
Abstract
Alignment refers to the interactive use of similar words to accomplish a linguistic and cognitive “common ground” in conversations. Alignment is thought to be unconscious, relying on priming mechanisms. This occurs uniquely in conversational contexts and has been shown in choices of words, grammatical constructions, and even indirect language and gestures. This study reports a couple who demonstrated very little pretherapy alignment, using a couples-based approach. The client realized an increase in utterances and words, and no change in incoherent utterances. Her nonaphasic spouse increased his use of alignment. Naïve observers of therapy sessions perceived later sessions as more positive than earlier sessions.
Aphasia Couples Therapy (ACT)
ACT (Boles, 2009) has at least a 20-year history under a variety of names, with Simmons-Mackie, Kearns, and Potechin (1987) introducing us to family member training, and Holland (1991) describing “Conversational Coaching.” Therapy of this type, termed aphasia couples therapy or ACT here, brings the individual with aphasia closer to the person (or at least a key person) with whom he or she communicates most often. ACT involves a negotiation of goals and outcome measures between the patient, the significant other, and the therapist. This section of the current article will review ACT as it pertains to therapy involving the person with aphasia interacting with a communication partner. Following this section, a comparison with other methods somewhat similar to ACT is made, followed by a description of a study involving alignment during ACT.
The current author used a form of ACT in several studies (Boles, 1997, 2000; Boles & Lewis, 2003). The four participants in Boles (1997) were consecutive cases enrolled in a university clinic. Three of the participants had moderate aphasia, whereas one presented with mild aphasia. One participant had Broca’s aphasia, one had transcortical sensory, and two presented with anomic aphasia. Communication partners comprised a sister-in-law, a committed partner, an adult daughter, and a husband. The nonaphasic partner was trained to become the “therapist,” with the speech-language pathologist (SLP) assuming the role of “coach,” encouraging the use of facilitative acts by both parties, while discouraging nonfacilitative acts. An ABA design was used, where the first A comprised data prior to treatment, B referred to the treatment phase, and the second A referred to data collected after termination of treatment. Each partner (aphasic and nonaphasic) had goals that were negotiated with the “coach” before therapy began. For example, in several cases, the nonaphasic partner’s goal was to decrease his or her relative frequency of talking and offer more open-ended questions during conversation. Those with aphasia were often encouraged (by their partners) to use more gestures, drawing, and circumlocution. Results generally were positive, with increased production (measured in words per minute, and relative contribution to the conversation measured in utterances) and efficiency (measured in changes in conversation repair). Positive changes were also noted in psychosocial well-being, which was measured by questionnaire in a Likert-type format, such that higher scores corresponded to self-evaluations of higher well-being.
Wilkinson et al. (1998) used conversation analysis in describing couples-based therapy. The couple had already been enrolled in a project focused on community-based aphasia therapy but was in a lull in that project at the time of this study. Although quantitative data were not provided, descriptions in the conversation analysis revealed that the nonaphasic husband, in postintervention conversations, decreased his error correction during times when he had already discerned the intent of the message from his wife. This allowed the couple to converse on a wider range of topics rather than focusing on the conversation repairs themselves. The therapy used by Wilkinson et al. was similar to ACT; however, the goals were determined by the speech pathologist in the study, and the outcome was described in great detail but was not subjected to quantitative analysis.
Oelschlaeger and Damico (2000) used conversation analysis to describe word search strategies in detail between a man with moderately severe Broca’s aphasia and his wife. Particular strategies used by both partners were demonstrated and described. This study was not intended as a pre–post comparison. However, these authors provide a compelling argument for the inclusion of communication partners in aphasia therapy, rather than relying on the generalization of strategies between therapist and patient to partner and patient. Similar to the study by Wilkinson and colleagues, this study was descriptive in nature, and data analysis was not attempted.
In a study similar to Boles (1997), Boles (2000) used the same therapy protocol with a man and his wife during 8 weeks of therapy. Recruitment was again a matter of convenience, as they had enrolled in a university clinic and agreed to participate. A key difference here was the language used. This couple requested therapy in English, but during conversations in their home, the couple chose their first language, Ilicano. Data were obtained only during sessions in English. Improvements were documented in the individual with aphasia for total utterances and questions asked in 10-min samples, along with decreases in incoherent utterances, and conversation repairs. Improvements were also noted in scores on the Functional Assessment of Communication Skills for Adults (FACS; Frattali, Thompson, Holland, Wohl, & Ferketic, 1995).
Other approaches have reported evidence of success in using conversational partners, including Kagan, Black, Duchan, Simmons-Mackie, and Square (2001). Their “Supported Conversation for Adults With Aphasia” (SCAA) resulted in significant improvement in conversational partners’ acknowledging and revealing the conversational competence of the person with aphasia. This group study used two standard measures for improvement—one measuring conversational skills and the other measuring participation in conversations. Although SCAA was a pioneering study in providing evidence for the use of conversation partners in aphasia therapy, it differs from ACT in two respects. First, SCAA was designed to train volunteers, as opposed to significant others, and second, the dependent measures were determined by the researchers, whereas the goals in ACT are negotiated between the therapist, the person with aphasia, and the significant other. Howe et al. (2012), Sherratt et al. (2011), and Worrall et al. (2011) made a strong case for considering the goals of family members and significant others when making decisions regarding therapy goals.
Hopper, Holland, and Rewega (2002) “coached” two couples to use facilitative strategies (which were negotiated with the couples prior to the onset of therapy), who were attempting to discuss videotaped material viewed by the person with aphasia with each other. The strategies were carefully selected, based on the ability to use them successfully, the desire by the person to use them, and the degree to which they were facilitative. These strategies included, for example, the use of gesture and drawing. The “coaching” by the investigators involved intervening during communication breakdowns and encouraging the use of one of the previously selected strategies. A multiple baseline across subjects design determined successful conveyance of co-constructed main concepts from the video clips, with both couples making modest but positive gains. In addition, naïve raters judged the posttreatment interactions to be superior to the pretreatment conversations. This study differed from ACT in that couples being coached were responding to videotaped stories of real-life events. In ACT, the couples are encouraged to have a conversation about anything they wish. In the work of Hopper et al., the number of main concepts present in the videos was used as a dependent variable. This is not the case in ACT.
Boles and Lewis (2003) used very similar methods to Boles (1997, 2000) with a man with moderate Broca’s aphasia. In this case, however, scaled questions were used to document change. For example, when the nonaphasic wife expressed difficulty with discussing “deeper” (i.e., nonsuperficial) issues in their conversations, she and her husband were asked to rate the ease of doing so, on a scale of 1 to 10. Positive changes were realized in nearly all these scaled questions, along with positive changes in the FACS (Frattali et al., 1995) and in the use of facilitative gestures.
Cunningham and Ward (2003) enrolled four couples in a 5-week training program, comprising education, video feedback, and role-playing. The individuals with aphasia were severely impaired, with both receptive and expressive difficulties in each case. Successful conversation repair improved in three of the four couples, increases in the number of repairs initiated by the aphasic individuals occurred in three of the four; and increases in the use of gestures occurred for three of the four dyads. It should be noted that these results were not statistically significant. Unlike ACT, the nonaphasic communication partners had no prior relationship to the person with aphasia. In addition, the therapy involved educational sessions, video observation by the participants, and role-playing. This contrasts with ACT sessions, which use feedback by the therapist during real-time conversational interaction.
Fox, Armstrong, and Boles (2009) modeled their study on that of Boles and Lewis (2003). A woman with mild aphasia and her husband participated in 14 sessions of conversation-based therapy. Like the previously cited work by Boles, the couple addressed each other during therapy sessions, with the therapist in the role of “coach,” giving suggestions and reinforcement in that role when deemed appropriate. The woman with aphasia reported slight to moderate movement in the positive direction for all scaled satisfaction measures taken except one (“How easy is it to talk to other people,” which remained at baseline level). Furthermore, improvements by the spouse in acknowledging and revealing his wife’s communicative competence (Kagan et al., 2001) were shown. Less compelling results occurred in each of the two participants’ individual goals. For example, goals for the woman with aphasia included an increase in topic initiations (a mean of 1.75 pretreatment and 2.0 post treatment), and turns interrupted by the nonaphasic husband (17.5% pretreatment and 19% post treatment). The authors acknowledged that in this case, the milder aphasia may have accounted for the more modest gains.
Alignment
Alignment refers to the interactive use of similar words to accomplish a linguistic and cognitive “common ground” in conversations (Brennan & Hanna, 2009; Garrod & Pickering, 2004; Shintel & Keysar, 2009). For example, if Speaker A says, “We saw the 8 o’clock show at the Tower,” Speaker B will more likely say, “oh what was the 8 o’clock?” versus simply “oh, tell me about it.” Alignment is thought to be unconscious, relying on priming mechanisms (Garrod & Pickering, 2004, 2009). This occurs uniquely in conversational contexts and has been shown in choices of words, grammatical constructions (Garrod & Pickering, 2009), indirect language (Roche, Dale, & Caucci, 2012), and gestures (Shockley, Richardson, & Dale, 2009).
A term used synonymously with alignment is entrainment, which is the influence one person has on another, in choice of words, posture, syntax, facial expression, and prosodic features (Iwata & Watanabe, 2013). Clayton (2012) offered a more general definition: “the process by which independent rhythmical systems interact with each other” (p. 49). Iwata and Watanabe argued that each participant in conversation brings a rhythmical system to the interaction.
Although entrainment often describes influences other than linguistic ones, Fridriksson et al. (2012) used entrainment in helping 13 patients with Broca’s aphasia improve their ability to speak. Patients were required to mimic a speaker in real time in three conditions: live, with audiovisual support, and audio-only support. This initial experiment was intended to find the condition under which patients might be most productive (measured in number of words and number of unique words). Speakers showed a preference for the audiovisual condition, producing twice as many words and a wider variety of words, compared with either the audio-only or live conditions. In a follow-up experiment in this study, the audiovisual condition was used with all 13 participants, with significant improvement in number of words used after 6 weeks of script training and 6 weeks after training. Entrainment, as used by Fridriksson et al., is similar to alignment in that both encourage the reiteration of what another speaker has said.
Although empirical evidence has not attempted to distinguish alignment from entrainment, alignment is described in the context of conversation, whereas entrainment has been used in other contexts, such as written discourse and music (Jucks, Becker, & Bromme, 2008), as well as the scripts noted above. The term alignment will be used in this article for describing the conversations between a woman with aphasia and her husband.
Rationale for the Use of Alignment
Wernicke’s aphasia is characterized by fluent output with speaking “errors” and misspoken utterances, and impaired auditory comprehension. Ms. E (pseudonym), a person with Wernicke’s aphasia, was one of the two participants in this study. Several features of Ms. E’s communicative profile led to a particular set of recommendations in therapy. These features included the observation that Ms. E was not oblivious to her speaking errors but had little ability to self-correct them, often saying, “never mind,” or “oh I don’t know” after such errors. Other times, her utterances could be partially interpreted and/or incomplete. For example, here is an excerpt from a conversation prior to the initiation of therapy. The couple is talking about one of their adult granddaughters. Mr. E had been trying to help this granddaughter find employment.
I also found a couple of ads on the computer that she could handle. A receptionist, medical receptionist. All you have to be is polite and answer the phone, and she can do that. And that isn’t what she’s trained for but so what? If she needs a job and if the job will help her stay here then she should look into it.
Yeah, that’s for sure. And he [meaning “she”] should look into their you know right there in the . . .
in Montana?
No. In the column that just right there that just right there to see if anything was there.
Well that’s a thought [apparently not understanding, but not confronting her with the vagueness either].
Thus, Ms. E participated in the conversation, and although testing classified her as a person with Wernicke’s aphasia, her contributions were pertinent to the conversation, if imprecise and requiring a good deal of inference from Mr. E. For his part, Mr. E appeared to either correctly interpret his wife’s contributions or ignore the lack of clarity; rarely did he overtly acknowledge the accuracy or lack thereof.
When the couple conversed, Mr. E dominated the conversation, apparently trying to fill the silence with his own contributions rather than giving Ms. E more time to respond or contribute. When Ms. E used a phrase or word that was unclear or even incoherent, Mr. E tended to proceed with the conversation as if she had not said anything, and/or without an attempt to repair the conversation, thus, without alignment.
The most poignant request by both members of the couple was for the habit of dialogue to be reestablished. Their habit, 2 years after the stroke, was for monologues to occur, with Mr. E dominating, followed by occasional interjections by Ms. E. They both agreed that a more balanced conversation was a top priority. It was hypothesized that increased reflection on the part of Mr. E (i.e., alignment) would help them accomplish their goal.
Other researchers have used strategies during conversational interaction. For example, Beckley et al. (2013) used nonverbal turn signaling, integration of writing and drawing, and the use of keywords as cues in working with couples in conversation-based therapy. Beeke, Maxim, Best, and Cooper (2011) targeted utterance construction (specifically, number of utterance turns, number of nonagrammatic turns, incomplete agrammatic turns, etc.) during conversations between couples. Positive results were reported for both quantitative and qualitative measures. However, the participants in these studies had relative strengths in auditory comprehension, with nonfluent, agrammatic aphasia.
In a descriptive study, Simmons-Mackie, Kingston, and Schultz (2004) used the term speaking for when a nonaphasic conversation partner interpreted the utterances of the person with aphasia. The success of the “speaking for” framework depended on several conditions. First, the nonaphasic partner had to be willing to speak for the aphasic partner; second, a willingness was necessary by the nonaphasic partner to “sublimate his or her own role as the author and principal of messages” (p. 123); and finally, the person with aphasia had to be willing to sanction the nonaphasic partner’s role as “spokesperson.”
The current study used alignment in a somewhat similar way as Simmons-Mackie and colleagues’ (2004) “speaking for” framework. However, whereas the nonaphasic person in Simmons-Mackie et al. used the “speaking for” framework in repair sequences, the current study prescribed frequent reflecting (i.e., alignment) utterances whether there was a breakdown in conversation or not. This technique was deliberately implemented so that, when there was no breakdown, an affirmation of communicative competence could occur (Kagan et al., 2001), and during conversational breakdowns, the person with aphasia in this study could “hear herself speak,” providing the opportunity for her to initiate a conversation repair, and/or her communication partner could do so. Thus, the emphasis in ACT was on proactive steps to improve communication rather than a focus on repairing breakdowns.
Purpose
How then, could those with aphasia accomplish alignment, when conversation is fraught with errors, missteps, and so on? Alignment, to date, has not been reported as a strategy per se (the article reviewed above by Fridriksson used “entrainment,” but this was not used in the context of conversation, using scripts instead). The current article addresses the overt implementation of alignment to determine its utility in improving the output of an individual with difficulty in auditory processing.
Simply reflecting back what has been heard is a simple, overt method for accomplishing alignment. Thus, it was assumed that training Mr. E to reflect what he heard during a conversation (whether an intended utterance or one with obvious “errors”) would have a positive impact on the conversations of this couple. This would occur in two ways. First, it would make the conversation more like the normal conversations described in the literature—complete with examples of alignment. Second, it gave Ms. E, with her difficulty comprehending the spoken word, a second opportunity to hear her own words. This would lend support to the auditory comprehension deficit experienced by Ms. E.
This study reports a couple who demonstrated no evidence of pretherapy alignment, who met twice weekly for 20 weeks using a couples-based approach. Among the dependent variables was a measure of the use of reflection (i.e., alignment). The following research questions were posed:
Method
Participants
Ms. E was a 75-year-old right-handed college graduate and retired office manager prior to the study. She had an unremarkable health history and was a youth group leader in her church before the stroke, 3 years prior. At that time, she sustained a left hemisphere stroke with paresis on the right side of her body, inability to speak, and significant difficulty with eating and swallowing. A computerized tomography (CT) scan revealed a large temporal-parietal lesion in the left hemisphere. She was able to walk short distances at home but used a wheelchair when in therapy sessions. She did not write or draw, even when encouraged to do so. She had limited use of her premorbidly preferred right hand, and did not attempt to write or draw with it. During an informal interview, she spoke fluently, with frequent failures to convey ideas. For example, when asked about her children, she responded, “they’re all right there and they have to be there at the—oh, I really can’t say, I’m sorry.” When asked to talk about one of her great-grandchildren, Ms. E said, “oh she is so cute, she is just a doll, just adorable.” She could usually state the names of her family members, with occasional prompting from her husband. However, she often confused personal pronouns, confusing “he” and “she” even when referring to herself. For example, when her husband asked her if she had enjoyed the visit from their son, she responded, “oh yes, she had a lovely time, and it was so good to see them all.”
Table 1 reports test data prior to initiation of treatment. The Western Aphasia Battery–Revised (WAB; Kertesz, 2007) results were consistent with Wernicke’s aphasia. That is, she spoke in fluent utterances but had a relative weakness in auditory comprehension, poor ability to repeat utterances, and little awareness of her deficits (Kertesz, 2007). Observations during informal interviews demonstrated that her auditory comprehension benefitted from more context. That is, she appeared to understand what was said to her in conversation (e.g., responding appropriately to highly contextualized questions and laughing at appropriate times during conversation), although she often required time to process what was said. For example, when asked how her previous weekend had gone, she responded, “Oh it was lovely. We drove to the place down there and we had a good time of it, yes.” Her scores in the auditory comprehension subtests were the main factor in classifying her deficits as Wernicke’s aphasia, and these scores were near the upper end of the cutoff, which otherwise would have placed her in the “conduction” category.
Test Results for Ms. E.
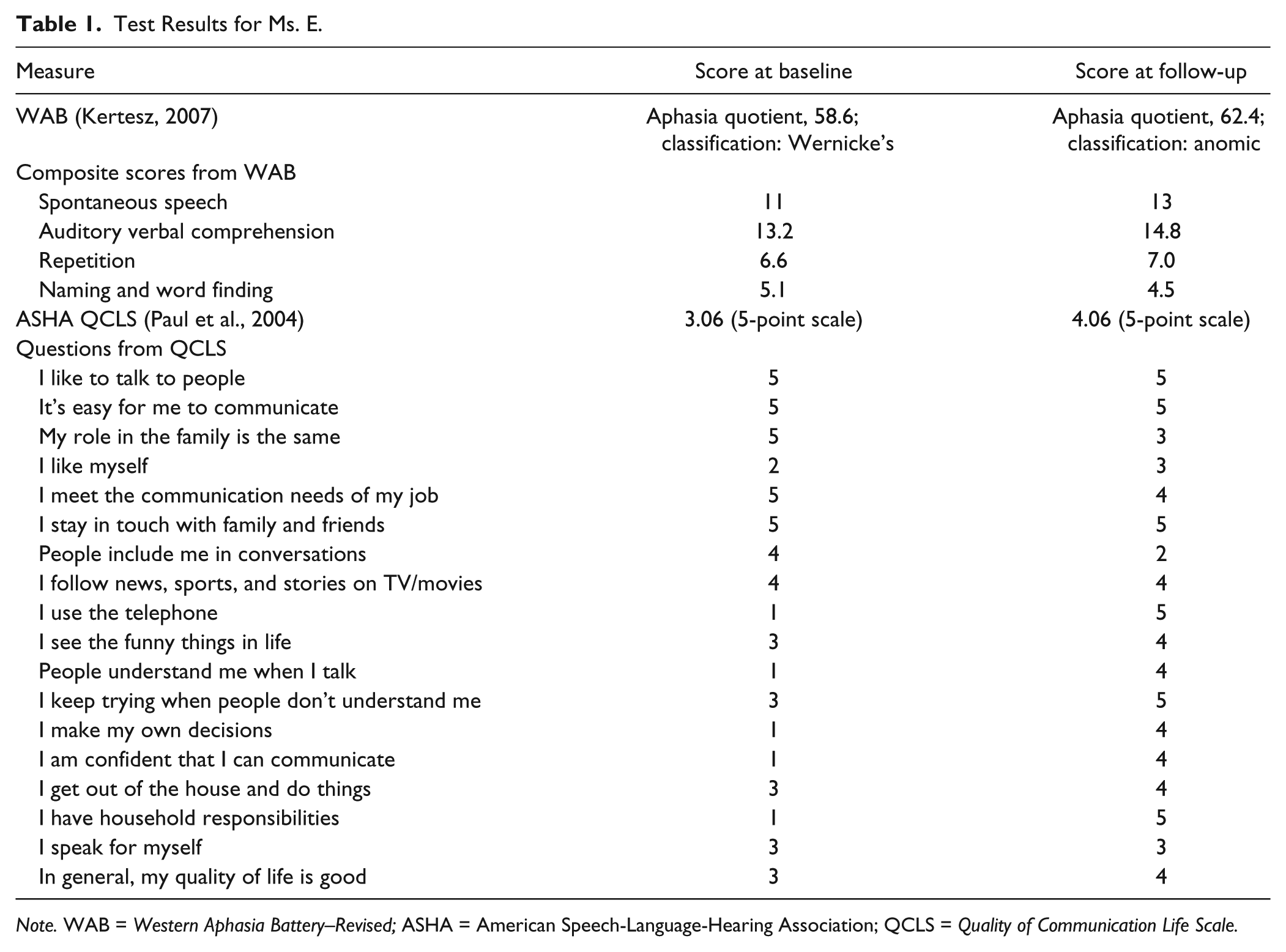
Note. WAB = Western Aphasia Battery–Revised; ASHA = American Speech-Language-Hearing Association; QCLS = Quality of Communication Life Scale.
Ms. E’s husband, Mr. E, a 75-year-old man, was an attorney and semi-retired professor at a law school, teaching one class per semester. He was active in local and national politics, which he enjoyed discussing in his conversations with his wife. He spent much of his time as caregiver to his wife. He was quite supportive of Ms. E and her efforts to improve communication, and indicated a willingness to change some of his own communicative behaviors to achieve a more interactive engagement with his wife.
Procedures
Informed consent
A written informed consent form was reviewed by the Institutional Review Board of this author’s university. This consent form was written with aphasia-friendly pictograms, such that Ms. E was aware of the intent and risks of the study. Both Mr. E and Ms. E signed the consent form, and a copy was given to them.
Analysis of conversations
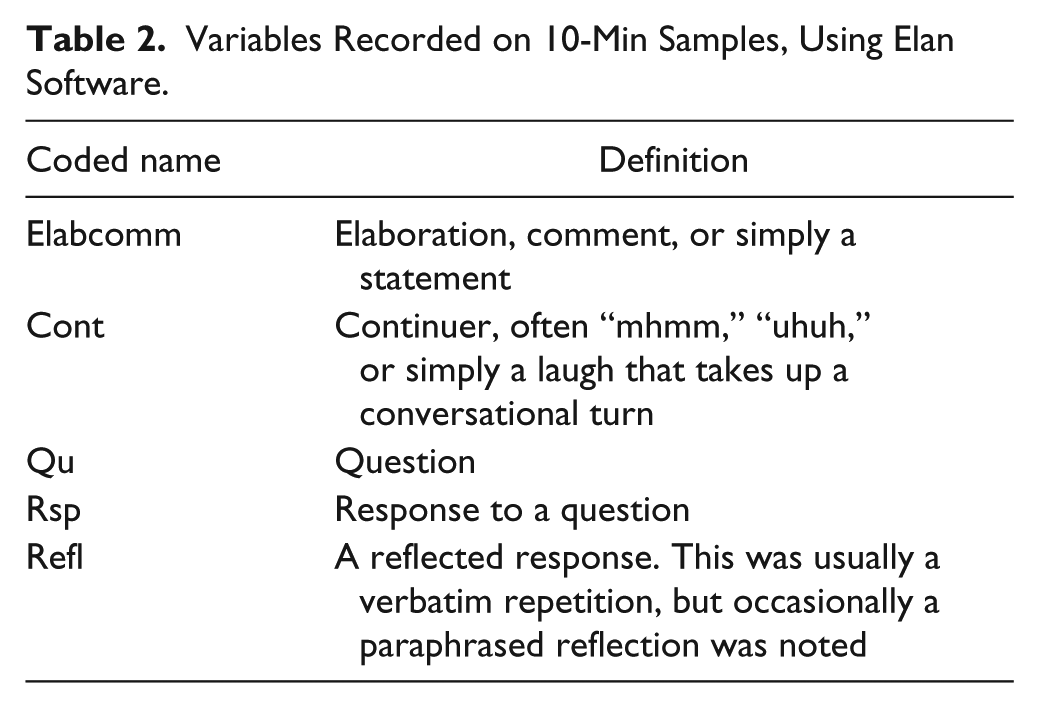
The couple was encouraged to talk about any topic they wished during the baseline and probe sessions throughout the study. They were left alone for a 10-min span, with conversations video-recorded for later analysis, using Elan software. Elan is free software distributed by the Max Planck Institute for Psycholinguistics. It was chosen for its ease of use for rapid analysis. Three initial baseline sessions were recorded. Dependent variables were negotiated between Mr. E, Ms. E, and this researcher, upon review and informal analysis of the baseline conversations, prior to the implementation of the therapy. These variables, listed in Table 2, were coded for analysis using Elan. These variables were considered the “purpose” of each utterance, whether an elaboration, a question, a response to a question, and so on. Thus, the variables represented pragmatic categories, rather than semantic or grammatical ones. From the variables listed in Table 2, the following goals were established, upon negotiating with the couple before therapy was implemented (see Table 3). The unit of time for each goal was per 10-min probe. For Ms. E: (a) increase in number of utterances, (b) increase in words per utterance, (c) increase in percentage of utterances for the 10-min conversation, and (d) increase in coherence/clarity in utterances. For Mr. E: (a) decrease in number of utterances, b) decrease in percentage of utterances for the 10-min conversation, and (c) increase in number of reflections (as a measure of alignment).
Variables Recorded on 10-Min Samples, Using Elan Software.
Variables Comprising Therapy Goals for 10-Min Samples.
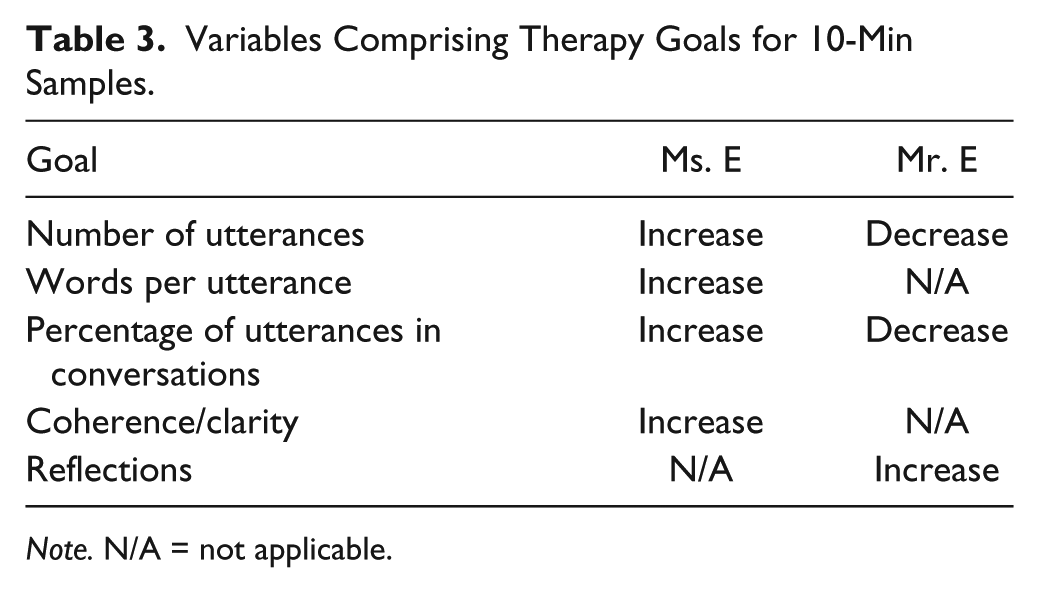
Note. N/A = not applicable.
To determine whether the conversations by the couple would be rated as more satisfying and/or more balanced, 54 graduate students who had no knowledge of the study or the nature of the therapy viewed the same three 10-min probe-session video clips and were asked to complete a three-item Likert-type scale (scaled 1–5) questionnaire. The three questions were as follows: (a) How satisfying was the conversation, (b) How much struggle occurred in the conversation, and (c) how balanced was the conversation. The 54 students used this rating for Probe 1 (not the Baseline Probe 1), Probe 9, and Probe 20. Like all sessions, the topics of conversation were not predetermined. However, in all three probes, the couple spent nearly the entire 10-min probe discussing extended family members.
Therapy sessions
Therapy sessions were conducted twice weekly for 60 min, for 20 weeks. Brief (usually 1–3 min) conversations were interrupted by the SLP when deemed useful to point out success (and occasional lack of success) with alignment, yielding the “conversational floor,” and other facilitative acts by either party. Following this feedback, the couple engaged in another brief conversation. This routine was followed throughout each session. The couple was encouraged to (and by self-report, usually complied with) a suggestion to converse every morning at breakfast for 5 min, using the suggestions given during therapy, as described above.
Probe sessions
Once weekly, prior to a session, the couple was video-recorded for 10 min, with the instruction to converse about any topic they liked. The therapist left the room with the video equipment running and returned to turn it off after 10 min had elapsed.
Results
Test score results are reported below followed by the results of the conversation measures. The latter are reported in the sequence of the research questions, posed in the “Purpose” section. Effect sizes are reported, as measured by the d-statistic (Beeson & Robey, 2006), which estimates the degree to which the follow-up data represent a change from the baseline data.
Test Scores
Ms. E’s aphasia quotient on the WAB changed from a baseline of 58.6 to 62.4, a nonsignificant change, in the 20-week duration of the study. Her Quality of Communication Life score changed from 3.06 to 4.06, on a 5-point scale (see Table 1).
Conversation Measures
The remaining results are presented in the form of the research questions posed at the end of the “Purpose” section of the article. They are numbered in this “Results” section just as they are in the previous section of the article. A second judge, trained by the author, viewed 4 of the 25 video recordings, selected randomly. Agreement with this author was .95 for utterance type and demarcations, and .99 for the actual counting of words. Intrajudge agreement by the author, using the same four recordings was .99 for utterance type and 1.00 for counting of words.
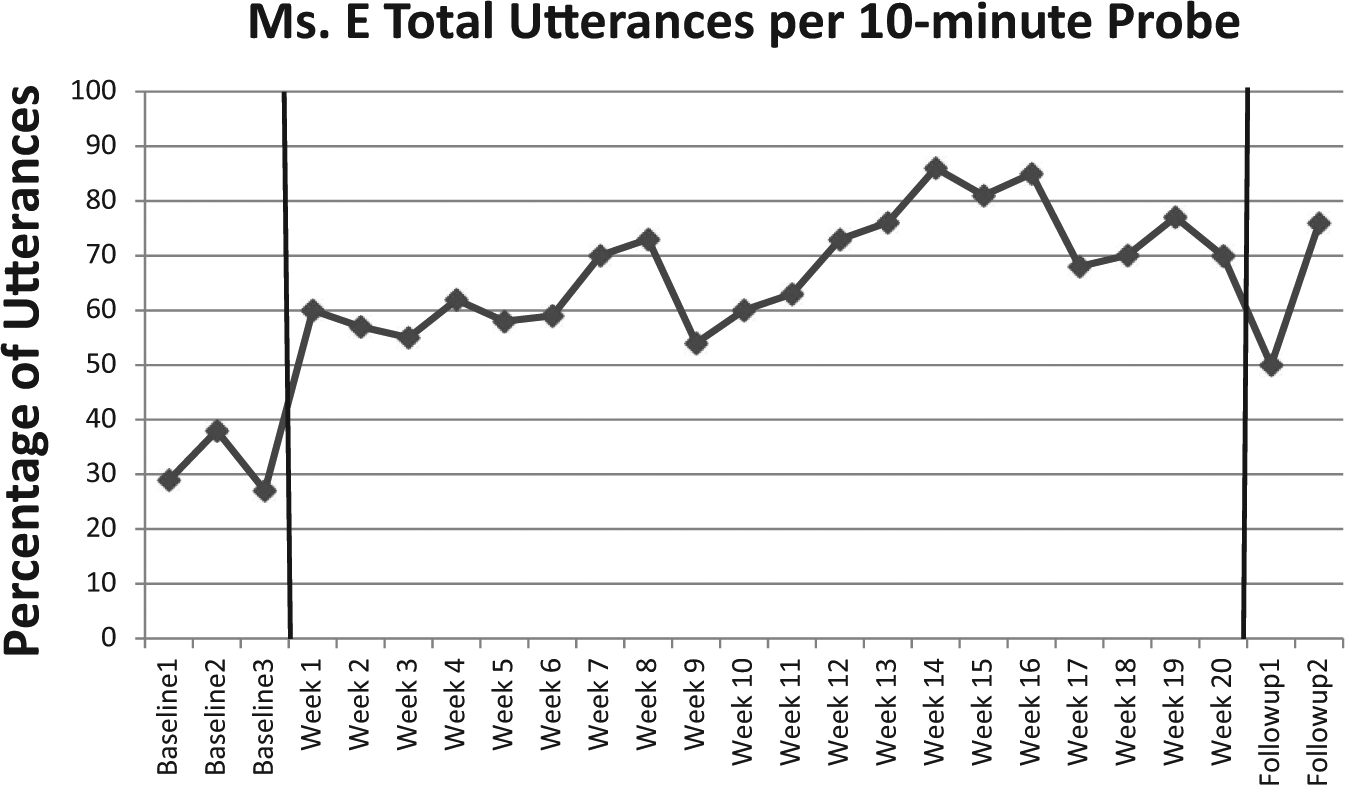
Would Ms. E increase her relative contribution of utterances in conversation? The relative contribution (measured in percentage of utterances contributed by Mr. and Mrs. E) of the participants is shown in Figure 1. The total contribution of utterances for both participants, of course, will always total 100%. The conversations were considerably more balanced immediately when therapy began and continued throughout the study. The d-statistic (Beeson & Robey, 2006) is a measure of effect size used in single-subject ABA designs. This statistic measures the degree of difference in means between the baseline measures and the follow-up measures. The d-statistic, as used in ABA designs, is expressed by the formula d1 = (XA2 − XA1)/SA1, where the mean for the baseline measures (XA1) is subtracted from the mean for the follow-up measures (XA2), and the remainder divided by the standard deviation of the baseline measures (SA1). Beeson and Robey (2006) considered a d-statistic effect size of 3.9 to be a medium-sized effect and 5.8 to be a large effect. The d-statistic for this research question, d = (0.496 − 0.278)/0.039, where the standard deviation was 0.039, revealed a value of 5.47, a medium effect size.
Would Mr. E reflect what Ms. E had said more frequently (i.e., increase alignment) when encouraged to do so? Figure 2 revealed a positive change in the number of reflective utterances by Mr. E, d = (10 − 0.667)/0.577, with a large effect size (d = 16.17).
Would there be an increase in Ms. E’s utterances? Figure 3 shows the number of utterances by Ms. E throughout the study. A medium effect size, d = (63 − 31.333)/5.859 occurred (d = 5.40)
Would there be an increase in the number of words per utterance for Ms. E? Figure 4 reveals a positive change in Ms. E’s verbal production, d = (274.1 − 99)/6.557, with a large effect size (d = 26.76).
Would there be a relationship between the reflections by Mr. E and the number of utterances by Ms. E? Pearson product correlations revealed a modest positive correlation between Mr. E’s use of reflections (hence, “alignment”) and the number of coherent words used by Ms. E (r = .62, n = 25, p = .001) and between Mr. E’s use of reflections and her utterances categorized as “comment, elaboration” (r = .68, n = 25, p = .000).
Would naïve observers of video clips of therapy sessions perceive later sessions as more positive than earlier sessions? One-way ANOVA with Tukey post hoc analysis revealed significant differences, F = 9.24; df(2, 160). Probe 1 was a less satisfying conversation to naïve observers than Probe 9 (p = .047), and Probe 1 was less satisfying than Probe 20 (p = .000). No difference in satisfaction was reported between Probes 9 and 20 (p = .138). Significant differences in balance were reported by the observers, F = 11.17; df(2, 161). The amount of balance in the conversation was judged to be least for Probe 1 and most for Probe 20, with significant differences between Probes 1 and 9 (p = .030) and between Probes 1 and 20 (p = .000), but not between Probes 9 and 20 (p = .080). Naïve observers did not perceive significant differences for the three probe sessions for degree of struggle (F = 2.96; p = .054).
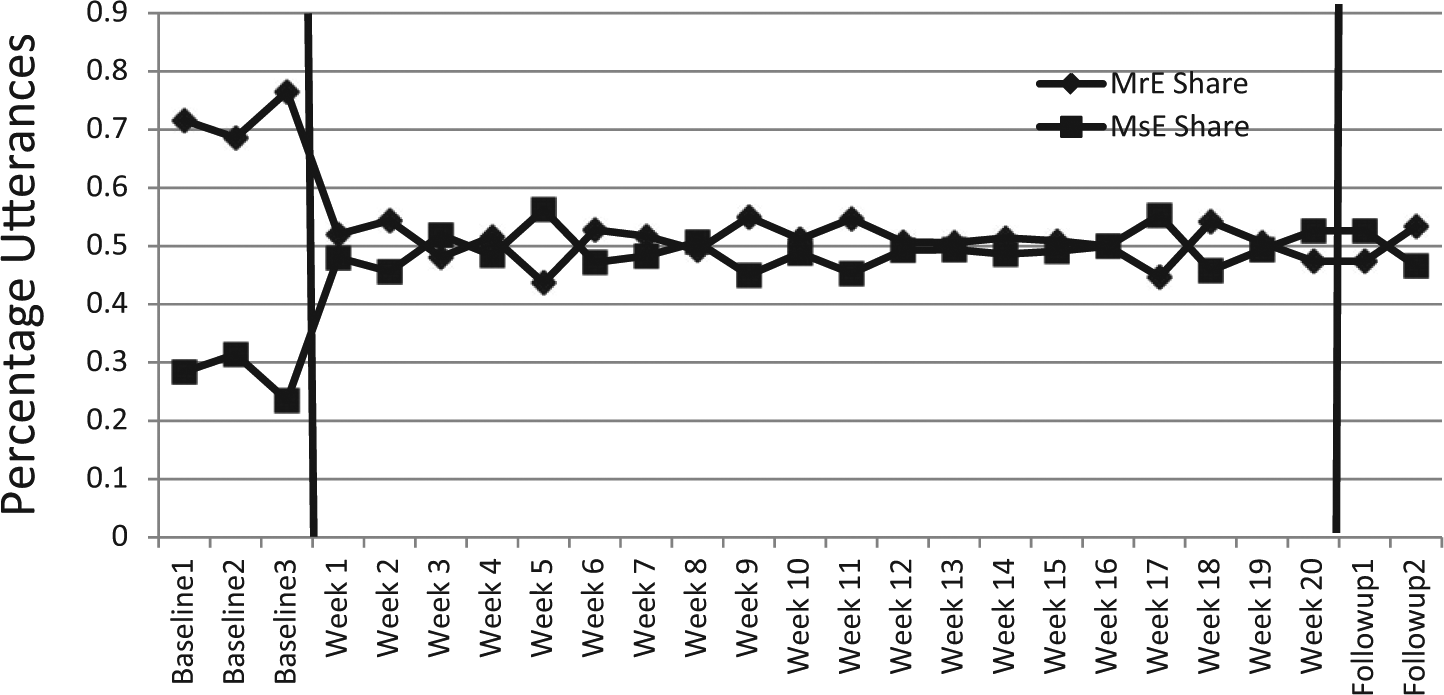
Relative contribution of utterances by Ms. E, the client with aphasia, and Mr. E, her husband.
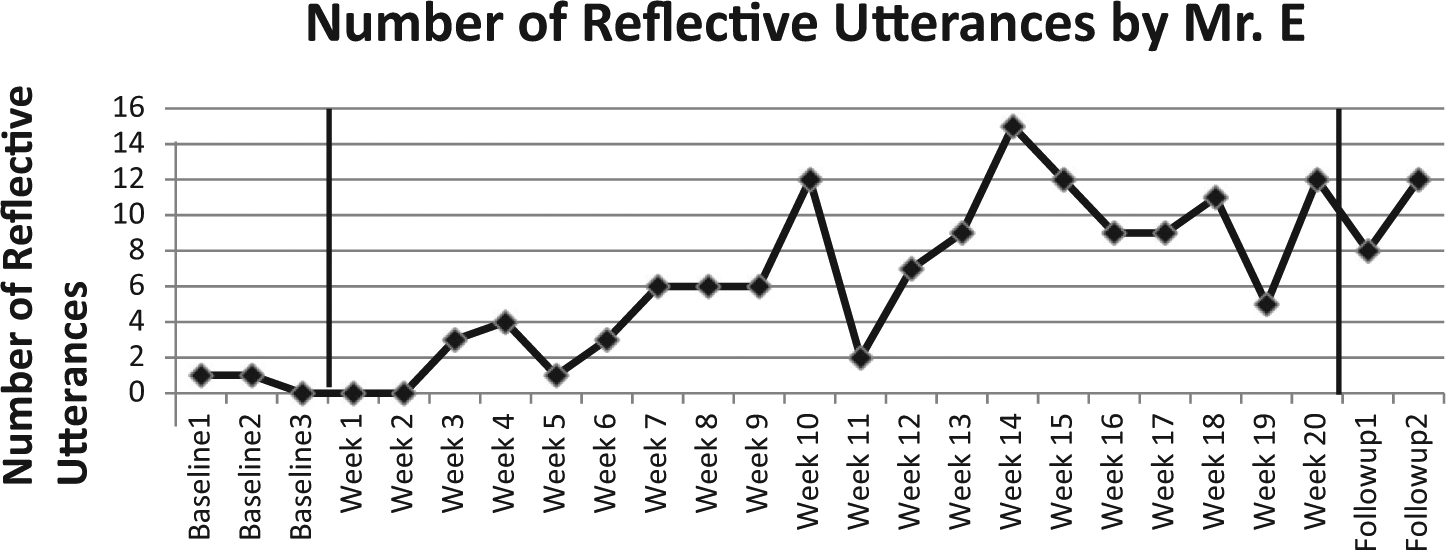
The use of reflective utterances on the part of the nonaphasic husband, Mr. E.
Contribution of utterances by Ms. E, the client with aphasia.
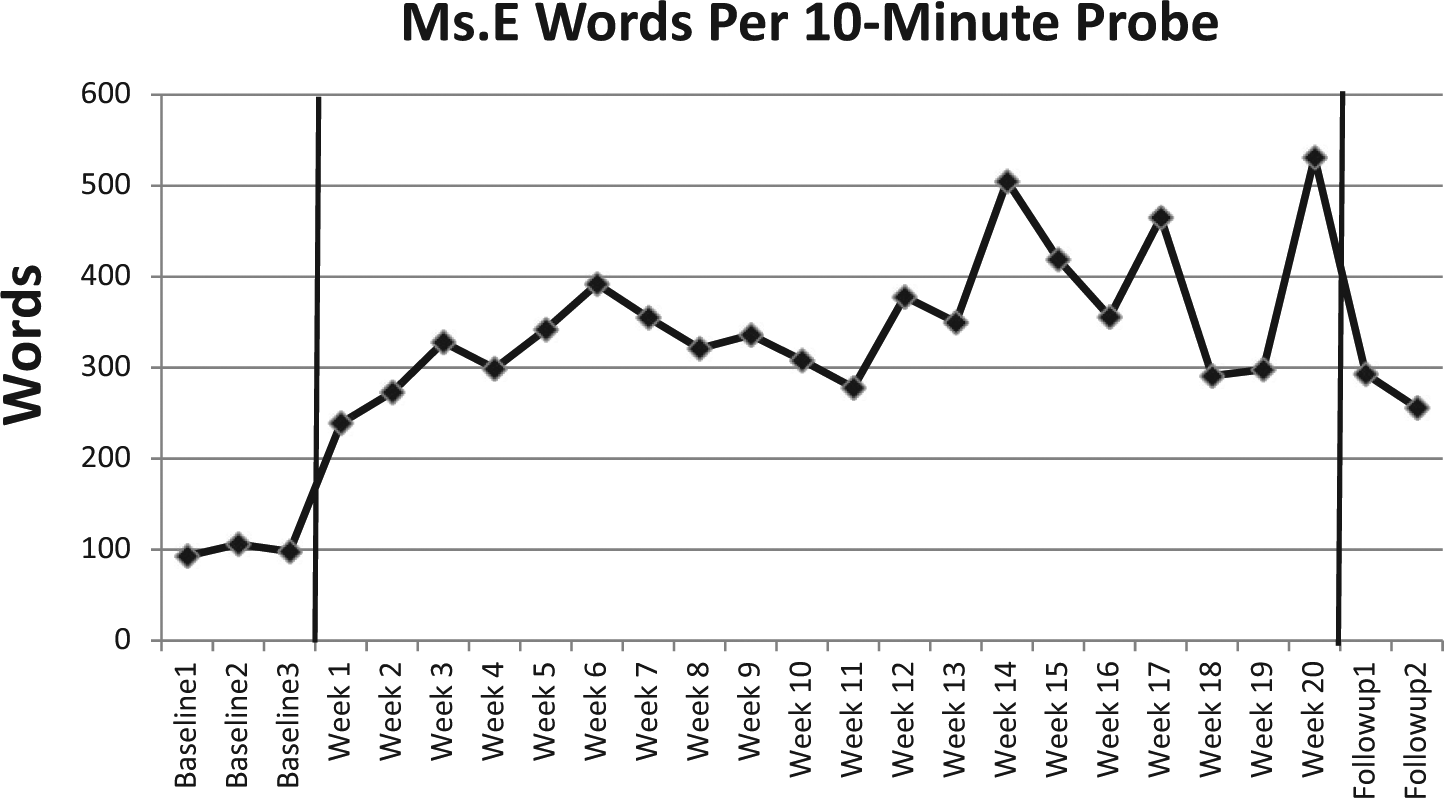
The number of words used per 10-min sample by Ms. E.
Quality of Communication Life
The mean score by E on the Quality of Communication Life Scale (QCLS) was 3.06 at baseline and 4.06 after Session 8. The questions on the QCLS were presented verbally and in writing, and the responses by Ms. E were made on a graphic thermometer-type display with icons representing positive (top of thermometer) and negative (at the bottom) responses.
Discussion
This article contributes to the growing literature on ACT. Ms. E, the woman with aphasia made measurable gains, with robust effect sizes in all conversation measures. The research questions will be addressed next.
The balance in conversation achieved by this couple (i.e., Research Question 1) was notable. They progressed from self-described monologues by Mr. E to equal participation by both parties, as Figure 1 shows. ACT facilitated this change in both members. For example, during therapy sessions, if Mr. E did not wait for his wife to respond, the therapist halted his interjection by either telling him directly (e.g., “ wait, give her time here”) or nonverbally (e.g., holding up a hand as if to say, “wait”).
The use of alignment was a central focus of this research. Significant others have been used in therapy in previous research, as described in the “Purpose” section. However, the specific use of reflective utterances as a technique for achieving improvement in communication during couples-based therapy has not been reported previously. It stands to reason, then, that an increase in alignment would be desirable in such a study, and that increase was realized (see Figure 2). These reflective utterances did not represent conversation repair. Rather, they became deliberate, prescribed responses to the responses on the part of Ms. E, the participant with aphasia.
Research Questions 3 and 4 addressed measures of increased verbal output by Ms. E. It would make little sense to recommend increases in alignment without an increase in one or more measures of communication improvement by the person with aphasia. Indeed, increases in both utterances and words by Ms. E were realized (see Figures 3 and 4, respectively).
It should be noted that Ms. E did exhibit some instability in terms of the number of utterances she produced per 10-min probe. She decreased her number of utterances from 70 in Session 20 to 50 utterances in the first follow-up session. However, in those same sessions, her husband Mr. E contributed 63 utterances in Session 20 and 45 utterances in the first follow-up session. Thus, this was not an example of Mr. E returning to a dominance of the conversation but rather both members of the couple having “less to say.”
Figure 4 also reveals a decrease in the two follow-up sessions compared with the sessions immediately preceding those data. Again, however, considering both members of the couple had decreased their spoken output, this was not a concern.
The next question was whether there was a relationship between the use of alignment by Mr. E and the increased verbal output (measured in number of utterances), and the number of coherent words by Ms. E (Research Question 5). However, it is possible to increase the number of one’s utterances without a change in substantive content. For example, saying “I see,” “is that so,” and so forth could increase the number of utterances, yet have no greater substantive contribution to a conversation. For that reason, a comparison of Mr. E’s reflective utterances and Ms. E’s utterances categorized as comments or elaborations was made, and indeed a positive correlation was found, as reported above in the “Results” section. Thus, it appears that a fairly direct route to improving the productive verbal output by a person with Wernicke’s aphasia is the use of deliberate, prescriptive alignment by the significant other during conversations. This gives the significant other a tool that goes well beyond passive observance of what the SLP is implementing.
Another measure intended as a kind of “safeguard” was to determine whether naïve observers would perceive conversations more positively toward the end of therapy compared with the beginning. Objective measures described above are useful indicators of success, and both the clients and therapist were pleased with the results; however, it would add validity to the study should people unfamiliar to this work perceive the video-recorded interactions more positively toward the end of the study (Research Question 6). That did occur, as these observers felt later probes were more satisfying than a baseline probe. Interestingly, no difference in satisfaction was reported by these observers between Probe 9 and Probe 20. One explanation for this is that perhaps fewer sessions would be just as beneficial as the 20-week, 40-session regimen reported here. Visual inspection of Figures 1 to 4 suggests this may be the case. Future research could address this issue.
ACT, like most aphasia therapies, requires measures for improvement that are not determined until an evaluation is implemented. Unlike more traditional methods, ACT relies on information from both members of the couple for its outcome measures. These measures do not come from test scores from the decontextualized tasks of traditional methods, such as naming common objects and repeating sentences, but rather from clinical observation and discussion of conversations prior to the implementation of therapy by the SLP and the couple. Obviously, people with aphasia and their spouses return home from therapy sessions to converse, rather than to have didactic decontextualized interactions.
It is not argued here that ACT is superior to more traditional methods. However, in aphasia therapy that excludes significant others from active participation, the strategies used by the therapist to elicit responses are unlikely to be used as skillfully by the significant others without direct instruction. ACT has generalization built into the method, by virtue of the fact that the person interacting with the patient is returning home with the patient.
Alignment
It would be difficult to overstate the importance of alignment in normal conversation. Garrod and Pickering (2004) argued that the success of conversations depends on it. In normal conversation, we accomplish this interactive common ground by using the very words that our conversation partner uses. Empirical evidence supports that phenomenon (e.g., Goudbeek & Krahmer, 2012; Shintel & Keysar, 2009). These descriptive studies did not manipulate alignment as an independent variable, as was true in the current study. Rather, they described it as an unconscious phenomenon in normal conversation. The results of this study show us that, although alignment is an unconscious phenomenon in normal conversation, it need not be. Furthermore, the conscious use of alignment can improve the quality of conversations by a couple and the perception of improved conversation quality by outside observers.
Making unconscious speech acts more deliberate is frequently implemented in aphasia therapy. We normally label objects, use particular grammatical markers, and make conversation repairs. We also encourage our patients to increase their use of these normally unconscious devices. It appears that the use of alignment can be an effective device for improving the communication of a person with Wernicke’s aphasia.
Previous Research
Most of the previous research using couples in treatment describe conversation repair—responding to breakdowns in communication. The work of Wilkinson et al. (1998), Hopper et al. (2002), and Cunningham and Ward (2003) used that strategy. Patients were given strategies for increasing the efficiency of conversation repairs. This contrasts with the current study in that a strategy (i.e., alignment) was encouraged proactively, whether or not a conversation repair was necessary.
The SCAA approach by Kagan et al. (2001) trained conversational partners to acknowledge and reveal conversational competence of the person with aphasia. This approach, though quite successful, differed from the current approach in that the partners had different relationships with the aphasic partners (they were trained volunteers), and alignment was not used as an independent variable.
Previous research by this author (Boles, 1997, 1998, 2000) and colleagues (Boles & Lewis, 2003; Fox et al., 2009) used similar therapy configurations, in that the significant other was a primary contributor to the implementation of therapy. However, these studies did not use alignment as an independent variable.
Alignment in Aphasia Therapy
Aphasia therapy can be challenging when a person’s weakness is auditory comprehension. Moreover, improving the comprehension of decontextualized utterances does not guarantee generalization to conversations. Spouses and significant others often request ideas for how they can help their loved one speak more effectively. By focusing the instructions to the couple on alignment, as described in this article, the patient was able to “hear herself speak” twice—once when she first uttered her words and a second time when her husband reflected that utterance back. This may have contributed to her increased participation and verbal production.
Thus, this article extends previous research on ACT and provides evidence that increasing alignment can be beneficial in a case of Wernicke’s aphasia. The use of alignment by the woman’s husband, in the form of reflective utterances, reinstated a naturally occurring phenomenon (alignment) into their conversations, creating more of a dialogue, and less of a monologue (i.e., by the nonaphasic spouse).
The current study used a single subject in its design. Although ACT has been used with a wide range of aphasia types and severity, the specific use of alignment has not. Future research with different aphasia types and severity could address this.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.