
Abstract
Homelessness among older individuals is increasing and women experiencing homelessness have been previously shown to have poorer health outcomes than their male counterparts. To address these concerns, the Bridges to Elders (BTE) program was developed to improve health and social outcomes for older women experiencing or at risk for homelessness. BTE consisted of a nurse practitioner (NP) and community health worker (CHW) dyad who provided intensive case management services for women 55+ with housing instability. This evaluation used a pretest/posttest design to examine three main outcomes from BTE: change in housing status, enrollment with a primary care provider (PCP), and diagnosis of uncontrolled chronic condition. The sample included 96 BTE participants enrolled from January 2017 to December 2018. The average age of participants was 66 years and had a mean BTE enrollment time of 7.6 months. Statistically significant improvements were achieved in all three outcomes measured: 17% (p < .009) increase in stable housing, 35% (p < .001) increase in PCP enrollment, and 47% (p < .001) decrease in the diagnosis of an uncontrolled chronic condition. The results indicated an NP/CHW dyad improved housing status, primary care access, and targeted health outcomes for older women who are experiencing or at risk for homelessness. Future studies examining the impact of NP/CHW dyads on additional social determinants of health and their impact on health outcomes are recommended.
Keywords
Homelessness among older adults in the United States, defined as those aged 55+, has been on the rise and in some metropolitan areas is projected to increase up to three times current numbers by 2030 (Culhane et al., 2019). This increase in the population of older homeless adults is concerning because homeless individuals in their 50s and 60s have been shown to have poor functional outcomes (e.g., cognitive impairment, urinary incontinence) when compared with a cohort of the general U.S. population in their 80s (Brown et al., 2017). Research has also revealed that older homeless individuals had mortality rates 3.5 times that of a comparable population of housed adults, and those who were experiencing homelessness for the first time after the age of 50 had an increased risk of death compared with those who were first homeless before age 50 (Brown et al., 2022).
Alarmingly, research has also demonstrated women experiencing homelessness have pronounced health disparities compared with their male counterparts. These disparities include higher rates of mortality (Aldridge et al., 2018; Brown et al., 2022), higher likelihood of chronic physical and mental health diagnoses (Winetrobe et al., 2017), and higher levels of psychological distress and victimization (de Vet et al., 2019). In addition, women were less likely to have case workers and service providers in their social networks, compared with males (Winetrobe et al., 2017) implying care coordination is lower among women experiencing homelessness.
The health disparities faced by women experiencing homelessness can be traced to the difficulties they encounter in accessing health and social services. Frequently cited barriers are difficulty navigating complicated systems due to competing needs, the disconnection between health care system and social services, including emergency overnight shelters, and reported poor and nontherapeutic relationships with health care providers (Allen & Vottero, 2020). Due to these barriers, women typically express a preference for women-specific programs that promote self-efficacy and provide a safe space free from violence and situations that may trigger memories of trauma (Magwood et al., 2019). In addition, women who are not accompanied by minor children, referred to as individual homeless, are often not considered in services designed for women experiencing homelessness, and prior research has indicated special consideration should be given to individual homeless women (McLeod & Walsh, 2014). Thus, women experiencing homelessness are an underserved and at-risk population that warrants further attention and specialized service. However, there is a gap in the literature addressing the appropriate resources and support needed for older women experiencing homelessness (Grenier et al., 2016; Sutherland et al., 2021). Previously published program evaluations examining interventions to improve health outcomes for this population are sparse. We located only one other program evaluation for older homeless women, which tested the effectiveness of a frailty intervention (Salem et al., 2017). While this intervention did not demonstrate statistically improved outcomes compared with a control group, the authors did recommend further exploration with multi-disciplinary health and social services providers to further explore how to improve services for older women experiencing homelessness.
Bridges to Elders
Bridges to Elders (BTE) was developed by Health Care Without Walls (HCWW), a nonprofit organization that provides free health and social care to women at-risk for or experiencing homelessness in Boston, MA. The services they provide include free medical and wellness care, and coordination with local resources to produce optimal health outcomes. HCWW recognized the unique vulnerabilities of the growing population of older homeless women receiving services in their walk-in clinics. To meet this need, they developed a program specifically for women aged 55 and older called BTE. The BTE program provided services out of one wellness clinic located within a day shelter in downtown Boston. The purpose of this article is to evaluate the outcomes of the BTE program to provide insight into the utility of a program aimed at improving the health of older women experiencing homelessness.
Framework for Program Evaluation
We used the Centers for Disease Control and Prevention (CDC, 1999) Framework for Program Evaluation to guide this evaluation. This framework outlines six steps in program evaluation: (1) engage stakeholders, (2) describe the program, (3) focus on evaluation design, (4) gather credible evidence, (5) justify conclusions, and (6) share lessons learned. This framework was developed to provide a standard, systematic way to evaluate public health programs. We followed the six steps in the development and writing of this program evaluation. Stakeholders, which included the NP, CHW, and the nonprofit organization’s leadership were involved in each step of the process to ensure accuracy, feasibility, and utility of the evaluation and to inform future programming efforts.
Method
Design
This evaluation study was a pretest/posttest design using a retrospective record review of all participants who enrolled in BTE from January 1, 2017 through December 31, 2018.
BTE Program Overview
The BTE program consisted of an NP and a CHW dyad who worked in tandem to address the health and social needs of women 55+ who are experiencing or at-risk for homelessness. The CHW, a lay provider familiar with the local community and resources available, provided intensive case management to address the social determinants of health (SDOH) to improve health outcomes, including assistance with finding and accessing primary care, housing, food, and transportation. The CHW ensured participants had active health insurance, assisted with scheduling the appointments, provided subway passes for transportation, and accompanied some participants to their appointment if necessary. The CHW formed relationships with local community health centers to keep open lines of communication between the participant, the primary care provider (PCP), and the BTE staff. The NP, board-certified in gerontological care, provided health education, clinical care for minor ailments and monitoring of chronic diseases, and communication with participants’ PCPs to address health concerns.
Each woman admitted to BTE services had an intake visit with the CHW and NP to assess for unmet social and medical needs, including a history and physical performed by the NP. Individualized plans were created for each of the participants and included assistance with housing applications, assistance with medical and dental insurance, including MassHealth and Medicare, and referrals to clothing and food banks.
The number of visits was individualized for each participant; some required only short-term assistance, such as help furnishing a new apartment or assistance with health insurance applications. Others required intensive management with multiple visits for assistance with housing applications or help navigating the health care system for their complex chronic conditions. The CHW determined participant eligibility and did an initial evaluation of the SDOH, including housing status, health insurance status, sources of income, and barriers to accessing primary health care. The participants were examined by the NP who took a medical history and performed a physical exam.
Participants
Program participants were recruited for enrollment at one daytime only shelter (i.e., no overnight beds) in Boston, MA by the CHW and shelter staff. Participants eligible for BTE were those who self-identified as a woman, were 55 years or older, and currently experiencing or at-risk for homelessness. Women were considered homeless if they were sleeping outside, in an emergency or transitional shelter, or staying temporarily with family or friends but not on the rental lease. At-risk for homelessness participants were identified as those who moved two or more times due to economic instability in the past year, those formerly homeless, and those paying greater than 50% of their income on rent.
Measures
Demographic information, including age, race, and ethnicity was self-reported by participants. A chart review of BTE participants revealed the four most commonly diagnosed chronic conditions among participants were diabetes, hypertension, mental health, and chronic pain. The presence of chronic conditions was determined by the medical history as reported by the participant and physical exam performed by the NP who confirmed the presence of chronic conditions. A diagnosis of diabetes was determined by an A1c greater than 6.5 or if the participant was taking oral or injectable medication for diabetes. Hypertension was diagnosed if a patient had two or more blood pressure measurements of 140/90 or higher or taking medication to lower blood pressure. Mental health diagnoses included depression, anxiety, psychotic disorders, such as schizophrenia, and a history of or active substance use disorder. Chronic pain was diagnosed as those with persistent pain lasting 3 or more months or the presence of a chronic pain disorder, such as arthritis or fibromyalgia. In addition, the total number of the four selected chronic conditions experienced by each participant was evaluated.
The program outcomes were evaluated based on program evaluation data, which were entered and tracked by the BTE NP. Three program outcomes were included in the evaluation: (1) enrollment with a PCP, (2) housing status, and (3) presence of an uncontrolled chronic condition. Each item was dichotomized as yes or no at enrollment into BTE and postenrollment evaluation was defined as when they completed the program or were enrolled for at least 6 months. Participants were considered enrolled with a PCP if they had at least one appointment in the last 12 months. Housing status was dichotomized as either stably housed or unstably housed. Unstably housed included living outside, in an emergency shelter, a transitional shelter or temporarily doubled up with friends or family. Presence of an uncontrolled condition was any chronic health condition that was not currently meeting criteria based on established medical guidelines as determined by the BTE NP. Examples of uncontrolled chronic conditions included but were not limited to the four chronic conditions used in the sample description analysis. Other examples of chronic conditions included in this outcome were asthma, chronic obstructive pulmonary disease, and dermatologic conditions like eczema.
Data Analysis
Descriptive statistics were used to describe self-reported demographic characteristics and the selected chronic conditions experienced by the BTE participants as recorded in the medical record. The number of participants diagnosed with each of the four selected chronic conditions and the frequency of the four chronic conditions each participant was diagnosed with were also analyzed with descriptive statistics by number (n) and percentage (%). McNemar’s test for paired dichotomous data was used to assess participant’s prechange and postchange (Smith & Ruxton, 2020). Statistical significance was set with p < .05 (Fagerland et al., 2013). This study was approved by the Institutional Review Board.
Results
Participant Characteristics
The total number of participants included in this study was N = 96. The mean age was 66.2 years (standard deviation [SD] = 7), with a range of 55 to 92 years (Table 1). Forty participants (44%) were non-Hispanic White, n = 18 (19%) non-Hispanic Black, and n = 25 (26%) Latina. Participants had a mean program enrollment time of 7.6 months (SD = 6.6). At enrollment, n = 55 (57%) had a mental health condition, n = 51 (53%) had hypertension, n = 45 (n = 47%) had chronic pain, and n = 23 (24%) had diabetes (Table 1). At least one of these four conditions was experienced by 90 participants in the sample (94%), only six (6%) of the women did not have any of these four chronic conditions. Thirty-one participants (33%) had one of the chronic conditions, n = 36 (38%) had two of the chronic conditions, n = 18 (19%) had three of the chronic conditions, and n = 4 (4%) had all four of the selected chronic conditions (Table 2).
Population Sample
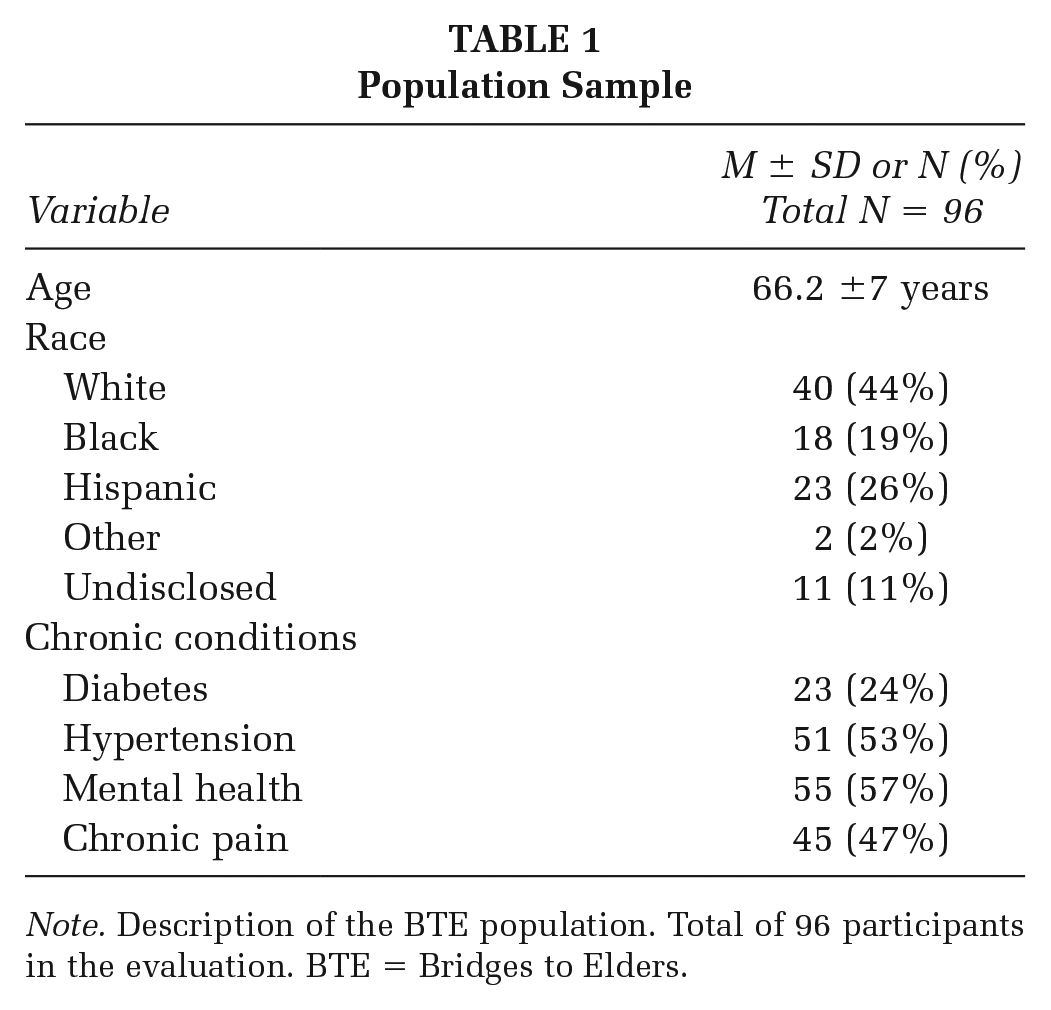
Note. Description of the BTE population. Total of 96 participants in the evaluation. BTE = Bridges to Elders.
Number of Chronic Conditions
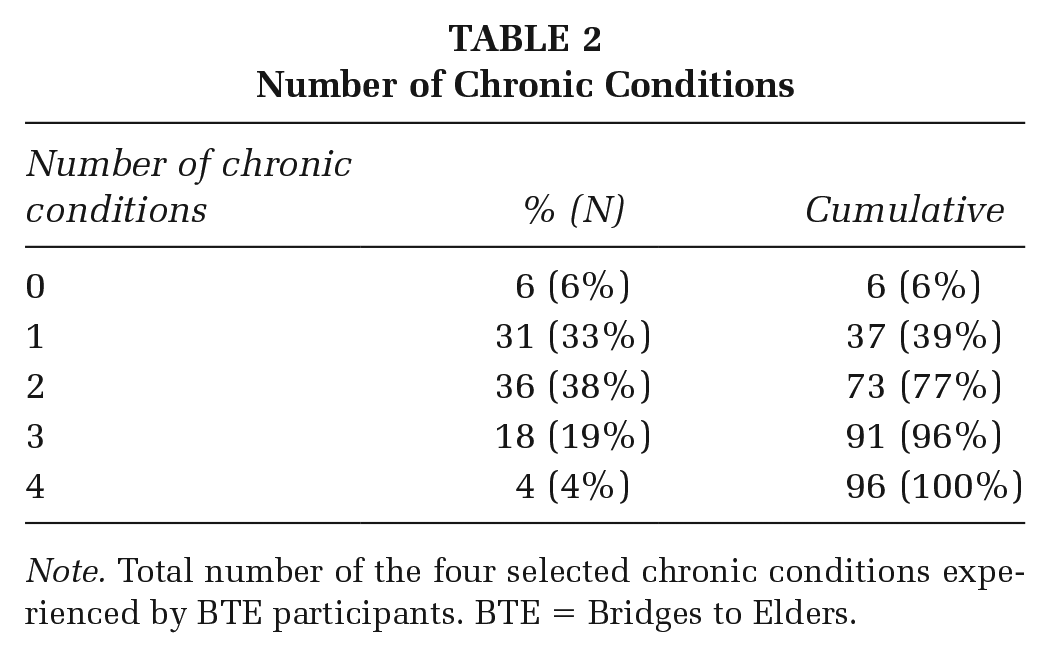
Note. Total number of the four selected chronic conditions experienced by BTE participants. BTE = Bridges to Elders.
Program Outcomes
The analysis revealed statistically significant improvement in all three outcomes examined: (1) enrollment with a PCP, (2) housing status, and (3) presence of an uncontrolled chronic disease (Table 3). Among 73 participants who had information on current enrollment with a PCP available, 49 (63.6%) participants reported having a PCP at the time of BTE enrollment, and the proportion increased to 98.6% (n = 72) at the end of program or post 6 months of enrollment, corresponding to a 35% increase (p < .001). Among 65 participants with housing status information, n = 31 (47.6%) reported stable housing at enrollment and the proportion was increased by 17% to n = 42 (64.6%) postenrollment (p = .009). Among the 66 participants with data available on uncontrolled chronic conditions, the presence of an uncontrolled chronic condition decreased from 65.2% (n = 43) at enrollment in BTE by 47% to 18.2% (n = 12) postenrollment (p < .001).
Program Outcomes
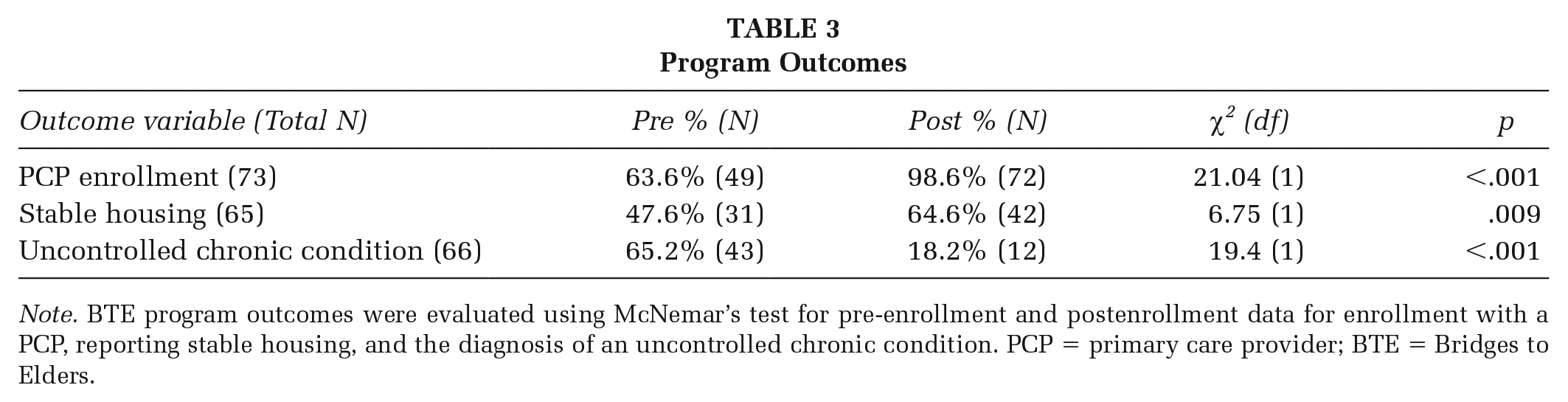
Note. BTE program outcomes were evaluated using McNemar’s test for pre-enrollment and postenrollment data for enrollment with a PCP, reporting stable housing, and the diagnosis of an uncontrolled chronic condition. PCP = primary care provider; BTE = Bridges to Elders.
Discussion
The program evaluation of BTE showed promising results and indicated that NP and CHW dyads are effective in addressing the SDOH outcomes of older women experiencing homelessness. Our findings align with previous research that has demonstrated NP and CHW dyads improved disease self-management in chronic obstructive pulmonary disorder (COPD; Kearney et al., 2022) and cardiovascular outcomes, such as improved hemoglobin A1c and reductions in blood pressure, through intensive medication management, patient education, and addressing barriers to treatment adherence (Allen et al., 2011). All three outcomes examined showed significant improvement after program enrollment. A 35% increase in the number of women with a PCP was found, only one person did not have a PCP in the postprogram evaluation. This result may be attributed to the holistic approach the CHW took toward connecting BTE participants with primary care. By addressing barriers and providing emotional support to BTE participants, all participants who wanted a PCP were able to see a provider.
The improvement in access to primary care may have also contributed to the decrease in uncontrolled chronic conditions because they had access to a health care provider to manage their medications. In addition, education and support regarding management of medications and symptoms provided by the NP likely contributed to the reduction in participants with uncontrolled health conditions. People experiencing homelessness have been found to have a poor ability to take control of their chronic health conditions when they must focus their attentions on housing and food (Shoemaker et al., 2020) and they also have difficulty navigating complicated health care systems due to poor SDOH (Stafford & Wood, 2017). The BTE program provided a potential solution to these problems using an NP and a CHW dyad to address the social determinants and help older homeless women navigate the complex and often divergent systems of health and social care.
There was also a 17% increase in stable housing among BTE participants, 11 participants were housed during their time in the BTE program. These results are particularly meaningful because the waitlist for federally supported Section 8 housing, the most stable form of housing, is very long in Boston. As of the writing of this article, applicants from 13 years prior are being selected for housing vouchers (Metro Housing Boston, n.d.). In addition, the Boston Housing Authority has indicated they receive 10,000 applications each year and have a current backlog of 40,000 applications (Boston Housing Authority, 2021). Although Boston housing programs prioritize those over 62 years of age and people experiencing homelessness, navigating the complex systems, and staying up to date with various waitlists can be overwhelming, particularly for those with chronic conditions and mental health disorders. The individualized approach taken by the BTE team helped participants remain on target with their goals and succeed in obtaining stable housing.
The participants in BTE had high rates of chronic conditions. In all, 94% of the participants had at least one of the four selected chronic diseases, with 61% having two or more. Previous studies have noted that people experiencing homelessness have rates of diabetes and hypertension similar to the general population; however, their conditions are less likely to be controlled than the general population (Asgary et al., 2016; Axon et al., 2016). In addition, the rates of mental health diagnoses and chronic pain among the BTE participants were similar to previous research (Clark & Ailshire, 2018; Landefeld et al., 2017). These results indicated that the participants in BTE had complicated health histories, and the intensive case management provided by the CHW and NP dyad was necessary to help navigate the complicated intersection of health and social needs to improve their overall health and well-being.
The data used in this evaluation were collected between January 2017 and December 2018, and between 5- and 6-year old at the time of publication. However, the findings from this study are still relevant as 64% of single older women in the state of Massachusetts, where BTE is located, had economic instability, which is a primary driver for homelessness (Mutchler et al., 2021). Massachusetts had the highest percent of older women experiencing economic instability in the United States, and an examination of the intersection between race and gender demonstrated that older Hispanic, Black, and Asian women experienced higher rates of economic instability than their White counterparts (Mutchler et al., 2021). In addition, homelessness among single females has increased 6% between 2020 and 2022, compared with 1% among men (De Sousa et al., 2023), indicating that the COVID-19 pandemic has had a greater impact on housing stability for women. The pervasive economic concerns in the United States and their greater impact on older women, particularly women of racial minorities, underscore the importance of developing programming like BTE to address their needs.
Limitations
There are several limitations to this study. First, this study was a retrospective database review and information was limited. In addition, there was no control group for comparison and some of the results may be attributed to other outside services BTE participants were accessing. The total sample size is relatively small, and participants were recruited from one location for participation in the program. Therefore, demographic descriptions may not be generalizable to other locations or populations. However, the rates of chronic diseases were similar to other studies conducted among people experiencing homelessness. In addition, 32% of participants were lost to follow up and program outcomes were not available among these participants. High rates of attrition among homeless participants have been previously noted in other studies (Western et al., 2016), which can be due to the transient nature of the homeless population and competing needs. However, the success of the participants who remained in the BTE program shows that CHW and NP dyads are effective for older women experiencing homelessness.
Implications For Practice, Policy, And Research
The results of this study showed that a community-based NP and CHW dyad can be effective in improving housing status, access to primary health care, and chronic health outcomes among older women experiencing homelessness in Boston. Patient-centered interventions designed to meet individual needs is essential in improving health outcomes and health equity and addressing poor SDOH is essential for health promotion among populations who have been marginalized by health and social systems. Future programming should be considered to expand the BTE model to more individuals experiencing homelessness in an urban environment. In addition, future research should be aimed at designing, implementing, and evaluating programs that address additional social needs and their relationship to health and social outcomes among populations experiencing homelessness. Finally, policies aimed at additional funding toward addressing SDOH and comprehensive case management using NP and CHW dyads are also recommended. The growing numbers of older women experiencing homelessness are concerning, and specialized programming to meet their unique needs will be required to improve their health and social needs. Women experiencing homelessness have also reported disproportionate rates of gender based violence and higher rates of chronic health conditions, which are compounded by systemic wealth inequities stemming from the gender pay gap (where women earn 82% of what a man earns) and the rising cost of living (Turk, 2022). Evidence-based solutions to improve the lives of older women experiencing homeless are imperative. The promising results of this evaluation show that NP/CHW dyads may be part of the solution to the homeless public health crisis.
Footnotes
Authors’ Note:
The authors acknowledge Health Care Without Walls, Adelina Vega, and Linda Cundiff for their invaluable contributions to the development and facilitation of the Bridges to Elders program. Writing of this manuscript was supported by the Department of Veterans Affairs Office of Academic Affiliations Advanced Fellowship Program in Health Services Research, the Center for Healthcare Organization and Implementation Research (CHOIR), Bedford VA Healthcare System.