
Abstract
Elder neglect is one of the most common forms of abuse of older people that usually receives little attention. Existing studies on elder neglect vary widely in their definitions, methods, and reported prevalence. By synthesizing this heterogeneous evidence, a systematic review can provide a more accurate and comprehensive understanding of the scope of the problem, identify consistent risk factors, and reveal gaps in current research. This systematic literature review aimed to determine the prevalence and risk factors of elder neglect. A comprehensive literature search was conducted in PubMed, Web of Science, the Cochrane Library, and Scopus up to January 2026 for studies published in the English language measuring the prevalence and risk factors of neglect in older adults. The quality of the evidence was assessed by two reviewers independently using the Joanna Briggs Institute (JBI) Critical Appraisal Tools. A total of 109 studies were included in this review. The prevalence rates of neglect among older adults ranged from –0.2% to 86.9%. The risk factors of neglect identified by these studies involved sociodemographic characteristics, health-related characteristics, psychological and social characteristics. Neglect is a widespread and often overlooked issue among older adults living in the community, with only a small portion being identified. Our review offers healthcare professionals insight into neglect and its risk factors, aiding in the development of social policies to prevent elder neglect. Also, this review informs stakeholders, guiding prevention, caregiver support, resource allocation, and research to improve elder neglect detection and intervention. These include social workers, caregivers (both formal and informal), policymakers, public health practitioners, community organizations, and researchers.
Introduction
The rapid aging population is becoming a marked worldwide social phenomenon. As populations around the world continue to age over the next several decades, abuse and neglect among older adults is expected to increase exponentially (Mydin et al., 2021). According to the World Health Organization (WHO, 2024), nearly one in six people aged 60 years and older experience some form of abuse in community-based settings. Indeed, the issue of abuse of older people and neglect has been deemed to have the “potential for becoming an epidemic” (Fearing et al., 2017). Both the WHO and the U.S. Centers for Disease Control and Prevention define abuse directed at older adults aged 60 years and older as an intentional single or repeated act, or failure to act that cause or create a risk of harm or distress to the older person. Common types of abuse include emotional or psychological abuse, physical abuse, sexual abuse, financial abuse or exploitation, and neglect or abandonment (Centers for Disease Control and Prevention, 2024; World Health Organization, 2024).
Neglect is the inability of older adults or their caregivers to meet basic needs, due to physical or mental impairment or diminished capacity, to perform essential self-care tasks. These needs include food, water, shelter, clothing, hygiene, and essential medical care (Centers for Disease Control and Prevention, 2024). A more general definition has been proposed: neglect points to the intentional and unintentional withholding of necessities that results in the older person’s failure to thrive, consistent with current conceptions of neglect as a failure to satisfy need, rather than the presence of abuse (Levine, 2003). Unintentional neglect in caregivers may stem from either ignorance or from the genuine inability to provide care, caregiver burden, and intentional neglect occurs when a caregiver deliberately fails to fulfill caretaking responsibilities, causing harm to older adults (Andela et al., 2021). Based on evidence, neglect is the most commonly reported form of mistreatment and abuse, which is considered a critical medical and social problem (Yu et al., 2021; Zawisza et al., 2020). A systematic review by Cooper et al. (2008) found that the prevalence of elder abuse and neglect worldwide ranged from 3.2% to 27.5%, whereas the prevalence in developing nations was reported to be from 13.5% to 28.8% (Sooryanarayana et al., 2013). Other research reported a prevalence of neglect ranging from 24% to 87% (Cohen et al., 2010; Griffore et al., 2009). In a systematic review and meta-analysis of 52 studies across 28 countries, the pooled elder neglect prevalence rate in community settings was 4.2% (Yon et al., 2017).
Neglect among older adults is associated with a range of negative physical and psychological health consequences from minor injuries to permanent disabilities, including depression, anxiety, posttraumatic disorder, increased risk of hospitalization, increased risk of morbidity, poorly controlled chronic diseases such as hypertension, diabetes, and heart disease, decreased quality of life, and premature death (Adib et al., 2020; Yunus et al., 2019). In addition, neglect is related to societal consequences such as loss of trust or quality of relationships, social isolation, increasing cost of care, increasing burden, and a negative impact on families and society (Atim et al., 2023; Aylaz et al., 2020; X. Dong et al., 2013; Yon et al., 2017). Existing literature demonstrates that neglect in older people is associated with multiple interrelated risk factors operating at individual, caregiver, and social levels (Acierno et al., 2017; Johannesen & LoGiudice, 2013; Lachs & Pillemer, 2015; X. M. Wang et al., 2015). Individual-level risk factors include advanced age, cognitive impairment, dementia, functional dependence, and chronic physical or mental health conditions (X. Q. Dong, 2015; Pillemer et al., 2016). Caregiver-related factors such as caregiver burden, psychological distress, inadequate caregiving skills, and substance misuse have also been consistently linked to a higher likelihood of neglect (Beach et al., 2005; Cooper et al., 2008). Furthermore, social and contextual factors—including social isolation, low socioeconomic status, poor family relationships, and limited access to formal support services—have been shown to increase vulnerability to neglect among older adults (Pillemer et al., 2016; World Health Organization, 2015).
Considering the increasing number of older adults, the experience of neglect and its negative effects are likely to become more prominent. A systematic review is essential to address variability in definitions, methods, and prevalence, providing a clearer understanding of elder neglect, identifying consistent risk factors, research gaps, and evidence-based guidance for prevention, policy, and practice.
Although multiple systematic reviews have explored the abuse of older people—highlighting wide variation in prevalence estimates and various associated risk factors—there remains a significant gap in research specifically addressing elder neglect. Early reviews primarily focused on overall abuse of older people rather than neglect specifically and often pooled different forms of abuse, limiting the ability to draw conclusions about neglect as a distinct phenomenon (Cooper et al., 2008; Pillemer et al., 2016). More recent reviews have provided global prevalence estimates and highlighted methodological heterogeneity across studies; however, they have either included neglect as a secondary outcome or restricted their analyses to specific settings or populations (Burnes et al., 2015; Yon et al., 2017). In contrast, the present review focuses exclusively on elder neglect, systematically analyzing its prevalence and risk factors. It also updates the evidence base by including studies published up to January 2026 and applies a comprehensive search strategy along with Critical Appraisal Tools (Joanna Briggs Institute [JBI]) across all study designs, enhancing methodological rigor. Together, these features distinguish our review and offer a more focused and current understanding of elder neglect. The research question was to review the spectrum of prevalence of neglect in the elderly and its associated factors worldwide. Therefore, the aim of this systematic review was to answer the research question using English literature on neglect in the elderly worldwide.
Methods
Study Eligibility Criteria and Selection
The inclusion criteria were primary studies that recruited older adults aged 60 years old or above as their participants, outcomes were any reported prevalence and determinants of elder neglect and self-neglect; written in English; used any type of quantitative research design, such as cross-sectional, descriptive, and cohort studies, and published between January 1980 and January 2026. Articles were excluded if they were qualitative studies, systematic reviews, randomized control trials, experimental studies, case reports, conference proceedings, only abstracts, commentaries, editorials, reviews, newsletters, and research protocols. In this review, we focused primarily on peer-reviewed studies published in scientific journals. Therefore, gray literature (e.g., dissertations, conference abstracts, government reports, unpublished manuscripts) was not systematically searched. Our decision was based on the need to ensure methodological rigor, comparability of study quality, and consistency in risk-of-bias assessment using standardized appraisal tools (JBI).
Study Design and Search Strategy
The current review was conducted as per the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021). Following the Peer Review of Electronic Search Strategies statement (Sampson et al., 2016), electronic searches were conducted by a health sciences librarian for eligible studies in each of the following databases: PubMed, Scopus, Web of Science, and Cochrane Library. For additional studies, citation and reference searches were conducted for eligible articles, and associated authors were checked for further relevant research. The top journals identified from the comprehensive searches were the Journal of Elder Abuse and Neglect, Clinics in Geriatric Medicine, the Journal of the American Geriatrics Society, the Journal of Adult Protection, and Trauma, Violence, and Abuse. In addition, we performed, a “snowball” search to recognize additional studies by searching the reference lists of publications eligible for full-text review and using Google Scholar to identify and screen them (up to January 1, 2026).
The search terms and their combinations were chosen after a sensitivity test on many possible free-text sentences, keywords, and MeSH terms. Then search terms were framed a priori, using Boolean logic. Additional search terms were included in consultation with an information specialist (librarian) who has extensive experience in systematic reviews. Some of the search terms include: “elder neglect,” “older adults,” “aged,” “elderly,” “seniors,” “abuse,” “neglect,” “self-neglect,” “mistreatment,” “maltreatment,” “intimate partner violence,” “violence,” “anger,” “hostility,” “conflict,” “prevalence,” “incidence,” and “epidemiology.” This phase of the study screening yielded a total of 13,541 articles (Figure 1).
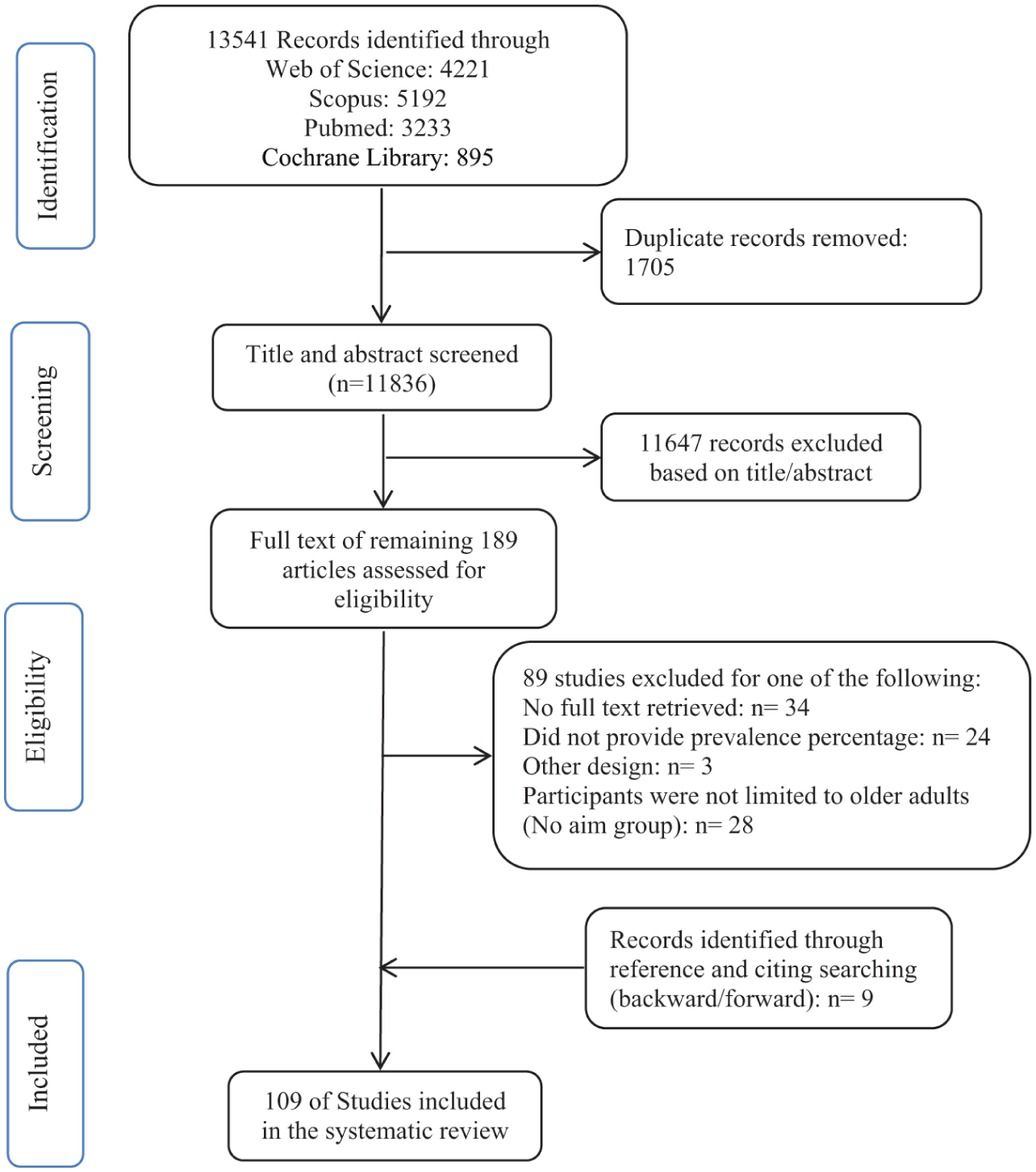
PRISMA flow diagram detailing the search strategy.
Screening the Full Text and Synthesis
All records of respective databases were downloaded by (Z.F.) and imported into the EndNote X8 Software, Clarivate. After removing duplicates, two members of the research team S.A. and Z.V. independently screened the studies for relevancy to the review topic. Disagreements about inclusion were resolved in an iterative process via discussion and refinement of the inclusion/exclusion criteria until 100% agreement was achieved (Z.V., S.A., and H.R.). Next, both S.A. and Z.V. reviewed the full texts of the articles and cross-validated the eligibility based on the inclusion as mentioned criteria. Inter-rater reliability was assessed using Cohen’s kappa, yielding κ = .72 (good agreement).
Data Collection Process
We designed a standardized data extraction form to extract study characteristics. The developed form was pilot-tested on five randomly selected included articles and then refined. Two review authors (S.A. and Z.V.) worked independently to extract study details. A third reviewer reviewed data extraction and resolved conflicts (H.R.). When information regarding the published articles was inadequate, corresponding authors were asked for additional information. The information in two articles was incomplete, and the missing details were obtained via email from the corresponding author. All results that were compatible with each outcome domain in each study were searched. Relevant information such as the authors’ names and year of publication, study setting, study design, the number of participants, prevalence, assessment instrument, and neglect risk factors were extracted (Supplemental Table S1).
Quality Assessment (Risk of Bias)
Two reviewers (S.A. and Z.V.) independently conducted the qualitative assessment using the JBI Critical Appraisal Tools. This tool comprises nine questions coded as “yes,” “no,” or “Unclear.” Based on the coding, each study was rated as good quality (total score 7–9), moderate quality (total score 4–6), or poor quality (total score 3 or less). The nine questions asked about sample frame, appropriate method of sampling participants, sample size adequate, description of study subjects and environment, data analysis, use of valid methods to identify conditions, measuring conditions in a standardized and reliable way for all participants, appropriate statistical analysis, and adequate response rate (Munn et al., 2015). In cases of ambiguity, a definite decision was taken by consensus with a senior researcher (H.R.). Accordingly, each domain was assessed as having a low, unclear, or high risk of bias.
Results
Search Process
The systematic search yielded 13,541 records as follows: PubMed (3,233), Web of Science (4,221), Cochrane Library (895), and Scopus (5,192). After 1,705 duplicates were removed, 11,836 records were left for screening. A total of 11,647 records were excluded based on their title/abstract. The full text of the remaining 189 records were retrieved, then independently reviewed and screened by 2 reviewers (S.A. and Z.V.); 89 records were excluded, with reasons listed in Figure 1. Nine articles were identified through reference and citation searches. Finally, 109 eligible studies were included in this review. The PRISMA flowchart was adopted to illustrate the search process, as shown in Figure 1.
Characteristics of the Included Studies
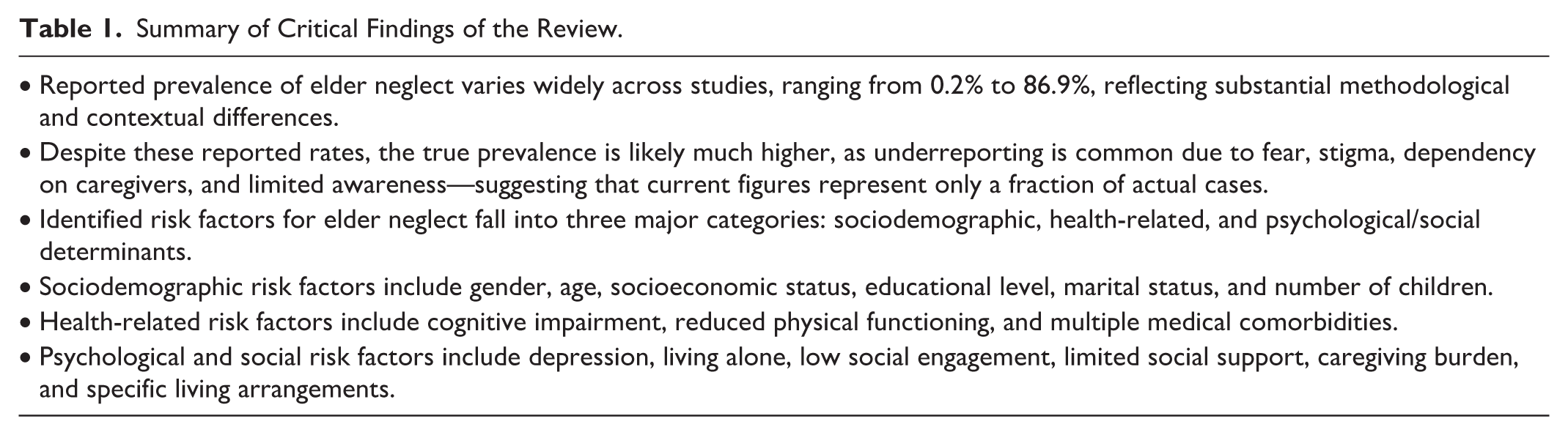
The characteristics of the included studies are summarized in Table 1. The years the studies were performed and published ranged from 1992 to January 2026. The number of participants was in the range of 45 to 206,000 per study. The mean age of participants was 73.10. The largest number of studies (32) was in the United States (ranged from 1.1% to 86.9%). Next were India with 12 studies (ranged from 4.3% to 74%), and Turkey with 11 studies (ranged from 1.12% to 62.6%). Of them, eight articles were published based on large-scale cohort studies conducted in the United States. Various measurement tools were used to assess neglect among older adults. Fifty-eight studies used researcher-made instruments to assess the status of elder neglect. Nineteen studies reported the prevalence of self-neglect (ranged from 6.88% to 86%) and four studies reported both. Based on the findings, the prevalence of neglect among older adults ranged from 0.2% to 86.9%.
Summary of Critical Findings of the Review.
Neglect Risk Factors
The results indicate that a wide range of factors have been identified as being associated with elder neglect across different studies. These factors can be categorized as follows.
Sociodemographic characteristics
Gender: Most studies reported that women experience higher levels of neglect than men, although a few studies found no significant gender differences.
Age: Findings suggest that the risk of neglect among older adults increases with advancing age.
Economic status: Older adults with lower income levels were more likely to experience neglect. Some studies also found that financial dependence on adult children was associated with higher levels of neglect.
Educational level: Educational attainment was inversely associated with elder neglect, indicating that individuals with higher levels of education experience lower rates of neglect.
Marital status: In most studies, older adults who were widowed, divorced, or living separately from their spouse experienced higher rates of neglect compared to those who were married.
Number of children: The reviewed studies reported a positive association between the number of children and the likelihood of experiencing neglect among older adults.
Health-Related Characteristics
Cognitive impairment: Several studies identified cognitive impairment as a risk factor for elder neglect.
Physical functioning: Limitations in activities of daily living were associated with poorer perceived health status and increased dependency, which in turn heightened vulnerability to neglect.
Number of medical comorbidities: The findings regarding comorbid conditions were inconsistent, with some studies reporting a significant association between chronic illness and neglect, while others found no such relationship.
Psychological and Social Characteristics
Psychological and social factors—including depression, living alone, level of social participation, availability of social support, caregiver characteristics, and living arrangements—were also found to play an important role in the occurrence of elder neglect.
The essential characteristics of the studies are shown in Supplemental Table S1.
Methodological Quality and Risk of Bias
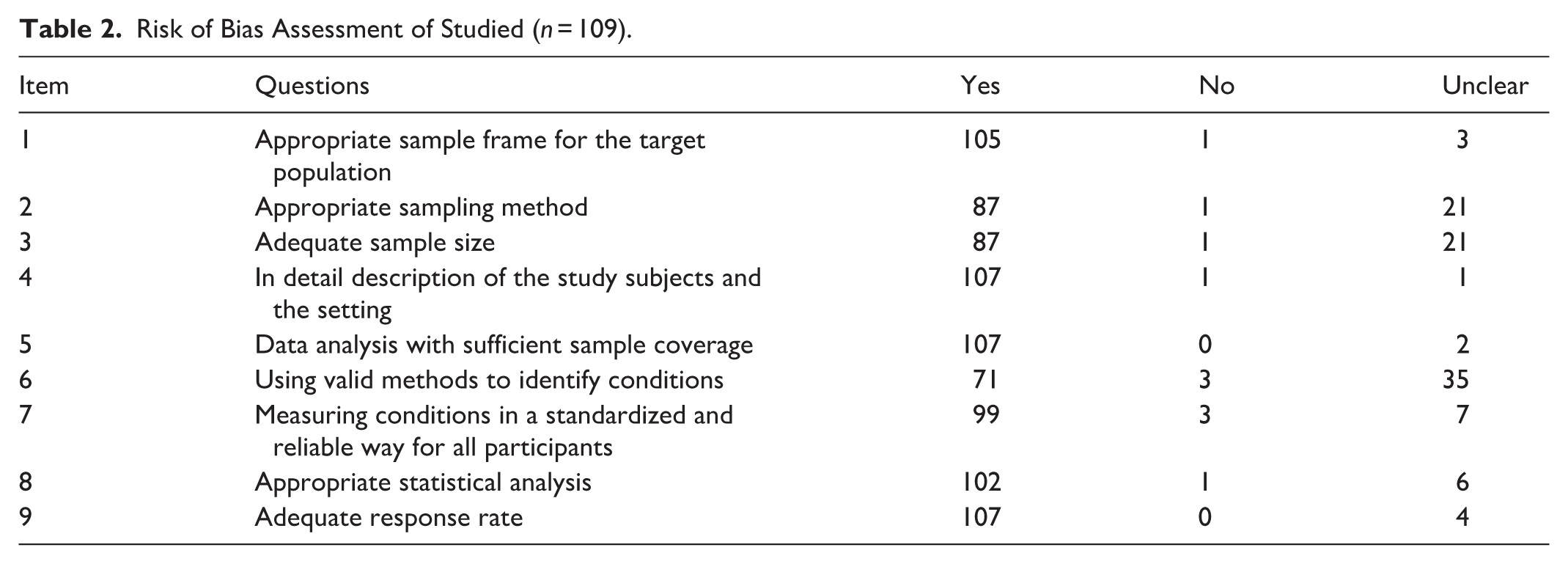
The risk of bias was assessed for involved studies, and it was shown in Table 2 and Figure 2. From the 109 included studies, 94 of them were assessed as having good qualities, 13 as moderate, and 2 as poor quality (88.23%, 10.78%, and 0.98%, respectively).
Risk of Bias Assessment of Studied (n = 109).
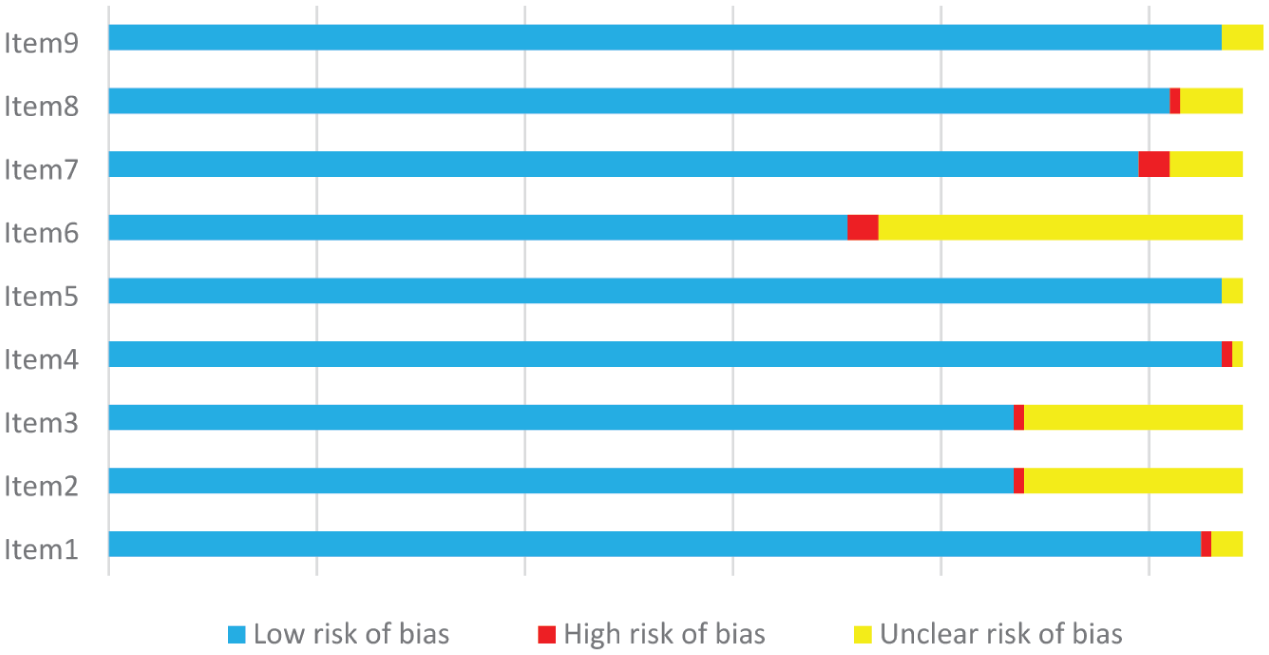
Risk of bias assessment of studied (n = 109).
In the quality appraisal, a substantial number of studies demonstrated unclear risk of bias across multiple methodological domains. Specifically, 35 studies were rated as “unclear” on Item 6 of the JBI checklist, indicating insufficient information regarding the use of valid methods to identify conditions. Additionally, 21 studies received “unclear” ratings for both sampling method and sample size adequacy. These findings indicate considerable variability in methodological rigor among the included studies (Table 2 and Figure 2).
Discussion
With the increasing aging population worldwide, elder neglect is recognized as a serious and increasing problem (Mydin et al., 2021). This systematic review study, based on a comprehensive search strategy, was conducted to better understand the prevalence and risk factors of elder neglect. The review showed that elder neglect prevalence has been estimated in different settings; also various methods were used for data collection in these studies. A sample of various studies that depict elder neglect prevalence is presented from major epidemiological studies, agency reports, healthcare professionals, caregivers and families, and medical record reviews. Overall prevalence rates of elder neglect have varied considerably across studies, from 0.2% to 86.9%.
Evidence has reported varying ranges of prevalence of elder neglect (Atim et al., 2023; Comijs et al., 1998; Kaur et al., 2015; Naughton et al., 2012). A notable finding of this review is the wide variation in reported prevalence estimates of elder neglect. This heterogeneity is largely driven by differences in how neglect is defined, the methodological approaches used—including sampling strategies and measurement tools—and the extent to which studies employ culturally appropriate instruments. Cultural norms, caregiving expectations, and stigma surrounding disclosure also influence reporting behaviors, contributing to underreporting. These factors collectively explain the broad range of prevalence estimates and highlight the need to interpret these figures within their specific methodological and cultural contexts. According to another aim of the study, risk factors for older adults can be categorized into sociodemographic, health-related, and psychological and social context aspects.
Sociodemographic Characteristics
Gender
Most included studies reported a higher prevalence of neglect among older women compared with men, although some studies found no significant gender differences (Anme et al., 2005, Ghodousi et al., 2011; Mardan et al., 2014; Özcan et al., 2017; Yusuf & Baiyewu, 2014). This gender disparity may be partly explained by women’s relatively disadvantaged socioeconomic and health status in later life, including lower educational attainment, financial dependence, and a higher burden of physical illness (Chokkanathan, 2017; Du & Chen, 2021). In addition, older women are more likely to live alone than men, which may increase vulnerability to neglect and self-neglect (Gorbien & Eisenstein, 2005). Sociocultural factors may further contribute to this pattern. In many societies, traditional gender roles and patriarchal family structures place older women in a less powerful position within the household, potentially increasing their exposure to neglect (Nerenberg, 2007). Conversely, several studies have shown that older men also experience neglect (Fulmer, 2008; Lachs et al., 1997; Oh et al., 2006; Wu et al., 2012). However, men may be less likely to disclose neglect due to stigma related to weakness, dependency, and masculinity norms, which could lead to underreporting (X. Dong & Wang, 2017; Thurston et al., 2016). In addition, bereavement and social isolation among older men may increase the risk of neglect and self-neglect (Dasbas & Isikhan, 2019). These findings highlight the importance of adopting a gender-sensitive approach in policies and interventions aimed at preventing elder neglect. Interventions should address structural gender inequalities and provide targeted support for vulnerable older women, while also considering barriers to help-seeking among older men.
Age
Most studies indicated that the risk of neglect increases with advancing age, likely due to age-related frailty, a higher prevalence of chronic diseases, and geriatric syndromes, and increasing care needs (Du & Chen, 2021; Naughton et al., 2013; Oh et al., 2006; Post et al., 2010; Zhang et al., 2010). However, several studies reported an inverse association in the oldest age groups, suggesting lower reported neglect among the oldest-old (Burnes et al., 2015; Oh et al., 2006; Post et al., 2010; Vida et al., 2002). This pattern may reflect underreporting related to learned helplessness, reduced awareness or ability to disclose neglect, or greater avoidance of potentially abusive relationships in advanced age. One study found no significant association between age and neglect (Keskinoglu et al., 2007).
Economic Status
Lower income was consistently associated with a higher risk of neglect, and financial dependence on adult children was also linked to greater vulnerability (Alizadeh-Khoei et al., 2014; Du & Chen, 2021). Limited financial resources may constrain caregivers’ capacity to provide adequate care, particularly in contexts of broader socioeconomic hardship, thereby increasing the risk of unintentional neglect (Yusuf & Baiyewu, 2014). Moreover, structural factors such as limited access to social services and inadequate public healthcare coverage further exacerbate the risk of neglect among economically disadvantaged older adults (Choi et al., 2009; L. Dong & Sun, 2022). Nevertheless, one study reported no significant association between perceived economic status and neglect (Yusuf & Baiyewu, 2014).
Educational Level
Educational attainment was generally inversely associated with elder neglect, with lower levels of education linked to higher reported neglect. This association may reflect limited health literacy, reduced access to resources, and fewer opportunities to seek support or report mistreatment among less-educated older adults (X. Dong et al., 2011; Yusuf & Baiyewu, 2014). Higher education may promote positive health behaviors and enhance individuals’ capacity to navigate health and social care systems (Kissal & Beşer, 2011). However, several studies reported conflicting findings, with higher levels of neglect observed among individuals with greater educational attainment (Aylaz et al., 2020; DeLiema et al., 2012; M. Lee & Kim, 2014; Mardan et al., 2014), indicating that the relationship between education and neglect may be context-dependent.
Marital Status
Most studies reported higher rates of neglect among older adults who were widowed, divorced, or living separately from their spouse compared with those who were married. Living alone and strained or disrupted family relationships may increase vulnerability to neglect. However, several studies reported contradictory findings, with married older adults experiencing higher levels of neglect than their unmarried counterparts (Jeon & Kong, 2022; Markovik et al., 2014; Mwaheb et al., 2023). One possible explanation is that spousal neglect may persist across the life course and continue into older age, particularly in long-standing relationships characterized by imbalance or conflict.
Number of Children
A positive association between the number of children and the likelihood of elder neglect was reported in several studies. In larger families, caregiving responsibilities may be diffused, increasing the risk that individual family members avoid responsibility and perceive care for older parents as a burden (Du & Chen, 2021).
The heterogeneity of findings across studies—particularly regarding gender and educational level—may be attributed to several methodological and contextual factors. First, variation in the definition and operationalization of neglect (e.g., self-neglect vs. caregiver neglect) may lead to different observed patterns. Second, sociocultural norms related to gender roles, caregiving expectations, and intergenerational relationships can shape both the occurrence of neglect and reporting behaviors, contributing to cross-cultural differences. Third, differences in measurement approaches (e.g., self-report instruments vs. structured interviews) may introduce reporting biases. Fourth, heterogeneity in sample characteristics, including socioeconomic status, household composition, and health status, may modify observed associations. Finally, broader contextual factors, such as access to formal care services, social protection systems, and community resources, likely interact with individual-level characteristics, further contributing to variability across settings. The inconsistent findings across studies regarding the effects of gender and education on elder neglect may stem from several methodological and contextual factors. First, studies vary widely in how they define and operationalize neglect, with some examining self-neglect and others focusing on caregiver neglect; these subtypes may differ considerably in their gender and education patterns. Second, sociocultural norms related to gender roles, caregiving responsibilities, and intergenerational expectations can influence both the occurrence of neglect and the likelihood of reporting it, leading to cross-cultural variation. Third, differences in assessment instruments—such as self-report questionnaires versus structured interviews—may introduce reporting biases that disproportionately affect certain demographic groups. Fourth, variations in sample characteristics, including socioeconomic status, household composition, and health status, can modify the association between demographic factors and neglect. Finally, broader contextual factors such as access to formal care services, social protection systems, and community resources may interact differently with gender and education in different settings. These combined factors likely contribute to the heterogeneity observed in the literature.
Health-Related Characteristics
Cognitive Impairment
Some studies reported that cognitive impairment tended to be a risk factor for neglect (Choi et al., 2009; L. Dong & Sun, 2022; Fang et al., 2019; Giraldo-Rodríguez and Rosas-Carrasco, 2013), while M. Lee and Kim (2014) observed a negative association between cognitive impairment and neglect (M. Lee & Kim, 2014). Higher levels of cognitive abilities were slightly associated with a higher frequency of self-neglect (M. Lee & Kim, 2014). Cognitive impairment in older adults is one of the major causes of functional dependency. They require assistance in their efforts to meet the basic and instrumental needs of their daily lives. On the other hand, older parents who are in good mental health have better self-efficacy, which helps prevent neglect (Giraldo-Rodríguez and Rosas-Carrasco, 2013; Yang et al., 2022).
Level of Physical Function
Experiencing problems in daily living activities exerts an unfavorable effect on the perception of health status, which renders the elder person dependent on people. It has been stated that older adults whose functionality is low are dependent upon their relatives, making it easier for them to experience conditions that may lead to neglect (Dasbas & Isikhan, 2019). One study found conflicting results that physical impairment reduced the likelihood of experiencing neglect (Atim et al., 2023).
Number of Medical Comorbidities
In the study of the Ghodousi et al. (2011), older adults had no significant mental, and physical diseases, but they were neglected. No association of underlying diseases with neglect (Ghodousi et al., 2011). In the study of Atmin et al. (2023), chronic medical conditions reduced the likelihood of experiencing neglect. This findings is inconsistent with studies that indicated increasing medical comorbidities were frequently seen in reported neglect cases among older adults. Those who rate their health status as tolerable/moderate or bad experience a higher rate of neglect than the ones who rate it as good (Cohen, 2008; Du & Chen, 2021; Maurya et al., 2024; B. Wang et al., 2020). It is thought that whether health status is evaluated as good or bad depends on being able to meet one’s own needs. Lack of adequate public social service and healthcare programs, including the provision of necessary medications and medical supplies and medication management, are also likely to be serious risk factors for self-neglect/neglect (Kissal & Beşer, 2011; Laumann et al., 2008; Oh et al., 2006).
Psychological and Social Characteristics
Depression
One of the reasons for neglect is the change in the traditional family and its values. Due to the phenomenon of youth migration, older adults are left alone. On the other hand, the inability of older adults to share their mental and physical condition with the family due to difficult economic conditions has reduced intimate feelings and undermined respect in the family. This may because the older adults to suffer from abandonment, emotional and psychological abuse, all of which may lead to mental disorders such as depression (Alexa et al., 2020; Aylaz et al., 2020).
Living Alone
The explanation for this finding is quite obvious in the sense that a spouse is an additional caregiver that would see to the needs of older adults. In today’s situation, due to changing values in the structure and cultural patterns of families and societies, elderly parents usually do not live with their adult children. They live alone or may be sent to nursing homes by their adult children. In this case, they may not receive appropriate frequent contact or regular visits from their children. At this point, it can be imagined that being alone makes the elderly person more vulnerable to risks such as daily care, medication use, balanced and regular nutrition, emergencies, etc., which leads to an increase in the rate of neglect due to lack of social support (Aylaz et al., 2020; Y. S. Lee et al., 2014; Wu et al., 2012).
Social Engagement
High neglect was also found to be negatively associated with social activity, which implies that elder neglect is closely related to the social environment. The social networks of older adults have decreased due to the death of their spouses and peers. Also, they are not ready or willing to create new social relationships, which leads to separation. As a result, they are exposed to neglect without adequate social support (Achenbaum & Bengtson, 1994). In the opposite direction, the findings of the Asiamah et al. (2022) study showed that high neglect was found to be positively associated with volunteering in the community. It is possible that older adults spend more time in volunteer activities to avoid or reduce abuse and neglect at home and join volunteers in the wider community (Asiamah et al., 2022).
Social Support
Most studies reported a negative association between social support and elder neglect. Reduced social opportunities due to life transitions such as retirement, bereavement, or declining health may increase vulnerability to neglect. Low social support can exacerbate psychopathology, contribute to social withdrawal, and reduce opportunities for the community to identify at-risk older adults (Amstadter et al., 2011; Farriol-Baroni et al., 2021). Conversely, higher levels of social support—through family, friends, or community networks—can protect against neglect by alleviating interpersonal strain, enhancing life satisfaction, and facilitating access to resources (Acierno et al., 2010; Chokkanathan, 2017).
Caregivers
Caregivers who assist older adults with daily activities may experience stress due to financial pressures, emotional demands, or competing responsibilities, which can lead to suboptimal care and neglect (Amstadter et al., 2011; Y. S. Lee et al., 2014; Naughton et al., 2012; Yadav et al., 2018). High emotional demands—including managing aggression, suffering, or physical pain of the older adults—may further compromise caregiving quality (Andela et al., 2021). In institutional settings, under-resourced or under-trained personnel may also contribute to neglect (Y. S. Lee et al., 2014; Pillemer, 2004).
Living Arrangements
Changes in family structures, urbanization, and economic pressures have disrupted traditional caregiving arrangements, often leading to isolation and neglect of older adults (Aslan & Erci, 2020; Ghodousi et al., 2011; Kissal & Beşer, 2011; Nemati-Vakilabad et al., 2023). Intergenerational conflicts and weaker family bonds, compounded by older adults’ limited access to modern communication technologies, further increase the risk of neglect (X. Dong et al., 2007; Kulakçı Altıntas & Korkmaz Aslan, 2020; Nemati-Vakilabad et al., 2023).
Neglect can be classified into self-neglect and caregiver neglect, each with distinct origins and consequences. Self-neglect arises from the older adult’s inability or unwillingness to care for themselves, often linked to cognitive decline, mental health issues, or functional loss. Caregiver neglect, on the other hand, results from inadequate care provided by a responsible caregiver, frequently causing emotional harm and relational betrayal. While both forms can lead to similar physical outcomes, their emotional repercussions and interventions differ. Most studies, however, do not differentiate between these types, limiting the understanding of specific risk factors and consequences. In this review, only 14 studies explicitly addressed self-neglect; nonetheless, the determinants identified for both types were largely similar (see Table 1).
Elder neglect arises from interconnected psychological, social, biological, and economic factors. Changes in living arrangements can increase loneliness, contributing to depression, while cultural and traditional influences shape the occurrence and reporting of neglect. Most cases remain unreported, highlighting the need for awareness and education for older adults and their families.
Healthcare professionals should routinely screen for elder neglect, including self-neglect, with culturally sensitive approaches, provide medical support, and implement home visits when necessary. Public awareness campaigns and community programs can further aid prevention.
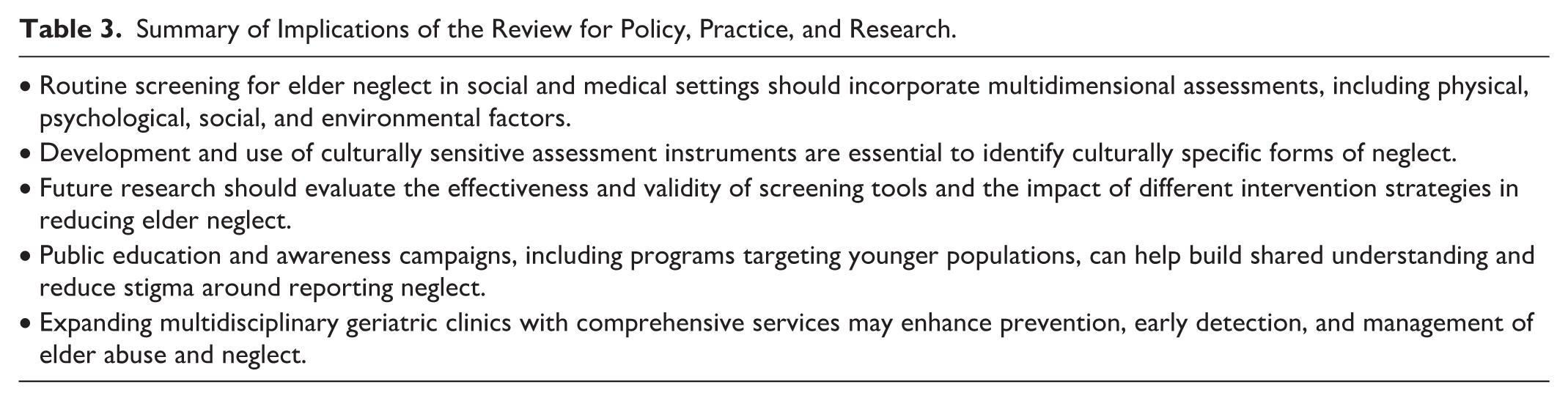
This review provides insight into the prevalence and risk factors of elder neglect, informing social policies, prevention strategies, and resource allocation. Findings are relevant not only for healthcare professionals but also for social workers, formal and informal caregivers, policymakers, public health practitioners, community organizations, and researchers. By highlighting key risk factors and patterns, the review can guide targeted prevention programs, improve caregiver training, and support interventions to protect older adults. A summary of these implications is presented in Table 3.
Summary of Implications of the Review for Policy, Practice, and Research.
Considering that neglect can be categorized into two distinct types—self-neglect and caregiver neglect—it is essential to differentiate between these two in order to understand their respective consequences. Both self-neglect and caregiver neglect can lead to similar physical outcomes, such as untreated health issues and substandard living conditions; however, they diverge in significant ways. Self-neglect arises from an older adult’s inability or unwillingness to care for themselves, and it is closely associated with cognitive decline, mental health challenges, and loss of functional abilities. In contrast, caregiver neglect occurs due to a responsible caregiver’s failure to provide adequate care, often resulting in more profound emotional damage, feelings of betrayal in relationships, and may necessitate legal or protective actions. In summary, the origins, emotional repercussions, and required interventions vary between these two forms of neglect. It is noteworthy that in the majority of research studies, the specific type of neglect is not clearly identified and is typically generalized as neglect, with the consequences of each type not being distinctly articulated. Therefore, there is a pressing need for more cross-sectional studies to investigate, analyze, and differentiate between these two forms of neglect. This systematic review indicates that only 19 studies explicitly addressed self-neglect and 4 studies reported both; however, as illustrated in Table 1, the determinants associated with both types do not significantly differ from one another.
Diversity and Generalizability
Elder neglect arises from the complex interaction of psychological, social, biological, and economic factors, which often reinforce one another. Changes in living arrangements can increase loneliness, which is closely linked to depression, while cultural, traditional, and social norms influence patterns of neglect across countries. Most cases remain within families, emphasizing the importance of education for older adults and their families to recognize neglect and access support services. Self-neglect, a gradual and understudied syndrome, may be mitigated through professional interventions such as rehabilitative services, assistive devices, and in-home care. Effective prevention and detection require culturally sensitive screening tools, public education, community-based programs, and expanded geriatric services. Longitudinal research is needed to clarify causal pathways and evaluate the effectiveness of interventions and screening practices.
Substantial diversity among studies—including variations in age, gender, socioeconomic status, living arrangements, geographic location, and cultural norms—likely contributes to the wide range of reported prevalence (0.2%–86.9%) and risk factors. Many studies lacked detailed reporting on race, ethnicity, sexual orientation, and other socioeconomic indicators, limiting the generalizability of findings to diverse or marginalized populations.
Limitations
This systematic review has some limitations. First, we did not search specifically for unpublished research reports, although we did obtain and review unpublished reports listed in the reference lists of retrieved articles. The omission of gray literature may result in some degree of publication bias. We did not contact experts in the field for other studies, and we only included English-language articles. Nevertheless, we did conduct a comprehensive search of existing databases. All of the studies adopted cross-sectional designs, which disallows the establishment of causal relationships between potential risk factors and neglect. Consequently, the risk factors mentioned in this review reflect associations rather than causations. Prevalence studies are conducted in different settings, with different types and definitions of elder neglect, and various instruments to measure the neglect. With such a variation, it is difficult to compare results. For example, if the prevalence of elder neglect is determined in the hospital that is very different from an epidemiological study conducted in an area. The present study is merely a systematic review without a meta-analysis due to the limited statistics that these studies provided. Hence, only a narrative review of the existing evidence was provided.
Methodological limitations, including unclear risk of bias, inadequate sampling procedures, small sample sizes, and invalidated measurement tools, further constrain the reliability of synthesized evidence. Consequently, findings should be interpreted with caution, and future research should prioritize rigorous study designs, transparent methodology, and validated assessment instruments. Our review offers healthcare professionals insight into neglect and its risk factors, aiding in the development of social policies to prevent elder neglect. Also, this review informs stakeholders, guiding prevention, caregiver support, resource allocation, and research to improve elder neglect detection and intervention. In addition to healthcare professionals, the findings of this review are relevant for a broader range of stakeholders. These include social workers, caregivers (both formal and informal), policymakers, public health practitioners, community organizations, and researchers. By highlighting prevalence patterns and risk factors, the review can guide the development of targeted prevention programs, inform policy-making, and improve training and support for caregivers and community staff involved in elder care. A summary of the implications of the review for policy, practice, and research is presented in Table 3.
Despite these limitations, this review has several notable strengths. First, it provides one of the most up-to-date and comprehensive syntheses of the prevalence and risk factors of elder neglect, incorporating studies published up to January 2026. Second, unlike previous reviews that examined abuse of older people broadly, this study focuses specifically on neglect as an independent subtype, allowing for a more detailed analysis of its unique characteristics. Third, the search strategy employed multiple major international databases and used an extensive set of keywords to maximize coverage of relevant studies. Fourth, the quality of evidence was systematically appraised using the JBI Critical Appraisal Tools, ensuring methodological rigor and consistency across different study designs. Finally, the stratified narrative synthesis—based on region, population characteristics, assessment tools, and types of neglect—provides nuanced insights that can guide future research and inform targeted intervention strategies. Together, these strengths enhance the robustness and practical value of the review.
Conclusion
This systematic review highlights the wide variability in the prevalence of elder neglect and identifies key risk factors, including sociodemographic, health-related, and psychological/social determinants. Methodological differences and cultural factors contribute to the observed heterogeneity, emphasizing the need for cautious interpretation. The review underscores the importance of culturally sensitive assessment tools, rigorous study designs, and multidisciplinary approaches to improve the detection, prevention, and management of elder neglect. Future research should focus on standardizing definitions, validating screening instruments, and evaluating intervention strategies to strengthen the evidence base.
Supplemental Material
sj-docx-1-tva-10.1177_15248380261451840 – Supplemental material for A Glance at the Prevalence and Risk Factors of Elder Neglect: A Systematic Review
Supplemental material, sj-docx-1-tva-10.1177_15248380261451840 for A Glance at the Prevalence and Risk Factors of Elder Neglect: A Systematic Review by Hassan Rezaeipandari, Somayeh Azimi, Zahra Vahidian and Zahra Fathifar in Trauma, Violence, & Abuse
Footnotes
Ethical Considerations
This study has been approved by the Research Ethics Committee of the School of Public Health at Shahid Sadoughi University of Medical Sciences, Yazd, Iran (IR.SSU.SPH.REC.1403.017).
Author Contributions
All authors read and approved the final manuscript. H.R. designed the study. Z.F. collected data. S.A. and Z.V. analyzed data and S.A. wrote the manuscript. H.R. and S.A. revised it critically for important intellectual content and edited the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The datasets used in this study are included in this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.