
Abstract
Based on the stimulus–response model of advertising, this study sought to increase admission rates to a local problem gambling service (PGS) in Windsor, Ontario, Canada, by adding a series of locally based 10 foot by 20 foot roadside billboard posters to PGS’s existing communications tools for a 24-week period. Using proof of performance reports, a pre–post survey of new callers to PGS, a website visit counter, and a media awareness survey, the findings showed that at least some individuals were influenced by billboard exposure, but admission rates continued to decline during the billboard campaign period. While one possible explanation for the communications failure was that the whole PGS communications campaign was below the minimal threshold for communications perception, another possible explanation is that the stimulus–response model of advertising used may not have been appropriate for such advertising that targets behavior change. Reflections on using an information-processing model instead of a stimulus–response model, and considerations of a two-step flow of communication, are provided. Recommendations are made regarding matching communications messages to stages of behavior change, use of online promotion, and strategies for future research.
Keywords
The successful recruitment of participants to health promotion programs, intended for their benefit, is one of the most difficult challenges for health promotion practitioners and administrators. In many areas where health promotion services are offered, the number of admissions to services is small compared with the number of people experiencing the problems that the services are mandated to address. For example, McDonald (1999) showed that “most community-based studies and programs have been unable to recruit more than 2% of targeted smokers” (p. 553) to smoking cessation programs. Services for problem gamblers are not dissimilar. The most recent Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 2013) classifies a “gambling disorder” under “Substance-related and addictive disorders” (p. 481) and defines a gambling disorder as “persistent and recurrent problematic gambling behavior leading to clinically significant impairment or distress” (p. 585). Those with the diagnosis must meet at least four of the indicated criteria within a 12-month period. Prevalence studies in the United States indicate that somewhere between 1.7% and 5.5% of the adult population has a gambling problem (Welte, Barnes, Tidwell, & Hoffman, 2011). The Canadian estimate of “problem gamblers” or people at “moderate risk” of problem gambling is an average of 3.8% among the provinces (Canadian Partnership for Responsible Gambling, 2012). However, it is estimated that only somewhere between 7% and 23% of problem gamblers, depending on region, ever seek formal treatment for their gambling behavior (Helen, Cordingley, Hodgins, & Cunningham, 2009), and typically only 1% to 2% of problem gamblers seek treatment in any given year (Rush, Shaw Moxam, & Urbanoski, 2002).
Prochaska and DiClemente’s transtheoretical model of health behavior change, first developed to address smoking cessation, is widely used in the addictions field and other areas of social service delivery. People with addictions are considered to pass through, and rotate to and from, five stages: precontemplation is when the individual is not even considering that there is a problem; contemplation means the person is thinking he or she has a problem but is not engaged in doing anything about it; preparation is when someone recognizes a problem and is taking small steps toward making a change but is not yet making significant changes; action is when the person demonstrates effective changes in behavior, experiences, and/or environment; and maintenance is when the change has been made for a period of time and the individual’s efforts are to prevent relapse (Prochaska, DiClemente, & Norcross, 1992). Relevant to health promotion, a person must reach at least the preparation stage before he or she takes action and actively begins to change (Prochaska & Velicer, 1997). As such, a person with a gambling problem would need to be at the preparation, action, or maintenance stage before he or she would initiate treatment by choice, influenced by advertising for problem gambling services (PGS). Hence, the target audience can be expected to be even smaller than if we targeted gamblers at all stages of readiness to change.
The literature reports on a number of barriers to seeking treatment for problem gamblers, including the impact of stigma, a belief that they don’t have a problem, avoidance (Rockloff & Schofield, 2004), a desire to solve the problem on one’s own (Hodgins & el-Guebaly, 2000), and a lack of information about what professional treatment services exist (Gainsbury, Hing, & Suhonen, 2014; Helen et al., 2009). Given that PGS’s mandate includes making the service known to others, given the little promotion that was occurring about the service at the time, and given an opportunity to receive research funding to study the effectiveness of billboard advertising for recruiting problem gamblers to this service, this study focused on the lack of information about what treatment options exist.
McGuire (1984) identifies five “communication input variables” that can be manipulated when campaigning for service provision use: source, message, channel, receiver, and destination. In McDonald’s (1999) systematic review of the literature, the only significant predictor for the rate of recruitment to smoking cessation programs was the type of “channel” used to convey the message. Although McDonald also found that direct recruitment (such as by telephone) was found to be more effective than indirect mass media type approaches, in the context of problem gambling, a direct approach would be very costly and fraught with ethical issues, given that there is no identifiable list of people who would benefit from PGS, problem gamblers only constitute about 5% of the population, there is significant stigma associated with problem gambling, and many problem gamblers do not acknowledge that they have a problem. As such, we decided to focus on the “channel” variable, but were limited to an indirect approach.
Taylor and Franke (2003) found that organizations using billboards as part of their promotional mix reported that the billboards “do help communicate with and attract new customers, allow for efficient targeting of consumers in a given trade area; and they are cost-effective compared to other media” (p. 151). Based on these encouraging findings, a billboard advertising campaign and research study was conducted for the PGS in Windsor, Ontario, Canada. The purpose of the PGS study was to assist health promotion practitioners and administrators to better understand the use of billboard poster advertising as part of their communications strategies for informing and recruiting clients to PGS. The general research question was, “What communication channels most influence first-time callers to contact PGS?” The specific hypothesis was that the introduction of a series of billboards around the city and surrounding region for a 24-week period would lead to an increase in the number of new admissions to PGS.
Literature Review
Compared with other types of advertising, research studies on the response to roadside billboard poster advertising are uncommon, and studies of their use for not-for-profit organizations even less so (Fortenberry & McGoldrick, 2010; Papas, Logan, & Tomar, 2004). Woodside (1990) reports that the majority of research on outdoor advertising has been limited to quasi-experimental or case study designs. Given the cost of true experimental research, it is expected that this will continue to remain the case. To our knowledge, only a few “true” experiments on outdoor advertising have been undertaken. For example, FTD (Florists’ Transworld Delivery), in 1960, increased its outdoor advertising in all of its promotional cities after it found that markets in which outdoor advertising was prominent demonstrated dramatic sales increases over markets in which the firm ran its usual promotional mix (Woodside, 1990). In 1989, Campbell’s Chunky Soups saw an 8% increase in sales response when the television advertising budget was shifted to outdoor poster boards located near supermarkets (Woodside, 1990). Bhargava and Donthu (1999) provide an example of a nonequivalent control group design in their strategy to promote a not-for-profit conservatory whose attendance had been declining. They included in the design a similar facility as a control condition: A regional science museum whose attendance was also in decline. These authors measured the impact of a 30-billboard campaign that produced 43 gross rating points (GRPs) on a daily basis over a 4-week period. Bhargava and Donthu report that the daily attendance for the conservatory increased 58% during the month of the campaign and 64% in the month following the campaign, while the daily attendance at the regional science museum continued to decline. They attributed the change in attendance directly to the impact of the billboard campaign.
Besides challenges in research design, another limitation in researching the effectiveness of billboard advertising is that the impact of this medium is usually confounded by the use of alternative media, particularly since billboard advertising is typically a support medium for print and electronic advertising as part of a broader campaign (Berneman & Kasparian, 2003; King & Tinkham, 1989). King and Tinkham’s (1989) study is one of the few research projects that sought to address this confounding impact by employing a time series quasi-experimental design to determine whether outdoor advertising alone could create and sustain awareness of an advertising message. They advertised and then tested recall (unaided claimed recall, unaided proven recall, and aided recall) on one fact: “Calvin Coolidge was the 30th President of the United States” (p. 48). To control for presidential knowledge versus campaign exposure, a control survey question asked who the fifth president of the United States was. Among sample respondents, claimed recall was 8.6% prior to the campaign, 38.9% during the campaign, 36.9% 1 month after the campaign, and 35.2% 2 months after the campaign. More interestingly, word-of-mouth activity was 3.9% prior to the campaign, 24.9% during the campaign, 23.4% 1 month after the campaign, and 21.6% 2 months after the campaign. The authors concluded that “once learned, the conscious impressions generated by the campaign appear to have been retained by the population” (p. 51).
More recently, Fortenberry and McGoldrick’s (2010) field experiment assessed the impact of billboard advertising on the patronage of two clinics of an urgent care center which, historically, had not done very much advertising. The authors noted that the cost per contact for billboard advertising was significantly lower than all of the traditionally available media choices of television, magazines, newspapers, the Internet, and radio. They looked at the impact that billboard advertising had on carrying patrons through a simple advertising hierarchy of effects model of awareness creation, information provision, and influence on patronage. They employed a 31-day billboard campaign that used nine 14 × 48 foot bulletins and seven 12 × 24 foot posters to produce a 133 GRPs impact in an area that had a population of 260,000 people. From the 2,380 patients using the clinic during the campaign, 72.7% of the 1,640 respondents were aware of the poster billboard campaign, with awareness of 65.4% among first-time users and awareness of 79.5% among existing clients. In terms of patronage impact, 63.6% of respondents reported that the presence of the billboards moderately influenced their patronage of the clinics.
The literature also provides examples where billboard postings showed limited success. For example, Papas et al. (2004) used a pre- and posttest nonequivalent control group design and found that although there were significantly more oral cancer examinations occurring at the advertised clinics 4 to 6 months after billboard advertising, there was no difference in reports of having seen the billboard campaign. In their community-based participatory research project with a purpose of recruiting women to a physical activity program, Peck, Sharpe, Burroughs, and Granner (2008) found word-of-mouth to be most effective (36%), newspaper advertisements the next effective (29%), and billboards the least effective (1%). These results, which conflict with other more positive results from billboard studies, highlight the importance of continued research on approaches to billboard use.
Billboard Campaign Setting for the Current Research Study
This study was conducted in Essex County, the most southwesterly county in Ontario, Canada. The core city, Windsor, is directly adjacent to Detroit, Michigan, in the United States. At the time of the study, the population of Essex County was considered to be 482,000 by the outdoor medium provider. Apart from Internet gambling services and options to purchase lottery tickets (which are ubiquitous), Essex County had three types of gaming venues, including one casino, one racetrack, and several bingo halls.
There is no prevalence data available for gambling problems specifically for Essex County. Given the accessibility to gaming venues in the County, and neighboring Detroit, intuitively one would expect the rate of problems to be at or above the general prevalence rates found in the literature. As previously stated, it is estimated that among Canadian provinces, there is an average of 3.8% who are “problem gamblers” or people at “moderate risk” of problem gambling (Canadian Partnership for Responsible Gambling, 2012). Consequently, for a Canadian population of 482,000, one would expect somewhere around 18,000 to 19,000 would have, or be at risk of having, a gambling problem. Given the statistic that only 1% to 2% of problem gamblers seek treatment in any given year (Rush et al., 2002), we would expect that approximately 180 to 380 of these people would be disposed toward seeking treatment in any particular year.
PGS, sponsored by one of the main local hospitals, has been in operation since 1994 (Hotel-Dieu Grace Healthcare, http://www.hdgh.org/problemgamblingservices) and uses a best-practices service model based on recommendations by the Centre for Addiction and Mental Health, Canada’s largest mental health and addiction teaching hospital and a world leader regarding addiction and mental health research (Centre for Addiction and Mental Health, 2012). Because of its demonstrated effectiveness for gambling disorders (Larimer et al., 2012; Petry, 2005; Petry et al., 2006), service providers at PGS are trained in cognitive–behavioral therapy, an approach that challenges cognitive distortions and addresses associated maladaptive behaviors. PGS is the only provider in the region and as such does not compete with other services. For gamblers, this service offers individual counselling, group counselling, day treatment, residential treatment, and aftercare services. For family members and friends of people with gambling problems, the services provide support and education through individual and group counselling, and through a 2-day family workshop. PGS has a residential program, but because most of its clientele were from outside the geographic area, the residential service was not included in the analysis of this study.
Prior to the initiation of the billboard poster campaign, PGS promoted their services via the following: a Yellow Pages listing and a White Pages listing in the local telephone directory; a newspaper insert called “The Chase” distributed four times a year in the only local newspaper—The Windsor Star (Circulation 89,000 households in Essex County); the PGS website (which did not contain a hit counter) that the newspaper insert referred to; the sponsoring hospital’s website; posters at the casino and bingo halls; a provincial problem gambling hotline; a responsible gambling information centre; and occasional but not recent community presentations.
PGS data indicated that on average, over the 3 years prior to the study, approximately 325 problem gamblers and 160 family members of problem gamblers attended the outpatient program per year. The number of “new” admissions per year was about 230 for gamblers and 110 for family members. While these numbers were aligned with the expectations stated in the literature, at the time that the current study was being proposed, there were concerns expressed by the manager and the staff that the number of outpatient clients had begun to decline over the previous year. Distribution tables were created demonstrating monthly admissions rates to treatment (N = 99, M = 32.46, SD = 10.8, range = 10-68, and skewness = .901); and monthly first-time callers (N = 61, M = 99.41, SD = 39.97, range = 30-202, and skewness = .653). When the Z-scores of monthly admissions 15 months prior to the campaign implementation were observed, there were 11 negative scores, and in the 6 months prior to the campaign implementation, they were all negative, indicating a below average admissions pattern had developed. In the Essex County context where social service agencies, such as PGS, are accountable to the government for funding, and at a time of budget cuts and increased competition for funds, such a decline in admission rates puts the agency at risk of reduced funding or even losing funding. Furthermore, around the globe, problem gambling treatment providers were questioning why the prevalence of people seeking treatment was so low. For all these reasons, PGS initiated the current study as part of efforts to raise awareness about PGS.
Communications Approach for Problem Gambling Services
The measurement of advertising impact of any communications effort varies in terms of the objectives of a communications campaign. The implementation of this study was implicitly based on the stimulus–response approach to advertising, the model of advertising that typically has been used (Weilbacher, 2003): Organizations advertise (the stimulus) and then await response. The response can then be compared with historical levels to see if there has been any change. The kinds of responses can vary from behavioral responses, such as sales change, phone calls, website hits, and page views. Alternatively, perceptual measures of advertising response can be made, including satisfaction ratings, attitudes, and awareness of the advertising in terms of recall. Finally, simple audience exposure to the advertising can be measured in terms of the ratings of the promotional campaign’s GRP or cost per thousand. The expectation in this study was that the “stimulus–response” approach to the billboard postings would increase awareness about PGS, which in turn would lead to more gamblers and family members of problem gamblers contacting PGS to receive services.
Fortenberry and McGoldrick (2010) comment that “careful planning of creative billboard treatments and appropriate scheduling patterns are essential to maximize their communications potential” (p. 81). Edgar and Volkman (2012) recommend giving careful consideration to three communications theories when developing messages: “The activation model examines individual needs for stimulation and the likelihood that messages will attract attention and continue to engage, depending on the audience’s need for sensation seeking” (p. 588); the extended parallel process model “is a useful tool for understanding how to construct effective risk messages that are grounded in fear appeals and scare tactics” (p. 588); and with Fisher’s narrative, “people are essentially storytellers and that we live in a world full of stories. When people hear another’s story, it helps provide an understanding about the world (e.g., an illness experience helps us understand more about the illness itself)” (p. 589).
The billboard research studies described above do not refer to these three communications theories. This study contributes to the literature because we gave considerable attention to all three. With respect to the activation model, we sought to target problem gamblers at the preparation, action, and maintenance stages of change, which would be those who would willingly initiate contact with PGS without an external mandate. To assess the unique needs of problem gamblers and family members of problem gamblers, and aligned with Fisher’s narrative approach, four focus groups involving a total of 17 problem gamblers and 14 family members of problem gamblers were held to hear their stories and to obtain feedback on sample creative executions developed from a search of the Internet and in collaboration with a local advertising agency (Calderwood & Wellington, 2013). We acknowledge that the two photographs on the billboard (shown in Figure 1) do not provide the audience with the same level of “narrative” that one can offer in an auditory television/radio advertisement or print material that has space for lengthier messaging. However, the idea of the two photographs, indicating a shift from a happy family to a broken family, came directly from focus group consensus about what best summarized their “story” and what led to them seeking support from PGS (Calderwood & Wellington, 2013).

One of the Eight Billboards Posted
Four variations of the family photograph were used (two posters for each of the four variations), with the goal of being relevant to a broad range of socioeconomic, race, and gender profiles: one with an African Canadian woman and African Canadian family; one with a White man in a business suit and mixed race family; one with an ethnic looking man in a sports shirt and a White family; and one of a White woman and White family. Based on the advice of focus group participants, for each pair of posters, one of the pair stated, “GAMBLING AGAIN? SHATTERED?”, and the other of the pair stated, “GAMBLING PROBLEM? SHATTERED?” This was important for addressing stage of change, as focus group participants felt that some potential clients may not be ready to outwardly admit that they have a “problem.”
It is noteworthy that the communications message is not intended to directly change gambling behavior, but to encourage gamblers, who are ready or getting ready to change, to make contact with PGS. PGS’s philosophy, aligned with best practices (including what is known as motivational interviewing) does not support the use of “scare” tactics. Their approach is one of “support,” including a harm reduction approach for clients who are not “ready” for abstinence. As such, a fear appeal model was intentionally not used. Based on the results of our focus groups, our intended audience (at preparation, action, or maintenance stages) typically were not in healthy family environments at risk of a future broken family. Rather, they had already experienced the breakdown of relationships and so could “identify with” the broken family photograph (Calderwood & Wellington, 2013). As such, the intent of the broken family photograph was not to scare those in healthy family relationships but to attract those who were at a point in their gambling process of being ready to make changes.
Method
Design
As indicated above, true experimental designs are typically not feasible for this type of research. As Woodside (1990) indicates, “where it is not possible to create randomized treatments and control groups, a self-critical use of quasi-experimental designs is recommended” (p. 230). Because of the unique nature of the setting for this research, and financial constraints, it was not possible to find an appropriate control city for comparison. As such, this study used time series data, analyzed according to a pretest–posttest quasi-experimental design. Four to eight billboards were posted over a 24-week period. Based on demographic data available from PGS at the time of the study, and on inconsistent empirical results regarding socioeconomic status as a risk factor (e.g., Gainsbury, Russell, & Blaszczynski, 2014; Johansson, Grant, Kim, Odlaug, & Gotestam, 2009), we had no reason to target any particular neighborhood more so than another. Our preference was to post billboards close to the local casino downtown, and close to the racetrack, but we were unable to do so because of city bylaws that only allowed posting in approved designated areas. As such, the postings occurred in commercial areas spread throughout Essex County. The billboards changed location in 4-week cycles to reach a wider audience and to reduce the potential for message wearout (Fortenberry & McGoldrick, 2010). As part of the poster campaign, a more memorable website address (www.gamblerhelp.ca) along with the addition of a counter to measure website visits was provided for the existing PGS website whose base address was associated with a more lengthy and complicated sponsoring hospital’s homepage.
Data Collection
This study was approved by the University of Windsor and the sponsoring hospital’s Research Ethics Boards. Five measures were used to address the question about which communication channels most influence first-time callers to contact PGS. First, the location GRP ratings measured by the Canadian Outdoor Measurement Bureau were reported to the outdoor medium provider who supplied them to the investigators as proof of performance. Second, the number of new referrals was monitored, graphed, and compared with baseline data found over the previous 3.5 years. Third, for 4 months prior to the first billboard posting, first-time callers to PGS were specifically asked by PGS secretaries, “Where did you learn about our service?” Secretaries were instructed to check “Yes” for each location the caller mentioned on a predetermined list of all the communication channels that PGS uses, including one bogus item—posters at a local grocery store—to assess overclaiming. Secretaries continued to ask the caller “Did you hear about the service from anywhere else?” until the caller stated each location that came to his or her mind. Once the caller could no longer think of other locations, the secretary asked specifically about the remaining locations on the list and checked off “yes when prompted” or “no recall” depending on the caller’s response. Secretaries were instructed to ensure that every row had one check mark.
The fourth data collection method included a website counter to measure the number of visitors to the PGS website, and an anonymous website survey containing seven questions: “How long have you been aware of our service before visiting this site?” “Where did you get the information that led you to this website?” with a checklist of all the options of where PGS advertises their website, as well as search engines. Respondents were also asked how likely they were to call PGS for an appointment, and for information. If they said they do not plan to call, they were asked for the reason. All respondents were asked how helpful the website had been and for suggestions for changing the website. Finally, for 1 month at the end of the 24-week billboard posting period, PGS secretaries and counsellors were requested to have all current or first-time clients, waiting for an appointment in the waiting room, complete a survey. This survey first asked, “Before you ever came to PGS, what source(s) of communication do you recall that informed you about us (please check all that apply)?” Respondents were provided the same list the secretaries used for the baseline survey with an option to place a check mark indicating “Yes” beside each item. On the following page, respondents were asked, “Now that you have attended services here at PGS, where do you notice communications about PGS (check all that apply)?” Again they were provided with the same list and the same option to check off “Yes” beside the relevant locations. On the next page, a photograph of one of the billboards was depicted, and respondents were asked, “In the past 6 months, have you noticed this billboard or a similar billboard advertising help for problem gambling in the Windsor area?” If so, respondents were asked a series of questions about when and where they saw it, how often, what mode of transportation they were using, and the impact it had on them. All respondents were asked, “If you had seen this billboard at the time that you were beginning to think about getting help for your gambling concerns, or for those of your family member, what would your first reaction have been?” and “If you had seen one of these billboards around the time you were beginning to think about getting help, how likely would you have been to call the number or visit the website displayed on it?” This survey ended with a request for the respondents to provide any other feedback about the billboard that they thought would be helpful in attracting more clients to PGS.
Results
Exposure to the Billboards
Based on the outdoor media provider’s proof of performance report, on average, an estimated 18.94% of the population (about 91,290 people) in the outdoor market coverage area of 482,000 people was exposed to the billboard posters on a daily basis throughout the billboard postings. During the first 4 weeks and the last 4 weeks of the campaign, the audience exposure was estimated to be as high as an average of 27.4% (132,068 people) and as low as an average of 10.8% (52,056). If one relates the values shown in the proof of performance report to the estimated prevalence of problem gamblers provided in the Canadian literature (3.8% as indicated above), then the effective reach over the duration of the campaign was 3,651 problem gamblers or those at moderate risk of problem gambling (the outdoor media provider’s estimated population of 482,000 × 3.8% × average market coverage of 18.9383% = 3,651). Given that the target audience for the billboards was problem gamblers who were ready or close to ready to seek treatment (and family members regardless of stage of change for the gambler), our expected number of problem gamblers who might call PGS for the first time is even smaller than the total estimate of the number of gamblers in the community. However, we were not able to estimate how much smaller. Some research has studied the reliability and validity of stages of change assessment instrument (the URICA) and treatment outcomes of problem gamblers seeking treatment at the range of stages (e.g., Petry, 2005), but no one has reported on the distribution of stages of change among those seeking treatment for problem gambling or what stage of change gamblers need to be at to notice advertising about available services. We could not find any research on the stages of change for family members of problem gamblers.
Number of Admissions
Figure 2 graphs the number of admissions to PGS for the billboard posting period and the 3.5 years prior to the billboard postings. It is noteworthy that these numbers include new clients to the service as well as returning clients. As indicated in the “Billboard Campaign Setting” section above, the numbers were declining just prior to the billboard postings. Figure 2 shows that for the 6 months of the billboard posting, a total of 118 calls to initiate service were made (30, 15, 31, 10, 10, and 22 per month, respectively). This total is down from the 218 calls made in the same months the previous year (29, 28, 68, 40, 36, and 17 per month, respectively). The spike of 31 during the study period and 68 the previous year were for January, when it is common to have an increase because of people’s New Year’s resolutions. Not only were the 118 total during the billboard postings less than the previous year, but the numbers were the lowest they had been in at least 3.5 years.
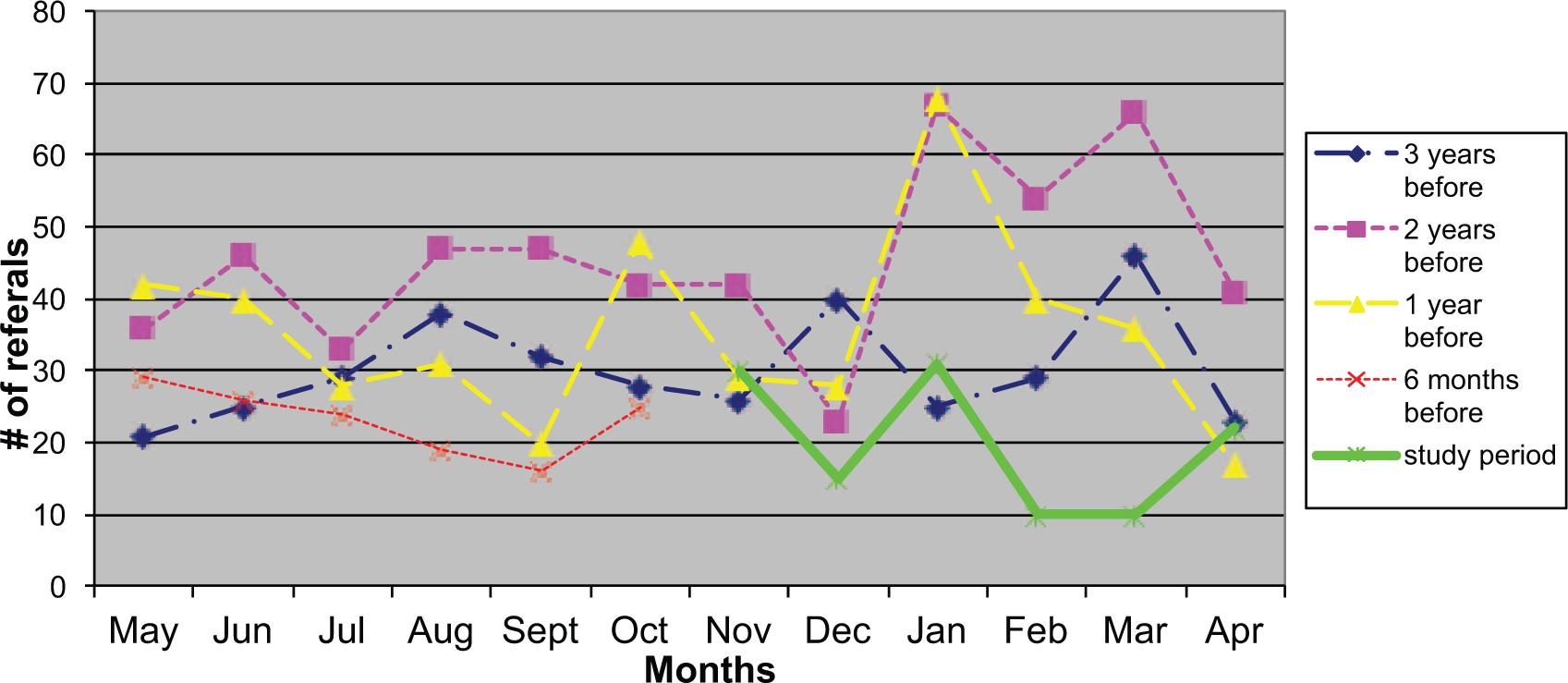
Admission Numbers for the Billboard Period and 3.5 Years Prior to the Billboard Postings
How First-Time Callers Learned About the Service
Due to new admissions being processed in a range of ways throughout a 24-hour day, the number of people who responded to the question about how they learned about the service was only 68, among which 4 reported having seen the billboard (3 when asked specifically about the billboard and 1 when asked how he or she learned about the service). As shown in Table 1, the main sources of information that first-time callers indicated for how they learned about PGS during the billboard campaign were personal communication sources (33.8%), the PGS listing in the telephone book (25.0%), followed by the Casino (16.2%), and the provincial Problem Gambling Hotline 1-800 number (8.8%). The billboard posters produced a 5.9% response during their actual posting period, the same rate of response as for the sponsoring hospital’s website or the agency newspaper insert. The percentage of respondents indicating bingo halls and the Responsible Gambling Information Centre as sources of information were lower at 4.4%. No one responded to the bogus option of “posters located at a local grocery store,” suggesting that little if any overclaiming was occurring. Table 1 compares the number of admissions to PGS during the 4 months before the billboards were posted to during the 24-week billboard campaign. A Pearson’s Chi-square analysis was used to compare the pretest group with the group exposed to the billboards, showing a statistically significant increase in “personal influence” as the means by which the poster campaign group learned of the service as compared with the manner in which the pretest group learned of the service. A marginally significant increase was found in the use of the telephone listings to learn of the service during the billboard postings.
Baseline and During Billboard Posting Measures of How First-Time Callers Learned About PGS (in Order of Frequency During the Billboard Posting)
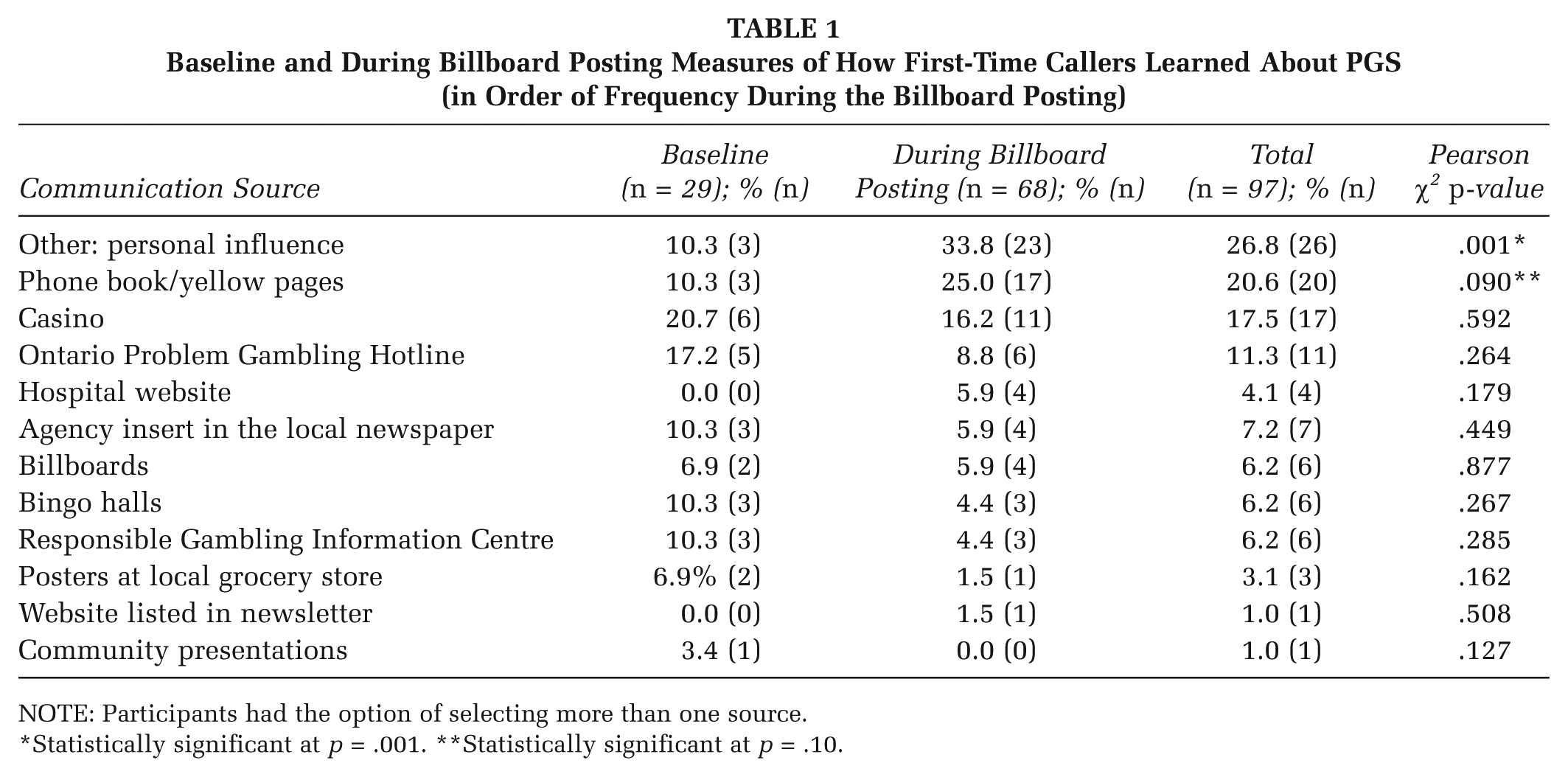
NOTE: Participants had the option of selecting more than one source.
Statistically significant at p = .001. **Statistically significant at p = .10.
Website Survey
More than 600 visits to the PGS website occurred during the posting period, and 28 visitors responded to the voluntary online survey producing a 4.67% response rate. The most common way respondents arrived at the website was through information provided by a search engine, such as Google (28.6%). The next most frequent method was via the roadside billboard posters (n = 3; 10.7%), which was the same frequency for personal communication through a family member or friend, and the same as personal communication through a health care professional. Less frequent (7.1%) were the sponsoring hospital website link, the PGS brochure, the provincial Problem Gambling Helpline, and the Responsible Gambling Council. Only one person arrived at the PGS website through information obtained at a gaming facility, and no one indicated having received information from the agency newspaper insert.
Existing PGS Clients’ Reports of Source of Communication(s) They Recalled
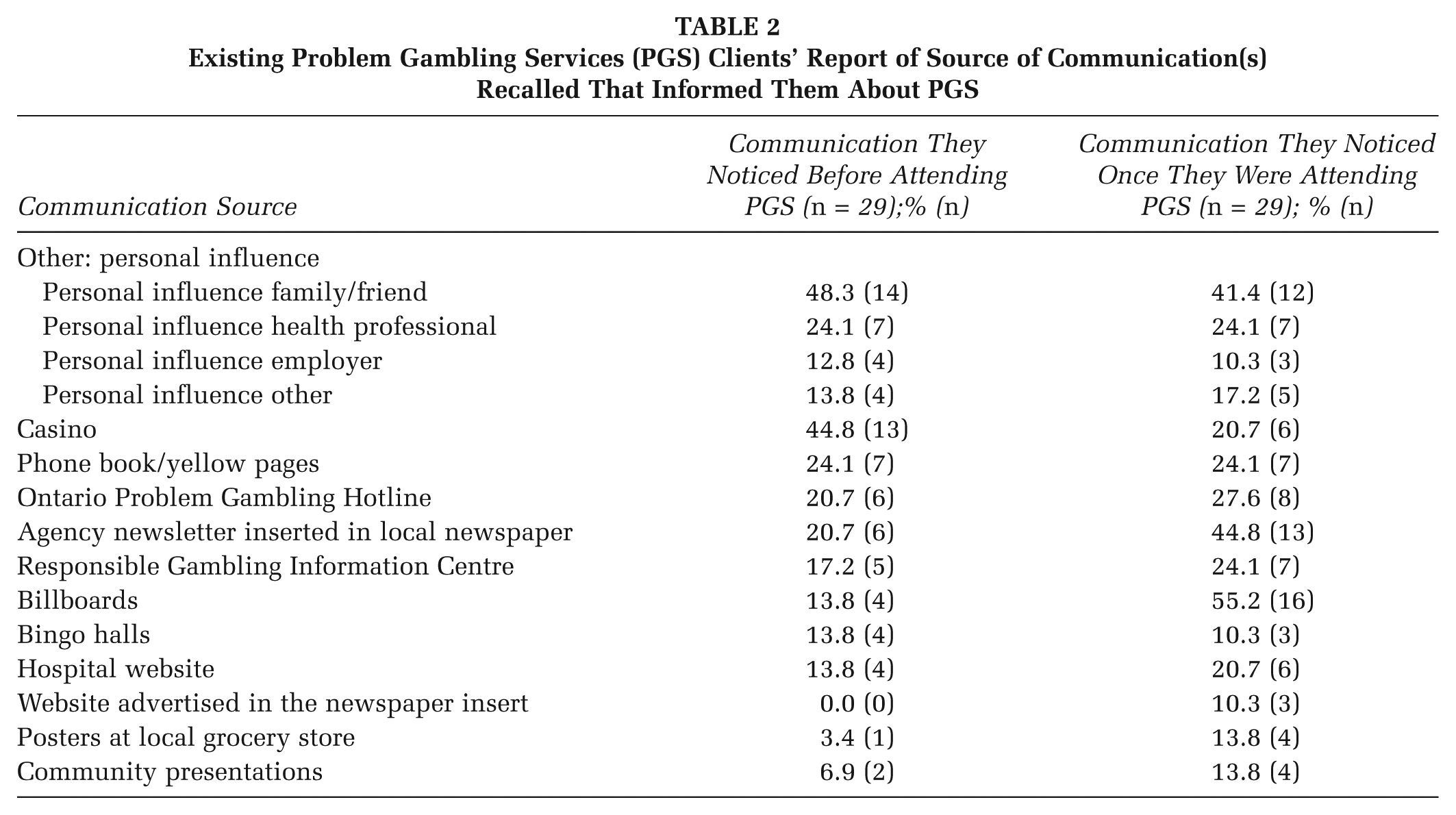
Despite having a client base of over 100 people visit PGS during the month when the survey for existing and incoming clients was administered, only 29 participants completed the survey to provide feedback about communication sources they recalled having informed them about the service. The secretaries and counsellors reported that in many instances it did not seem appropriate to request clients to complete the survey if they were in crisis or distress. Table 2 shows that 16 (55%) of the 29 participants reported having noticed the billboard posters. Of the 16 who noticed the billboards, only 6 indicated they “learned about the service” through the billboards. Using “aided recall,” another 10 respondents remembered they had seen the billboard posters once they were presented with a photograph of one. Again, participants were provided with the bogus option of indicating posters on display in a local grocery store—the fact that no one identified this option suggests that participants were not confabulating their memory of the billboards. When asked about what could be changed about the billboard to make it more effective, responses consistently indicated that the billboard itself did a good job of portraying the intended message.
Existing Problem Gambling Services (PGS) Clients’ Report of Source of Communication(s) Recalled That Informed Them About PGS
Discussion
Recognizing that the outdoor medium provider that offered the billboard poster service has an inherent bias toward claiming high exposures, and given that local prevalence data (particularly for those at the preparation, action, and maintenance stages) for problem gamblers was not available, a fully reliable estimate of exposure to the billboard posters by problem gamblers is difficult to ascertain. However, given that a continued decline in new admissions occurred during the study period, we can conclude that at least in this case there is no support for the hypothesis that “the introduction of a series of billboards around the city and surrounding region for a 24-week period would lead to an increase in the number of new admissions to PGS.” As shown in Figure 2, for part of the study period, the numbers were the lowest they had been in years. Intitially, the investigators speculated that the lack of response was likely because the communications effort was below the advertising threshold of response. Within the stimulus–response model of advertising, the term threshold refers to “that level of advertising which precipitates an initial response, defined in some way, on the part of an individual or group of individuals. It is assumed that below this level advertising has virtually no effect” (Corkindale & Newall, 1978, p. 331). The campaign averaged only 18.9 GRPs although it did have a peak period of 27.4 GRPs. As described above, Fortenberry and McGoldrick (2010) had a campaign with 133 GRPs, and King and Tinkham’s (1989) campaign had 100 GRPs. Fortenberry and McGoldrick (2010) indicate that effective campaigns require at least 100 GRP’s to have sufficient impact. Bharghava and Donthu (1999) suggest that between 35 and 45 GRPs are needed to generate measurable campaign results. Regardless of the required GRPs for an impact, in this study, it could be concluded that with such low GRPs, PGS is not doing enough communication to have any impact. However, this conclusion is belied by the fact that the majority of clients using the service reported learning about it from one of many sources of communication employed by PGS.
Weilbacher (2003) argues that the stimulus–response model of advertising is inappropriate, that realistically, consumers use an information-processing model when they encounter information, and that advertised products or services will only be perceived by consumers who are already predisposed to receive them. This view of advertising fits with the transtheoretical model of health behavior change (Prochaska & Velicer, 1997), which suggests that unless a problem gambler is in the preparation stage of change, or beyond, they will not notice the advertising. This model has empirical support for problem gamblers based on the reported findings of Rush et al. (2002), who note that typically only 1% to 2% of problem gamblers seek treatment in any given year. The implication for health promotion communicators is that because the timing of when an individual will come to realize they need treatment for their gambling problem is uncertain, the timing of communication of the availability of services cannot be uncertain. Thus, we suggest there may be a need for a continuous and highly visible communications presence by organizations like PGS.
The statistically significant increase in “personal influence” (33.8%) as the means by which those exposed to the billboards learned about the service, and the marginally significant increase in the use of the telephone listings (25.0%), are consistent with King and Tinkham’s (1989) finding of an increase in word-of-mouth influence associated with a billboard campaign. These findings suggest a two-step flow of communication as described by Krugman, Reid, Dun, and Barban (1994): Even if a billboard campaign did not evoke a direct stimulus–response link in the form of an individual seeing the billboard and then calling PGS, that increasing awareness of the service in the general public’s mind (including friends, family members of gamblers, and health care providers) could have led to discussions about problem gambling, and recommendations being made through word-of-mouth. Similarly, because individuals were most likely operating a vehicle when they viewed the billboard, they could not easily write down the phone number. Instead, they may have used the phone book to aid their recall some time later after having seen the billboard. As such, it is possible that the billboards were having an indirect impact.
It is noteworthy that the rate of learning about the service through the billboards (5.9%) was the same as the rates for learning about the service through the sponsoring hospital’s website and through the agency insert in the local newspaper. Moreover, the fact that four (5.9%) first-time callers indicated having seen the billboards suggests that the billboards were influencing at least some individuals to make contact with PGS. Given that the typical response rate of billboard posters has been reported by Shipman (1994) to range from 1.8% to 2.8% and some studies, such as Peck et al. (2008), reported a billboard response rate of only 1% for recruiting women to a physical activity program, the finding that 5.9% of new callers indicated that they learned about PGS via the billboard campaign could actually be interpreted as a success. Furthermore, although only 6 of the 29 current clients who completed the survey about the billboard indicated having learned about the service through the billboards, 10 more of them indicated having seen the billboard with aided recall after being presented with a photograph of one of the billboard posters. While not as meaningful as the numbers indicating a self-report of having learned about the service, this total of 34.5% suggests that the billboards were being noticed by a number of problem gamblers and family members of problem gamblers, despite not spontaneously indicating having seen them. Although not as impressive as the 72.7% reported by Fortenberry and McGoldrick (2010), who had a campaign with 133 GRPs, the findings in this study still suggest the billboards were having some impact with an average of 19 GRPs. From a social service perspective, it is not only important to consider statistical significance but also clinical significance. Although the increases in calls was not significant, any evidence of an “impact” (e.g., at least six website visitors getting to the website because of the billboards) is meaningful when we know of such a high cost to the individual and society due to problems related to gambling.
The decline in number of new admissions, both during the study and prior to the study, remains a concern. In New Zealand, Abbott (2007) reports a noted unexplained trend since 2005 of a reduction in new helpline callers and new clients seeking counselling for problem gambling, so it may be that this is part of a general trend affecting many geographic regions. There were a number of possible explanations for the study findings. For example, gamblers and family members may have been seeking and receiving the help and/or support they needed from alternative sources, particularly since recent years has seen a surge of Internet options and a surge in the amount of education and training about problem gambling for the general public and for health care providers (e.g., clergy, physicians, and Employee Assistance Programs). People concerned about gambling may have been accessing self-help options, such as books, online information and chat groups, or Gamblers Anonymous. The fact that more than 600 visits were made to the PGS website during the 6-month study period is good evidence that online resources were being used. Furthermore, no one has researched the reputation of gambling services, and in particular how the reputation compares with that of self-help groups and online options. It may be that over time the PGS has become less reputable, and other options more reputable, but to date, we do not have data to examine this.
Recommendations
We recommend that health promoters be cautious about the stimulus–response model of advertising and give careful consideration to the information-processing model of behavior described by Weilbacher (2003), which indicates that communication needs to be constantly present in some form so that it can be seen when people are ready to perceive it. This model is consistent with the transtheoretical model of health behavior change that has been used for decades in the treatment of addictions; people must be ready for change before certain communications strategies can be effective. This suggests that a certain threshold of communication needs to be consistently present in the catchment area where services operate and locations close to gaming venues, so that it is available at the time an individual is “ready.”
Barriers to providing consistent advertising in fixed locations would need to be addressed. First, the focus of this study is on not-for-profit organizations, typically known to have small, if any, advertising budgets. We recommend that not-for-profit organizations have a sufficient budget allocation to carry out the advertising and evaluation of the advertising. Perhaps the budgeting for treatment services and health promotion program communications should be determined and allocated separately to avoid the dilemma of funding communications at the expense of treatment or vice versa. Second, choosing a location close to the support services and to gaming venues may not be viable because of city bylaws (as was the case in this study), so advocacy and creativity may be required to find “meaningful” locations for billboard postings. Third, with such a recent increase in online use, which is only expected to increase even further, we recommend future initiatives explore advertising through electronic means, such as chat rooms, websites, and twitter. Social services, if not already, should be considering how to provide services online, as already many chat rooms and online supports exist and are in competition with in-person services. Studies need to be conducted to compare the impact of roadside billboard promotion with online advertising, which in many instances might be much less expensive and might have the potential to reach a larger target audience. Fourth, the view of “fixed” locations, facilitating a presence at the time an individual becomes “ready” to perceive the message, contradicts a concern expressed by Fortenberry and McGoldrick (2010) about advertising “wearout.” If a billboard remains in the same location for too long, people stop noticing it because it becomes commonplace. Again, further research is required to assess whether a fixed location or rotating locations is more effective with populations similar to problem gamblers.
In this study, the findings across a range of communication sources indicate the importance of multiple channels, multiple messages, and multiple paths. We also highlight the importance of evaluating the effectiveness of all channels, messages, and paths. As discussed above, it is important to measure and consider both direct and indirect impact as a two-step flow of communication may be occurring. In this case, PGS had no data assessing the effectiveness of their preexisting communication channels, making it difficult to draw conclusions about changes to word-of-mouth, and telephone influences, seen during the billboard posting period. We recommend for future studies that formative research examining existing communication channels and level of awareness be conducted prior to such a study. Particularly, given that PGS also provides services to family members of problem gamblers, it is important to study the influence that family members have in the process of recruiting gamblers to services. Furthermore, given that the agency was not used to this type of continuous evaluation, response rates were low, making it difficult to draw conclusions from the surveys that assessed this one 24-week billboard posting period. Given the low response rate for the online survey, we recommend that researchers consider incentives for future online surveys. Strategies would have to be implemented to ensure the same respondent did not repeat the survey numerous times to obtain compensation. And there are ethical considerations if the compensation is to put their name in a draw for a prize—a form of gambling (which in this case we are trying to dissuade). Given the low response rate for existing clients, we recommend that researchers have a strong collaborative relationship with receptionists and other staff who are administering the survey, to monitor and encourage more compliance, and/or to identify barriers to survey completion early enough in the study to develop strategies to minimize a low response rate.
In keeping with Edgar and Volkman’s (2012) recommendation to use the activation model and consider “narratives,” we highly recommend input from service users for any promotional campaign, such as the focus groups held at the start of this study (Calderwood & Wellington, 2013) and service user surveys. For example, in this study, we learned from participants to expect that promotional messages and campaign themes designed to encourage people to contact PGS for the first time would differ from the approaches designed to reinforce the altered behaviors of people who have participated in treatment and wish to maintain their abstinence or harm reduction behaviors. Part of obtaining feedback from service users should include the extended parallel process model, as described by Edgar and Volkman, to assess whether service users would be motivated by fear tactics. We suggest that depending on stage of behavior change, fear tactics may not be appropriate. Furthermore, it is important that we also reach out to service users to obtain their views about the reputation of gambling services, and in particular how the reputation compares with that of self-help groups and online options. This would contribute to our understanding of general admission declines across geographic regions.
Footnotes
Acknowledgements
We sincerely acknowledge the contributions made by Nick Rupcich, Mirna Karkanawi, Evelyn Smith, staff, and clients at the Windsor Regional Problem Gambling Services. We also thank Dr. Ron Frisch, Melissa Simas, Marina Denisova, Kristina Verner, and Jason West at the University of Windsor. In addition, we appreciate the input provided by the participating advertising companies.
This project was funded by the Ontario Problem Gambling Research Centre and the Windsor Regional Hospital, Windsor, Ontario, Canada.