
Abstract
Civic health equity is the principle that all people deserve a fair and just opportunity to participate in their communities and to have a voice in the systems that shape their lives. Yet despite its importance to population health, civic engagement remains inconsistently addressed in health professions education. Inequities in civic participation contribute to unequal political representation and policy responsiveness, disproportionately affecting historically marginalized communities, and limit the ability of future health professionals to engage with the structural and policy drivers of health. This paper describes the development and implementation of a civic health equity metric within the Planetary Health Report Card (PHRC), an international, student-led, faculty-supported initiative that evaluates how health professional schools integrate planetary health and social accountability into educational practice. First introduced in the 2026 PHRC assessment cycle, the metric was developed through iterative leadership discussions informed by existing frameworks. It assesses whether health professional curricula prepare students to understand civic participation and advocacy as mechanisms for addressing environmental and structural determinants of health. The metric is part of the PHRC curriculum domain and uses a standardized scoring system ranging from 0 to 3 points, with required qualitative justification from participating institutions. To promote feasibility and broad adoption, it is explicitly nonpartisan and educational in nature, aligning with 501(c)(3) requirements. By embedding civic health equity within an established assessment framework, this metric provides educators with a practical tool to identify curricular gaps, support equitable access to civic learning, and strengthen health promotion–oriented training.
Keywords
Introduction
Civic health equity is the principle that all people deserve a fair and just opportunity to participate in their communities and to have a voice in the systems that shape their lives (Wright, 2026). Yet despite its importance to population health, public health is increasingly threatened by the erosion of civic engagement. The health interests of historically marginalized communities are often sidelined as these groups face persistent barriers to participation in democratic processes. Sociodemographic factors such as age, education, race, ethnicity, and socioeconomic status are closely tied to both civic participation and health outcomes. Studies have demonstrated that communities with lower participation in local elections experience worse health outcomes, with particularly low voting rates observed among Latinx populations (26.8%; Kansas Health Foundation, 2016). Because elected officials are most responsive to those who engage in civic processes, inequities in participation translate directly into inequities in political representation and policy responsiveness (Adams, 2025).
Many of the same forces that shape health – commonly described as the social determinants of health (SDOH) – also contribute to civic disengagement. The World Health Organization defines SDOH as the conditions in which people are born, grow, live, work, and age, as well as their access to power, money, and resources (Braveman et al., 2011). These factors have a significant impact on health inequities and are also found to be connected to political participation (Rodriguez, 2018). Individuals with lower socioeconomic status have been shown to experience worse health outcomes and shorter life expectancy, which in turn reduces participation in voting (Rodriguez, 2018).
This dynamic is also shaped by the political settings in which one lives. Decisions that weaken health care systems or social protections can adversely affect health outcomes and contribute to further civic disengagement, reinforcing cycles of structural disadvantage (Woolhandler et al., 2021). Although this relationship and its significance have been well-established, civic health remains inconsistently addressed within public health training and health professions education. Pertinent literature has called for more intentional instructional and assessment approaches, along with innovative educational frameworks that account for the experiences and needs of marginalized and underserved populations (Doobay-Persaud et al., 2019). Addressing civic health equity within health professions education is therefore a public health necessity.
Why Health Professional Students and Institutions Matter
Health professionals occupy a uniquely trusted role in society. Across global contexts, the public consistently identifies health care workers as reliable sources of information not only about individual health but also about broader societal actions needed to promote public health, including responses to climate change and other systemic threats (Campbell et al., 2025). This trust carries with it a responsibility for health professionals to be informed and engaged citizens and, when appropriate, to help patients and communities understand how policies may influence their health.
Civic engagement and health equity have been shown to exist in a mutually reinforcing relationship: Greater levels of civic participation support the development of policies that promote health equity, while improved health equity enables broader civic participation (Habib et al., 2023). Health care professionals are therefore uniquely positioned to promote health by engaging in civic processes and advocacy. However, the extent to which future health professionals are prepared to fulfill this role depends on the training, institutional culture, and structural support they receive during their education. Without explicit guidance and support, civic engagement may be perceived as an optional, extracurricular, or politically sensitive matter rather than being considered as a core component of professional responsibility (Barrere-Cain et al., 2022).
Development of the Civic Health Equity Metric
The Planetary Health Report Card (PHRC) is a student-led, faculty-supported international initiative that evaluates how health professional schools integrate planetary health into education, research, community engagement, and institutional practices (Planetary Health Report Card, 2026; see Supplemental File). Implemented annually across medical and other health professional schools worldwide, the PHRC publicly reports institutional results to promote transparency, accountability, and continuous improvement. By providing a standardized, comparative framework, the PHRC aims to support institutions in identifying strengths and recognizing gaps while advancing planetary health and sustainability initiatives within health professionals education.
The civic health equity metric was first introduced in the 2026 PHRC assessment cycle, reflecting growing recognition of civic engagement as an important upstream determinant of health. Prior to 2026, the PHRC framework did not formally assess civic health equity, though related themes of community engagement and advocacy appeared within other domains. The decision to develop a dedicated metric arose from leadership discussions that emphasized that while clinical care contributes to health outcomes, it represents only a portion of what shapes population health. The majority of health is determined by social and environmental conditions, including housing, transportation, labor protections, food systems, and environmental quality, all of which are strongly influenced by public policy (Braveman et al., 2011; Rodriguez, 2018).
These ideas were central to the metric’s development. Student leaders and faculty advisors examined whether and how civic engagement could be appropriately incorporated into an institutional assessment framework. Civic engagement was framed as both directly health-promoting – through empowerment, agency, and social connection – and indirectly impactful by enabling policies that improve social and environmental conditions (Habib et al., 2023). Participants emphasized that civic engagement takes many forms, including volunteering, organizational involvement, advocacy, public comment, and electoral participation.
Leadership conversations also highlighted the role of health professionals as trusted voices in civic spaces. Advocacy activities such as submitting public comments, writing op-eds, meeting with legislators, and educating patients about policy impacts were described as increasingly recognized ethical responsibilities within the health professions (Adams, 2025; Barrere-Cain et al., 2022).
In addition, the civic health equity metric was informed by existing educational efforts, including the Climate Resources for Health Education (CRHE) modules developed by Columbia University. While CRHE offers curricular resources linking climate, policy, and health, the PHRC adapted these concepts into an institutional self-assessment framework with reflection, capacity-building, and accountability at its core.
Metric Structure and Implementation
The PHRC comprises five domains: Planetary Health Curriculum, Interdisciplinary Research, Community Outreach and Advocacy, Support for Student-Led Planetary Health Initiatives, and Campus Sustainability. The civic health equity metric is housed within the Curriculum domain. As with other curriculum metrics, it is scored from 0 to 3 points (Figure 1).
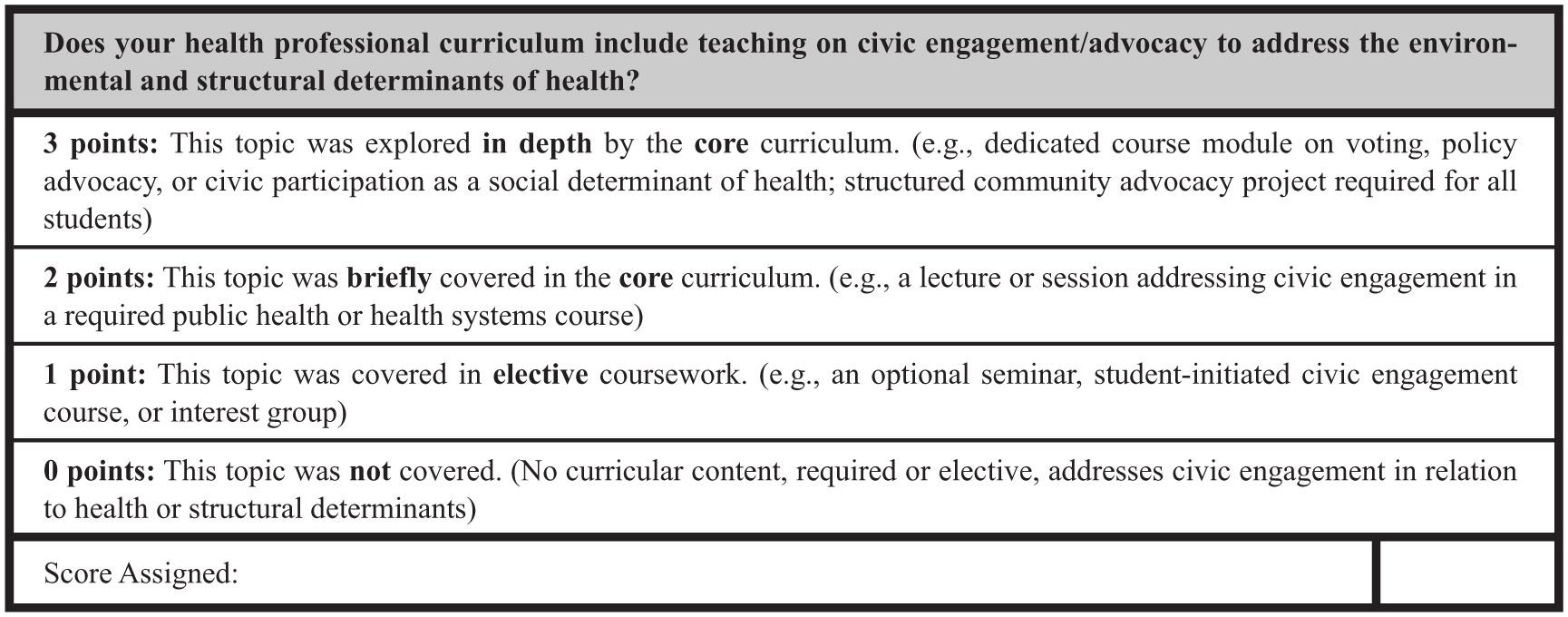
Scoring criteria for the PHRC’s civic health equity metric as provided to participating schools.
Schools are required to provide a qualitative explanation for their score, including examples of how curricular content meets the scoring criteria. These explanations are reviewed by members of the PHRC global organization prior to publication, supporting transparency and consistency in scoring across institutions.
Importantly, this metric explicitly situates civic engagement within the context of environmental and structural determinants of health, rather than addressing civic participation or public health in isolation. To receive credit, curricula must meaningfully engage students in examining how civic responsibility intersects with health equity and policy.
Applicability Across Health Disciplines
Civic engagement education is relevant across all health professions. Medical students may learn how to submit public comments on zoning, transportation, or air quality regulations. Nursing students may document housing conditions such as mold or poor ventilation during home assessments, contributing data to advocacy efforts for stronger housing codes. Pharmacy students may advocate for medication access during extreme weather events. Physical and occupational therapy students may engage with inclusive disaster-preparedness planning. Health care management students may learn how to interface with governmental bodies on health care system sustainability.
Health care professionals have long played important roles as civic advocates at local, national, and global levels. The PHRC aims to capture and assess this dimension of professional responsibility as it relates specifically to environmental and public health.
Political, Legal, and Institutional Considerations
The civic health equity metric was developed with careful attention to political, legal, and institutional contexts. In alignment with 501(c)(3) requirements, the metric is explicitly nonpartisan and educational in nature, focusing on civic participation skills such as voter education, access, and engagement rather than political ideology, candidates, or parties. This distinction was central to addressing stakeholder concerns regarding political sensitivity and institutional risk.
Recognizing that institutions operate within diverse regulatory and political environments, the metric emphasizes clarity of intent, defined guardrails, and transparency in scoring and implementation. Scoring criteria focus on whether civic engagement content is incorporated into the curriculum and at what depth, without prescribing the political content or viewpoint of that instruction. Structured feedback from participating institutions is solicited following each assessment cycle, allowing for incremental refinement of the metric while maintaining longitudinal comparability.
Implications for Practice
Integrating a civic health equity metric within the PHRC positions civic engagement as a foundational determinant of health rather than a peripheral or extracurricular activity. For educators, the metric provides a practical framework for identifying curricular gaps related to governance literacy, policy engagement, and democratic participation as determinants of population health. It supports the intentional integration of civic health concepts into existing coursework, including public health, ethics, health systems, and planetary health curricula.
For institutions, the metric offers a mechanism for accountability, strategic planning, and sustained investment in civic health education. Repeated application across reporting cycles enables institutions to move beyond ad hoc or symbolic commitments toward more formalized and sustainable approaches aligned with social accountability mandates. By providing a standardized assessment framework, the metric can also help institutional leaders justify resource allocation, faculty development, and protected time for civic engagement activities.
For students, the metric legitimizes civic participation as a core professional competency and reduces reliance on informal or self-directed opportunities that disproportionately advantage those with greater time, financial resources, or social capital. In doing so, it promotes more equitable access to civic learning experiences across health professions education.
Implications for Research
The inclusion of a civic health equity metric within the PHRC creates multiple opportunities for future research. As a newly introduced metric first implemented in the 2026 assessment cycle, longitudinal data on institutional trends are not yet available, and the metric’s predictive validity with respect to graduate outcomes has not been established. Longitudinal analyses of collected data will be important for examining changes in civic health education over time, both within individual institutions and across regions. Cross-sectional studies may explore associations between civic engagement education, institutional characteristics, and surrounding community contexts.
Given the PHRC’s international scope, comparative analyses across countries and regions may identify shared practices and contextual differences in how civic engagement is taught across health professions. It is worth noting that the frameworks and examples underlying this metric’s development reflect primarily North American and European educational traditions; future iterations should continue to solicit feedback from institutions in low- and middle-income countries to ensure relevance across global contexts. Qualitative analyses of institutional score explanations may further elucidate pedagogical approaches, barriers to implementation, and facilitators of effective civic health education.
Because PHRC participation is voluntary, institutions that engage may differ systematically from those that do not, which should be considered when interpreting aggregate findings. In addition, the binary framing of “core” versus “elective” curriculum, while useful for standardized comparison, may not fully capture the variety and depth of civic health education occurring within an institution – a nuance worth exploring in future qualitative work. Future research may also investigate downstream outcomes, including the influence of civic engagement training on graduate advocacy behaviors, professional identity formation, and engagement with policy processes. Together, these research directions can help refine educational approaches and strengthen the evidence base for civic health equity as a core component of health professional training.
Supplemental Material
sj-pdf-1-hpp-10.1177_15248399261460394 – Supplemental material for Assessing Civic Health Equity in Health Professions Education: Development of a Novel Metric Within the Planetary Health Report Card
Supplemental material, sj-pdf-1-hpp-10.1177_15248399261460394 for Assessing Civic Health Equity in Health Professions Education: Development of a Novel Metric Within the Planetary Health Report Card by Emma Willcocks, Aaron Avenido, Aghna Wasim, Fiona Conway, Jessica Mo, Roma A. Kankaria and Sümeyye Eylül Yılmaz in Health Promotion Practice
Footnotes
Acknowledgements
The authors are grateful to the Planetary Health Report Card leadership team and board of directors, as this work would not be possible without their support. The authors also thank all the health professional school students and mentors who have participated in PHRC for the time and effort they put toward their passion for planetary health education.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.