
Abstract
Childhood obesity remains a public health problem requiring mobilization across diverse social and political sectors. The faith-based sector can contribute to obesity prevention advocacy when existing resources are supported and leveraged. This article describes an advocacy resource assessment conducted in six Chicago faith organizations. Key administrators and congregation members were surveyed to identify organizational resources that could be mobilized for childhood obesity prevention advocacy. Survey data were analyzed using SPSS and Excel. Descriptive statistics were calculated for each organization and for all combined. Organizational resources for advocacy were identified, with varying degrees of resources within organizations. Congregation members and faith leaders expressed interest in advocacy training and activities but acknowledged competing organizational priorities. Participating organizations received a stipend to pursue recommended action items based on their assessment. Faith organizations have unique resources and human capital and can be key partners in childhood obesity prevention. Conducting an assessment prior to planning interventions and advocacy approaches can strengthen partnerships, leverage assets among partners, and ensure efforts are relevant and beneficial for faith organizations. It may also be strategic to incorporate funding in grant budgets in order to empower faith organizations to act on findings from the assessment process.
Keywords
Introduction and Background
Childhood obesity persists as a critical public health problem, with contradictory evidence of a decline in national rates for any age-group (Ogden, Carroll, Kit, & Flegal, 2014; Skinner, Perrin, & Skelton, 2016). Disparities continue, with children in low-income and racial and ethnic minority neighborhoods at greatest risk (Ogden et al., 2014). A social ecological approach is necessary to address this issue, with multilevel strategies focusing on contributing factors ranging from individual knowledge to public policy (Davison & Birch, 2001). Faith organizations can be effective loci for change because of their deep-rooted experience in social change movements (Campbell et al., 2007) and prominent role in communities (Demark-Wahnefried et al., 2000).
In a review of the public health literature, faith organizations have historically participated in primary prevention activities that have overall been found to improve health outcomes (DeHaven, Hunter, Wilder, Walton, & Berry, 2004). Intervention studies have focused on individual behavior change within faith organizations comprising primarily minority populations (Davis, Goldmon, & Coker-Appiah, 2011; Resnicow et al., 2002). Faith-based childhood obesity prevention interventions have been tailored to the individual organizational level (Reifsnider, Hargraves, Williams, Cooks, & Hall, 2010). A 2013 study by He et al. detailed a sample of Latino church leaders’ perspectives on childhood obesity. However, to our knowledge, there is no existing published literature that reports on a childhood obesity prevention assessment focused on advocacy among multiple faith organizations that included faith leaders and members.
Recognizing the power of the faith community as partners in public health intervention, the Robert Wood Johnson Foundation previously initiated its Faith-Based Advocacy: Galvanizing Communities to End Childhood Obesity program and funded the Consortium to Lower Obesity in Chicago Children (CLOCC), a program of the Ann & Robert H. Lurie Children’s Hospital of Chicago, and its project “Chicago Faith-Based Advocacy to Improve and Transform Health” (Chicago FAITH). The goal of Chicago FAITH was to support Chicago faith leaders and organizations to drive childhood obesity prevention advocacy and environmental change. The Chicago FAITH project’s steering committee (Chicago FAITH steering committee) comprised three CLOCC staff and eight leaders of faith-based or faith-focused organizations. The Chicago FAITH steering committee guided all project components. The project components included childhood obesity prevention advocacy trainings for faith organizations, seed grants for faith-based advocacy projects, healthy lifestyle messages and talking points for communication by leaders to congregations, a faith community summit, and an organizational advocacy resource assessment. In this article, we focus on the organizational advocacy resource assessment. Six faith organizations that were represented by their leaders on the Chicago FAITH steering committee participated in the assessment.
Method
The purpose of the advocacy resource assessment strategy (ARAS) was to identify resources within faith organizations that could be mobilized for childhood obesity prevention advocacy. The specific questions guiding ARAS were the following:
Does the organization have an infrastructure that can be used to mobilize congregants for childhood obesity prevention advocacy?
Does the organization have policies in place, or could it adopt policies, that contribute to childhood obesity prevention?
Has the organization had experiences in health programming or general advocacy that can be put to use for childhood obesity prevention advocacy?
Are there key congregants or organization staff with interest and/or experience in health advocacy?
The Ann & Robert H. Lurie Children’s Hospital of Chicago Institutional Review Board approved this study. Two surveys (“key administrator” and “congregant”) were created to identify organizational infrastructure that could be used to mobilize congregants, health-promoting policies, experience in health programming or advocacy, and congregants with interest and/or experience in advocacy for childhood obesity prevention. CLOCC staff conducted the assessment. Each organization received an individualized report of its findings and recommendations for further action.
Six faith-based organizations in Chicago, Illinois, participated in the ARAS study. All organizations were part of the Chicago FAITH steering committee and of the Christian faith. The specific organizational denominations represented included one Methodist, four Baptist, and one Episcopal. Regardless of specific denomination, all of the participating organizations had leaders who were invested in community advocacy and spread that word through their ministry. Five of the congregations were primarily African American and one was predominantly Hispanic. The size of the faith organizations varied between 75 and 7000 members, with the majority of the organizations having 800 members or less. Two hundred and twenty-three congregants and six key administrators participated in the study. No incentives were provided to individual members for their participation. However, a stipend was provided to each participating organization to plan activities based on the recommendations from the assessment in order to build activities for childhood obesity prevention advocacy.
The Chicago FAITH steering committee developed two ARAS surveys. A “key administrator survey” was conducted with the faith leader of the organization or an individual identified by the faith leader as someone who was familiar with the organization’s infrastructure. The survey assessed current health promotion polices, prior advocacy experiences, and the interests and experiences of the respondent pertaining to health advocacy. Congregants of participating organizations completed a “member survey” that was available on paper or online. The paper version was available during worship times, at ministry meetings, and in the main office. The survey assessed individual advocacy skills, interest in participating in organizational activities for childhood obesity prevention, and availability for related activities. The member survey data were entered into SurveyMonkey and exported to SPSS and Excel for analysis. Due to the small sample size, descriptive statistics were calculated and reported for each organization and then compared to the other participating organizations. Data from the member surveys were combined with the key administrator survey for each organization to determine overall organizational childhood obesity prevention advocacy interest and resources.
Results
CLOCC staff administered the surveys. Six faith organizations participated, with a combined total of six administrator surveys and 223 member surveys. All participants were at least 18 years of age.
Key Administrator Survey Findings
The availability of organizational resources ranged across organizations, with some having a wide range and others having very limited resources to mobilize for childhood obesity prevention advocacy. Limited financial resources were often cited as a barrier. Organizational priorities were also identified as a factor influencing the availability of resources for obesity prevention advocacy, with some organizations focusing solely on sustaining faith activities, others focusing on social issues such as community violence and immigration, and a few focusing on childhood obesity prior to their involvement in Chicago FAITH.
Existing ministries within the organization (e.g., health ministries, youth ministries) were identified as an important resource for health promotion and advocacy, including childhood obesity prevention. Several organizations identified physical space, communication mechanisms, and relationships with the media as key assets that could be leveraged by the faith organization for childhood obesity prevention advocacy. Faith organizations also identified the various ways they already engage with children and their families. These included having a school on site, hosting a community food pantry, hosting organizational meals for their members, and holding health promotion events such as health fairs and exercise classes. Some organizations already had health promotion-related organizational policies in place, such as a healthy catering requirement or nutrition requirements for their food pantry. All six organizations identified their previous advocacy experience as a potential asset for childhood obesity prevention. Faith organizations had varying levels of experience with adopting or advancing health-related policy.
Member Survey Findings
The number of surveys completed by members at each organization ranged from 15 to 60. Fifty percent of the respondents indicated they had been involved in their congregation for at least 10 years. Every organization had some members with education and professional backgrounds relevant to health promotion. For example, 15% of respondents stated they had a background in public health or medicine, and 7% had a background in government. Respondents indicated work experience and/or education in public health, sociology, professional sports, psychology, political science, criminal justice, nursing, school administration, early childhood and K-12 education, job training, business, substance use prevention education, nonprofit management, and public relations. Several respondents indicated they were retired.
Advocacy experience among respondents ranged from working on political campaigns to advocating for other child and youth health-related issues, such as gun violence prevention, affordable housing, and school-related issues. Most (83%) respondents stated they believed childhood obesity is a public health problem in the community where their faith organization is located (organizational range: 72% to 89%). Respondents believed that childhood obesity is caused by a variety of factors, especially lack of knowledge, parenting practices, genetics, and the cost of healthy food.
Respondents’ willingness to participate in childhood obesity prevention advocacy varied (organizational range: 33% to 78%). Respondents indicated willingness to participate in advocacy in the following ways: communication, logistics, community organizing, working with youth on the issue, reaching out to policy makers, and fund-raising. Respondents also stated they were “willing to learn” and do “whatever I can do to help.” Most respondents (organizational range: 53% to 78%) were interested in learning more about childhood obesity prevention through these advocacy initiatives and agreed that training could be helpful. Training topics of interest included: basic government information, environmental change strategies, Childhood Obesity 101, how to be an effective advocate, and nutrition and physical activity fundamentals. The majority of respondents indicated willingness to meet on the topic once per month. However, there were requests to find additional ways for members who are unable to travel to meetings to engage in these efforts.
Respondents provided a variety of responses as to why they would be willing to participate in childhood obesity prevention initiatives. Some of these responses included, “Children are our future,” “The children are at great risk,” “Because I believe that this church influences the community in this area,” “We have to teach the right way so that they can teach their children,” “Church should be an extension of the neighborhood or community,” “It would help us to have a greater relationship with the community,” and “What better place than a church to be promoting health in the community.”
Recommendations Provided to Faith Organizations
Each participating organization was invited to a group meeting to discuss the findings from the ARAS. At this meeting, each organization that was present received a report that contained the results from their organizational assessment. Although the majority of the participating organizations attended the meeting, not all of the organizations were able to send a representative to this meeting. A CLOCC staff member individually communicated the results from the assessment to the organizations that could not attend the group meeting. A sample of recommendations provided to these organizations that may be helpful to other faith communities interested in pursuing childhood obesity prevention advocacy strategies may be found in Table 1.
Examples of Childhood Obesity Prevention Advocacy Strategies Recommended to Participating ARAS Faith Organizations
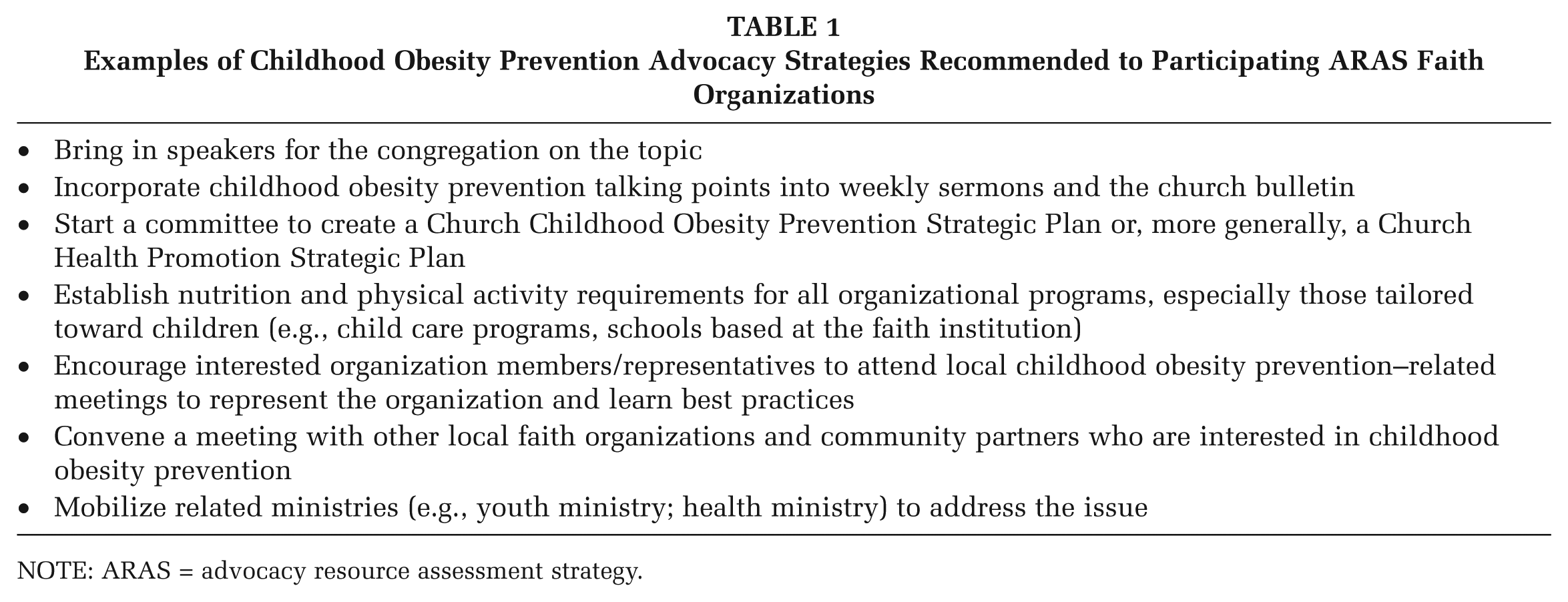
NOTE: ARAS = advocacy resource assessment strategy.
Discussion
Faith organization administrators indicated an interest in childhood obesity prevention and engaging their organization in this issue. They identified competing organizational priorities as a barrier given limited time and resources. Thus, when working with faith organizations on a health-related initiative, it is important to assess, acknowledge, and respect competing organizational priorities. Despite these competing priorities, faith organization members expressed an interest in the issue and willingness to contribute time to it within their faith organization. Members also indicated they needed more training on childhood obesity prevention in order to engage in advocacy related to this issue. However, it was evident that members already possessed many skills and areas of expertise that could be leveraged for childhood obesity prevention advocacy initiatives.
The ARAS study conducted for the Chicago FAITH initiative is significant in two ways. We are unaware of studies in the literature that assessed childhood obesity prevention advocacy capacity and interest among faith organizations. The active engagement of faith leaders in the design of the study was also unique. In addition, there were several lessons learned from this study and the overall Chicago FAITH initiative that could be applied to health promotion interventions, including policy, systems, and environmental change interventions, in partnership with faith organizations. Meaningful engagement of faith leaders can facilitate organizational participation in and response to health promotion and advocacy activities. An organizational assessment, such as ARAS, can help partners identify and match existing assets to health promotion and advocacy efforts while considering organizational constraints. An assessment can also help identify opportunities to strengthen or add to existing assets, such as training and information dissemination.
The faith leaders who participated in Chicago FAITH understood the importance of modifying their own environment prior to working outside the organization on community-level changes. For example, one coalition of ministers had been advocating for a new grocery store to come to their community for years before joining the partnership. Partnering with faith leaders will also increase health practitioners’ knowledge relative to how faith organizations function. Such knowledge is vital when developing interventions that will be relevant to faith organizations and the communities they serve.
Funding for sustaining this type of work with faith organizations is a challenge. However, engaging the faith community in childhood obesity prevention should be a priority for public health professionals and community advocates. As an incentive for their participation in ARAS, each faith organization received a stipend to act upon recommendations provided to them based on their organization’s assessment. One required activity was to convene an organizational meeting to discuss the assessment findings and potential next steps. Health promotion professionals should be prepared to partner with faith organizations over the long term to help them mobilize their existing advocacy skills and resources to address this issue and to provide them with obesity prevention-specific and health promotion best practices.
There are several limitations for this study. Findings cannot be generalized to other faith organizations. Those in this study were all Christian but of different denominations. Thus, each organization is unique and may differ in their emphases on community advocacy so this can skew results. This article reports on a study among a small group of organizations with leaders who voluntarily joined a childhood obesity prevention initiative. There was no comparison group of nonengaged leaders. Response rates varied across the organizations and were low in some. Additional strategies could have been deployed to increase response rates for the member survey, such as an incentive for survey completion. The survey was written in English only, potentially limiting the participation of congregants whose primary language was Spanish. However, despite these limitations, this study demonstrates how a health promotion–related assessment can be developed and implemented in collaboration with faith organizations.
Conclusions
Faith-based organizations are an important partner for childhood obesity prevention because of their significance in communities that experience health disparities. These organizations often provide resources to families that extend beyond their religious mission (Cnaan, Sinha, & McGrew, 2004), and they can be a center for familial and community activities. Thus, their potential impact on the overall health and well-being of families and communities is significant. Faith organizations are often deeply rooted in social justice movements with the power to use their collective voices to promote societal and community change. Given that childhood obesity is a social and environmental justice issue that is affected by resources and infrastructure that are present in some communities and not in others (Cutts, Darby, Boone, & Brewis, 2009), faith organizations are a natural sector that should be mobilized to address these inequities.
These organizations have diverse assets that can be mobilized but have other priorities that must be considered. Thus, it is important that health professionals do not expect faith organizations to prioritize obesity prevention, or other related public health issues, over the issues that are of greatest concern to them at the time. It may be possible to find the common elements of these issues to form a partnership. For example, in the participating faith organizations’ communities for this project, some of the faith leaders identified gun violence prevention as a high priority. It was possible for our partners to discuss the common concerns with gun violence and childhood obesity (e.g., fear of exposure to violence may be inhibiting outdoor physical activity for children and families in affected communities).
In addition, identifying the diverse ways in which faith organizations can be engaged can help balance competing priorities. For example, working with organizations in a community to form a coalition or steering committee, such as the one formed for the Chicago FAITH project, can assist these organizations to share resources and develop a strategic plan to (1) share best practices at the organizational level and (2) address the community health issue. An assessment such as ARAS can help organizations find strategies that draw on existing resources while diminishing the costs of engagement. It is likely that the findings from the assessment can also be applied to other locally relevant health issues in helping determine organizational resources for health promotion, as well as member interest, skills, and availability for this work.
The childhood obesity epidemic continues to be a societal and social justice issue. A social ecological and multisector approach that engages organizations that influence and have an impact on children and their families on a daily basis is critical to address this persistent public health problem. Faith organizations are a key stakeholder and partner in this work and should be approached for partnership opportunities. Recognizing and leveraging these organizations’ advocacy skills could be key to ameliorating the obesity epidemic throughout the United States, especially in underserved communities at disproportionate risk.