
Abstract
Individuals with intellectual disabilities are at increased risk of trauma exposure, yet trauma-related symptoms are often undertreated. Single-case experiments have been used to evaluate trauma-specific interventions for this population. This study aimed to estimate overall treatment effects and examine variability in effects across participants and studies. We conducted a systematic review and multilevel meta-analysis. We searched eight databases, followed by study selection, data extraction, quality assessment, and used a three-level model to estimate overall effects across repeated measurements, participants, and studies, as well as to examine moderators (age, sex, treatment type, symptoms, and risk of bias). We included data from 62 participants across 10 studies. Trauma-specific interventions significantly reduced symptoms, reflected in both immediate level change (β = −3.09, 95% CI [−4.56, −1.63], p < .001) and decreasing symptom trajectories over time (β = −.50, 95% CI [−0.71, −0.29], p < .001). Effects were stronger for individuals aged ≤18 years and for studies with high risk of bias. This synthesis provides evidence that trauma-specific interventions reduce trauma-related symptoms in individuals with intellectual disabilities. Youth appeared particularly amenable to current treatment models for psychological trauma. However, the evidence is limited by the small sample sizes and high risk of bias. More rigorous, well-reported, and geographically diverse studies are needed to reduce uncertainty about treatment options and establish reliable, generalizable conclusions.
Keywords
Introduction
Intellectual disabilities (ID) refer to noteworthy limitations in cognitive functioning and adaptive behavior, manifesting in childhood (American Psychiatric Association [APA], 2013, 2022; Schalock et al., 2021; World Health Organization [WHO], 2019, 2022). Worldwide prevalence of ID, while variable, is estimated at 1.42% in males and 1.37% in females (Cuypers et al., 2021; Nair et al., 2022). Among individuals with ID, violence, abuse, and neglect are particularly prevalent, while their effects in the form of psychological trauma are underrecognized and undertreated (Kildahl et al., 2020; Kildahl & Helverschou, 2024; McNally et al., 2021; Rouleaux et al., 2024). Trauma-related symptoms in individuals with ID often manifest initially through externalizing or behavioral expressions, which may be a challenge for timely diagnosis and intervention (McNally et al., 2021). Nevertheless, valid diagnoses can be made (Versluis et al., 2024) and psychosocial interventions may be effective in treating trauma-related symptoms, despite concerns about cognitive limitations hampering psychotherapy (Tapp et al., 2023; Willner, 2006).
An important question is therefore whether existing psychosocial interventions for trauma-related symptoms are effective for people with ID (Byrne, 2022; McNally et al., 2021). Clinical guidelines cautiously recommend trauma-focused cognitive behavioral therapy (TF-CBT) and eye movement and desensitization and reprocessing (EMDR) as first-line treatments for post-traumatic stress disorder (PTSD) in children, adolescents and adults (International Society for Traumatic Stress Studies, 2023; National Institute for Health and Care Excellence [NICE], 2016, 2018). Such interventions were regarded in earlier reviews as feasible because these appeared to be well accepted and tolerated by people with ID (Keesler, 2020; Luteijn et al., 2020; L. Mevissen & de Jongh, 2010). Nevertheless, narrative syntheses of findings leave the strength of the evidence for positive treatment effects uncertain. This limitation also applies to reviews focused on a specific type of intervention such as EMDR (Jowett et al., 2016; Smith et al., 2021; Williamson & Rayner-Smith, 2024) and compassion-focused therapy (Cowles et al., 2020).
Most primary research investigating the effects of trauma-specific treatments on individuals with ID used single-case experimental designs (SCEDs; see for reviews Keesler, 2020; L. Mevissen & de Jongh, 2010). SCEDs allow testing of treatment effects with high internal validity, which is well suited for psychological research in clinical and applied settings (Blackston et al., 2019; Kazdin, 2021). In SCED, single or multiple participants act as their own control in within-participant comparison among frequently repeated measurements, controlling for individual level confounds. SCEDs involve repeated measurements of the outcome during baseline and intervention phases. Thus, when analyzing SCED data quantitatively, two levels of analysis are possible: participant level, by computing a separate effect size for each participant, and study level, by computing an effect size across participants. Nevertheless, generalizability remains limited in SCED studies due to the small number of participants (Blackston et al., 2019; Kazdin, 2021).
As external validity of treatment effects in SCED research depends on replication from one participant to another, the analysis of single-case experimental data within and across studies is of critical importance. This is essential if this body of work is to inform large-scale effectiveness studies and implementation. Recent developments in meta-analytic techniques can help assess both replicability of effects across participants and studies, providing insight in how the effects may differ across these levels (Moeyaert, 2019; Moeyaert et al., 2020). Quantitative synthesis is not only important for estimating the central tendency and distribution of effects found thus far but also to explore how effects vary between participants and between studies. To that end, multilevel synthesis can test moderators (Declercq et al., 2022; Moeyaert, 2019; Moeyaert et al., 2020, 2022).
Basic demographic moderators such as age and sex are usually tested in an exploratory manner, without specific expectations. Clinical heterogeneity may also be explored through differences in treatment type and level of ID. EMDR and TF-CBT, considered first-line treatments for PTSD, are based on different theories, such as adaptive information processing theory (Hill, 2020), working memory theory (Wadji et al., 2022), or emotional processing theory (Rauch & Foa, 2006), which may apply differentially for people with ID. Greater severity of ID might increase the complexity of treatment management (L. Mevissen & de Jongh, 2010), potentially affecting outcomes. Lastly, rigorous experimental methods reduce risk of bias in effect sizes, potentially explaining heterogeneity of effects as well (Moeyaert et al., 2021).
Objectives and Research Question
This meta-analysis of SCEDs synthesized the effects of trauma-specific interventions on trauma-related symptoms for individuals with ID. Heterogeneity in effects across participants and studies was investigated with moderator analyses. We hypothesized that trauma-specific interventions would reduce trauma-related symptoms in individuals with ID. Additionally, we investigated moderators at both participant-level and study-level to explain sources of heterogeneity. First, we asked what the average effectiveness was of trauma-specific treatments across studies and participants. Second, we asked to what extent treatment effects varied across treatment type, participant age, and level of ID. Our questions were pursued by modeling a three-level hierarchical structure (participant-level, study-level, and meta-analytic-level) and performing multilevel meta-analysis of SCED studies.
Method
This study was done following the “Cochrane Handbook for Systematic Reviews of Interventions” (Higgins et al., 2023), the “Preferred Reporting Items for Systematic Review and Meta-Analyses of Individual Participant Data Statement” (Stewart et al., 2015) to address the specific requirements of reporting SCED meta-analyses, as well as practical guidelines in mental health research review (Cuijpers, 2016). The protocol was pre-registered on the international prospective register of systematic reviews (PROSPERO ID: [CRD42023473242]). The search, selection of studies, data extraction, and quality assessment were conducted independently by the first and third author. Discrepancies were resolved through discussion; if no agreement was reached, the third author was consulted. Cohen’s kappa was used to evaluate level of agreement among the reviewers, calculated separately for study selection, data extraction, and quality assessment. The results were interpreted according to the accepted ranges proposed by Hanegraaf et al. (2024).
Eligibility Criteria
We included any type of SCED study, conducted in any settings at any point in time, that quantitatively assessed the effects of trauma-specific interventions on individuals with intellectual disabilities (APA, 2013, 2022), intellectual disability (Schalock et al., 2021), disorders of intellectual development or borderline intellectual functioning (BIF; WHO, 2019, 2022), as well as syndromes associated with ID and outdated terms such as mental retardation. There were no restrictions for participants’ sex, age, ethnicity, language, severity, concomitant diagnoses, or whether they concurrently received medical interventions. Participants with acquired brain injury after the age of 18 or any form of dementia were excluded. Formal PTSD diagnosis was not required; trauma was defined and assessed as operationalized in the original studies and ranged from clinically diagnosed PTSD to PTSD symptoms or other trauma-related symptoms. Trauma-specific interventions were understood as any psychosocial intervention to reduce trauma-related symptoms or disorders such as EMDR, TF-CBT, exposure therapies, writing therapies, narrative therapies, imaginary rescripting, intensive trauma therapies, creative arts therapies, and body and movement-oriented therapies. There were no restrictions for intervention length or for therapists’ level of experience. Trauma-related symptoms had to be measured using tools such as self-report scales, caretaker or clinician-rated instruments, or observational scales. Comparisons were based on the repeated, systematic measurements of the outcomes of interest before, during, and after active manipulation of the treatment condition.
Identification and Selection of Studies
On January 9 and 10, 2024, a systematic literature search of SCED studies was conducted using multiple electronic databases: Cochrane Library, EBSCOhost, Embase, Lens.org, PubMed, Scopus, VU library, and Web of Science. The search strings included keywords and terms related to individuals with intellectual disabilities, trauma-specific interventions, and SCED, which were combined using Boolean operators. The searches were not restricted by language nor publication date, but when possible filtered by study design. Full search strings are included in Supplemental Material A. In total, 14,061 records were identified from databases. The first author imported all records to EndNote, a citation and reference management tool (Clarivate, 2024). The second author imported records in the ASReview tool, using an active machine learning technique to systematically screen large amounts of records (Van de Schoot et al., 2020). Duplicates were identified and removed, followed by a screening of titles and abstracts. Then, reports were sought for full-text retrieval and were assessed for eligibility. The search was further supplemented through a manual search of relevant journals and by scanning reference lists from prior reviews. We updated our search strings and databases in June 2025, which identified one additional study, bringing the total number of included studies to 10. The PRISMA flow diagram, which summarizes each phase of the selection process and incorporates both the exhaustive strategy (Endnote) and the efficient strategy (ASReview), is presented in Figure 1 (Page et al., 2021). For the included studies, agreement between the two reviewers was strong (κ = .82; 95% CI = [.58, 1.00]). An overview of the excluded studies and the reasons for their exclusion is available in Supplemental Material B.
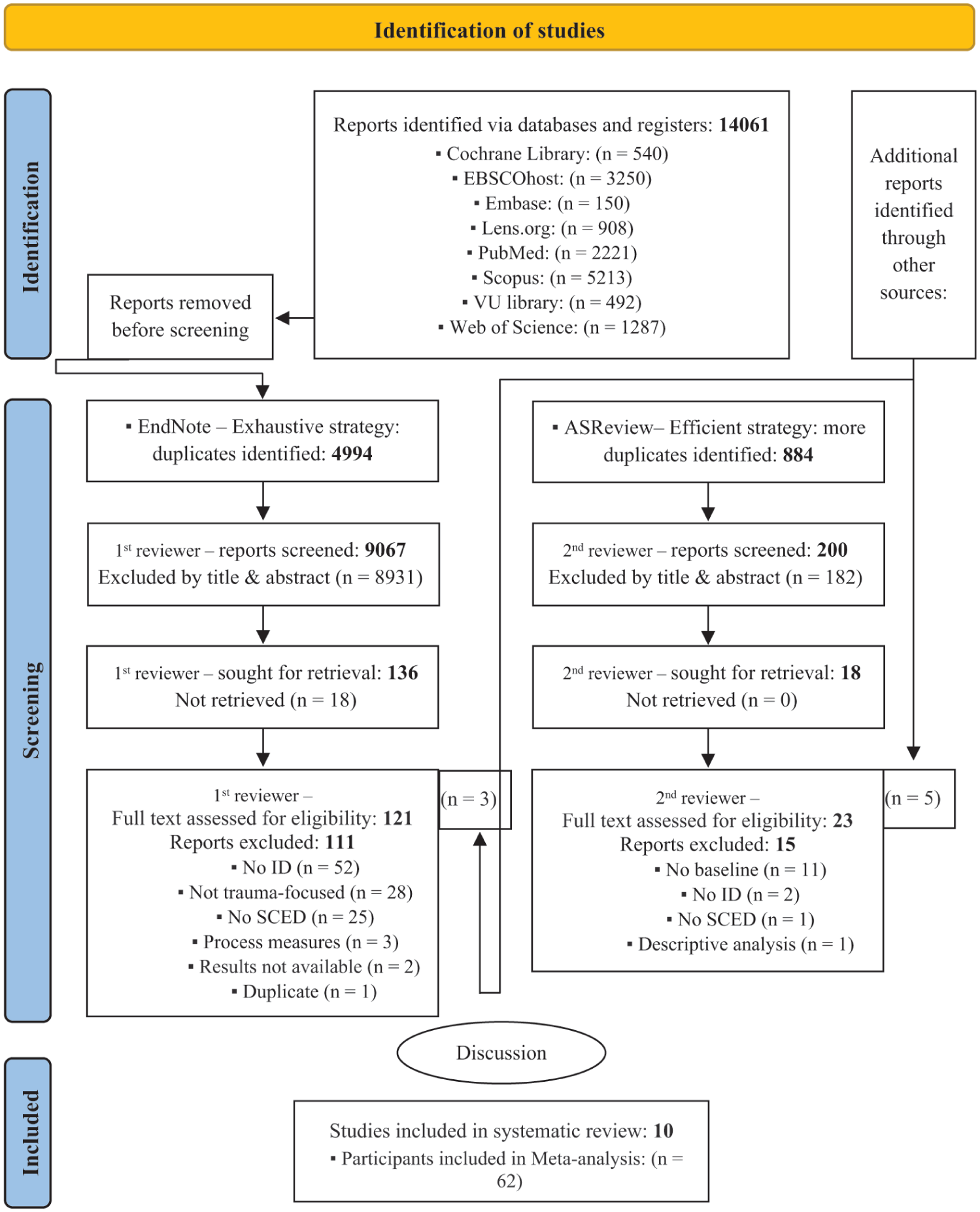
The PRISMA flow diagram of the inclusion and reasons for exclusion of studies.
Data Extraction
Items for data extraction and coding instructions can be found in Supplemental Material C. These items were coded and saved using an Excel form for: (a) general information, (b) individual participant data, (c) data for quality assessment, and (d) meta-analysis. The PlotDigitizer software program version 3.1.5 was used for data extraction from single-case graphs [https://plotdigitizer.com/app], as its validity and reliability was found to be nearly perfect (Aydin & Yassikaya, 2022; Moeyaert, Maggin, et al., 2016). Authors from three studies kindly shared their raw data (Hoogstad et al., 2024; L. Mevissen, Ooms-Evers, et al., 2020; Versluis, de Jongh, et al., 2025). Reliability for data extraction was very good, as indicated by the agreement between the two reviewers (κ = .94; 95%CI = [0.93, 0.95]).
Quality Assessment
A critical appraisal of the methodological quality of the included studies was conducted using the Risk of Bias in N-of-1 Trials (RoBiNT) scale, which is particularly well-suited for a variety of SCED frequently employed in psychological research (Tate et al., 2013, 2015). The RoBiNT comprises a 7-item internal validity subscale and a 8-item external validity/interpretation subscale. Each item on the scale is evaluated using a 3-point rating system. However, the items differ in weight concerning overall methodological rigor, which can be categorized as very high, high, moderate, fair, low, or very low. Then, these categories are grouped into low, moderate, or high risk of bias. The RoBiNT scale has demonstrated excellent psychometric properties, including high inter-rater reliability and construct validity. In this study, the agreement between the two reviewers was good (κW = .78; 95% CI = [0.70, 0.86]).
Meta-Analysis
In this one-stage individual participant data meta-analysis, raw data from multiple participants and studies were pooled (Declercq et al., 2022). To handle dependency among the data, we built a three-level structure that takes into account the nested structure of SCED data (Baek et al., 2022, 2023; Moeyaert et al., 2017, 2020, 2022). This type of meta-analysis allows the computation of three sources of variability: (a) within participants, (b) between participants, and (c) between studies. The overall weighted effect size is therefore unbiased and precise across all included studies and allows for examining variability in the effect size between studies and in the effect size between participants from studies. For constructing a three-level structure, two modeling assumptions were made: (a) level one, level two, and level three residuals (errors) have a normal distribution, and (b) intervention effectiveness can be captured as a change in symptom level and linear time trend between baseline and intervention conditions. The model started with single-level, then two-level, and finally three-level analysis (Figure 2).
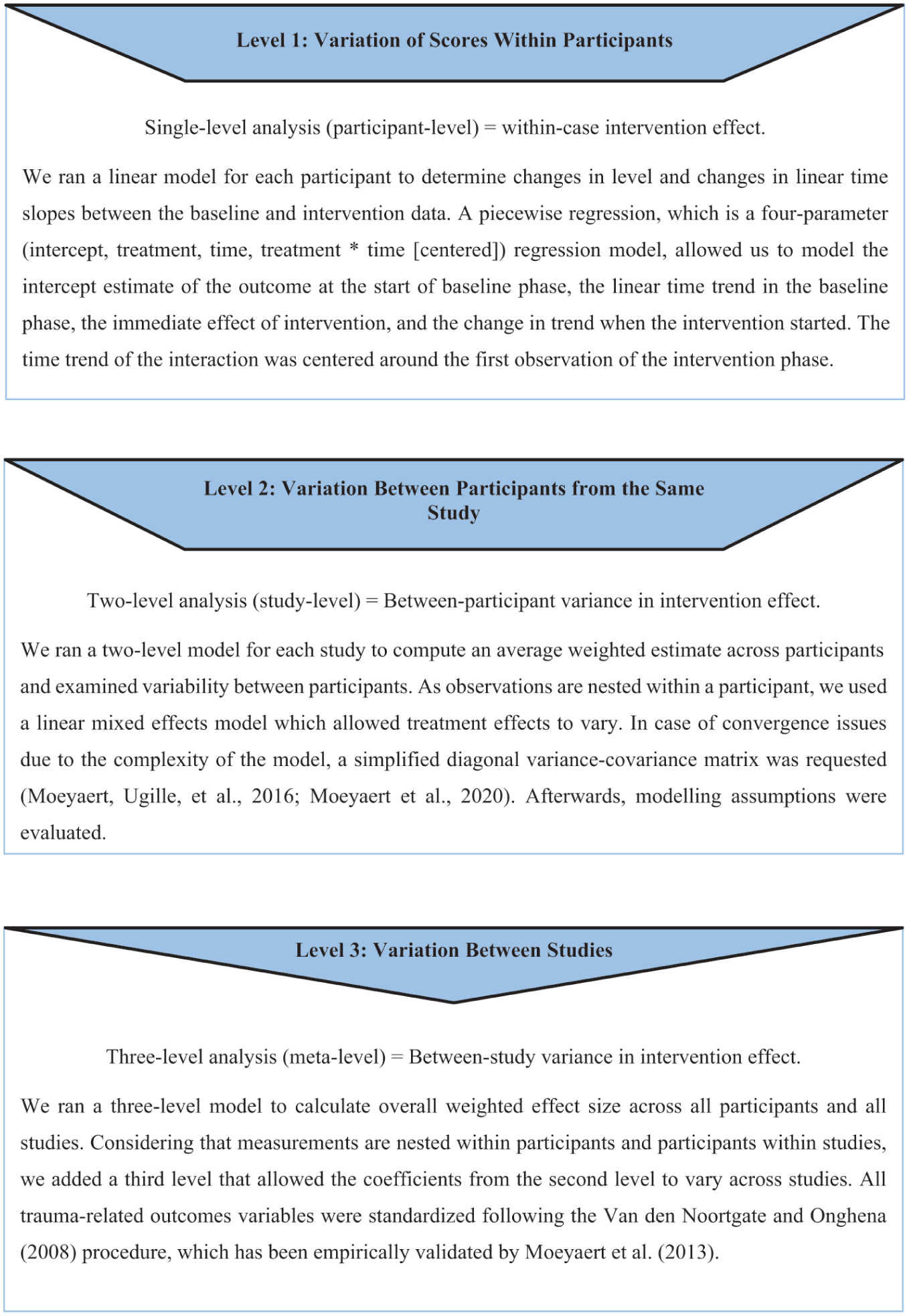
Hierarchical structure of meta-analysis.
Heterogeneity
We planned to investigate six potential moderators at both the participant and study levels by adding them individually to our model: (a) Age: over 18 versus 18 and under; (b) Sex: male versus female; (c) Treatment: EMDR versus Smart Start for Trauma (SST), Kind IN Gezond Systeem-Intellectual Disabilities (KINGS-ID), Child-Centered Play Therapy (CCPT), and Prolonged Exposure (PE); (d) Risk of bias: high versus moderate/low; and (e) Symptoms: PTSD versus other trauma-related symptoms. However, (f) Intellectual functioning: ID severity could not be tested because MID and BIF could not be differentiated in L. Mevissen, Ooms-Evers, et al. (2020).
All analyses were performed in Rstudio version 2023.12.1.402 (Posit Team, 2024), an integrated development for R (R Core Team, 2024), using the package “Linear and Nonlinear Mixed Effects Models” (version 3.1-146; Pinheiro et al., 2021), “Read Excel Files” (version 1.4.3; Wickham & Bryan, 2023), and “Data Visualization for Statistics in Social Science” (version 2.8.15; Lüdecke, 2024).
Results
Table 1 presents the main characteristics of the included studies and participants.
Characteristics of Included Studies and Participants.
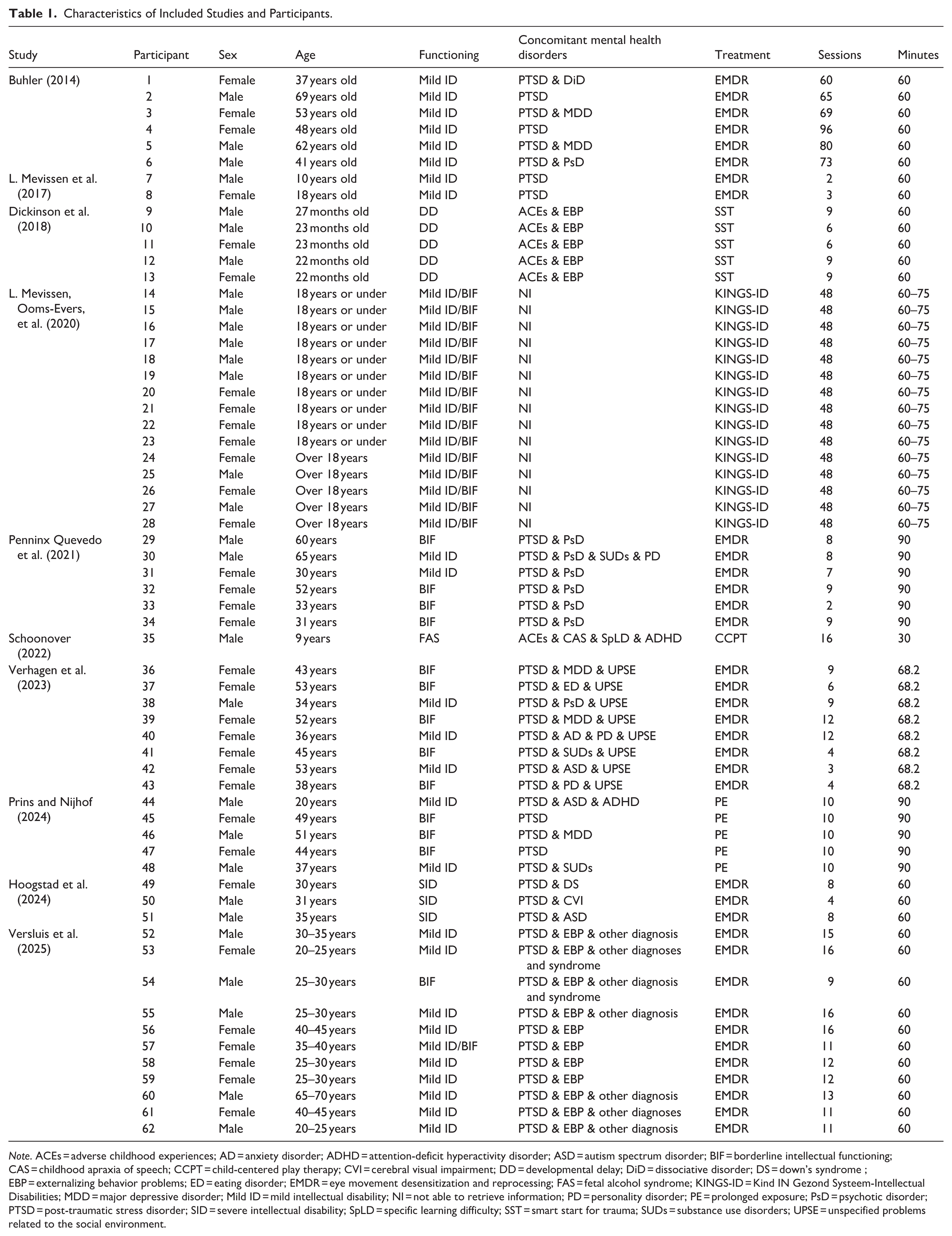
Note. ACEs = adverse childhood experiences; AD = anxiety disorder; ADHD = attention-deficit hyperactivity disorder; ASD = autism spectrum disorder; BIF = borderline intellectual functioning; CAS = childhood apraxia of speech; CCPT = child-centered play therapy; CVI = cerebral visual impairment; DD = developmental delay; DiD = dissociative disorder; DS = down’s syndrome ; EBP = externalizing behavior problems; ED = eating disorder; EMDR = eye movement desensitization and reprocessing; FAS = fetal alcohol syndrome; KINGS-ID = Kind IN Gezond Systeem-Intellectual Disabilities; MDD = major depressive disorder; Mild ID = mild intellectual disability; NI = not able to retrieve information; PD = personality disorder; PE = prolonged exposure; PsD = psychotic disorder; PTSD = post-traumatic stress disorder; SID = severe intellectual disability; SpLD = specific learning difficulty; SST = smart start for trauma; SUDs = substance use disorders; UPSE = unspecified problems related to the social environment.
Characteristics of the Included Studies
Seven studies took place in the Netherlands and three in the United States. Most studies used some type of multiple baseline SCED. The sample size of the included studies varied from 2 to 19 participants; nonetheless, not all participants were included. L. Mevissen, Ooms-Evers, et al. (2020) included 19 family members, among whom 6 parents and 10 children had mild ID or BIF. As the report did not include time-series graphs, the first author shared the raw data of 15 out of 16 participants with ID/BIF.
Verhagen et al. (2023), Prins and Nijhof (2024), and Versluis, de Jongh, et al. (2025) originally included 9, 12, and 12 adults, respectively. After excluding participants with insufficient data, the number of participants was 8 for Verhagen et al. (2023), 5 for Prins and Nijhof (2024), and 11 for Versluis, de Jongh, et al. (2025).
Schoonover (2022) assessed CCPT in five children who had been exposed to adverse childhood experiences (ACEs). We included one with fetal alcohol syndrome (FAS; Kodituwakku, 2009; Williams et al., 2015). We included participants with developmental delay, as in previous reviews (Byrne, 2022; Jowett et al., 2016; Luteijn et al., 2020; Smith et al., 2021). Participant data were removed when there was no variability on the dependent variable as this prevents standardizing the raw data which is needed for meta-analysis (Moeyaert et al., 2013; Van den Noortgate & Onghena, 2008).
Out of the 62 participants, 46.8% were male, and age ranged from 22 months to 69 years. Five children, under the age of three, had developmental delay. Usually, children this young are not able to do an IQ test, and significant developmental delays are seen as a form of ID in early childhood (Lee et al., 2023; Schalock et al., 2021). Three of the included participants had SID and the rest had mild ID or BIF. Participants presented a heterogeneous profile of concomitant diagnoses. For the included participants of L. Mevissen, Ooms-Evers, et al. (2020), we were unable to retrieve information regarding the specific concomitant diagnoses. Excluding participants from this study, the most common were PTSD, psychotic disorders, unspecified problems related to the social environment, major depressive disorders, personality disorders, and substance use disorders. Studies used different trauma-specific interventions, which included EMDR, CCPT, SST, PE, and KINGS-ID.
The number, duration, and frequency of sessions varied considerably among the studies. For trauma-specific interventions, Schoonover (2022) reported the shortest session length (30 min), while Penninx Quevedo et al. (2021) had the longest (90 min). L. Mevissen, Ooms-Evers, et al. (2020) and Versluis, de Jongh, et al. (2025) tested the most intensive trauma treatments, whereas Buhler (2014) tested the most prolonged treatment. Additionally, participants from L. Mevissen et al. (2017) received the shortest treatment duration; one participant received 120 min of EMDR, while another received 180 min. The characteristics of the trauma-specific interventions used in the included studies are available in Supplemental Material D.
Studies used a variety of measures to assess trauma-related symptoms. Buhler (2014) used multiple outcomes covering trauma-specific and a broader range of symptoms. We included repeated measures from the Trauma Symptom Checklist for Children (Briere, 1996), the Brief Symptom Inventory (Derogatis, 1993; Wieland et al., 2012), and the Aberrant Behavior Checklist (Aman & Singh, 1986; Rojahn et al., 2003). L. Mevissen, Ooms-Evers, et al. (2020) also used multiple outcomes; however, we could only get the raw data for PTSD symptoms, which were measured with the Diagnostic Interview Trauma and Stressors – Intellectual Disability (E. H. M. Mevissen et al., 2018; L. Mevissen, Didden, et al., 2020; Versluis et al., 2024). Hoogstad et al. (2024) used the Diagnostic Interview Trauma and Stressors – Severe Intellectual Disability (Hoogstad et al., 2023; L. Mevissen et al., 2021) to measure trauma symptoms, and a visual analog scale (Yeung & Wong, 2019) to measure frequency dysfunctional behaviors. Versluis, de Jongh, et al. (2025) included repeated measures of PTSD symptoms using the Trauma Screener–Intellectual Disability (Versluis, Schuengel et al., 2025), as well as behavioral problems with the Behavior Problems Inventory (Rojahn et al., 2001). In the remaining studies, repeated measures were taken for only one main outcome, all of which were included in this meta-analysis. PTSD symptoms were assessed using the Adapted Anxiety Disorder Interview Schedule-Child PTSD-ID-Adults (L. Mevissen, Didden, et al., 2020; L. Mevissen et al., 2016) in the studies by L. Mevissen et al. (2017), Penninx Quevedo et al. (2021), and Verhagen et al. (2023), and with the PTSD Symptom Scale (Minnen & Arntz, 2017) in the study by Prins and Nijhof (2024). For the studies that did not report PTSD symptoms across the phases, behavioral problems were included. Behavioral problems were measured using the Direct Observation Form (McConaughy & Achenbach, 2009) in the study by Schoonover (2022) and the Eyberg Child Behavior Inventory (Eyberg & Pincus, 1999; Reyes-Martín et al., 2022) in the study by Dickinson et al. (2018).
Risk of Bias
The rationale for the RoBiNT scale scores for risk of bias can be found in Supplemental Material F. A summary is presented in Table 2. Only Buhler (2014) demonstrated a low risk of bias, while Schoonover (2022) showed a moderate risk. For the others, the risk of bias was high. Common risk factors for bias were failure to provide a detailed description of the specific environment, not establishing and reporting inter-rater agreement for the specific study, lacking key information such as baseline characteristics, duration of sessions and symptom change in aggregates and/or averages, and lacking measurements for treatment adherence. In most studies, there was no mention of blinding, outcomes were self-reported, and therapists collected part or all of the data themselves. Some studies were rated as having a higher risk of bias in the sampling of behavior due to insufficient data points for each participant in every phase. For example, L. Mevissen et al. (2017) and Penninx Quevedo et al. (2021) reported only two data points in the intervention phase for one participant. It is worth noting that L. Mevissen, Ooms-Evers, et al. (2020) was rated higher for risk of bias due to the combination of lacking graphical displays and key information for each participant.
Risk of Bias.
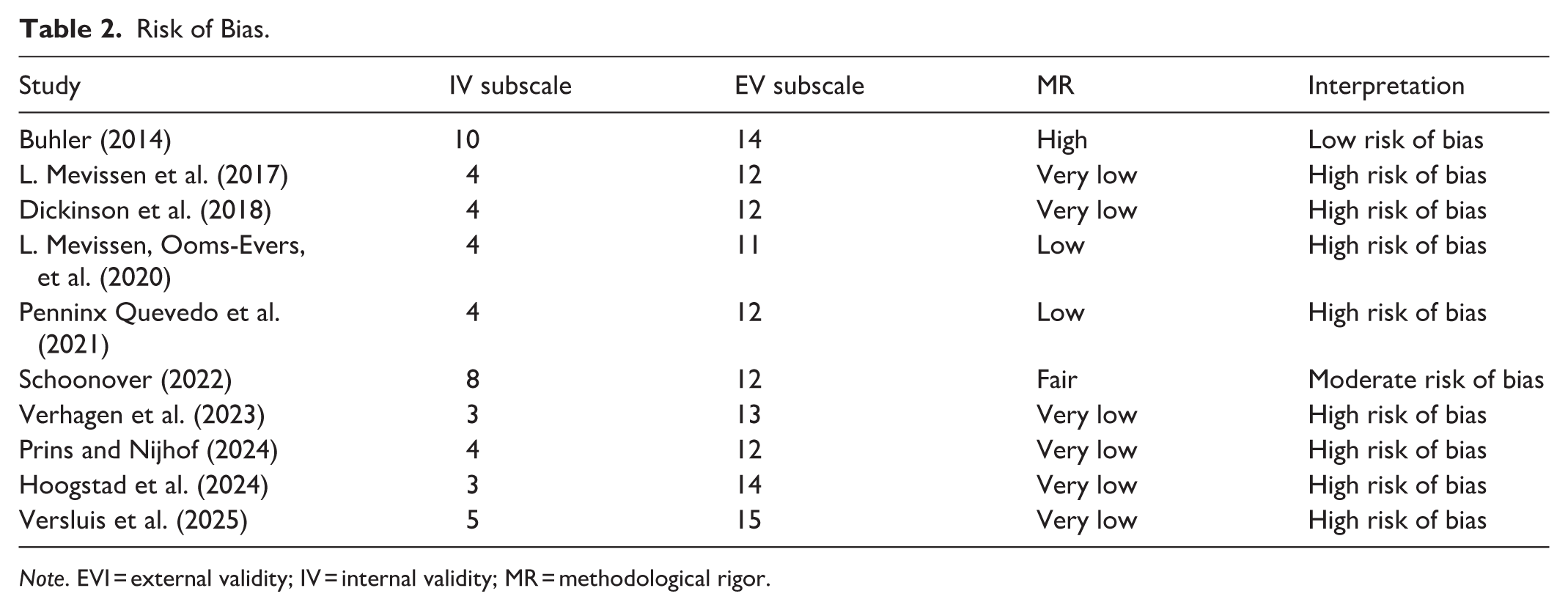
Note. EVI = external validity; IV = internal validity; MR = methodological rigor.
Effects and Moderators of Trauma-Specific Interventions
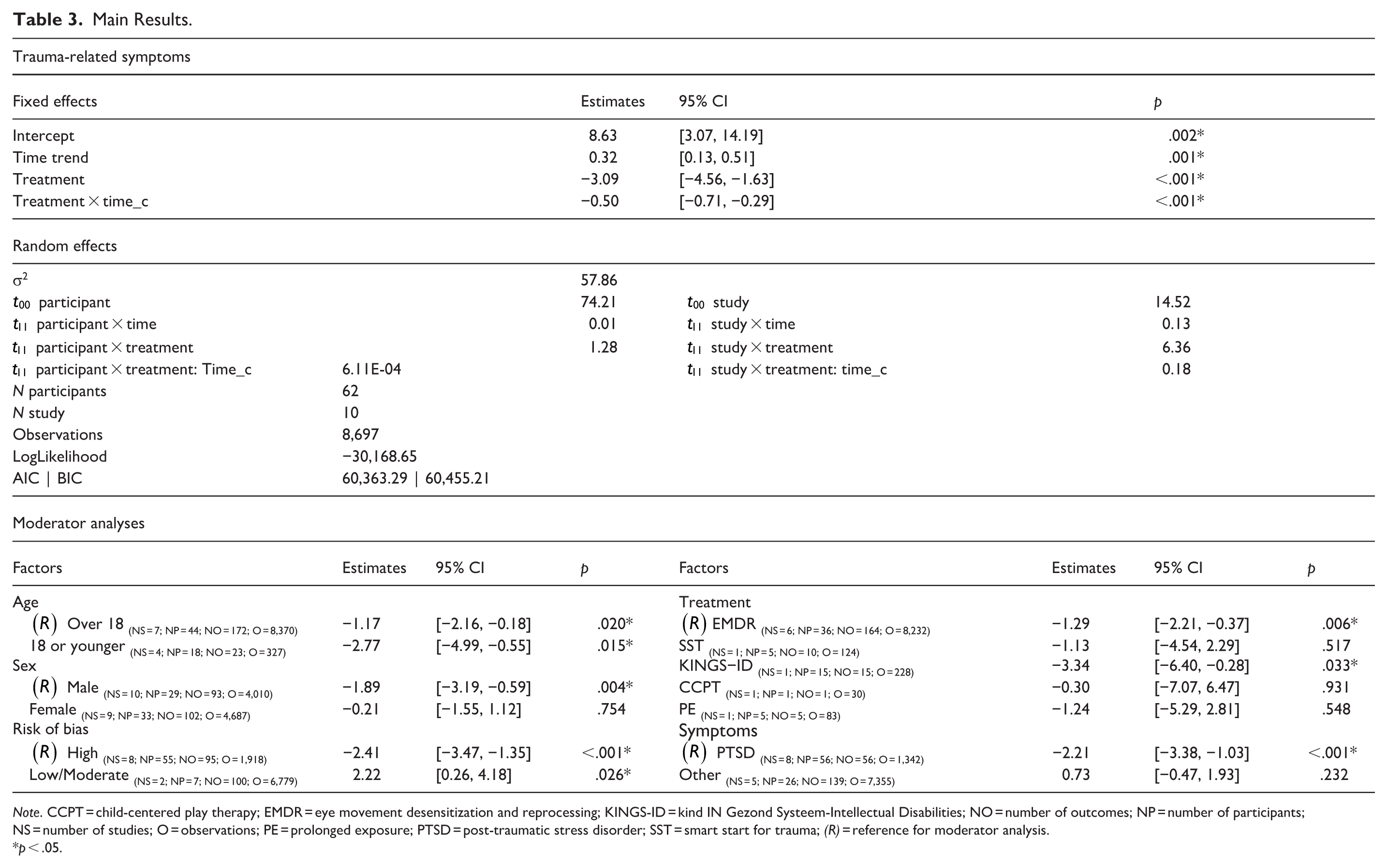
The main results are displayed in Table 3. Results from the meta-analysis of all trauma-related symptoms showed negative and significant effects for the shift in level (β = −3.09; 95% CI = [−4.56, −1.63]; p < .001) and in slope (β = −.50; 95% CI = [−0.71, −0.29]; p < .001). The negative level shift indicates an immediate reduction in symptoms from baseline to the onset of the intervention. The negative slope indicates that the interventions became increasingly effective over time, with symptoms continuing to decrease throughout the intervention and follow-up phases. Furthermore, the intercept (β = 8.63; 95% CI = [3.07, 14.19]; p = .002) and time trend (β = .32; 95% CI = [0.13, 0.51]; p = .008) during the baseline phase were positive, indicating that symptoms were increasing prior to the intervention.
Main Results.
Note. CCPT = child-centered play therapy; EMDR = eye movement desensitization and reprocessing; KINGS-ID = kind IN Gezond Systeem-Intellectual Disabilities; NO = number of outcomes; NP = number of participants; NS = number of studies; O = observations; PE = prolonged exposure; PTSD = post-traumatic stress disorder; SST = smart start for trauma; (R) = reference for moderator analysis.
p < .05.
The model that included moderators revealed significant differences in therapeutic effects for age group, treatment type, and risk of bias. Effects were not significantly different for male and female clients nor for type of symptoms (Table 3). Specifically, individuals up to age 18 showed a stronger treatment effect (−2.77 points stronger, 95% CI = [−4.99, −0.55], p = .015) than individuals over 18 years of age (−1.17 points, 95% CI = [−2.16, −0.18], p = .02). Testing treatment type as a moderator showed that compared to the reference treatment of EMDR (−1.29 points, 95% CI = [−2.21, −0.37], p = .006), KINGS-ID showed a greater effect (−3.34 points stronger, 95% CI = [−6.40, −0.28], p = .033). The effects of SST, CCPT, and PE did not significantly differ from EMDR. Analyses with study risk of bias as a moderator showed that compared to tests with high risk of bias as the reference group with the strongest effect (−2.41 points, 95% CI = [−3.47, −1.35], p < .001), tests with low-to-moderate risk of bias showed a significantly weaker effect (2.22 points less strong, 95% CI = [0.26, 4.18], p = .026).
Discussion
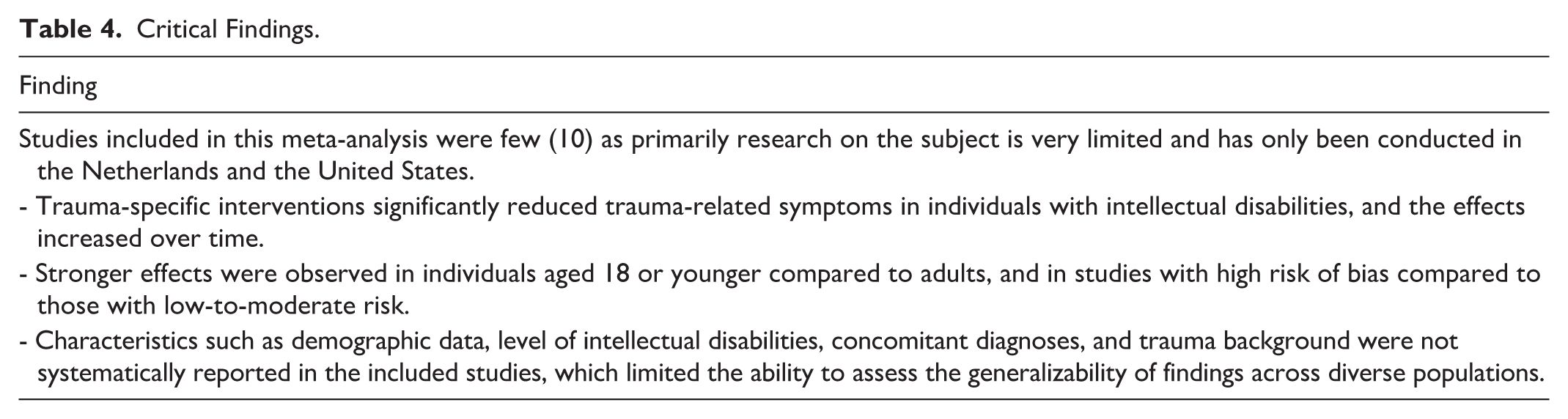
This quantitative synthesis provides evidence that trauma-specific interventions effectively reduce trauma-related symptoms in individuals with ID, aligning with positive expectations noted in previous narrative reviews (Byrne, 2022; Keesler, 2020; Luteijn et al., 2020; Mevissen & de Jongh, 2010). Critical findings from the included studies are summarized in Table 4. Notably, stronger effects were observed on individuals aged 18 or younger, compared to adults. Studies with low-to-moderate risk of bias demonstrated lower effect in comparison to those with higher risk of bias. Regarding differences between treatments, participants receiving the combined KINGS-ID intervention improved more than those receiving EMDR only.
Critical Findings.
The finding that younger participants may experience greater benefits from these interventions could be attributed to several factors. For instance, heightened neuroplasticity in youth may enable them to respond more effectively to trauma interventions, as their brains are more adaptable and capable of integrating new learning and coping strategies (Tymofiyeva & Gaschler, 2021). Additionally, youth often receive greater environmental support, which can enhance treatment efficacy (Bastien et al., 2020; Gkintoni et al., 2024; L. Mevissen & de Jongh, 2010).
Findings also suggest that variations in study quality impact effect size estimates in SCED research. Specifically, a higher risk of bias was associated with greater effectiveness of trauma-specific interventions, highlighting the importance of methodological rigor in future studies to be better able to compare effectiveness of different treatments. This aligns with findings from SCED and traditional meta-analyses, which show that lower-quality studies tend to report inflated effect sizes (Cuijpers et al., 2020; Moeyaert et al., 2021; Tapp et al., 2023).
The current synthesis suggests that trauma-specific treatments were effective for people with ID, nonetheless uncertainty remains regarding which treatments work best for whom and under which circumstances. Only EMDR has been tested within multiple SCED studies, as required for including interventions in guidelines, and proven effective across these studies. TF-CBT was only tested in one study, being part of the KINGS-ID intervention that combined EMDR and TF-CBT (L. Mevissen, Ooms-Evers, et al., 2020). There was a relatively large variation of treatments in this small set of studies. Although KINGS-ID showed superior effectiveness compared to EMDR alone, conclusions regarding relative efficacy remain uncertain because the participants differed not only on treatment but also on other participant-level and study-level characteristics. A recent meta-analysis found that age, sex, nor treatment significantly moderated treatment effects for PTSD in people without ID (Wright et al., 2024). We tested differences in treatments on both male and female and found no differences in effect sizes.
Limitations
When the number of studies is small (10) and when the studies include a limited number of measurement observations within subjects (e.g., L. Mevissen et al., 2017), the standard error of the treatment effects may be underestimated (Baek et al., 2022). We had to exclude a small number of cases due to the lack of variation on the outcome measure, which might have slightly inflated the treatment effect. Ideally, each moderator category would include multiple studies to enable more robust, meaningful comparisons and to enhance the reliability and interpretability of conclusions for the moderator analyses. Moderators had to be tested individually rather than simultaneously in a meta-analytic model, so that their unique effects could not be estimated. Limits to the data also precluded the ID severity moderator analysis and precluded examination of moderator interactions, such as assessing whether the interventions’ effectiveness varied for younger female participants. Although we initially planned to analyze age in years, these data were not always available. Consequently, age was dichotomized (under 18 vs. over 18), reducing our ability to detect more nuanced developmental differences.
The current review synthesized interventions for trauma as defined and assessed by the study authors, which varied from clinically diagnosed PTSD to PTSD symptoms or reports of ACEs. This variation across studies relates to gaps in validated diagnostic instruments for PTSD, in particular for people with moderate-to-severe ID (Hoogstad et al., 2025).
Reliability for the study selection, data extracted, and quality assessment was good within the review team. Results revealed a high risk of bias across most studies, with only one study rated as low and one as moderate. This aligns with other findings indicating the methodological quality in SCED research remains low in psychology and health sciences (Ganz & Ayres, 2018; Jamshidi et al., 2018). Notably, SCED studies included were either Dutch or American, showing a dearth of studies in other locales. Both countries generally adopt the same, DSM-based, definition of PTSD but vary in their criteria for mild ID, with the Netherlands being an international outlier in including people with borderline ID in that group (Orío-Aparicio et al., 2025). This context should be taken into account when generalizing the findings to other countries. For establishing evidence-based treatments, positive results are needed in a minimum of five methodologically strong SCED studies, conducted by at least three different teams at different geographical locations (Kratochwill et al., 2013). These requirements were not met for the reviewed treatments. Without more SCED studies and/or randomized controlled trials, future reviews will continue to face methodological challenges tied to sample size limitations. Increasing numbers of primary studies are needed to examine if individuals with ID with a specific psychiatric phenotype are more likely to respond to a particular type of trauma-specific intervention (Glasson et al., 2020).
Implications for Further Research and Practice
We encourage researchers to reduce the risk of bias to avoid overestimated effectiveness. Bias in this area of research may be reduced in particular by employing concurrent designs and direct inter-subject and systematic replications as well as post-treatment phases (Tate et al., 2013, 2015). To reduce this risk further, reports should provide graphical data displays and key information for each participant. Symptom changes should be measured with instruments with known reliability and validity for the population and time-series observations should be conducted by trained observers with consistent assessment styles.
The importance of addressing publication bias has long been recognized (Cuijpers, 2016; Higgins et al., 2023). Studies with null or non-significant results are less likely to be published, leading to publication bias (Ferguson & Heene, 2012). Including gray literature in meta-analyses, as done in this study, helps mitigate this bias by capturing a broader range of findings (Nair & Borkar, 2023). However, selective reporting and the lack of preregistration present ongoing challenges in SCED research, making it difficult to estimate how many studies with null effects remain unpublished or unreported. Adaptations of methods such as trim-and-fill, funnel plots, and Egger’s test have been proposed for assessing publication bias in SCED studies, but these methods are rarely applied and lack the widespread acceptance seen in traditional meta-analyses (Shadish et al., 2014). Additionally, these adaptations lack validation and are unable to accommodate the complexity inherent in three-level meta-analyses (Pustejovsky & Ferron, 2017; Shadish et al., 2014). We advocate for the creation of a universally recognized SCED preregistration platform to enhance transparency and minimize the risk of overlooking null results. Additionally, future research should focus on developing and validating a specific metric for publication and small-sample bias in SCED meta-analyses to establish it as a widely accepted standard.
The current synthesis demonstrates the feasibility of incorporating repeated measurements and randomized timing of treatment within psychotherapy with people with ID (Tate et al., 2015), which further can be synthesized using meta-analytic techniques (Baek et al., 2023; Moeyaert, 2019; Moeyaert et al., 2017, 2020). Furthermore, there is a pressing need to evaluate intervention effectiveness across levels of ID, as there may be limits to the extent to which trauma-specific interventions can be tailored to the needs of individuals with severe to profound ID. Advancing such approaches would not only strengthen evidence-based treatments but also bridge the gap between clinical practice and empirical research.
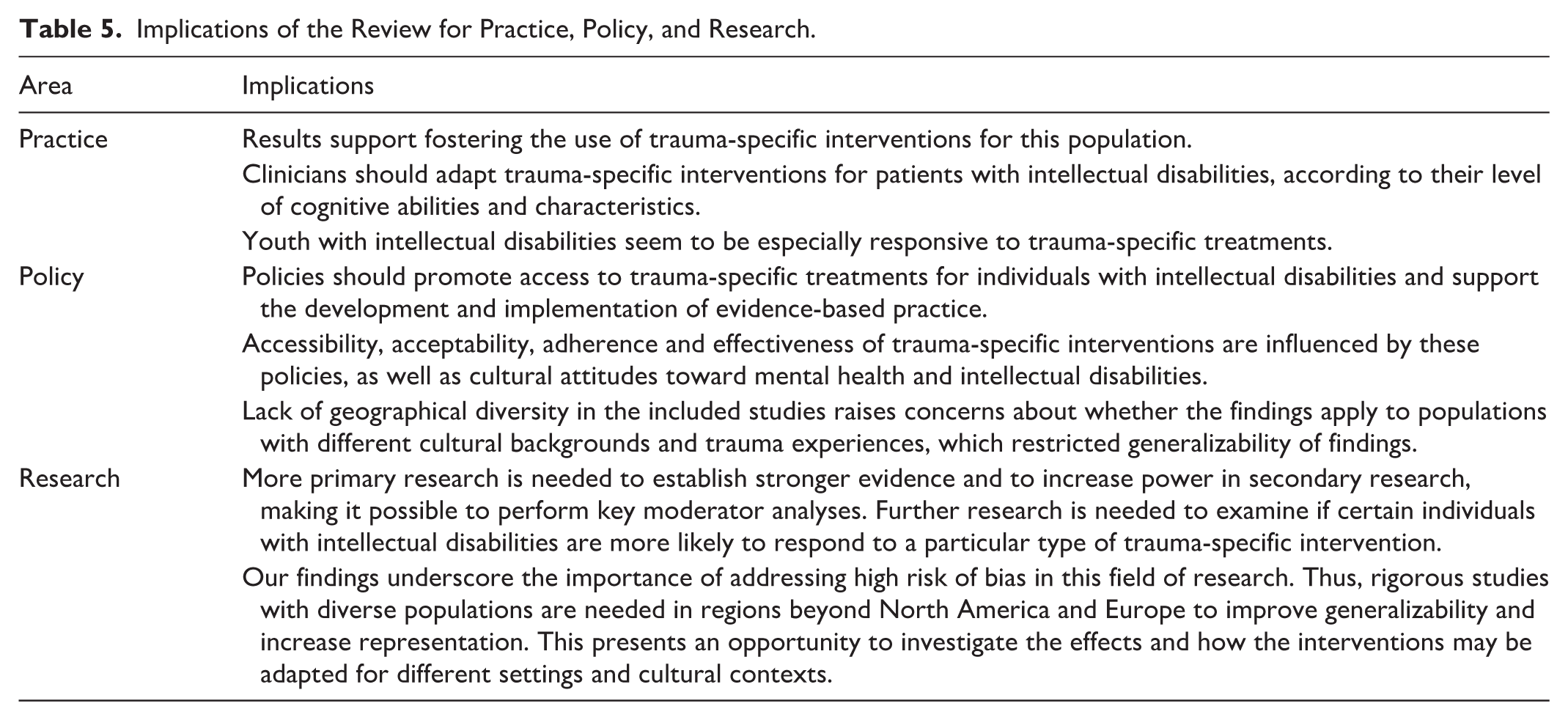
For clinical practice, the findings support the use of trauma-specific interventions for people with ID, while emphasizing the importance of careful monitoring and individualized tailoring given the heterogeneity in support needs within this population (NICE, 2016; Schalock et al., 2021). At present, the limited differences in effectiveness between treatment types, combined with the generally high risk of bias across studies, preclude recommending one intervention as superior. However, EMDR has been evaluated most extensively, including in studies with both high and low risk of bias. Table 5 summarizes the implications for practice, policy, and research.
Implications of the Review for Practice, Policy, and Research.
Conclusion
This meta-analysis suggests that trauma-specific interventions are effective for individuals with ID. However, it remains unclear at what levels of ID severity these interventions remain effective, and the high risk of bias across the included studies introduces uncertainty regarding the reliability of these effects.
Supplemental Material
sj-docx-1-tva-10.1177_15248380261455829 – Supplemental material for Trauma-Specific Interventions for Individuals With Intellectual Disabilities: A Meta-Analysis of Single-Case Experiments
Supplemental material, sj-docx-1-tva-10.1177_15248380261455829 for Trauma-Specific Interventions for Individuals With Intellectual Disabilities: A Meta-Analysis of Single-Case Experiments by Maria Ximena Benavides Corcelles, Carlo Schuengel, Manon Jacomarg Smit and Mariola Moeyaert in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
The authors would like to thank Annemieke Hoogstad and Liesbeth Mevissen for their assistance by sharing the raw data of their SCED studies. Additionally, artificial intelligence-assisted technologies were used for writing assistance and in part of the screening process (ASReview).
Ethical Considerations
This systematic review did not collect and process personal data or involve human participants and was therefore not submitted for ethical review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.