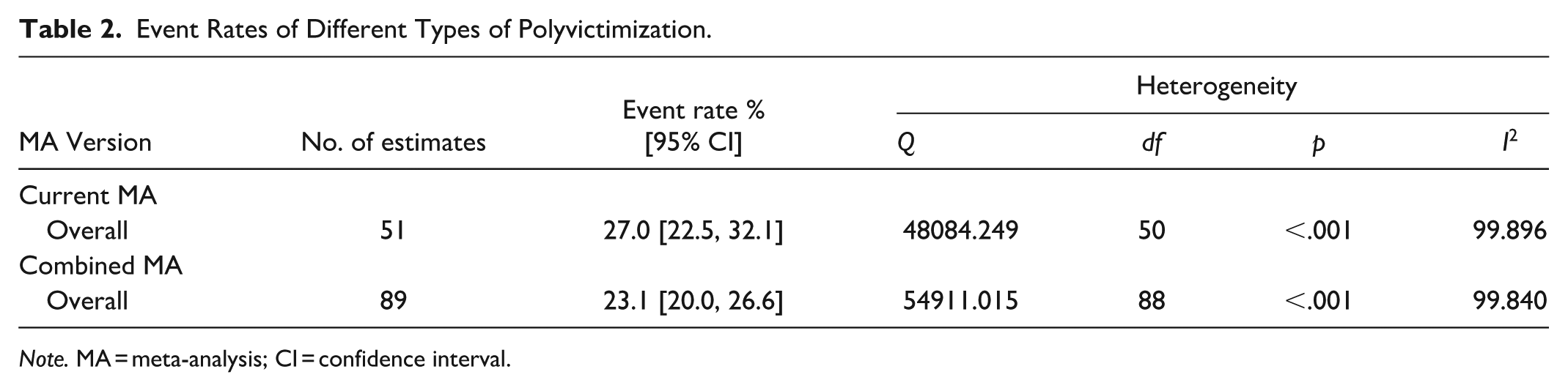
Note. MA = meta-analysis; CI = confidence interval.
Subgroup Comparisons of Rates of Polyvictimization
Table 3 shows the subgroup comparison using a total of 89 estimates (combined MA). The event rate of family polyvictimization is 11.3% (95% CI [1.8, 46.8]), based on 3 estimates, with heterogeneity (Q = 781.923, p < .001, I2 = 99.744). Similarly, for child polyvictimization, the event rate is 35.1% [22.5, 50.1], based on 19 estimates, with heterogeneity (Q = 17565.631, p < .001, I2 = 99.898).
Subgroup Comparisons of Event Rates of Polyvictimization.
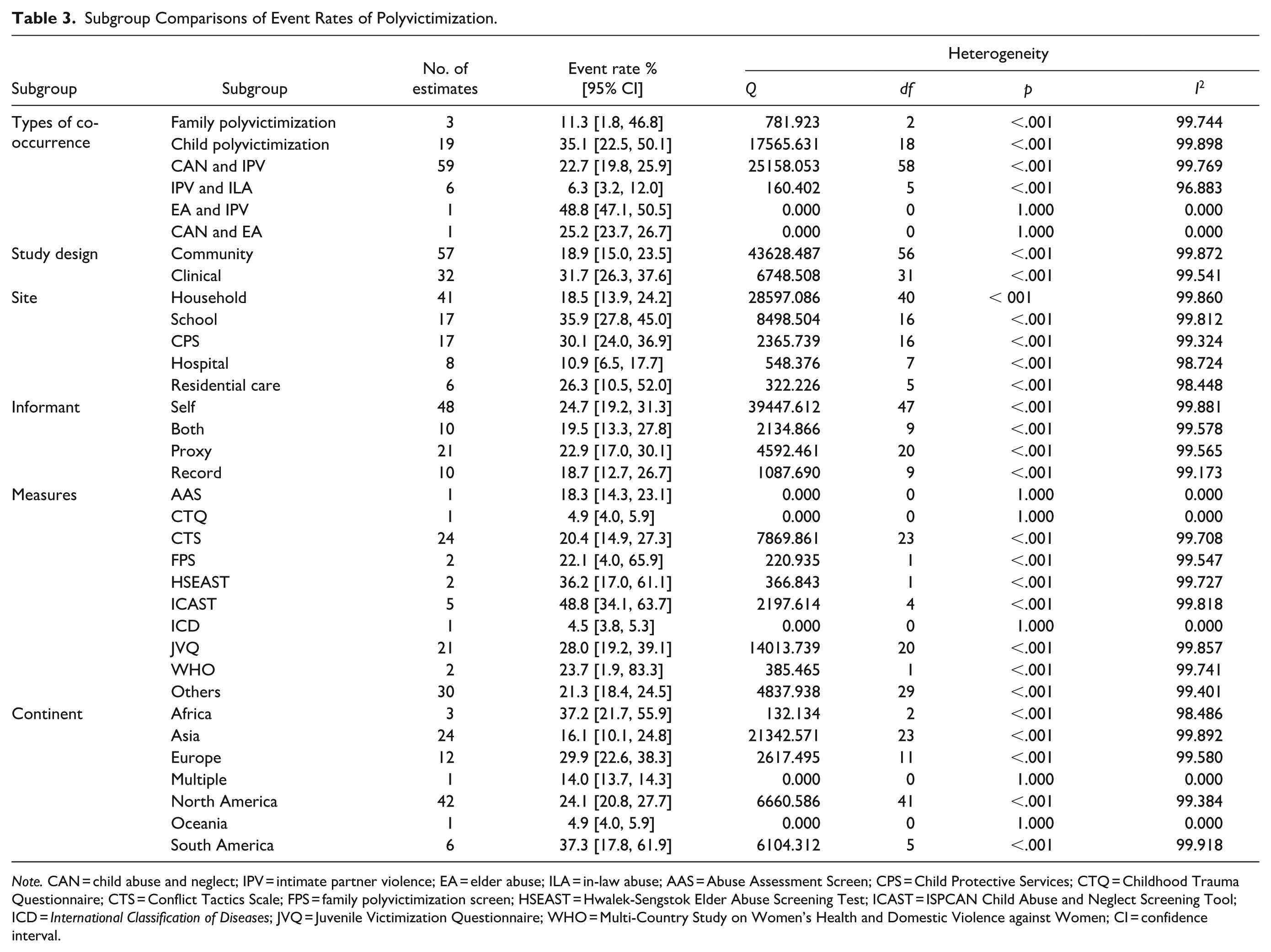
Note. CAN = child abuse and neglect; IPV = intimate partner violence; EA = elder abuse; ILA = in-law abuse; AAS = Abuse Assessment Screen; CPS = Child Protective Services; CTQ = Childhood Trauma Questionnaire; CTS = Conflict Tactics Scale; FPS = family polyvictimization screen; HSEAST = Hwalek-Sengstok Elder Abuse Screening Test; ICAST = ISPCAN Child Abuse and Neglect Screening Tool; ICD = International Classification of Diseases; JVQ = Juvenile Victimization Questionnaire; WHO = Multi-Country Study on Women’s Health and Domestic Violence against Women; CI = confidence interval.
For the co-occurrence of two types of family violence, the most common form is CAN and IPV. The event rate of CAN and IPV co-occurrence is 22.7% (95% CI [19.8, 25.9]), based on 59 estimates, with significant heterogeneity (Q = 25158.053, p < .001, I2 = 99.769). For IPV and ILA, the event rate is 6.3% [3.2, 12.0], based on 6 estimates, with significant heterogeneity (Q = 160.402, p < .001, I2 = 96.883). For EA and IPV as well as EA and CAN, only 1 estimate in each case was recorded.
Comparisons of Rates in the Characteristics of Studies
There are several study characteristics that show higher rates of co-occurrence, such as the investigation of clinical samples (31.7%, 95% CI [26.3, 37.6]), particularly recruited from CPS (30.1% [24.0, 36.9]). For the community samples (18.9% [15.0, 23.5]), the school-based studies showed the higher rates of co-occurrence (35.9% [27.8, 45.0]).
The informants do not seem to produce very different event rates. The rates obtained from the self-reported studies (24.7%), followed by proxy-only studies (22.9%), and both (19.5%) were comparable. The record-based study, which relies on reports from professionals after investigations, appears to have a slightly lower rate (18.7%), but this difference may not be significant. For the measures employed, there are no clear patterns related to the rates of co-occurrence.
Notably, while North America previously accounted for the majority of studies in our earlier analyses (Chan et al., 2021), this updated version includes more studies from other continents, particularly from Africa, South America, and Asia. These regions consistently report higher event rates of polyvictimization compared to North American studies. For instance, South America (37.3% [17.8, 61.9]) and Africa (37.2% [21.7, 55.9]) are the regions with the highest event rates. North America (24.1% [20.8, 27.7]) and Europe (29.9% [22.6, 38.3]) report intermediate rates, with Asia reporting a lower event rate in the combined analysis (16.1% [10.1, 24.8]). This shift in representation underscores the importance of including diverse geographical contexts, as studies from higher-rate regions may reflect differences in cultural, social, or systemic factors contributing to polyvictimization. Heterogeneity is significant across all continents (I2 > 97%).
Odds Ratios of Factors Associated with Polyvictimization
Table 4 lists the ORs on several factors associated with polyvictimization. The factors are comparable in the ORs, with relatively higher values in disability (OR = 3.000, 95% CI [2.023, 4.448]) and violence approval (OR = 3.319 [1.897, 5.807]). However, there is a great variation among the studies investigating the factors. For each factor, only a few studies, ranging from 2 to 7, provided analyses. It makes it difficult to obtain widely studied factors for comparison.
Odds Ratios of the Factors Associated with Polyvictimization.

Note. ACE = adverse childhood experiences; SES = socioeconomic status; PTSD = post-traumatic stress disorder; CI = confidence interval.
p < .05. **p < .01. ***p < .001.
Publication Bias
The funnel plot (Figure 3) shows a relatively symmetrical distribution of studies around the pooled effect size, with no substantial asymmetry indicative of publication bias. The Classic Fail-Safe N indicates that 1,023 additional studies with null results would be required to render the observed effects non-significant (p > .05). This high number, relative to the 51 observed studies, suggests that the results are robust against publication bias. Egger’s regression test resulted in a non-significant intercept (6.96, p = .206), suggesting no evidence of small-study effects. The Duval and Tweedie’s trim-and-fill method estimated that adjusting for two potentially missing studies would have a minimal impact on the pooled effect size, with the fixed-effects estimate changing from 25.86% to 25.79% and the random-effects estimate decreasing slightly from 27.05% to 25.09%. These small adjustments indicate that the results are stable and unlikely to be heavily influenced by publication bias. In all, the statistical tests and visual inspection of the funnel plot provide no strong evidence of publication bias, supporting the reliability of the meta-analysis results.
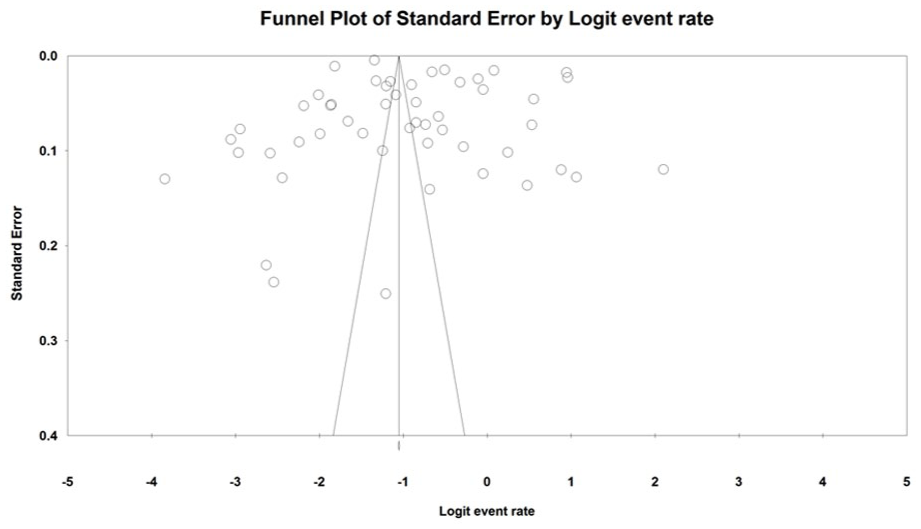
Funnel plot of standard error by logit event rate.
Discussion
The updated meta-analysis includes a significantly larger sample size of 543,196 participants, compared to 99,956 in the previous meta-analysis, for the general synthesis of effect sizes (Table 5). The effect size in the current meta-analysis is larger than the previous one (27.0% vs. 18.3%). With the 87 studies providing 89 estimates, the overall event rate of co-occurrence is 23.1%. The increase in the co-occurrence rate may be related to the geographical regions where the studies were conducted. While North America accounted for the majority of studies in our earlier meta-analysis (Chan et al., 2021), this updated version includes more studies from other continents, such as Africa and South America. These regions consistently report higher event rates of polyvictimization compared to North American studies. The differences in co-occurrence rates between regions are challenging to explain definitively but may be influenced by variations in family structures. For instance, regions with a higher prevalence of extended family households, including grandparents or other relatives living in the same household, may report more types of family violence. This could increase the likelihood of identifying and reporting co-occurring victimization, contributing to higher event rates.
Summary of Critical Findings.
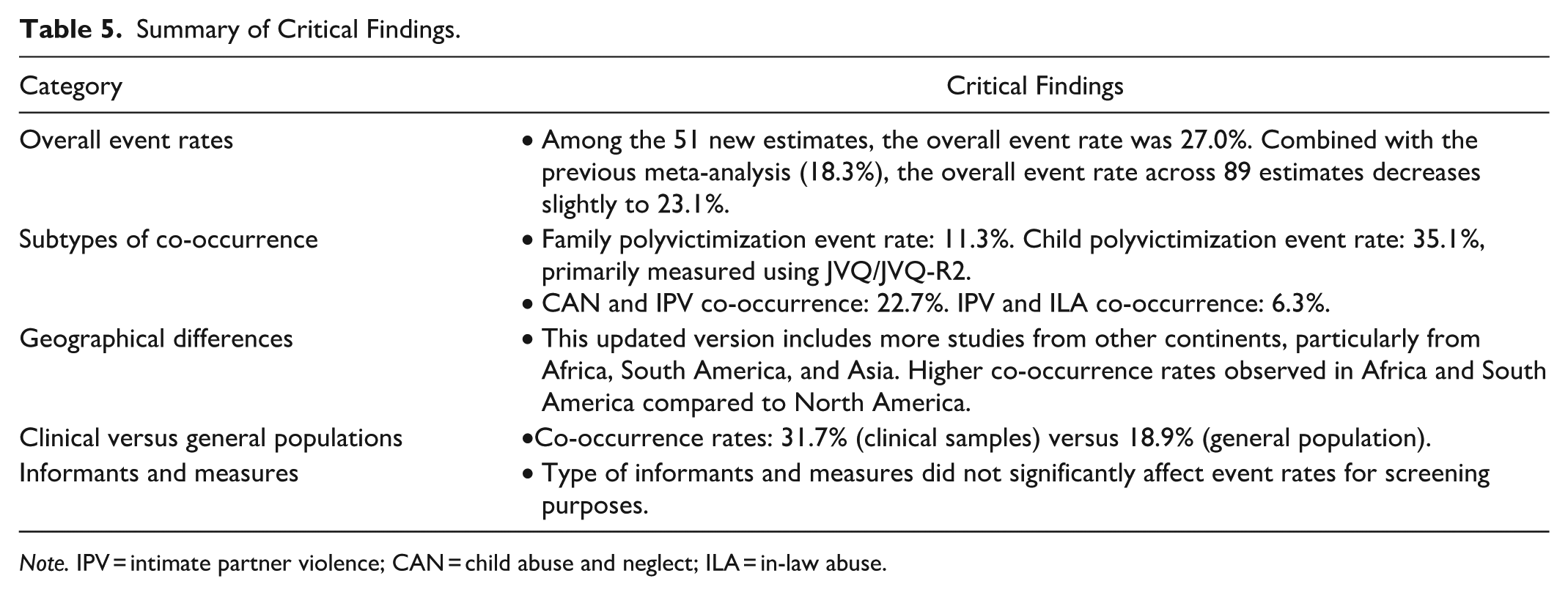
Note. IPV = intimate partner violence; CAN = child abuse and neglect; ILA = in-law abuse.
In North America, the nuclear family model is quite prevalent, particularly in the United States and Canada. A significant percentage of households consist of nuclear families, although there has been a rise in single-parent households and non-traditional family structures in recent years (Mitchell & Li, 2023; Organisation for Economic Co-operation and Development, 2016; Sassler, & Lichter, 2020). In South America, while nuclear families are common, extended family living arrangements are also prevalent (Cabib et al., 2023; Esteve et al., 2022; Reynolds et al., 2018). Cultural norms often emphasize close family ties, leading to a mix of nuclear and extended family households. In African countries, extended families are more common than nuclear families. This is influenced by cultural traditions that emphasize communal living and support systems (Nwanmuoh et al., 2024; Okeke-Ihejirika et al., 2022). Asia presents a varied picture. In countries like Japan and South Korea, nuclear families are common, especially in urban areas (Jiang et al., 2024). This is similar to Hong Kong, a metropolitan Chinese society. According to our most recent population study, 43.2% of Hong Kong families live with at least one grandparent in the same household (Chen & Chan, 2025). In South Asia and parts of Southeast Asia, extended families are more prevalent due to cultural norms and economic factors (Dommaraju, 2023; Lajom & Sibunruang, 2024). While nuclear families are a common household structure globally, the prevalence varies widely depending on regional, cultural, economic, and social contexts. We do not intend to draw a conclusion and raise the possibility of examining the family structure, rather than focusing on parents and children, when investigating multiple types of family violence.
Notably, there is a mild increase in the number of studies on family polyvictimization, with an event rate of 11.3% (95% CI [1.8, 46.8]). The number of studies on child polyvictimization has increased significantly, with an event rate of 35.1% [22.5, 50.1]. Our findings show that the prevalence of family victimization co-occurrence is higher in clinical samples compared to the general population (31.0% vs. 18.9%). This result highlights the greater likelihood of identifying a second victim in the same family once the first victim comes to the attention of health or social services.
Sub-group analyses indicate that the type of informants and measures do not seem to affect the event rates. Most studies reported the occurrence of victimization for screening purposes, allowing for the computation of co-occurrence rates. While variations in the types of informants and measures do not impact screening, this does not imply that they have no effect for assessment purposes, which may depend on the quality of responses.
Limitations and Future Research
One of the study objectives is to investigate the correlates of family polyvictimization. Several factors have been identified as significantly associated with polyvictimization. However, the variations in ORs are not significant, likely due to the considerable variation among the studies examining these factors. For each factor, only a few studies, ranging from 2 to 7, provided analyses, making it challenging to identify widely studied factors for comparison. Therefore, interpretation should be cautious when comparing the ORs, as the differences may not reliably indicate the relative importance of the factors.
Among the various types of family polyvictimization, the major proportions are found in child polyvictimization (21%) and the co-occurrence of CAN and IPV (66%). Child polyvictimization is primarily measured using the JVQ or JVQ-R2, which can include multiple types of family victimization, such as child maltreatment, sibling violence, witnessing domestic violence, and witnessing a parent’s assault on a sibling. The JVQ can potentially be coded for family polyvictimization if perpetrators are specified and multiple victims are identified (e.g., child, sibling, or parents). However, it cannot identify other victims like the elderly or adult children. Studies using the JVQ do not typically code for multiple victims. Some items are grouped into broader categories, such as peer or sibling, and “parent” in Module G of JVQ-R2 may refer to parents, stepparents, parents’ intimate partners, foster parents, or grandparents. To maximize the JVQ’s potential in measuring family polyvictimization, researchers may need to adjust item responses to align with their research goals.
The investigation of the co-occurrence of CAN and IPV is understandably more manageable as it focuses on the nuclear family structure. However, families often live in extended arrangements, not only in South American, African, or Asian cultures. In the United States, for example, African American grandparents are underrepresented in studies (Kelley et al., 2013). Investigations should consider the dynamics of family members who play a role in the occurrence of CAN or IPV. If CAN occurs in the context of family polyvictimization, welfare plans should be tailored to engage other family members to protect child victims and ultimately end family violence.
The strengths of this review include updating the prevalence estimates of family polyvictimization by incorporating a greater number of studies and covering larger, more diverse populations from various regions. As a result, the effect sizes computed are more representative of a broader population. The findings also indicate that the prevalence of overlapping family victimization is higher in clinical samples, underscoring the increased likelihood of identifying a second victim within the same family once the first victim comes to the attention of health or social services.
Implications for Research, Practice, and Policy
Future research should prioritize the investigation of family-level risk factors for polyvictimization, with particular attention to diverse family structures and cultural contexts (Table 6). There is a need to adapt and expand existing assessment tools, such as the JVQ, to measure family polyvictimization beyond child victims, including elderly family members and adult children. Additionally, more studies are needed to address gaps in the literature concerning underrepresented populations, such as African American grandparents and extended family members. Examining the co-occurrence of victimization within extended family arrangements will provide a deeper understanding of the dynamics and patterns of family violence.
Implications for Practice, Policy, and Research.
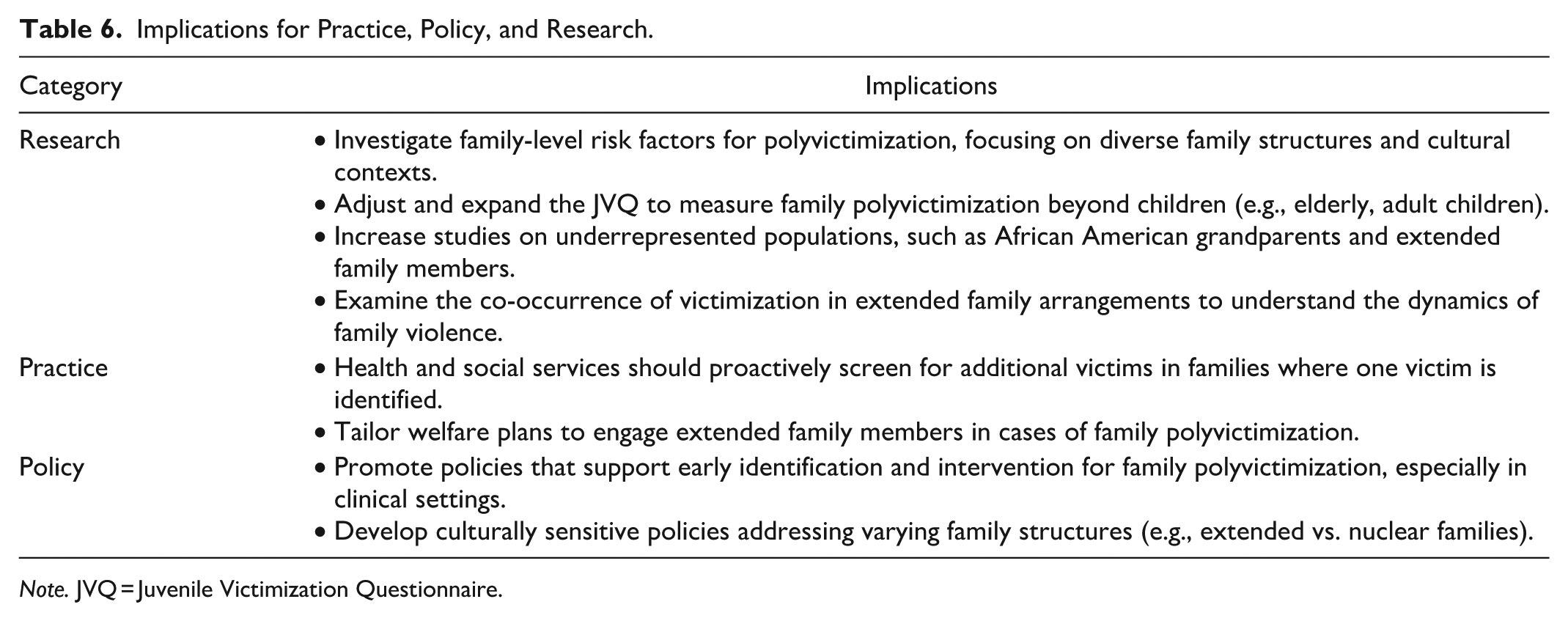
Note. JVQ = Juvenile Victimization Questionnaire.
In practice, health and social service providers should proactively screen for additional victims whenever a single victim is identified within a family. This approach can help uncover hidden cases of polyvictimization and ensure that all affected individuals receive appropriate support. Furthermore, welfare plans should be tailored to engage extended family members, recognizing their potential roles in both the risk and protection of family members in cases of polyvictimization.
At the policy level, there is a pressing need to promote policies that support the early identification and intervention of family polyvictimization, particularly within clinical settings where the risk is higher. Policymakers should also focus on developing culturally sensitive policies that address the needs of families with varying structures, such as extended versus nuclear families, to ensure that interventions are both effective and inclusive.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work described in this paper was supported by a fellowship award from the Research Grants Council of the Hong Kong Special Administrative Region, China (Project No. PolyU/SRFS2223-5H01).