
Abstract
Children with disabilities are at heightened risk of violence, but existing meta-analyses rarely explore the impact of multiple disabilities and polyvictimization. This study updates global estimates and investigates how different disability types intersect with victimization risk. Databases of literature published on or before July 2024 were searched. Inclusion criteria required studies to (a) involve participants aged ≤18 years with professionally diagnosed disabilities, (b) report comparative data with non-disabled peers, and (c) present quantitative measures of victimization. A total of 44 publications (1,734,560 children) met the inclusion criteria and were included in the analysis. Random-effects models estimated pooled odds ratios (ORs), with subgroup analyses conducted. The overall OR was 2.04 (95% CI [1.84, 2.52]). Polyvictimization was significantly associated with visible disabilities (OR = 2.04 [1.42, 2.93]), invisible disabilities (OR = 3.16 [1.76, 5.70]), and multiple disabilities (OR = 4.17 [2.25, 7.74]). Children with multiple disabilities had markedly high risk for physical violence (OR = 4.07 [2.12, 7.81]). Subgroup analyses showed that children in secondary school (OR = 4.16 [2.83, 6.11]) experienced the highest risks for polyvictimization. Child self-reports yielded the highest ORs (OR = 4.16 [2.82, 6.11]) compared to mixed or parent reports. Children with invisible and multiple disabilities face disproportionate risks, particularly for polyvictimization. These findings underscore the need for early identification and tailored prevention efforts. Future research should address definitional inconsistencies and expand representation across regions and populations.
Introduction
Victimization against children remains a critical public health and social justice concern worldwide. Approximately one in four children experiences violence each year, with particularly negative health outcomes documented among vulnerable subgroups such as children with disabilities (Hillis et al., 2016). Existing evidence consistently suggests that children with disabilities experience disproportionately higher rates of victimization compared to their peers without disabilities, facing diverse forms of violence, including physical, emotional, sexual, and peer-related abuse across various contexts (Fang et al., 2022; Fisher et al., 2008; Jones et al., 2012). These elevated risks and serious consequences highlight the necessity of understanding the relationship between disability and victimization for these especially vulnerable children.
Several meta-analyses have established a robust association between childhood disability and increased victimization risk. Jones et al. (2012) found that children with disabilities were 3.68 times more likely to experience violence than their non-disabled peers, including a 3.56-fold increased risk for physical violence and a 2.88-fold increased risk for sexual violence. More recently, Fang et al. (2022) reported that children with disabilities experienced significantly higher rates across various types of victimization, with an odds ratio (OR) of 2.08 compared to children without disabilities.
While these analyses have broadly considered various classifications of disabilities and victimization types, important nuances remain inadequately addressed. Existing reviews have rarely examined the compounded risks faced by children with multiple disabilities, which refer to those who experience more than one form of impairment concurrently. Previous research suggests that the co-occurrence of impairments is associated with more severe challenges and a heightened risk of victimization (Seppälä et al., 2020; Tietze et al., 2012). Therefore, multiple disabilities may represent a major risk factor for child victimization. Additionally, polyvictimization has also been largely overlooked in previous meta-analyses. Polyvictimization is defined as exposure to two or more distinct types of victimization, rather than repeated instances of a single type (Bidarra et al., 2016; Pearson et al., 2023). It has emerged as a powerful marker of cumulative trauma, strongly linked to adverse developmental and mental health outcomes. Children who experience polyvictimization tend to report poorer physical and psychological well-being, along with higher rates of psychopathological and psychosomatic symptoms (Chan et al., 2017). However, existing meta-analyses have focused on single disability types or individual forms of violence, overlooking how intersecting vulnerabilities may increase overall risk. The current meta-analysis addresses these critical gaps by systematically examining both multiple disabilities and polyvictimization, aiming to provide a more comprehensive and actionable understanding of the complexity of violence experienced by children with disabilities.
To accurately assess this relationship, clear definitions of both disability and victimization are essential. For this study, children with disabilities are defined as individuals 18 years of age or younger (with flexibility to include 19-year-olds when studies are otherwise eligible) who have impairments that may hinder their full and effective participation in society on an equal basis with others (United Nations, 2006). This definition encompasses a spectrum of conditions, including visible disabilities (e.g., physical or sensory impairments easily recognized by others), invisible disabilities (e.g., emotional or neurodevelopmental conditions not readily observable), and multiple disabilities (i.e., co-occurrence of two or more impairments in an individual). Past research has demonstrated a strong link between visible disabilities and victimization experiences related to stigma, bullying, discrimination, and overt aggression from peers and community members (Carter & Spencer, 2006; Pinquart, 2017). In contrast, invisible disabilities may profoundly impact social interactions and communication, thereby heightening vulnerability through mechanisms such as peer misunderstanding, social isolation, caregiver frustration, and punitive reactions to misinterpreted behaviors (de Beer et al., 2022; Humphrey & Hebron, 2015). Despite these insights, no meta-analysis to date has explicitly distinguished between visible and invisible disabilities, leaving important gaps in our understanding of how disability visibility influences victimization risk. Our definition of victimization is similarly broad, covering not only family-based maltreatment but also bullying, emotional abuse, community and environmental violence, neglect, physical violence, sexual violence, and polyvictimization.
This meta-analysis aims to advance research in three ways. First, it employs a more detailed categorization of disability and victimization types, explicitly differentiating visible from invisible disabilities. Second, it systematically addresses the issue of multiple disabilities, examining whether children experiencing co-occurring disabilities are at uniquely elevated risk. Finally, this analysis explicitly explores polyvictimization, investigating how multiple forms of victimization cumulatively impact children with disabilities.
In addition, building upon previous research that has identified variability in victimization risk across demographic and geographic (Fang et al., 2022; Jones et al., 2012), we conduct a more detailed targeted subgroup analysis to further examine how these factors may influence the relationship between disability and victimization. Specifically, we explore key demographic variables (e.g., sex and age groups), geographic variation (e.g., regional and developmental contexts), and methodological characteristics (e.g., study design and reporting source). Subgroup analyses are particularly important because they help identify which children are most at risk and under what conditions, thereby informing more precise policy responses and targeted intervention strategies.
We hypothesize that children with disabilities are at significantly higher risk of experiencing both individual forms of victimization and polyvictimization compared to children without disabilities. We further predict that risk patterns will vary significantly by disability visibility and multiplicity, with potentially greater vulnerability among children with multiple and/or invisible disabilities. By comprehensively categorizing disability types and assessing victimization experiences, this research offers a more nuanced understanding of vulnerability patterns that can inform targeted prevention efforts.
Method
Search Strategy
We searched Scopus, PsycINFO, MEDLINE, Sociological Abstracts, Social Services Abstracts, ProQuest Dissertations & Theses Global, ERIC, CINAHL, and Social Science Citation Index to identify studies published from inception to July 2024. We included observational studies (both longitudinal and cross-sectional) that measured violence against children with disabilities. The following terms were searched in titles, keywords, and abstracts using various combinations: (a) child*, kid, adolescent, teen*, youth, minor, infant; (b) violence, aggress*, adversity, trauma*, risk*, maltreat*, victimi*, abuse, bully*, neglect*, harass*, scam, fraud, dox*; and (c) physical, sensory, visual, intellectual, developmental, cognitive, mental, learning, attention deficit, disabilit*, disabl*, handicap*, impair*, disorder*, chronic ill, dyslexia. The electronic database search yielded 19,409 studies, which were scanned according to inclusion and exclusion criteria.
Inclusion and Exclusion Criteria
Studies were included if they met the following criteria: (a) measured violence perpetrated against children (aged ≤18 years) with disabilities; (b) reported specific disability types (e.g., vision loss) or specific disorders (e.g., mental health disorders); (c) provided clear definitions and measurement methods for violence; (d) used a quantitative research design and included children without disabilities as a comparison group; (e) reported prevalence, ORs, or raw data sufficient to calculate these outcomes; (f) published in English.
Studies were excluded if they: (a) were review articles, qualitative studies, or narrative studies; (b) focused primarily on other populations, such as adults (aged >18 years); (c) examined outcomes unrelated to violence (e.g., social challenges, educational outcomes); (d) lacked professionally diagnosed disabilities (e.g., self-reported depression); (e) focused on disabilities resulting from violence; (f) had data that were insufficient, unavailable, or not convertible for analysis. We manually contacted authors of published articles to obtain gray literature and missing data. Unpublished gray literature was excluded to ensure that all included sources had undergone at least some form of editorial or peer review, thus enhancing the reliability and transparency of the findings. After removing duplicates and screening abstracts based on the above criteria, a total of 19,188 studies were excluded, leaving 221 studies eligible for further full-text screening.
Quality Assessment and Data Extraction
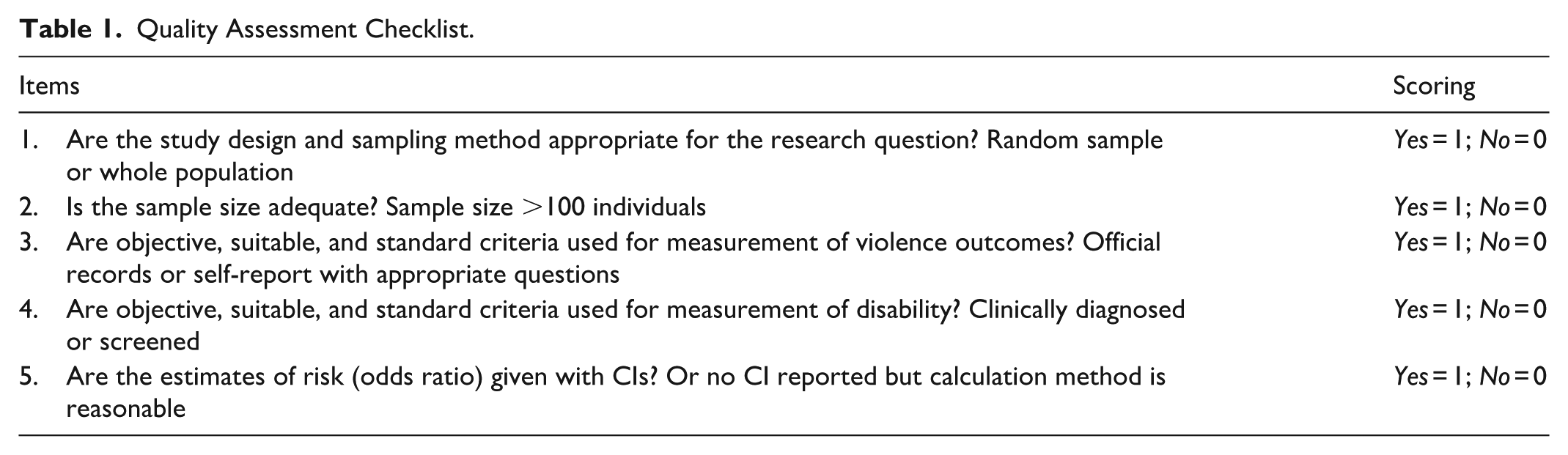
Studies were independently assessed for quality by two reviewers based on a modified quality assessment checklist (Table 1). The checklist contained five items covering key aspects of methodological rigor, including clarity of research objectives, appropriateness of study design, transparency in data collection methods, adequacy of data analysis, and consideration of potential biases. Each item was scored as 0 (not met) or 1 (met), yielding a total quality score ranging from 0 to 5 for each study. Studies scoring 4 or 5 were considered “high quality,” reflecting strong adherence to methodological standards. The results of the quality assessment are shown in Table 2. All of the studies received scores higher than 4, meaning that they provided data to compute effect sizes with satisfactory methodological quality. The average score of the included studies was 4.9, reflecting their high quality. No study was excluded in this process. Interrater reliability was computed using Cohen’s k and showed a high level of agreement (weighted k = 0.95).
Quality Assessment Checklist.
Study Characteristics.
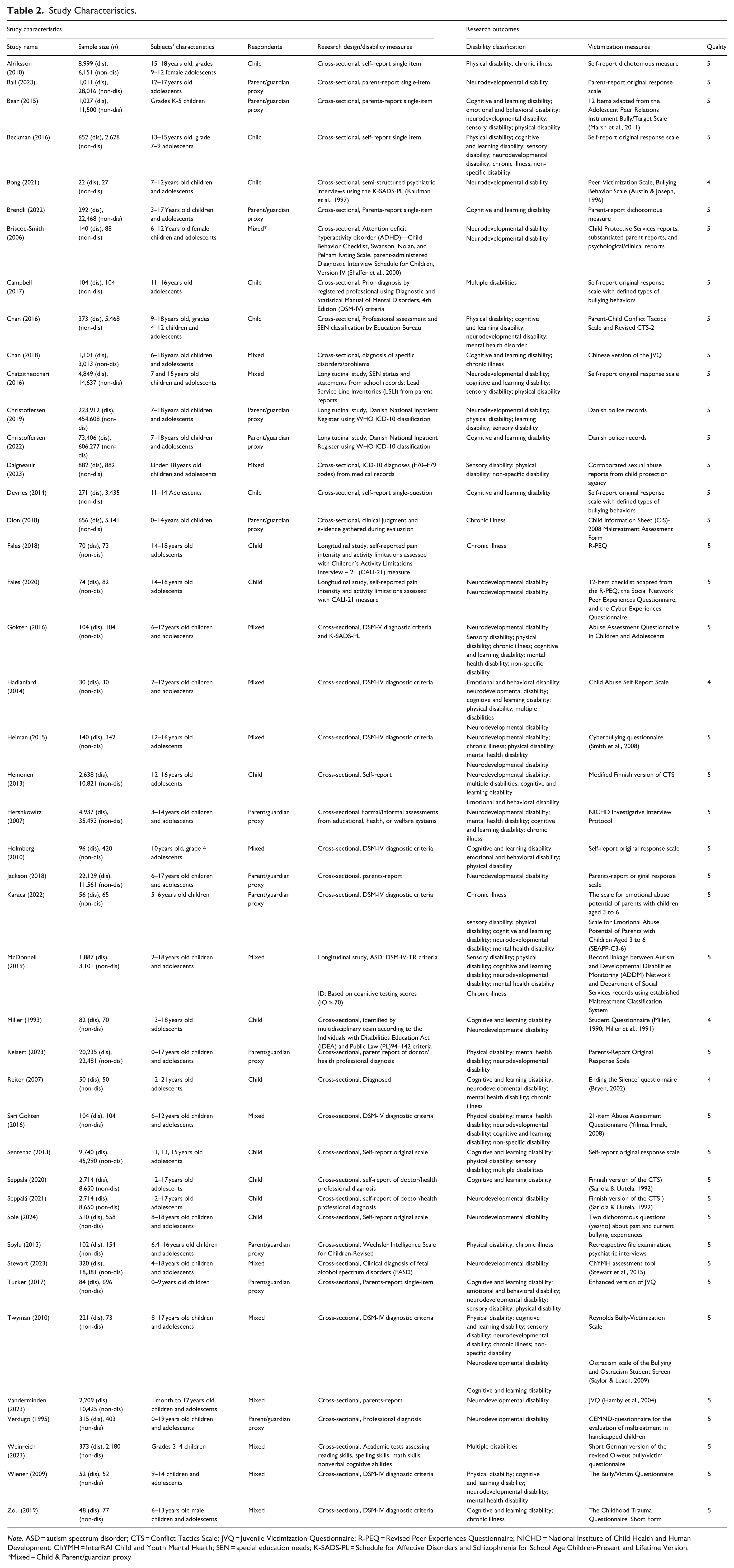
Note. ASD = autism spectrum disorder; CTS = Conflict Tactics Scale; JVQ = Juvenile Victimization Questionnaire; R-PEQ = Revised Peer Experiences Questionnaire; NICHD = National Institute of Child Health and Human Development; ChYMH = InterRAI Child and Youth Mental Health; SEN = special education needs; K-SADS-PL = Schedule for Affective Disorders and Schizophrenia for School Age Children-Present and Lifetime Version.
Mixed = Child & Parent/guardian proxy.
For each study, data were extracted by one reviewer and checked for accuracy by another. We developed a coding sheet in order to define the variables of each study. The items were coded as follows: (a) publication information (author[s] and year of publication); (b) study characteristics (country in which the study was conducted, sample size, subjects and respondents’ profiles [i.e., child or parent proxy], study design, and measures of disability); and (c) research outcomes (violence type and measurement instrument).
Subjects’ Characteristics and Outcome Measures
Table 3 summarizes the key characteristics of the subjects and the outcome measures of interest. Children with various disabilities were included across studies based on diverse definitions. When studies reported more than one type of disability or victimization, each type was independently classified into the relevant category, resulting in some studies appearing in multiple categories. Disability types were categorized as follows: chronic illness, cognitive and learning disabilities, emotional and behavioral disabilities, mental health disabilities, neurodevelopmental disabilities, physical disabilities, sensory disabilities, multiple disabilities, and non-specific disabilities. For example, autism spectrum disorder (ASD) without co-occurring intellectual disability was coded under “neurodevelopmental disabilities,” whereas ASD with intellectual disability was categorized as “multiple disabilities.” Additionally, all disabilities were further classified as either visible (e.g., cognitive and learning disability, physical disability) or invisible (chronic illness, emotional and behavioral disability, mental health disability, neurodevelopmental disability, sensory disability). We classified cognitive and learning disabilities as visible because, as noted by previous research (Chatzitheochari et al., 2016), students with these disabilities are often visibly identified due to their enrollment in special education programs or receipt of specialized educational support. Key outcomes of interest included bully-victimization, community and environmental violence, emotional violence, maltreatment, neglect, physical violence, sexual violence, polyvictimization, and non-specific violence (violence reported without specific categorization).
Key Characteristics of Subjects and Outcome Measures of Interest.
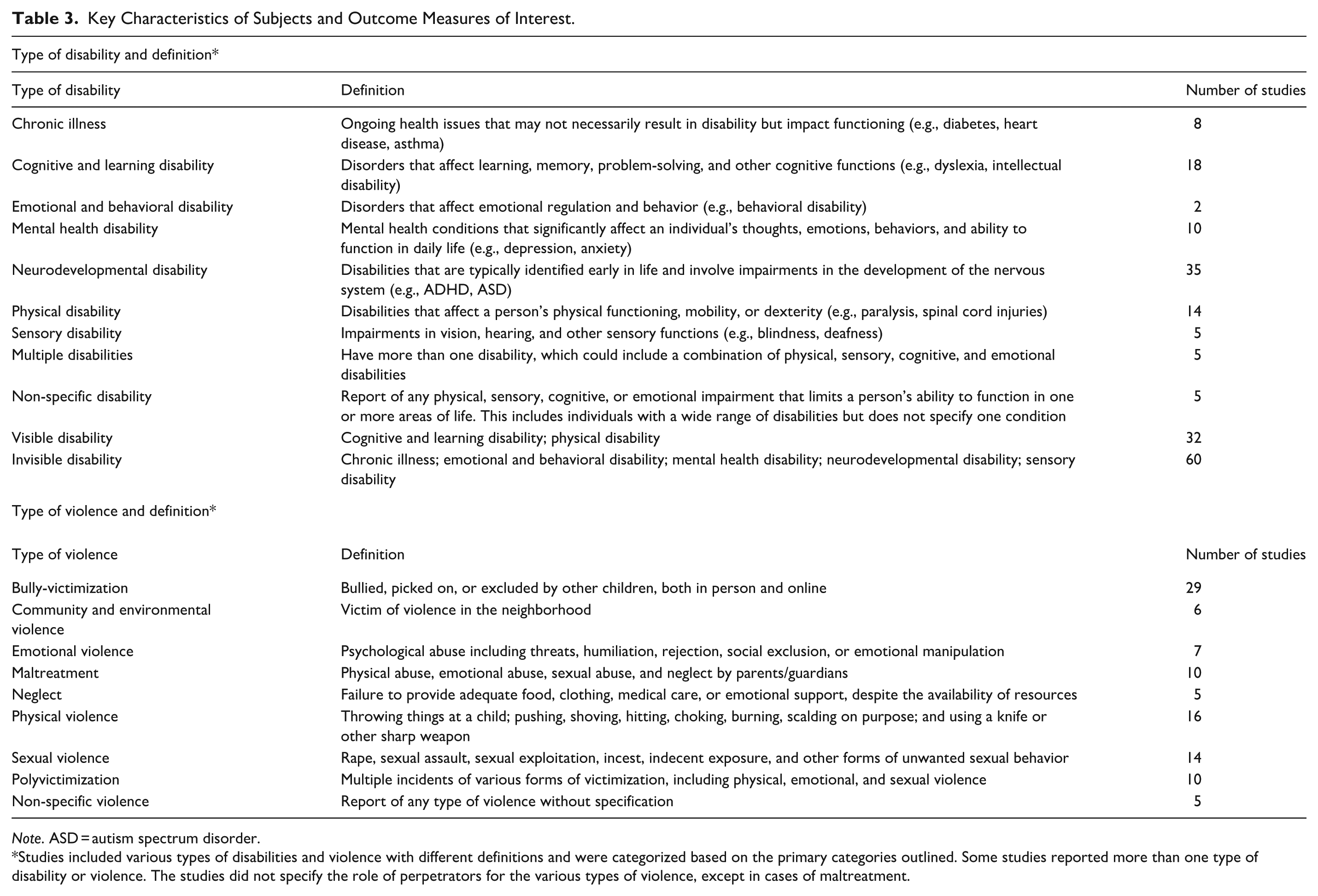
Note. ASD = autism spectrum disorder.
Studies included various types of disabilities and violence with different definitions and were categorized based on the primary categories outlined. Some studies reported more than one type of disability or violence. The studies did not specify the role of perpetrators for the various types of violence, except in cases of maltreatment.
Data Analysis
A crude OR and 95% CI were calculated to compare children with disabilities to children without disabilities. Pooled ORs with 95% CIs for the risk of violence were computed using a random-effects model (DerSimonian & Laird, 1986). Analyses were conducted with Comprehensive Meta-Analysis software (Version 4.0; Borenstein et al., 2021). Heterogeneity among studies was assessed using the I² statistic. Subgroup analyses were conducted to test differences in effect sizes within and between specific subgroups. For subgroup analyses by age, we defined preschool as 0 to 5 years, primary school as 6 to 11 years, and secondary school as 12 to 18 years. Publication bias was evaluated using multiple complementary approaches. Visual inspection of funnel plots was used to detect asymmetry, and Egger’s regression test was conducted to statistically assess small-study effects. In addition, the Trim and Fill method was applied to estimate the potential number of missing studies due to publication bias and to adjust the overall effect size accordingly.
Results
Study Characteristics
Figure 1 describes the study selection process. A total of 44 studies met the inclusion criteria. The study characteristics are summarized in Table 2. Across the 44 studies, sample sizes varied considerably. For children with disabilities, sample sizes ranged from 22 to 223,912. For children without disabilities, sample sizes ranged from 27 to 606,277. The total number of participants was 1,734,560, constituting a large sample for analysis. The included studies varied from large-scale, national registry-based research (Christoffersen, 2019, 2022) to smaller clinical samples (Bong et al., 2021).
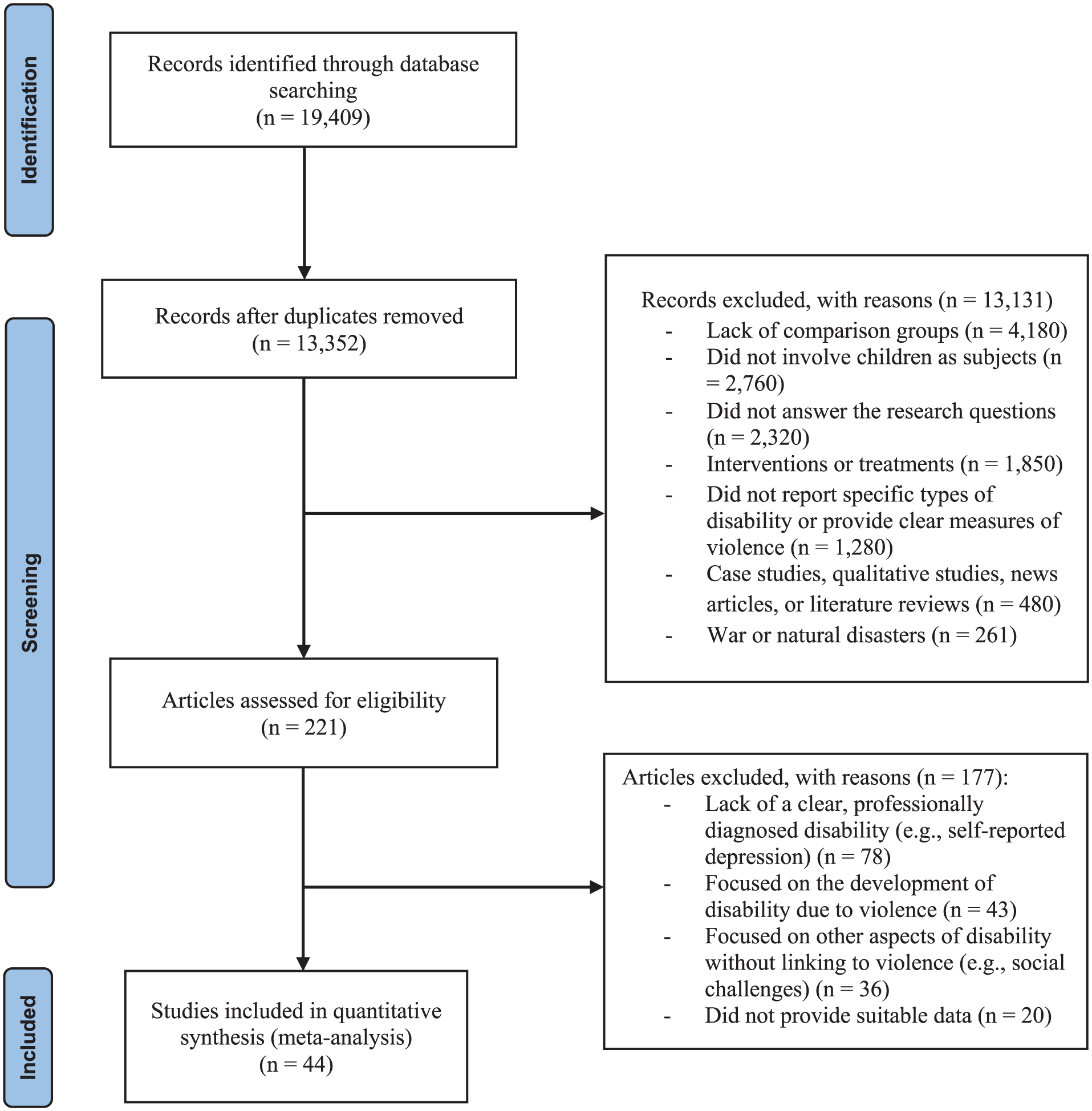
Summary of the search and article selection procedures.
Subjects’ ages ranged broadly from infants as young as 1 month to adolescents up to 18 years old, with one study including participants up to 19 years old (Verdugo, 1995). Most studies targeted children and adolescents aged 6 to 18 years. Among the included studies, three specifically focused on single-sex samples (Alriksson-Schmidt et al., 2010; Briscoe-Smith & Hinshaw, 2006; Zou et al., 2019), while the remaining studies included both male and female participants.
Victimization and disability data were collected primarily through two types of respondents across the 44 included studies. Specifically, 15 (34%) studies relied on child self-reports, 13 (29.5%) studies used parent or guardian proxy reports, and 16 (36.4%) studies employed mixed methods (i.e., both child and parent proxy respondents).
Regarding research design, 38 of the 44 (86.4%) studies were cross-sectional, and 6 (13.6%) employed longitudinal designs (Chatzitheochari et al., 2016; Christoffersen, 2019, 2022; Fales et al., 2018, 2020; McDonnell et al., 2019). Disability status was assessed using various methods: 13 (29.5%) studies used formal clinical diagnoses based on DSM-IV/V criteria, 13 (29.5%) relied on professional assessments by educational or healthcare professionals, and 18 (41%) employed single-item self-report or parent-report measures.
A variety of instruments were used to measure victimization. Nine (20.5%) studies employed original response scales in either self-report or parent-report formats. Four (9%) studies utilized the standardized Conflict Tactics Scale (CTS) (Chan et al., 2016; Heinonen & Ellonen, 2013; Seppälä et al., 2020, 2021), and three (6.8%) studies employed the Juvenile Victimization Questionnaire (Chan et al., 2018; Tucker et al., 2017; Vanderminden et al., 2023). Additionally, three studies (6.8%) used dichotomous yes/no measures for bullying or abuse (Alriksson-Schmidt et al., 2010; Brendli et al., 2022; Solé et al., 2024). The remaining 25 studies utilized various standardized or study-specific victimization tools tailored to specific contexts or populations.
Overall Violence and Overall Victimization
As shown in Tables 4 and 5, the overall OR of any violence type was 2.04 (95% CI [1.84, 2.52]) for children with disabilities compared to children without disabilities, under the random effect model. Over 99% of the total variation across studies was due to heterogeneity (I2 = 99.11%), which shows the wide variance in effect size.
Random-Effects Pooled Odds Ratios for Different Types of Disability in Relation to Overall Violence.
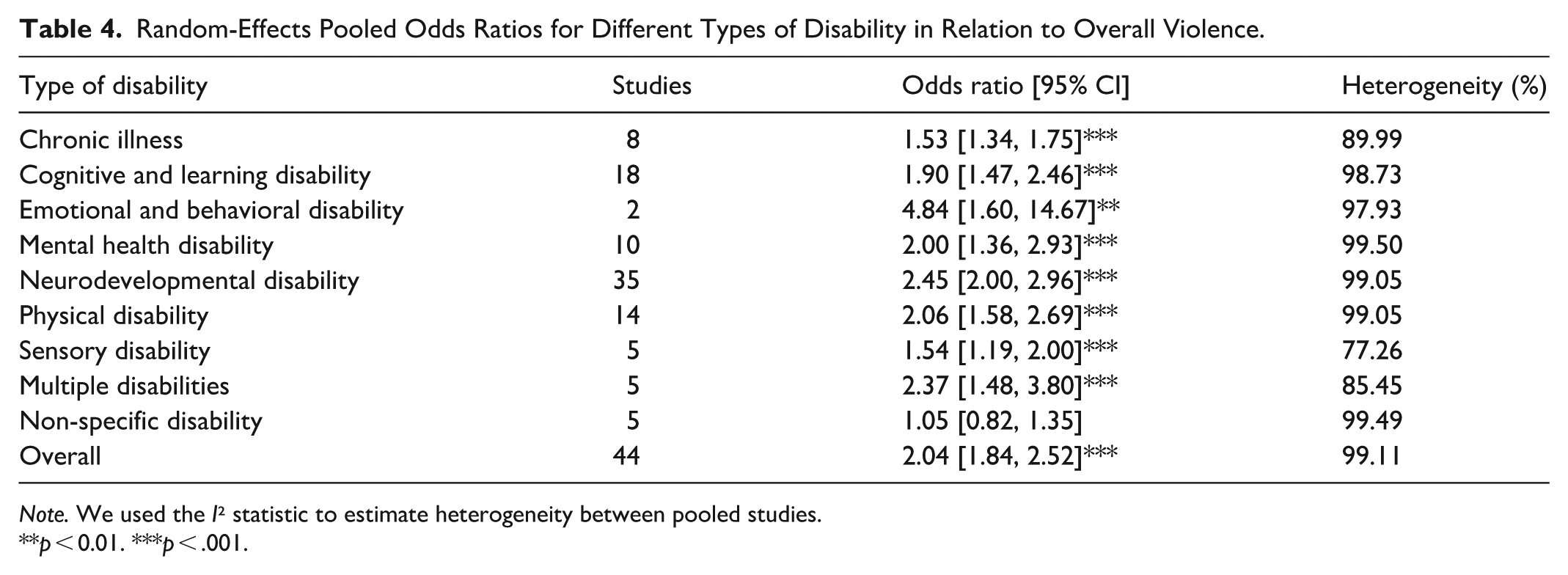
Note. We used the I² statistic to estimate heterogeneity between pooled studies.
p < 0.01. ***p < .001.
Random-Effects Pooled Odds Ratios for Different Types of Violence in Relation to Overall Disability.
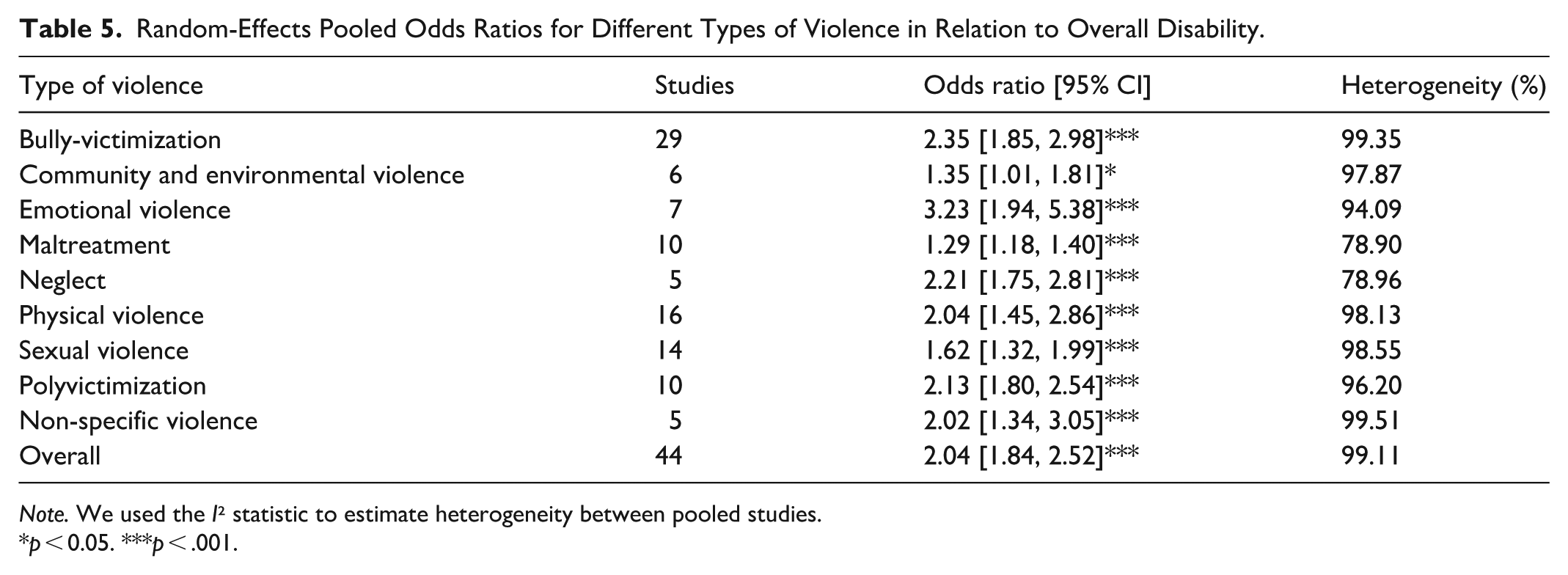
Note. We used the I² statistic to estimate heterogeneity between pooled studies.
p < 0.05. ***p < .001.
Table 4 presents the OR for victimization by disability category. All disability types were significantly associated with increased risk of violence, except for non-specific disabilities. Among these, risk of violence was raised in children with emotional and behavioral disabilities (4.84, 95% CI [1.60, 14.67]). Children with neurodevelopmental disabilities (2.45 [2.00, 2.96]), multiple disabilities (2.37 [1.48, 3.80]), and physical disabilities (2.06 [1.58, 2.69]) also demonstrated significant associations. Mental health disabilities, cognitive and learning disabilities, sensory disabilities, and chronic illnesses were similarly associated with increased victimization risk, with ORs equal or below 2. High heterogeneity was observed across disability categories, with I² values ranging from 77.26% (sensory disabilities) to 99.50% (mental health disabilities).
Table 5 shows the OR for different types of violence in relation to overall disability. All types of violence examined were significantly associated with disability. An increased risk of emotional violence was shown in children with disabilities compared with controls (3.23, 95% CI [1.94, 5.38]), followed by bully-victimization (2.35 [1.85, 2.98]), neglect (2.21 [1.75, 2.81]), polyvictimization (2.13 [1.80, 2.54]), and physical violence (2.04 [1.45, 2.86]). Community and environmental violence, maltreatment, sexual violence, and non-specific violence were also significantly associated with disabilities, with ORs ranging from 1.50 to 1.95. Substantial heterogeneity was shown across violence types, with I² values ranging from 78.90% (maltreatment) to 99.51% (non-specific violence).
Table 6 describes the associations between violence types and disability visibility (visible, invisible, and multiple disabilities). For children with visible disabilities, significant associations were found across all violence types examined. The association with non-physical violence showed an OR of 2.24 (95% CI [1.51, 3.33]). Polyvictimization (2.04 [1.42, 2.93]) and physical violence (1.84 [1.37, 2.45]) also demonstrated significant associations.
Random-Effects Pooled Odds Ratios for Invisible/Visible Disability, Physical/Non-Physical Violence, and Polyvictimization.
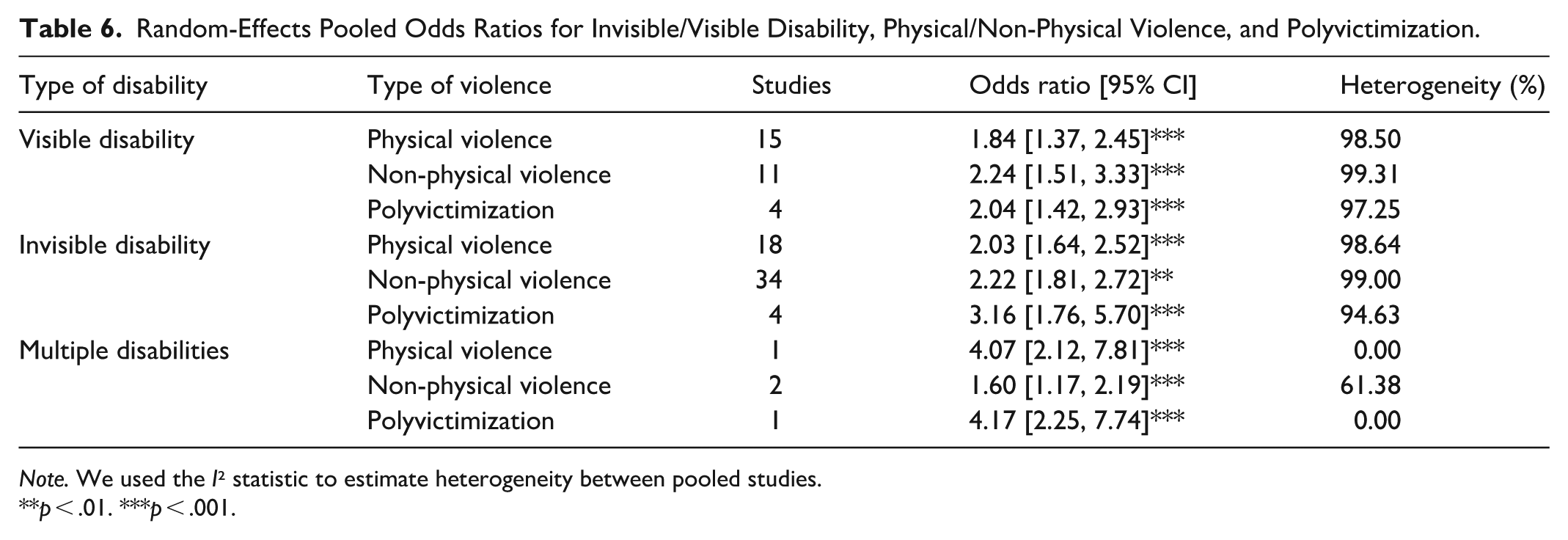
Note. We used the I² statistic to estimate heterogeneity between pooled studies.
p < .01. ***p < .001.
For children with invisible disabilities, risk of polyvictimization was raised (3.16, 95% CI [1.76, 5.70]). Invisible disabilities were also significantly associated with non-physical violence (2.22 [1.81, 2.72]) and physical violence (2.03 [1.64, 2.52]).
Children with multiple disabilities also exhibited increased risk of polyvictimization (4.17, 95% CI [2.25, 7.74]) and physical violence (OR = 4.07 [2.12, 7.81]). A significant association was observed for non-physical violence as well (1.60 [1.17, 2.19]).
Heterogeneity remained consistently high across most categories, ranging from 61.38% (non-physical violence among multiple disabilities) to 99.31% (non-physical violence among visible disabilities).
Subgroup Analyses
Table 7 shows subgroup in associations between overall disability and overall victimization. Significant subgroup differences were identified based on geographical region and study design. Specifically, analyses indicated significant regional variation (p < .001), with the highest odds of victimization observed in Oceania (2.68, 95% CI [2.34, 3.07], k = 1), followed by Asia (2.63 [1.68, 4.11], k = 12), North America (2.37 [1.91, 2.92], k = 18), and Europe (1.78 [1.50, 2.12], k = 12). The single study from Africa showed non-significant results. Significant differences were also found based on study design (p < .001), with cross-sectional studies (2.24 [1.84, 2.73]) reporting significantly higher associations than longitudinal studies (1.32 [1.07, 1.63]).
Subgroup Analysis of the Association Between Overall Disability and Overall Victimization (n = 44).
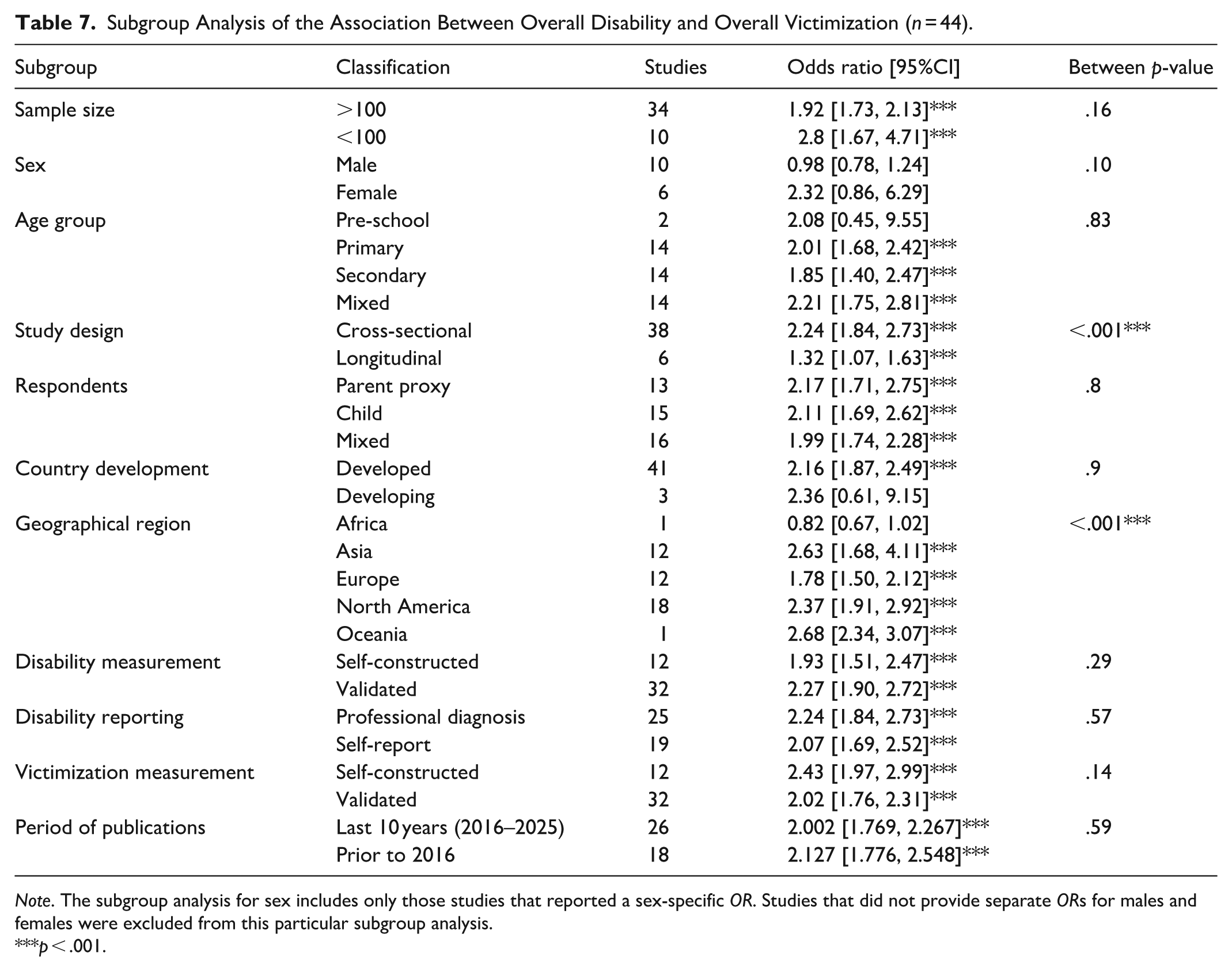
Note. The subgroup analysis for sex includes only those studies that reported a sex-specific OR. Studies that did not provide separate ORs for males and females were excluded from this particular subgroup analysis.
p < .001.
No significant subgroup differences emerged in analyses based on sex (p = .10), age group (p = .83), or country development status (p = .90). Additionally, methodological factors including sample size (p = .16), type of respondents (p = .80), disability measurement (p = .29), disability reporting (p = .57), victimization measurement approaches (p = .14), and period of publications (p = .59) also showed no significant between-group differences.
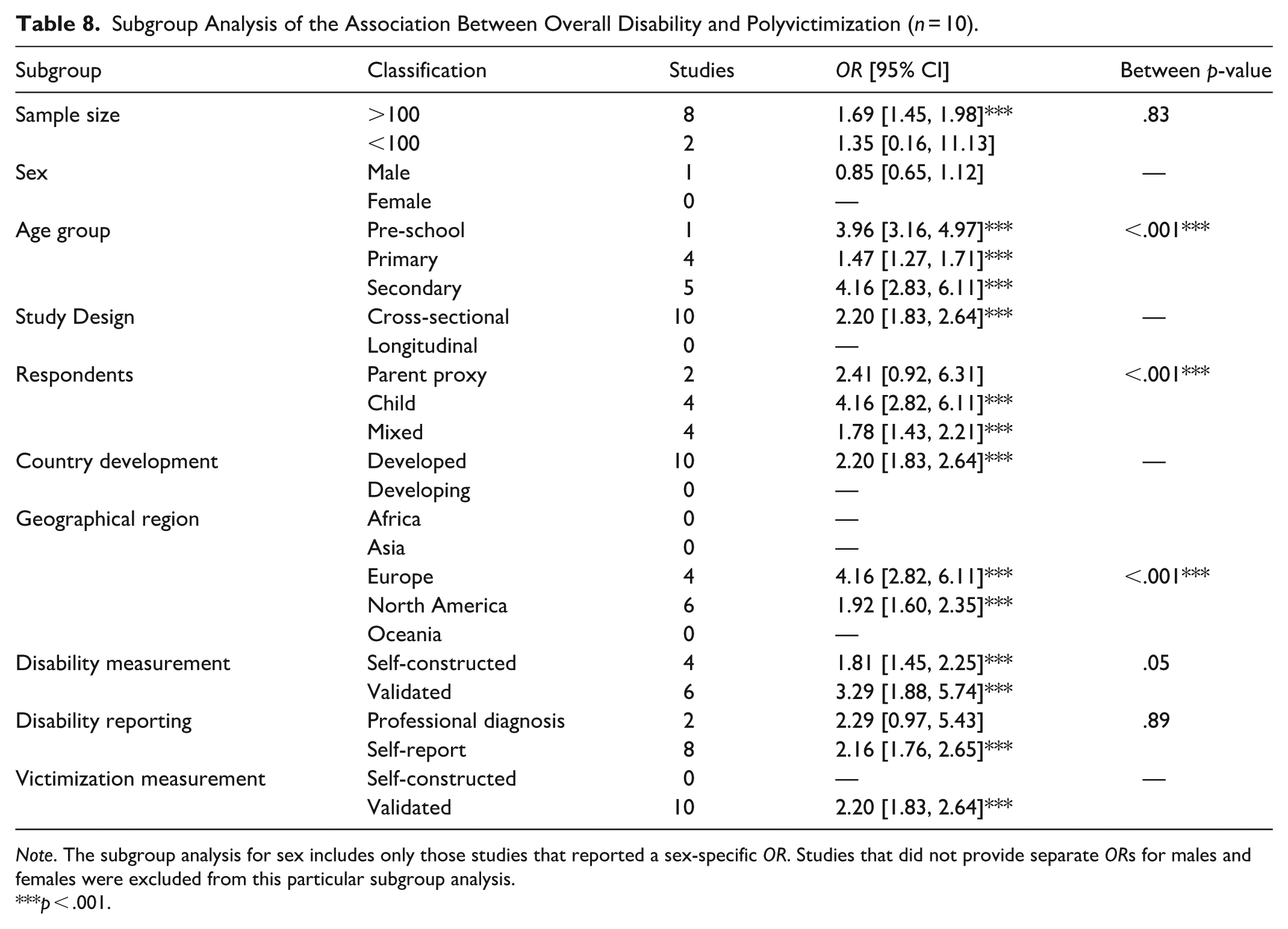
The above pattern is similar to overall disability and victimization, but a different pattern is observed in the association of overall disability and polyvictimization. As shown in Table 8, age groups showed significant differences for polyvictimization (p < .001), with secondary-aged children having the highest odds (4.16, 95% CI [2.83, 6.11]), followed by pre-school children (3.96 [3.16, 4.97]). Primary-aged children showed relatively lower odds (1.47 [1.27, 1.71]).
Subgroup Analysis of the Association Between Overall Disability and Polyvictimization (n = 10).
Note. The subgroup analysis for sex includes only those studies that reported a sex-specific OR. Studies that did not provide separate ORs for males and females were excluded from this particular subgroup analysis.
p < .001.
Significant subgroup differences also emerged based on respondents for polyvictimization (p < .001). Child self-reports indicated the highest odds (4.16, 95% CI [2.82, 6.11]), followed by mixed respondents (1.78 [1.43, 2.21]). Parent proxy reports showed elevated but statistically non-significant odds (2.41 [0.92, 6.31]).
Additionally, geographical regions revealed significant variability (p < .001). European studies showed higher odds of polyvictimization (4.16, 95% CI [2.82, 6.11]) compared to North American studies (1.92 [1.60, 2.35]). However, there were no studies from Africa, Asia, or Oceania examining polyvictimization.
While disability measurement approaches approached significance (p = .05), no significant differences were found for sample size (p = .83) or disability reporting type (p = .89). Subgroup analyses for sex, study design, country development status, victimization measurement, and period of publications could not be conducted due to insufficient data.
Publication Bias
We used funnel plots to examine the publication bias. Most of the studies were distributed symmetrically around the combined effect size, as shown in Figure 2. A substantial number of studies clustered at the top-center of the graph, indicating high precision, while only a few were located toward the bottom. This symmetrical distribution suggests that the possibility of publication bias is low. The Duval and Tweedie Trim-and-Fill analysis further confirmed this interpretation, showing that no studies were trimmed or imputed.
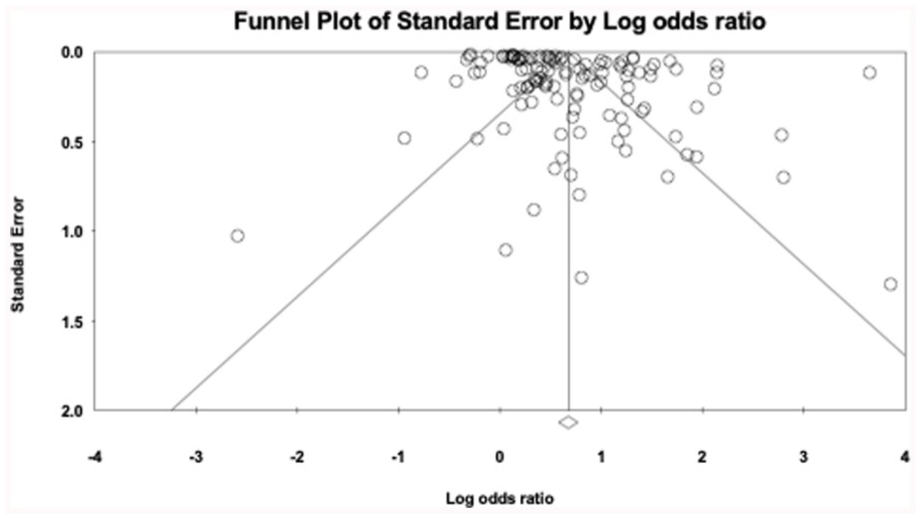
Funnel plot of standard error by log odds ratio.
Discussion
As research on violence against children with disabilities continues to expand, the current meta-analysis offers a more up-to-date and detailed examination of the risks associated with specific types of violence and different disability categories. Our findings indicate that children with disabilities face approximately twice the risk of experiencing violence compared to their non-disabled peers (OR = 2.04). This seems to be lower than the estimate reported in the 2012 meta-analysis by Jones et al. (OR = 3.68) but closely aligns with the more recent findings of Fang et al. (OR = 2.08). Compared to previous meta-analyses, our study incorporates a broader global sample and includes a wider range of disability and victimization types, including multiple disabilities and polyvictimization, which may contribute to more moderate, yet still concerning, effect sizes. Additionally, our inclusion criteria were more stringent with respect to diagnostic clarity and methodological quality, which may have resulted in a more conservative estimate. Nevertheless, the elevated risk of violence remains clear, highlighting the global urgency of addressing this issue through increased awareness, policy attention, and targeted interventions.
Consistent with previous results, we also found that children with all identified forms of disabilities experienced higher levels of violence (Fang et al., 2022). Specifically, children with multiple disabilities and those with invisible disabilities were particularly at risk for polyvictimization (OR = 4.17 and OR = 3.16, respectively), a pattern that aligns with cumulative risk models (Burchinal et al., 2000; Evans et al., 2013). These children may face overlapping disadvantages, such as greater dependency on caregivers, impaired communication, and increased social isolation, which elevate their exposure to repeated or concurrent forms of violence (Emerson & Hatton, 2007).
We also analyzed the visibility of disabilities and its relationship with victimization. The results reveal that both visible and invisible disabilities are significantly associated with high risks of physical violence, non-physical violence, and polyvictimization. The association between visible disabilities and victimization may be partly explained by the social stigma and discrimination attached to children with apparent physical differences, which can increase their exposure to bullying, social exclusion, and targeted aggression (Carter & Spencer, 2006). However, we note that the categorization of visible and invisible disabilities is exploratory and lacks a consistent definition. Our findings should therefore be viewed as preliminary, offering an indication that visibility may influence effect sizes and pointing to a potential direction for future research.
Importantly, invisible disabilities have the strongest association with polyvictimization (OR = 3.16). While these disabilities may not be outwardly apparent, they can affect communication, emotional regulation, or behavior, potentially leading to social misunderstandings, peer rejection, or punitive responses from caregivers (Kendall & Kessler, 2002). Similarly, children with multiple disabilities experienced markedly increased risk for polyvictimization (OR = 4.17), reflecting the cumulative challenges they face, as discussed in cumulative risk theory.
Additionally, our results revealed that children with disabilities are at significantly higher risk for all specific types of violence examined. Notably, polyvictimization was associated with a more than twofold increase in risk (OR = 2.13), suggesting the profound vulnerability of children with disabilities to cumulative victimization experiences. This finding is particularly concerning given that polyvictimization has been linked to more severe and problematic psychological, behavioral, and developmental consequences than exposure to a single form of violence (Finkelhor et al., 2007). Thus, children with disabilities are not only more likely to experience violence but are disproportionately subjected to multiple, co-occurring forms of victimization. The intersection of multiple vulnerabilities, such as functional impairments, dependency, and limited protective capacity, may explain this heightened exposure across diverse settings (Baumgardner, 2019; Fisher et al., 2016; Vanderminden et al., 2023).
Factors Affecting the Overall Effect Size
The subgroup analyses revealed several factors that may influence the magnitude of the association between disability and victimization. In terms of target characteristics, no significant differences were found based on sex or age group in the overall association between disability and violence. However, in the analysis of polyvictimization, age-related differences became significant, with adolescents in the secondary school age group exhibiting the highest odds. This may be due to their wider exposure to multiple social environments (e.g., school, community, online platforms), where risks of cumulative victimization are higher. It is worth noting that the insignificant findings should not be interpreted as evidence that sex and age have no impact on overall OR. Rather, the consistently heightened risk across subgroups suggests that disability itself may be a particularly robust and overriding predictor of victimization risk. Therefore, one should be cautious when concluding that sex and age are unrelated to the overall effect of disability on victimization based solely on the present findings.
Geographically, country development level did not significantly moderate the overall effect, but differences emerged across world regions, with higher odds reported in Asia, North America, and Oceania, and lower odds in Europe and Africa. Given the very small number of studies from Africa and Oceania, these subgroup estimates should be interpreted with caution as they are underpowered for meta-analytic conclusions. More importantly, these areas appear to be critically understudied, possibly due to structural research barriers, publication bias, or data collection challenges. As a result, current estimates may reflect sampling and publication gaps rather than genuine differences in risk. More research is urgently needed in underrepresented regions to better assess global disparities in violence against children with disabilities.
In terms of methodological factors, study design had a significant impact on effect sizes. Cross-sectional studies tended to report higher odds of victimization than longitudinal studies, possibly due to differences in measurement timing. Notably, all studies on disability and polyvictimization were cross-sectional. Thus, subgroup comparisons by study design were not possible for that specific outcome, underscoring the need for future longitudinal research to examine cumulative and time-based patterns of victimization.
An especially important finding relates to the source of information. Studies using child self-reports consistently yielded higher odds of reported victimization, than those relying on parent-proxy reports, especially for polyvictimization. This supports prior evidence suggesting that caregivers may be unaware of or underreport children’s experiences of violence (Chan, 2015). Given the sensitive nature of abuse and the potential for concealment or misinterpretation, our results emphasize the value of incorporating direct child perspectives in both research and practice to avoid underestimation of victimization. Policymakers and practitioners should be cautious about relying solely on adult proxies when designing assessments, interventions, or reporting mechanisms.
Finally, although differences in measurement tools and sample size were not statistically significant in the subgroup analyses of overall disability and polyvictimization, we did find a marginally significant difference (p = .05) in the subgroup analysis comparing validated vs. self-constructed disability measures. Studies using validated measurement tools tended to report larger effect sizes than those relying on author-constructed or unvalidated instruments. This suggests that higher-quality measurement may be more sensitive in detecting the true association between disability and victimization. Future research should therefore prioritize standardized and validated assessment tools to improve data reliability and cross-study comparability.
Despite subgroup analyses accounting for certain moderators, considerable heterogeneity remained across studies. This likely reflects the broad diversity in sample populations (e.g., age, disability types, geographic regions), measurement tools for both disability and violence, and study designs (e.g., cross-sectional vs. longitudinal). Such variability, while expected in a global meta-analysis, complicates direct comparisons and highlights the need for greater standardization in future research.
Strengths and Implications
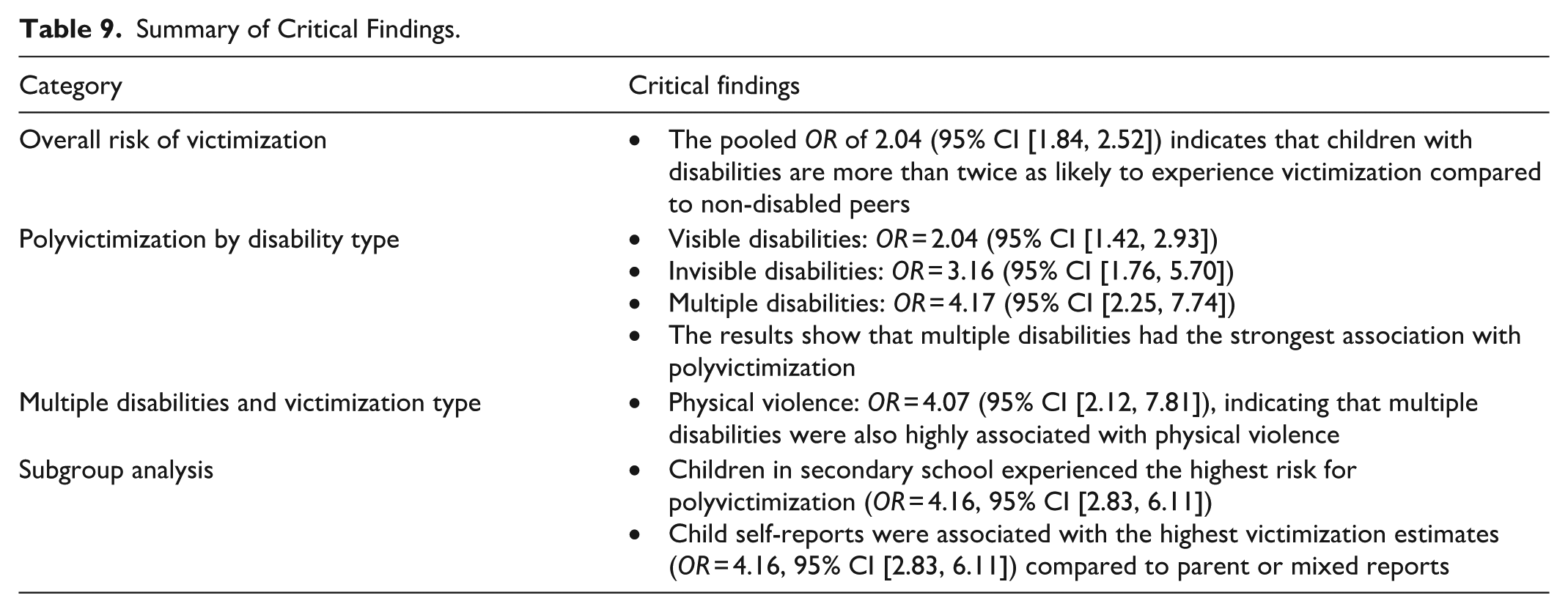
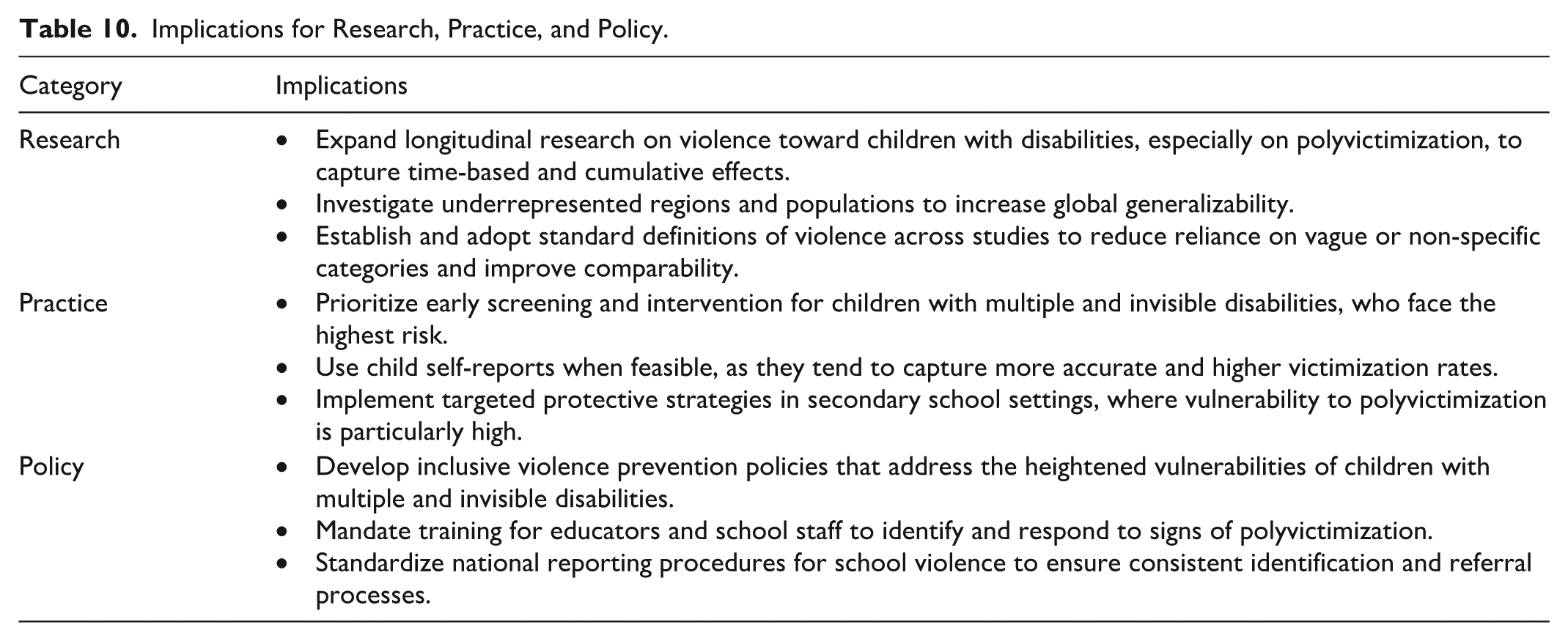
Critical findings and implications of the study are summarized in Tables 9 and 10. This meta-analysis offers important advancements over previous reviews by providing a more detailed and nuanced understanding of the association between disability and victimization among children. While earlier meta-analyses established a general link between disability and increased violence risk, the current study extends this work by analyzing a broader range of disability types and a wider spectrum of violence, particularly highlighting the risks associated with multiple disabilities and polyvictimization. These groups emerged as especially vulnerable, underscoring the compounded risks faced by children with complex or overlapping challenges.
Summary of Critical Findings.
Implications for Research, Practice, and Policy.
A further unique contribution of this study is its examination of visible and invisible disabilities in relation to polyvictimization. This analysis is especially meaningful in practice. Unlike clinical categories that require professional diagnosis, visible disabilities are often immediately apparent to educators, caregivers, or community members, allowing for earlier recognition and protection. In contrast, invisible disabilities are more easily overlooked or misunderstood, despite our findings showing that they are strongly associated with polyvictimization and other forms of violence. These results underscore the urgent need for greater vigilance among health professionals, educators, and child protection workers. Early identification and intervention efforts should not rely solely on formal diagnoses but also consider behavioral cues and functional challenges that may signal hidden vulnerabilities.
By presenting robust overall effect sizes and offering disaggregated analyses by disability type and victimization subtype, this study provides valuable evidence to inform targeted violence prevention and response strategies. The findings emphasize the importance of screening for multiple forms of abuse and recognizing the intersectionality of disabilities when assessing children’s risk. In doing so, the current meta-analysis not only addresses key shortcomings of prior research but also contributes actionable insights that can improve the safety and well-being of children with disabilities across diverse settings.
Limitations and Future Research
Despite the strengths of this meta-analysis, several limitations should be acknowledged. While the majority of studies provided clear and specific definitions of disability, a small portion of the research (n = 5) reported non-specific disability categories without identifying the nature, type, or severity of impairment. This lack of clarity may introduce heterogeneity into the findings and limit the precision of subgroup analyses in the present study. Substantial heterogeneity also remained across studies, even after accounting for potential moderators. This likely reflects differences in study populations, measurement instruments, and methodological designs. While random-effects models addressed this variability to some extent, it may still influence the interpretability and generalizability of the pooled estimates.
Another key limitation is the predominance of cross-sectional data among the included studies, which limits the ability to establish causal relationships between disability and violence exposure. Longitudinal research is needed to better understand the temporal sequencing and potential bidirectionality of these associations. Additionally, while some types of violence, such as bully-victimization, community violence, and maltreatment, were well-defined and often clearly distinguished as intra- or extra-familial, other forms of violence lacked this level of specificity. This issue was particularly pronounced in the case of polyvictimization, where many studies reported multiple types of victimization but did not clarify the relationship to the perpetrator or context of abuse. The failure to differentiate between familial and non-familial violence may obscure important nuances in how children with disabilities experience harm, limiting the ability to tailor prevention and intervention strategies to specific risk settings. Future research would benefit from adopting standardized and comprehensive definitions of both disability and violence to enhance comparability across studies and improve the precision of meta-analytic estimates.
Finally, we restricted inclusion to articles published in English, which may have introduced language bias and underrepresented non-English-speaking regions. This could skew geographic representation and limit the global generalizability of findings. Future meta-analyses would benefit from broader language inclusion to ensure a more comprehensive synthesis of international evidence. Additionally, some geographic subgroup analyses were based on a small number of studies (e.g., Africa and Oceania), resulting in underpowered comparisons. Thus, the estimates derived from these subgroups should be interpreted cautiously. Future research should aim to include sufficient data from underrepresented regions to allow for more robust and meaningful geographic subgroup analyses.
Conclusion
This meta-analysis provides the most comprehensive and up-to-date synthesis of the relationship between disability and victimization among children. By examining a wide range of disability categories, including multiple, visible, and invisible disabilities, and analyzing diverse forms of violence such as polyvictimization, the study offers critical insights into populations at highest risk. Our findings highlight the urgency of developing targeted prevention and intervention strategies that account for the complexity and diversity of disability experiences. At the same time, the results underscore the need for more rigorous, standardized, and inclusive research, particularly longitudinal studies and those conducted in underrepresented regions, to better understand contextual and causal pathways. To translate evidence into impact, policymakers and practitioners must prioritize inclusive child protection frameworks that actively identify, monitor, and support children with disabilities across settings. Embedding disability-informed approaches into violence prevention, education, and social services is essential to safeguarding the rights, dignity, and well-being of this vulnerable population worldwide.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work described in this paper was supported by a grant from the Research Grants Council of the Hong Kong Special Administrative Region, China (Project Number PolyU 15601022) and APSS Research Fund (P0046000).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.